

Abstract
Objective
Computer-tailored interventions have become increasingly common for facilitating improvement in behaviors related to chronic disease and health promotion. A sufficient number of outcome studies from these interventions are now available to facilitate the quantitative analysis of effect sizes, permitting moderator analyses that were not possible with previous systematic reviews.
Method
The present study employs meta-analytic techniques to assess the mean effect for 88 computer-tailored interventions published between 1988 and 2009 focusing on four health behaviors: smoking cessation, physical activity, eating a healthy diet, and receiving regular mammography screening. Effect sizes were calculated using Hedges g. Study, tailoring, and demographic moderators were examined by analyzing between-group variance and meta-regression.
Results
Clinically and statistically significant overall effect sizes were found across each of the four behaviors. While effect sizes decreased after intervention completion, dynamically tailored interventions were found to have increased efficacy over time as compared with tailored interventions based on one assessment only. Study effects did not differ across communication channels nor decline when up to three behaviors were identified for intervention simultaneously.
Conclusion
This study demonstrates that computer-tailored interventions have the potential to improve health behaviors and suggests strategies that may lead to greater effectiveness of these techniques.
MESH Keywords: behavioral research, exercise, smoking cessation, diet therapy, behavioral medicine, mammography, telemedicine
Introduction
Health behaviors account for an estimated 60% of the risk associated with chronic illnesses such as diabetes, cardiovascular diseases, and some cancers (Institute of Medicine, 2001). With chronic illness responsible for the majority of deaths in the United States (Centers for Disease Control, 2008), effective strategies must be developed and disseminated for improving health-related behaviors on a population level. Computer-tailored interventions have become an increasingly common strategy for altering health risk behaviors such as tobacco use, poor diet, and lack of exercise that are linked to chronic disease. While early computer-tailored interventions relied largely on print materials as a communication channel, with more recent advances they can readily be provided via personal computer or even mobile phone, further reducing their cost and expanding their availability. Tailored messages are thought to foster behavior change by providing personally relevant feedback. For instance, a program could assess an individual’s self-efficacy to quit smoking and suggest specific ways to increase confidence for dealing with the smoking cues they identified as most difficult.
As methods of computer tailoring have developed, numerous variations on the concept of tailoring have been employed in research trials, differing across number of contacts, communication channel, theory, number of contacts, and other intervention options. Such design decisions have usually been based on the assumption that each would contribute to the efficacy of an intervention, yet little research has compared these potential moderators of treatment efficacy across studies. These options have also led to confusion in distinguishing computer-tailored from computer-delivered interventions. While computer-delivery is a type of communication channel (such as printed letters), “computer-tailoring” is a method of assessing individuals and selecting communication content using data-driven decision rules that produce feedback automatically from a database of content elements. Computer tailoring is thus a form of tailored communications which involve a “combination of strategies and information intended to reach one specific person based on characteristics that are unique to that person, related to the outcome of interest, and derived from an individual assessment” (Kreuter and Skinner, 2000). This meta-analysis focuses on interventions that tailored feedback to individual users by means of computer algorithms, regardless of whether the feedback was delivered via print, telephone, or computer terminal.
Prior reviews of tailoring have drawbacks that limit their utility for advancing the effectiveness of this methodology. Reviews that focus solely on one behavior such as mammography (Sohl, 2007), smoking (Strecher, 1999), or nutrition (Brug, et al., 1999) may confuse effects of computer-tailoring with behavior-specific findings. Those that examine a specific intervention medium such as interactive computer (Norman, 2007, Portnoy, et al., 2008) or print (Noar, et al., 2007) limit tailoring to a single communication channel. Finally, those that have not employed meta-analytic data analysis methods (Kroeze, et al., 2006, Ryan and Lauver, 2002, Skinner, et al., 1999, Strecher, 1999) succumb to the drawbacks of significance testing and are limited in their ability to analyze moderators. This study extends and builds upon the most comprehensive meta-analytic review to date (Noar, et al., 2007) by examining both print and computer-delivered interventions, by modeling weighted group variance for statistical tests, and by systematically examining publication bias and study quality as is presently recommended (Lipsey and Wilson, 2001). Unlike past reviews, this meta-analysis also examines the effects of computer-tailored interventions across multiple outcome time points and examines the efficacy of employing dynamic tailoring (assessing intervention variables prior to each feedback) versus static tailoring (providing one baseline assessment on which to base all successive feedbacks), which are important analyses for informing future intervention design.
The present study accounts for these additional moderators and reports the efficacy of computer tailoring in facilitating health-related behavior change for smoking cessation, physical activity, healthy dietary practices, and regular mammography screening across multiple outcome time points. We hypothesize that non-engagement in each behavior as a participation criterion and comparison to assessment-only control groups will be related to larger effect sizes (Tunis, et al., 2003). Based on previous findings suggesting differences in study design, we also expect that studies completed outside of the United States (Noar, et al., 2007), and those lower study quality ratings (Moher, et al., 1998) will show larger effects. Additionally, we expect that interventions provided for multiple behaviors simultaneously will show comparable effect sizes to those that concentrate on one behavior alone (Prochaska, et al., 2008) and that dynamic tailoring will not differ from static tailoring (Heimendinger, et al., 2005, Strecher, et al., 2005). As demographic characteristics are often controlled for in randomization, we predict that age, gender, and minority representation will not be related to effect size.
Methods
Search strategy
A combination of search methods was used to locate all published and in-press studies that employed a tailored intervention. The electronic databases PsycInfo, PubMed, CINAHL, and the Cochrane library were searched for studies using following terms: “(tailor*) and (compute* OR feedback OR individualized)”, “expert system”, “e-health AND (tailor* OR feedback OR individualized)”. Reference lists from published studies were examined, and authors were contacted for additional information. Electronic databases were then re-searched for articles published by authors previously identified to locate studies that may have employed similar techniques.
Selection criteria
The search was inclusive of studies published from 1988 (the year of the first tailored feedback study) to March 2009. Studies selected for analysis met the following criteria: a) were “computer-tailored” in that they used computers to choose individual feedback based on decision algorithms; b) provided the intervention primarily via communication channels that did not use live counselors; c) included a non-tailored comparison group; and d) reported sufficient statistical information to calculate effect size (e.g. means, standard deviations, odds ratios, t- and p-values). The final analysis included smoking cessation, physical activity, dietary practices, and mammography screening because the largest number of studies have been completed focusing on these behaviors, thereby limiting heterogeneity and enabling stable comparisons across behaviors.
Outcome selection
As has been suggested for improving the interpretation of clinical trial data (Thompson and Schoenfeld, 2007, Tunis, et al., 2003), the minimal intervention (usually informational pamphlet; see Table 4), was chosen as the reference group for effect size calculation over assessment-only control groups where possible. When studies reported results at more than one time point, the final time point was used, which ensures independence of data and is consistent with procedures used by other reviews (Higgins and Green, 2009, Lancaster and Stead, 2006). For longitudinal analysis, effect sizes were grouped into discrete categories by final outcome time point from baseline with each study contributing no more than one effect size. We also controlled for intervention length by regressing months since intervention completion on effect size.
Table 4.
Description of Studies Included for Analysis of Effect Size (Studies published 1988-2009)
| Study | Health Behaviors and Outcome Measures | N (Baseline) | Intervention Methods | Sample and Recruitment Characteristics | Number of Treatment Contacts | Length of Treatment (months) | Final Assessment (months from baseline) | Retention Rate (%) | Quality Rating (out of 22) |
|---|---|---|---|---|---|---|---|---|---|
| Anderson, Winett, Wojcik, Winett, & Bowden, 2001 | Dieta,c | 464 | Up to 15 dynamically feedbacks+ or no treatment* delivered at grocery store | General population proactively recruited in person at grocery store | 15 | 4 | 6 | 45.0 | 16 |
| Armitage & Conner, 2001 | Dietb | 801 | Behavioral feedback+ or brochure* | Employees proactively contacted at worksite | 1 | 1 | 5 | 64.5 | 15 |
| Ausems, Mesters, van Breukelen, & De Vries, 2004 | Smokingh | 2,376 | 3 tailored letters+, tailored letters plus in-school lessons, in-school lessons only, or assessment-only control group* | Vocational secondary school students in the Netherlands | 3 | 2.5 | 18 | 75.4 | 16 |
| Aveyard, Griffin, Lawrence, & Cheng, 2003 | Smokingg | 2,471 | 3 dynamically tailored feedbacks+, counseling, brochure* or manual-only conditions | Random sample proactively recruited from medical clinic | 3 | 6 | 12 | 50.0 | 16 |
| Bastani, Maxwell, Bradford, Das, & Yan, 1999 | Mammographyi | 902 | Behavioral feedback + manual+ or brochure only* | Proactive random digit dial of general population | 1 | 1 | 12 | 84.0 | 15 |
| Becona & Vasquez, 2001 | Smokingg | 300 | 6 weekly non- tailored pamphlets, 6 pamphlets plus 2 tailored letters+, or manual only control group* | Respondents to advertisements in newspapers, radio, and local television | 6 | 2 | 12 | 82.0 | 17 |
| Block & Wakimoto et al., 2004 | Dietc | 481 | One-time experience with tailored CD- OM+, CD-ROM plus two reminder telephone calls, or a stress management CD-ROM control condition* | Respondents to fliers posted in state agencies serving low- income persons | 1 | 1 | 2 | 98.0 | 18 |
| Bock, Marcus, Pinto, & Forsyth, 2001 | Phys Activityj | 194 | 4 dynamically tailored letters and manual+ or brochure only* delivered at home | Respondents to fliers and announcements | 4 | 6 | 12 | 33.0 | 16 |
| Borland, Balmford, & Hunt, 2004 | Smokingg | 1,058 | 3 dynamically tailored letters+ or brochure-only* delivered at home | Callers to cancer info line | 5 | 12 | 12 | 70.0 | 17 |
| Borland, Balmford, Segan, Livingston, & Owen, 2003 | Smokingg | 1,578 | 3 dynamically tailored reports+, counseling calls, or manual-only* conditions delivered at home | Callers to cancer info line | 3 | 6 | 12 | 76.6 | 17 |
| Brug, Glanz, van Assema, Kok, & Van Breukelen, 1998 | Dietb,d,e | 762 | 2 dynamically tailored letters, tailored letter, or brochure-only* conditions delivered at home | Respondents to fliers and announcements | 2 | 2 | 3 | 91.8 | 17 |
| Brug, Steenhuis, van Assema, Glanz, & DeVries, 1999 | Dietb,d,e | 347 | Tailored report+ or behavioral feedback-only* delivered at home | Proactively recruited employees from worksite | 1 | 1 | 2 | 91.0 | 12 |
| Brug, Steenhuis, van Assema, & de Vries, 1996 | Dietb,d,e | 507 | Tailored letter + or brochure* delivered at home | Proactively recruited employees from worksite | 1 | 1 | 2 | 51.0 | 15 |
| Bull, Jamrozik, & Blanksby, 1999 | Phys ActivityL | 763 | Tailored report+, brochure*, or assessment-only plus physician advice delivered at home and clinic | Proactively recruited patients from clinic list | 1 | 1 | 12 | 57.0 | 17 |
| Bull, Kreuter, & Scharff, 1999 | Phys ActivityL | 272 | Tailored report+, personalized feedback, brochure* or assessment only delivered at home | Proactively recruited patients from clinic list | 1 | 1 | 3 | 75.0 | 17 |
| Burnett, Magel, Harrington, & Taylor, 1989 | Dietb | 77 | Tailored letters+ or informational brochure only* delivered at school | Proactively recruited students from high schools | 3 | 3 | 3 | 99.0 | 12 |
| Campbell & Bernhardt et al., 1999 | Dietc | 459 | Tailored +, culturally tailored bulletin, or assessment-only* conditions delivered at home | Proactively recruited from church attendees | 1 | 10 | 12 | 82.0 | 16 |
| Campbell & Carbone et al., 2004 | Dietb,c | 410 | Tailored interactive computer feedback+ or assessment-only* condition delivered at clinic | Proactively recruited patients from clinic list | 1 | 0 | 2 | 74.8 | 18 |
| Campbell, DeVellis, Strecher, & Ammerman, 1994 | Dietb,c | 558 | Tailored letter+, brochure*, or assessment-only conditions delivered at home | Proactively recruited patients from medical clinic | 1 | 1 | 4 | 82.0 | 18 |
| Campbell & Honess et al., 2004 | Dietb | 526 | Tailored feedback or assessment-only* condition delivered via computer at clinic | Proactively recruited patients from medical clinic | 1 | 1 | 3 | 72.0 | 17 |
| Campbell & James et al., 2004 | Dieta,c Phys Activityj |
850 | 4 tailored newsletters+ and targeted videotapes or lay health advisor (LHA)* conditions | Proactively recruited church attendees | 4 | 9 | 12 | 69.0 | 19 |
| Campbell & Tessaro et al., 2002 | Dietb,c Phys Activityk Smokingg |
859 | 2 dynamically tailored letters+ or assessment-only* conditions delivered at home | Proactively recruited employees for worksite intervention | 2 | 6 | 18 | 63.0 | 18 |
| Cardinal & Sachs, 1995 | Phys Activitym | 113 | Tailored letter+ or behavior feedback* conditions delivered at home | Proactively recruited employees for worksite intervention | 1 | 1 | 7 | 75.0 | 10 |
| Champion & Skinner et al., 2002 | Mammographyi | 1,390 | Tailored letter+, counseling calls, or assessment-only* conditions delivered at home | HMO members contacted via mail and phone | 1 | 1 | 2 | 71.0 | 16 |
| Champion & Skinner et al., 2007 | Mammographyi | 1,245 | Tailored letter+, counseling calls, or assessment-only* conditions delivered at home | HMO members contacted via mail and phone | 1 | 1 | 4 | 91.8 | 16 |
| Clark & Rakowski et al., 2002 | Mammographyi | 1,324 | 2 dynamically tailored letters+, brochure*, or assessment-only conditions delivered at home | HMO members contacted via mail and phone | 2 | 6 | 20 | 77.0 | 16 |
| Curry, McBride, Grothaus, Louie, & Wagner, 1995 | Smokingg | 1,317 | Tailored report +manual+, tailored report +manual+call, or manual-only* conditions, delivered at home | Proactive random digit dial of general population | 1 | 1 | 21 | 76.0 | 15 |
| Curry, Wagner, & Grothaus, 1991 | Smokingg | 1,217 | 3 dynamically tailored letters+ or brochure* delivered at home | Respondents to fliers and announcements | 3 | 3 | 12 | 95.0 | 16 |
| Delichatsios & Friedman et al., 2001 | Dieta,d Phys Activity |
298 | Automated calls+ or physical activity control* conditions delivered at home | HMO members contacted via mail and phone | 11 | 6 | 6 | 50.0 | 18 |
| Demark-Wahnefried & Clipp et al., 2007 | Dieta,c Phys Activityk |
543 | Tailored mailed print materials+ or nontailored mailed materials* delivered at home | Proactively recruited cancer survivors from registries via letters | 7 | 10 | 12 | 95.6 | 21 |
| DiNoia & Contento et al., 2008 | Dietc | 549 | 4 CD-ROM tailored feedback interventions+ or assessment-only* conditions delivered at youth agencies | Students proactively recruited from after school programs | 4 | 1 | 2 | 92.0 | 17 |
| Dijkstra, 2005 | Smokingf | 202 | Personalized feedback delivered through interactive computer+ or brochure* delivered at university | Students proactively recruited through school | 1 | 1 | 4 | 70.0 | 15 |
| Dijkstra & DeVries et al., 1998 | Smokingg | 1,546 | Self-efficacy and outcome tailored information+, self-efficacy tailored information, outcome-tailored information, or no information* conditions delivered at home | Respondents to advertisements in newspapers in the Netherlands | 1 | 1 | 14 | 64.0 | 15 |
| Dijkstra, De Vries, & Roijackers, 1999 | Smokingg | 843 | 3 tailored letters, 1 tailored letter+, manual-only* or assessment-only conditions delivered at home | Respondents to fliers and announcements | 1 | 1 | 6 | 89.0 | 13 |
| Elder & Ayala et al., 2006 | Dietb | 357 | Tailored newsletters+, or tailored letters+counseling, or targeted brochure*, conditions delivered at home | Proactive random digit dial of general population | 12 | 3 | 12 | 79.0 | 17 |
| Etter & Perneger, 2004 | Smokingh | 2,934 | 4 dynamically tailored letters+, brochure* or assessment-only conditions delivered at home | Proactively recruited random sample of general population contacted by mail | 4 | 12 | 24 | 82.2 | 12 |
| Etter, 2005 | Smokingg | 11,969 | Tailored feedback+ or information-only* conditions delivered through computer over Internet | Respondents to smoking cessation website | 1 | 2 | 3 | 35.0 | 17 |
| Frenn & Malin et al., 2005 | Dieta Phys Activityk |
132 | Eight-session Internet/video intervention in school+ or assessment-only* conditions | Students recruited via consent form sent to parents | 8 | 1 | 1 | 77.0 | 15 |
| Greaney & Riebe et al., 2008 | Phys Activityn | 1,274 | Dynamically tailored letters+brief calls+manual+ or assessment-only* conditions delivered at home | Respondents to fliers and announcements | 12 | 12 | 24 | 76.0 | 15 |
| Haerens & Deforche et al., 2007 | Dietb | 307 | Computer-tailored interactive intervention+ or assessment only* conditions | Students recruited from secondary school classes | 1 | 1 | 3 | 91.0 | 18 |
| Hageman & Walker et al., 2005 | Phys Activityk | 31 | 3 tailored+ or nontailored* online newsletters | Respondents to ads placed in newspapers | 3 | 2 | 3 | 90.0 | 17 |
| Heimendinger & Oneil et al., 2005 | Dietc | 3,402 | 4 dynamically tailored+, 4 tailored, 1 tailored letters, or brochure-only* conditions delivered at home | Proactively recruited callers to cancer info line | 4 | 5 | 12 | 57.0 | 18 |
| Irvine & Ary et al., 2004 | Dietb,c | 517 | Tailored intervention at workstation+ or wait-list control* conditions | Employees recruited via advertisements/fliers | 3 | 1 | 2 | 90.0 | 17 |
| Johnson, Driskell, Johnson, Dyment et al., 2006 | Dietn Phys Activityn |
404 | 3 dynamically tailored letters + manual+ or assessment-only* conditions delivered at home | Proactive random digit dial of general population | 3 | 6 | 18 | 58.0 | 14 |
| Johnson & Paiva et al., 2008 | Dietn Phys Activityn |
1,277 | 4 tailored letters+ or assessment-only* conditions delivered at home | Proactive random digit dial calls or respondents to advertisements | 4 | 9 | 12 | 66.0 | 13 |
| Jones & Edwards, 2003 | Dietn Smokingn | 1,029 | Multiple tailored letters+ or brief physician advice* conditions delivered at home and clinic | Respondents to posters in clinics and newspapers | 12 | 12 | 12 | 77.7 | 16 |
| King & Friedman et al., 2007 | Phys Activityj | 218 | Tailored automated telephone feedback+, tailored human advice, or health education group* conditions | HMO members contacted via mail and phone | 15 | 12 | 6 | 86.7 | 18 |
| Kosma, Cardinal, & McCubbin, 2005 | Phys Activityk | 151 | 4 tailored interactive website interventions+ or assessment-only* conditions | Respondents to fliers and announcements | 4 | 1 | 1 | 49.6 | 16 |
| Kreuter & Strecher, 1996 | Dietb Phys Activityj Mammographyi Smokingg |
1,317 | Tailored letter+, behavioral feedback or assessment-only* conditions delivered at home | Proactively recruited medical clinic patients | 1 | 1 | 6 | 86.0 | 15 |
| Kreuter & Sugg-Skinner et al., 2005 | Dietc Mammographyi |
416 720 | Tailored+, culturally tailored letters, or assessment-only* conditions delivered at home | Proactively recruited medical clinic patients | 6 | 18 | 18 | 71.8 | 16 |
| Kristal, Curry, Shattuck, Feng, & Li, 2000 | Dietb,c | 1,459 | Tailored letter+manual+brief calls+ or assessment- only* conditions delivered at home | Proactively recruited HMO members | 2 | 12 | 12 | 87.0 | 18 |
| Kypri & McAnally, 2005 | Dietn Phys Activityj |
218 | Web-based assessment and feedback+ or assessment only* conditions delivered at school | Patients recruited from college health service | 1 | 1 | 2 | 86.0 | 16 |
| Lennox & Osman et al., 2001 | Smokingh | 2,553 | Tailored letter+, personalized information or assessment-only* conditions delivered at home | Patients proactively recruited from medical clinic | 1 | 1 | 6 | 78.1 | 15 |
| Lipkus, Lyna, & Rimer, 1999 | Smokingh | 266 | Tailored letter + advice + counselor call, tailored letter + brief advice+, or advice-only* conditions delivered at home and clinic | Random sample of medical clinic patients | 2 | 1 | 16 | 62.2 | 17 |
| Lipkus, Rimer, Halabi, & Strigo, 2000 | Mammographyi | 1,934 | Tailored letter+, counselor call, or reminder* delivered at home | Sample of HMO members | 1 | 12 | 12 | 96.0 | 16 |
| Lutz & Ammerman et al., 1999 | Dietc | 710 | 4 tailored letters+, nontailored letters, or assessment-only* conditions delivered at home | Proactively recruited from random sample of HMO members | 4 | 4 | 6 | 80.8 | 18 |
| Marcus & Bock et al., 1998a | Phys Activitym | 1,559 | 2 tailored letters+ or brochure conditions delivered at home | Reactively recruited employees from worksite | 2 | 1 | 3 | 73.0 | 16 |
| Marcus & Napolitano et al., 2007 | Phys Activityk | 239 | Telephone-based individualized feedback, print-based individualized feedback+, or contact control* conditions | Reactively recruited employees via newspaper and workplace advertisements | 14 | 12 | 12 | 85.4 | 17 |
| McKay & King et al., 2001 | Phys Activityk | 65 | 8-week online tailored intervention+ or internet information-only* conditions | Respondents to e-mail postings to diabetes specific UseNet groups, listserves, web sites, and on-line community groups | 5 | 2 | 2 | 87.0 | 18 |
| Meyer & Ulbricht et al., 2008 | Smokingh | 1,499 | 3 tailored letters+, brief physician advice, or assessment-only* conditions | Proactively recruited patients in primary care clinics | 3 | 6 | 18 | 61.9 | 16 |
| Napolitano & Fotheringham et al., 2003 | Phys Activityk | 65 | 12 weekly tip sheets plus 3 months of access to an interactive web-based program+ or assessment-only conditions* delivered at home | Employee respondents recruited from worksite advertisements | 12 | 3 | 3 | 80.0 | 15 |
| Nitzke & Kritsch et al., 2007 | Dietc | 2,024 | 2 tailored reports plus newsletters+ or mailed non-tailored pamphlet* conditions delivered at home | Respondents to advertisements directed at low-income persons | 4 | 6 | 12 | 62.0 | 19 |
| Oenema, Tan, & Brug, 2005 | Dietb,d,e | 782 | 2 tailored feedback sessions delivered by CD-ROM+, brochure*, or assessment-only conditions delivered at home | Proactively recruited employees from worksite | 2 | 1 | 1 | 79.0 | 15 |
| Owen, Ewins, & Lee, 1989 | Smokingg | 208 | 4 tailored letters+, brochure*, or assessment-only conditions delivered at home | Respondents to fliers/announcements | 4 | 1 | 9 | 88.0 | 13 |
| Papadaki & Scott, 2005 | Dietd,e | 72 | 4 tailored dietary and psychosocial feedbacks+ or brochure* conditions delivered via internet | Respondents to advertisements in newsletters, flyers, postings on the worksites’ Intranet and email | 4 | 6 | 6 | 80.0 | 19 |
| Patrick & Sallis et al., 2001 | Dietb,c Phys Activityk |
148 | 2 tailored feedbacks + follow up letters or calls+ or tailored feedback* only conditions delivered at clinic and home | Proactively recruited students from high schools | 2 | 4 | 4 | 79.0 | 17 |
| Peterson & Aldana, 1999 | Phys Activityk | 784 | Tailored letter+, brochure*, or assessment-only conditions delivered at worksite | Proactively recruited employees from worksite | 1 | 1 | 2 | 67.0 | 10 |
| Pinto & Friedman et al., 2002 | Phys Activityj | 298 | 6 dynamically tailored automated calls+ or assessment-only* conditions delivered at home | Proactively recruited HMO members via mail and phone | 6 | 6 | 6 | 79.8 | 18 |
| Prochaska & Sallis, 2004 | Phys Activityk | 138 | Tailored feedback provided via computer in school+ or assessment-only* conditions | Proactively recruited middle school students | 1 | 1 | 3 | 99.0 | 14 |
| Prochaska, DiClemente, Velicer, & Rossi, 1993 | Smokingf | 756 | 4 dynamically tailored letters+, dynamically tailored letters + manual + counselor call, brochure*, or manual conditions delivered at home | Respondents to fliers/announcements | 4 | 6 | 18 | 70.0 | 12 |
| Prochaska, Velicer, Fava, Rossi, & Tsoh, 2001a | Smokingg | 4,144 | 3 dynamically tailored mailed reports+ or assessment only* conditions delivered at home | Proactive random digit dial of general population | 3 | 6 | 18 | 67.0 | 15 |
| Prochaska & Velicer et al., 2001b | Smokingh | 1,447 | 3 dynamically tailored letters+, dynamically tailored letters + manual, dynamically tailored letter + manual + counselor call, or assessment-only* conditions delivered at home | Proactively recruited HMO members via mail and phone | 3 | 6 | 18 | 62.9 | 14 |
| Prochaska & Velicer et al., 2005 | Dietn Smokingf Mammographyi |
5,407 | 3 dynamically tailored letters + manual+ or assessment-only* conditions delivered at home | Proactively recruited patients from medical clinic | 3 | 12 | 12 | 75.0 | 16 |
| Prochaska & Velicer et al., 2004 | Dietn Smokingg |
2,460 | 3 dynamically tailored letters + manual+ or assessment-only* conditions delivered at home | Proactively recruited parents of participants in related student study | 3 | 12 | 12 | 70.0 | 17 |
| Rakowski & Ehrich et al., 1998 | Mammographyi | 1,864 | 2 dynamically tailored letters+, brochure, or assessment-only* conditions delivered at home | Proactively recruited HMO members from list of enrollees | 2 | 5 | 20 | 75.0 | 19 |
| Rakowski & Lipkus et al., 2003 | Mammographyi | 2,023 | Tailored letter at either 2 mos or 10+ mos post-assessment or reminder letter* delivered at home | Proactively recruited HMO members from list of enrollees | 1 | 10 | 15 | 80.0 | 18 |
| Rimer & Halabi et al., 2002 | Mammographyi | 1,287 | 2 dynamically tailored letters+, tailored letter + counselor calls, or reminder letter* delivered at home | Proactively recruited HMO members from list of enrollees | 2 | 13 | 24 | 96.0 | 17 |
| Saywell, Champion, Skinner, Menon, & Daggy, 2004 | Mammographyi | 1,390 | Tailored letter+, tailored letter + counselor calls, or assessment-only* conditions delivered at home | Proactively recruited HMO members from list of enrollees | 1 | 1 | 2 | 75.0 | 13 |
| Schumann & John et al., 2008 | Smokingg | 485 | 3 tailored letters+ or assessment-only* conditions delivered at home | Proactively recruited from hospital population survey | 3 | 6 | 24 | 71.4 | 18 |
| Shiffman, Paty, Rohay, Di Marino, & Gitchell, 2001 | Smokingh | 4,209 | Tailored print feedback + nicotine patch+, or manual + nicotine patch* conditions delivered at home | Callers to quit line asked to participate | 6 | 3 | 1 | 63.9 | 18 |
| Skinner, Strecher, & Hospers, 1994 | Mammographyi | 489 | Tailored letter+ or brochure-only* conditions delivered at home | Proactively recruited medical clinic patients | 1 | 5 | 8 | 89.0 | 12 |
| Smeets & Brug et al., 2008 | Phys Activityj | 936 | Tailored letter+ or assessment-only* conditions delivered at home | Random population-based mailing | 1 | 1 | 3 | 52.0 | 17 |
| Strecher, Kreuter, Den Boer, & Kobrin, 1994a | Smokingg | 296 | Tailored letter or brochure-only* conditions delivered at clinic | Proactively recruited medical clinic patients | 1 | 1 | 4 | 70.8 | 14 |
| Strecher, Kreuter, Den Boer, & Kobrin, 1994b | Smokingg | 1,588 | Tailored letter+ or assessment-only* conditions delivered at clinic | Proactively recruited medical clinic patients | 1 | 1 | 6 | 67.0 | 14 |
| Strecher & Marcus et al., 2005 | Smokingg | 1,978 | 4 tailored print feedbacks + nicotine patch+ or manual + nicotine patch * delivered at home | Recruited callers to cancer info line | 4 | 6 | 12 | 43.9 | 17 |
| Strecher, Shiffman, & West, 2005 | Smokingh | 3,971 | 3 tailored newsletters plus support email sent via email+ or informational website only* conditions delivered at home | People who purchased nicotine patch and logged onto to suggested website | 3 | 3 | 3 | 53.3 | 15 |
| Velicer & Friedman et al., 2006 | Smokingg | 2,054 | Tailored letter+, tailored letters + call, or manual-only* conditions in combination with patch delivered at home | Proactively contacted from VA hospital population | 1 | 1 | 30 | 61.0 | 16 |
| Velicer, Prochaska, Fava, Laforge, & Rossi, 1999 | Smokingh | 2,882 | 2, 3, or 6 dynamically tailored letters, 1 tailored letter+, or manual-only* conditions delivered at home | Proactively recruited from HMO member list | 1 | 1 | 18 | 74.0 | 17 |
= % kCalories from fat;
= Fat FFQ;
= Fruit and Vegetable Servings/Day;
= Fruit Servings/day;
= Veg Servings/day;
= 24 hr point prevalence smoking abstinence;
= 7 day point prevalence smoking abstinence;
= 28 day point prevalence smoking abstinence;
= % adherent to mammography screening;
= % adherent to CDC physical activity recommendations;
= recalled minutes of physical activity;
= % increasing physical activity;
= % making progress in stage of change for physical activity;
= % reaching action or maintenance stages.
Indicates group to which intervention was compared
Indicates treatment group outcome used for analysis
Effect size determination
We employ Hedges g as the effect size (ES) statistic. Hedges g, as defined by Borenstein et al. (2009), is a derivation of the mean difference (d) effect size that uses a pooled variance component and uses a correction factor (J) for underestimation of the population standard deviation such that
| (eq. 1) |
where
| (eq. 2) |
and
| (eq. 3) |
To combine outcomes with continuous and dichotomous formats, the odds ratio was transformed to a standardized mean difference (Lipsey and Wilson, 2001). Each effect size was weighted by its inverse variance weight in calculating mean effect sizes.
Variance modeling
Random and fixed effects estimates were calculated. A fixed effects model was employed for moderator analysis because this model increases statistical power for detecting heterogeneity; a random effects estimate assumes additional variance beyond the set of studies and facilitates generalizability of results. Variability of the variance component was tested with the Q test, the significance of which indicates that additional variance beyond that expected for the given N exists in the scores and implies the existence of moderators.
Moderator analysis
Categorical moderators were examined using a test appropriate for meta-analysis that employs weighted data and compares within and between groups heterogeneity (Lipsey and Wilson, 2001) using the Q statistic. Meta-regression was employed for analysis of continuous moderators using a necessary correction for standard errors and statistical test values (Biostat, 2006). With a sample size of 10 or more studies (the case for most comparisons in the present study), statistical power for detecting differences between groups was sufficient.
Sources of bias
If insufficient information was reported for effect size calculation, the study was excluded, but if the study indicated that the effect was simply “nonsignificant” it was included with the effect size entered as zero (which was needed only for one outcome). Mean effects were assessed for degree of publication bias using two techniques: Orwin’s fail safe N and trim and fill. Orwin’s fail-safe N calculates the number of studies with a null effect size needed to reduce the overall effect to clinical nonsignificance. Clinical significance was set to g = 0.10 (OR = 1.18), which would represent a difference in success rates about five percentage points higher in the treatment vs. control group, a minimum assumed to be a meaningful effect in population-based interventions (Rossi, 2003). Trim and fill is a technique developed by Duval and Tweedie (2000) that assesses the symmetry of a plot of effect size by sample size (funnel plot) under the assumption that when publication bias exists, a disproportionate number of studies will fall to the bottom right of the plot. This technique determines the number of asymmetrical outcomes, imputes their counterparts to the left, and estimates a corrected mean effect size.
Coding and reliability
The primary author and trained master’s level graduate student conducted the initial literature search and independently selected studies for inclusion. A coding manual was developed based on a prior meta-analysis of health behavior interventions (Hall and Rossi, 2008). To ensure data quality, a random subset of half the studies were coded by a trained masters-level graduate student and discrepancies resolved. In addition, the primary author coded all studies twice as a further check. Studies were assessed for quality using a 22-point coding scheme based on the CONSORT (Boutron, et al., 2008) and QUOROM guidelines (Moher, et al., 1999) (see Table 5). The primary database was created using the Comprehensive Meta-Analysis software package (Biostat, 2006).
Table 5.
Study Quality Rating Criteria
| Topic | Item | Descriptor |
|---|---|---|
| Introduction | 1 | Provides scientific background and explanation of rationale. |
| Methods Participants | 2 |
|
| Interventions | 3 |
|
| Objectives | 4 | Is the hypothesis/objective of the study clearly described? |
| Outcomes | 5 | Are the main and secondary outcomes clearly defined? |
| Measures | 6 | Was actual data or reference provided on reliability and validity of outcome measures? |
| Sample size & power | 7 | Description of systematic methods to determine sample size – specifically, mention that power analysis was done in study planning. |
| Randomization | 8 | Were study participants randomized to intervention/control groups? |
| Implementation | 9 | Reporting of who enrolled participants and assigned them to groups? |
| Statistical methods | 10 | Were statistical methods used for main outcomes reported (e.g. ANOVA) and appropriate? |
| Adjustments | 11 | Was there adequate adjustment for confounding in the analyses or mention of moderator analyses including clustering by provider when appropriate? |
| Results Participant flow | 12 | For each group report the numbers randomly assigned, receiving intended treatmnet, completing the study, and analyzed for the primary outcomes. |
| Recruitment | 13 | Specifies dates of recruitment and follow-up. |
| Baseline data | 14 | Baseline demographic and clinical characteristics of each group (age, gender, race) along with difference analysis on outcome variables based on potential moderators. |
| Numbers reported | 15 |
|
| Outcomes and estimation | 16 | For all results, a summary of results including
|
| Ancillary analysis | 17 | Were any results based on data mining or comparisons that were not planned? |
| Adverse events | 18 | Have all important adverse events that may be a consequence of intervention been reported? Should be answered yes if study mentions intent to measure such events. |
| Discussion | 19 | Interpretation of results taking into account study hypotheses, sources of potential bias or imprecision and the dangers associated with multiplicity of analyses or outcomes. |
| External validity | 20 | Generalizability of the findings – mention as to what extent were subjects and intervention representative of populations to which this intervention may be used. |
| Overall evidence | 21 | General interpretation of the results in the context of current evidence. |
| Funding | 22 | Acknowledgment of funding source/sponsorship or conflicts of interest. |
Results
Search Results
The initial search retrieved 1,724 references. Of 173 potential studies that described an intervention, 85 were excluded (see Table 6). Of 13 unique behaviors intervened upon, only four were represented by a sufficient numbers of studies (at least 10) to include for analysis. These were smoking cessation (k = 32), dietary fat reduction (k = 26), increasing fruit and vegetable intake (k = 25) physical activity (k = 25), and mammography screening (k = 12). In sum, 88 unique studies and effect sizes were used to compute the overall effect size with 119 effect sizes in total included for behavior-specific analyses representing 106,243 participants (see Table 4).
Table 6.
Studies Excluded from Analysis
| Behavior | Citation | Exclusion Criteria |
|---|---|---|
| Diet | Blalock, DeVellis, & Patterson et al., 20021 | Insufficient data reported |
| Diet | Brinberg & Axelson, 19902 | Counselor based |
| Diet | Brinberg, Axelson, & Price, 20003 | Counselor based |
| Diet | Brug & van Assema, 20004 | Results reported in Brug et al, 1998 |
| Diet | Brug, Glanz, & Kok, 19975 | No intervention provided |
| Diet | De Bourdeaudhuij, Brug, Vandelanotte, & Van Oost, 20026 | Randomization and analysis according to family, not individual |
| Diet | de Vet, de Nooijer, de Vries, & Brug, 20087 | No control group |
| Diet | Esters, Boeckner, & Hubert et al., 2008 8 | No behavioral outcomes reported |
| Diet | Glanz, Murphy, & Moylan, et al., 20069 | No control group |
| Diet | Glasgow, Toobert, Hampson, & Strycker, 200210 | Counselor based |
| Diet | Gould & Anderson, 200211 | No control group |
| Diet | Jantz, Anderson, & Gould, 200212 | No behavioral outcomes reported |
| Diet | King, Estabrooks, & Strycker et al., 200613 | Counselor based |
| Diet | Oenema & Brug, 200314 | No behavioral outcomes reported |
| Diet | Oenema, Brug, & Lechner, 200115 | No behavioral outcomes reported |
| Diet | Sorensen, Thompson, & Glanz et al., 199616 | Community intervention, no tailored component |
| Diet | Stevens, Glasgow, & Toobert et al., 200217 | Counselor based |
| Diet | Stevens, Glasgow, & Toobert et al., 200318 | Counselor based |
| Diet | Veverka, Anderson, & Auld et al., 200319 | No behavioral outcomes reported |
| Diet | Winett, Wagner, & Moore et al., 199120 | Not theoretically tailored |
| Diet | Kreuter, Bull, Clark, & Oswald, 199921 | No behavioral outcomes reported |
| Diet | Tate, Wing, & Winett, 200122 | Employed manually tailored intervention |
| Diet | Tate, Jackvony, & Wing, 200323 | Employed manually tailored intervention |
| Diet Phys Activity | Glasgow, Boles, & McKay et al., 200324 | Counselor based |
| Diet Phys Activity | Clark, Hampson, Avery, & Simpson, 200425 | Counselor based |
| Diet Phys Activity | Booth, Nowson & Matters, 200826 | No control group |
| Diet Phys Activity | Plotnikoff, McCargar, & Wilson et al., 200527 | Not tailored |
| Diet Phys Activity | Vandelanotte, Reeves, & Brug et al., 200828 | Results reported in Vandelanotte et al., 2005 study |
| Diet Phys Activity | Vandelanotte, De Bourdeaudhuij, & Sallis et al., 200529 | Insufficient data reported |
| Mammography | Allen & Bazargan-Hejazi, 200530 | Counselor based |
| Mammography | Champion, Maraj, & Hui et al., 200331 | Counselor based |
| Mammography | Gustafson, McTavish, & Stengle et al., 200532 | No tailored feedback provided |
| Mammography | Jibaja-Weiss, Volk, & Kingery et al., 200333 | Not theoretically tailored |
| Mammography | McCaul & Wold, 200234 | Employed manually tailored intervention |
| Mammography | Meldrum, Turnbull, & Dobson et al., 199435 | Targeted intervention, not theoretically tailored |
| Mammography | Rimer, Halabi, & Skinner et al., 200136 | Reported in Rimer et al., 2002 |
| Mammography | Stoddard, Fox, & Costanza et al., 200237 | Counselor based |
| Mammography | Williams-Piehota, Pizarro, & Schneider, et al., 200538 | Lacked sufficient control group |
| Mammography | Ryan, Skinner, & Farrell et al., 200139 | No intervention provided |
| Phys Activity | Brownson, Hagood, & Lovegreen et al., 200540 | Results confounded with multilevel community intervention |
| Phys Activity | Castro, King, & Brassington, 200141 | Focused on maintenance |
| Phys Activity | Demark-Wahnefried, Clipp, & McBride et al., 200342 | Results reported in Demark et al., 2007 |
| Phys Activity | Hurling, Fairley, & Dias, 200643 | Insufficient data reported |
| Phys Activity | Jacobs, Ammerman, & Ennett et al., 200444 | Examined maintenance only |
| Phys Activity | Marshall, Leslie, & Bauman et al., 200345 | No control group |
| Phys Activity | Marcus, Emmons, Simkin-Silverman et al., 199846 | Results reported in Bock et al., 2001 |
| Phys Activity | Marcus, Lewis, & Williams et al., 200747 | Results not reported |
| Phys Activity | Purath, Miller, & McCabe et al., 200448 | Counselor based |
| Phys Activity | Van Sluijs, Van Poppel, & Twisk et al., 200549 | Counselor based |
| Smoking | Burling, Marotta, & González et al., 198950 | Not behaviorally tailored |
| Smoking | Carpenter, Watson, & Raffety et al., 200351 | Intervention focused on provider training |
| Smoking | Chouinard & Robichaud-Ekstrand, 200552 | Counselor based |
| Smoking | Cobb, Graham, & Bock et al., 200553 | No control group |
| Smoking | Gilbert, Nazareth, & Sutton et al., 2008 54 | Results not reported |
| Smoking | Klesges, DeBon, & Vander et al., 200655 | Counselor based |
| Smoking | Lenert, Munoz, & Perez et al., 200456 | No control group. Non-randomized design |
| Smoking | Levinson, Glasgow, & Gaglio et al., 200857 | No behavioral outcomes reported |
| Smoking | Orleans, Boyd, & Bingler et al., 199858 | Counselor based |
| Smoking | Pallonen, Veliver, & Prochaska et al., 199859 | No control group |
| Smoking | Rimer, Orleans, & Fleisher et al., 199460 | Counselor based |
| Smoking | Shegog, McAlister, & Hu et al., 200561 | No behavioral outcomes reported |
| Smoking | Shiffman, Rolf, Hellesbush et al., 200262 | No tailored intervention |
| Smoking | Stoddard, Delucchi, & Munoz et al., 200563 | No control group |
| Smoking | Wang & Etter, 200464 | No control group |
| Smoking | Webb, Simmons, & Brandon, 200565 | No behavioral outcomes reported |
| Smoking | Wiggers, Oort, & Dijsktra et al., 200566 | No behavioral outcomes reported |
| Smoking | Velicer & Prochaska 199967 | No behavioral outcomes reported |
| Alcohol Use | Butler, Chiauzzi, & Bromberg et al., 200368 | Insufficient number of same behavior for comparison |
| Alcohol Use | Kypri, Saunders, & Williams et al., 200469 | Insufficient number of same behavior for comparison |
| Injury Prevention | McDonald, Solomon, & Shields et al., 200570 | Insufficient number of same behavior for comparison |
| Injury Prevention | Nansel, Weaver, & Donlin et al., 200271 | Insufficient number of same behavior for comparison |
| Organ Donation | Reubsaet, Brug, & Kitslaar et al., 200472 | Insufficient number of same behavior for comparison |
| Pain | Nicholson, Nash, & Andrasik, 200573 | Insufficient number of same behavior for comparison |
| Pain | Wilkie, Huang, & Berry et al., 200174 | No intervention provided |
| Risk Perception | Kreuter & Strecher, 199575 | Insufficient number of same behavior for comparison |
| Risk Perception | Emmons, Wong, & Puleo et al., 200476 | Insufficient number of same behavior for comparison |
| Cancer screening | Kreuter, Skinner, & Steger-May et al., 200477 | Behavior change not reported |
| Cancer screening | Marcus, Mason, & Wolfe et al., 200578 | Insufficient number of same behavior for comparison |
| Cancer screening | de Nooijer, Lechner, & de Vries, 200279 | Behavior change not reported |
| Sexual Risk Prevention | Bellis, Grimley, & Alexander, 200280 | No intervention provided |
| Sexual Risk Prevention | Chesney, Koblin, & Barresi et al., 200381 | Baseline data only |
| Sexual Risk Prevention | Scholes, McBride, & Grothaus et al., 200382 | Insufficient number of same behavior for comparison |
| Stress reduction | Evers, Prochaska & Johnson et al., 200683 | Insufficient number of same behavior for comparison |
| Sun Protection | Bernhardt, 200184 | Insufficient number of same behavior for comparison |
| Sun Protection | Hornung, Lennon, & Garrett et al., 200085 | Insufficient number of same behavior for comparison |
Table 1 summarizes study attributes. Most studies used a proactive (vs. reactive) recruitment strategy that individually reached out to participants (70.4%), and of those, 33.0% used random sampling to identify the study population. Interventions were mainly delivered at home (81.8%), using print (75.0%) and computer (21.6%) communication channels. Medical institutions (38.6%), printed advertisements (such as in newspapers) (17.1%), and worksites (12.5%) were the most popular recruitment approaches. The majority of studies were conducted in the United States (72.7%), with 21.6% in Europe and the rest in Australia and New Zealand. Studies were characterized by moderate to high recruitment (61.4%, range = 9.1–98.0%) and retention rates (74.4%, range = 33.0–99.0). The average age of participants was 41.8 years (range = 12.1–74.9) and 69.4% were female (range = 17.0–100.0%). Studies recruited an average 23.2% of participants who identified as other than White with 10% being the median percentage of non-White participants.
Table 1.
Study Attributes (Studies published 1988-2009)
| Attribute | k | % |
|---|---|---|
| Recruitment Strategy | ||
| Proactive | 62 | 70.4 |
| Reactive | 26 | 29.6 |
| Random Sampling | 29 | 33.0 |
| Delivery Site | ||
| Home | 72 | 81.8 |
| Home + Clinic | 1 | 1.1 |
| Clinic | 6 | 6.8 |
| Store | 1 | 1.1 |
| School | 4 | 4.7 |
| University Lab | 1 | 1.1 |
| Worksite | 2 | 2.3 |
| Community Center | 1 | 1.1 |
| Intervention Method | ||
| Computer | 19 | 21.6 |
| 66 | 75.0 | |
| Automated Phone | 3 | 3.4 |
| Recruitment Strategy | ||
| Medical Clinic | 18 | 20.4 |
| HMO insurer lists | 16 | 18.2 |
| General Advertisements | 15 | 17.1 |
| Worksite | 11 | 12.5 |
| Random Dial or Mailing | 8 | 9.1 |
| School | 8 | 9.1 |
| Call in Center | 6 | 6.8 |
| Community Center | 3 | 3.4 |
| Church | 2 | 2.3 |
| Website | 1 | 1.1 |
| Country | ||
| United States | 64 | 72.7 |
| Europe | 19 | 21.6 |
| Australia | 4 | 4.6 |
| New Zealand | 1 | 1.1 |
| Behaviors Intervened Upon | ||
| One | 65 | 73.9 |
| Two | 16 | 18.2 |
| Three | 6 | 6.8 |
| Four | 1 | 1.1 |
| Mean (SD) | Median | |
| Recruitment Rate (%) | 61.4 (23.1) | 68.0 |
| Retention Rate (%) | 74.4 (14.7) | 75.0 |
| Mean Age | 41.8 (12.0) | 41.1 |
| % Female | 69.4 (20.4) | 67.3 |
| % Minority | 23.2 (30.5) | 10.0 |
Overall Mean Effect Size
The overall effect size for the 88 tailored interventions was g = 0.17 (95% CI = 0.14-0.19) using a fixed effects model and g = 0.17 using a random effects model (95% CI = 0.14-0.20). Orwin’s fail safe N revealed that an additional 58 studies with null effects would be needed to reduce the overall effect size to a clinically nonsignificant outcome (g = 0.10). Trim and fill analysis for publication bias imputed eleven studies to the left of the mean, which would minimally reduce the fixed effect estimate to g = 0.15 (95% CI = 0.13-0.17) (see Table 2).
Table 2.
Effect Sizes and Moderator Analyses (Studies published 1988-2009)
| Moderator | k | g | 95% CI | p |
|---|---|---|---|---|
| Mean Effect Size | ||||
| Fixed | 88 | 0.17 | 0.14-0.19 | < .001* |
| Random | 88 | 0.17 | 0.14-0.20 | < .001* |
| Homogeneity | Q (87) = 148.8, p < 0.001 | |||
| Health Behavior | ||||
| Smoking Cessation | 32 | 0.16 | 0.12-0.19 | < .001* |
| Dietary Fat Reduction | 26 | 0.22 | 0.18-0.26 | < .001* |
| Fruit/Veg | 25 | 0.16 | 0.10-0.21 | < .001* |
| Mammography | 12 | 0.13 | 0.08-0.18 | < .001* |
| Physical Activity | 25 | 0.16 | 0.10-0.21 | < .001* |
| Tailoring Method | ||||
| Static | 51 | 0.14 | 0.11-0.16 | .01 |
| Dynamic | 37 | 0.19 | 0.16-0.21 | |
| Number of contacts (static tailoring only) | ||||
| 1 | 34 | 0.13 | 0.09-0.17 | .02 |
| 1+ | 18 | 0.20 | 0.15-0.24 | |
| Recruitment Strategy | ||||
| Reactive | 26 | 0.17 | 0.13-0.21 | .85 |
| Proactive | 62 | 0.18 | 0.16-0.20 | |
| Communication Channel | ||||
| Computer | 19 | 0.16 | 0.12-0.21 | .89 |
| 66 | 0.17 | 0.14-0.19 | ||
| Automated Phone | 3 | 0.21 | 0.01-0.42 | |
| Longitudinal Effects | ||||
| 1-3 months | 27 | 0.18 | 0.14-0.21 | .04+ |
| 4-6 months | 16 | 0.20 | 0.13-0.27 | |
| 7-12 months | 25 | 0.19 | 0.16-0.23 | |
| 13-24+ months | 19 | 0.12 | 0.08-0.16 | |
| Engagement in Behavior at Baseline | ||||
| No | 49 | 0.18 | 0.15-0.22 | .10 |
| Yes | 39 | 0.15 | 0.13-0.18 | |
| Comparison Group | ||||
| Assessment Only | 39 | 0.18 | 0.15-0.21 | .19 |
| Minimal Intervention | 49 | 0.15 | 0.12-0.18 | |
| Country | ||||
| U.S. | 64 | 0.18 | 0.15-0.20 | .12 |
| Non-U.S. | 24 | 0.14 | 0.10-0.18 | |
| Number of Behaviors Intervened Upon | ||||
| 1 | 65 | 0.15 | 0.13-0.17 | .01 |
| 2 | 16 | 0.21 | 0.16-0.26 | |
| 3 | 6 | 0.24 | 0.18-0.31 | |
| 4 | 1 | 0.12 | -0.04-0.29 | |
| Demographics | B | p | ||
| Mean Age | -0.01 | .84 | ||
| % Female (excluding mammography) | -0.06 | .27 | ||
| % Minority | 0.03 | .35 | ||
| Study Quality | 0.01 | .07 | ||
| Retention Rate | 0.06 | .33 | ||
| Publication Bias | ||||
| Orwin’s Fail Safe N | 58 | |||
| Trim and Fill | 11 imputed to left of mean, g = 0.15 (0.13-0.17) | |||
Indicates significance of mean effect size
Final outcome with each study was included once to ensure independence of observations
Effect Sizes by Behavior
Dietary Improvement
For dietary improvement behaviors, 26 studies reported dietary fat outcomes and 25 reported fruit and vegetable intake outcomes (see Table 4), which were analyzed separately. For dietary fat intake, the continuous variable of mean fat intake score was the preferred outcome (16 studies). Percent calories from fat (5 studies) and percent reaching Action or Maintenance stages (representing less than 30% of calories from fat) for fat reduction (5 studies) were used alternatively when fat intake scores were not reported (see Table 4). The mean effect size for dietary fat reduction was g = 0.22 (95% CI = 0.18-0.26), p < .001 (see Table 2).
Twenty-five studies assessed fruit and vegetable intake and reported results using three variables: a combined fruit/vegetable outcome (18 studies), separate fruit and vegetable outcomes (5 studies), and percent reaching Action or Maintenance stages for eating 5 fruits and vegetables (2 studies) (see Table 4). The combined measure was the preferred outcome and the mean of both outcomes was taken when fruit and vegetable consumption were reported separately. The mean effect size was g = 0.16 (95% CI = 0.10-0.21, p < .001) (see Table 2).
Physical Activity Promotion
The 25 studies focused on increasing levels of physical activity and reported a variety of outcomes, which were chosen in decreasing order of clinical importance: percent of participants reaching CDC physical activity criteria (10 studies), seven-day physical activity recall (11 studies), and percent increasing physical activity (4 studies) (see Table 4). The mean effect size was g = 0.16 (95% CI = 0.10-0.21, p < .001) (see Table 2).
Smoking Cessation
Studies reported smoking abstinence using various outcome measures including 24-hour, 7-day, 28-day, 10-week, 6-month, and 9-month point prevalence. Since 24-hour, 7-day, and 30-day point prevalence abstinence measures are highly correlated (Velicer and Prochaska, 2004) these outcomes were analyzed together to increase the number of included studies. Where studies reported more than one of these measures, 28-day abstinence was preferred (9 studies), followed by 7-day point prevalence (19 studies), and then by 24-hour point prevalence (4 studies) (Hughes, et al., 2003) (see Table 4). The mean effect for the 32 studies reporting point prevalence outcome was g = 0.16 (95% CI = 0.12-0.19, p < .001). Nine-month, six-month and 10-week sustained abstinence outcomes were analyzed separately to preserve similarly of measurement. Nevertheless, we calculated the mean effect for the 16 studies reporting prolonged abstinence measures and found a significant mean effect where g = 0.24 (95% CI = 0.20-0.31, p < .001).
Mammography Screening
Twelve studies reported the percentage of participants adherent to mammography recommendations. The mean effect size was g = 0.13 (95% CI = 0.08-0.18, p < .001).
Longitudinal Outcomes
Examination of effect size over time provides an important estimate of behavioral maintenance associated with tailored interventions. As shown in Table 2 and Figure 1, effects peak from 4-12 months post baseline with a mean effect size of g = 0.20, and while they decline after 12 months post-baseline, the mean ES at long-term follow-up (g = 0.12) remains statistically significant (95% CI = 0.08-0.16). To control for length of intervention, months since intervention completion were regressed on ES. A significant negative trend of decreasing effect size (B = -0.006, p = .001) was found, suggesting that after a year the average effect for computer-tailored interventions would decrease by an average of g = 0.07.
Figure 1.

Trends in effect size over outcome time point
Moderator Analysis
Intervention characteristics
Number of intervention contacts was related to effect size (B = 0.01, p < .001) such that mean effect size increased by an average of g = 0.01 for every additional contact. Dynamic tailoring (i.e. iterative assessments and feedback) was associated with larger mean effect sizes (g = 0.19) than static tailoring (g = 0.14) p = .01 (see Table 2). Since some studies provided static feedback based on one baseline assessment at more than one time point, differences in mean effect size between numbers of contacts (1 vs. more than 1) of statically tailored materials was also assessed. Inclusion of more than one statically tailored communication was associated with larger effect sizes than use of only one contact (g = 0.20 vs. 0.13, p = .02). Interestingly, longitudinal examination of effect size trends for dynamic versus static tailoring (inclusive of multiple contacts) reveals a trend indicating that dynamic tailoring results in higher effects in three of four time point categories (see Figure 2 and Table 3). While effects for all interventions decrease over time, only the effect size for dynamic tailoring remains statistically significant at long-term follow-up past 12 months (g = 0.14), even though the time from final intervention to assessment was longer for dynamically tailored studies (5.3 months) versus statically-tailored studies (3.5 months).
Figure 2.
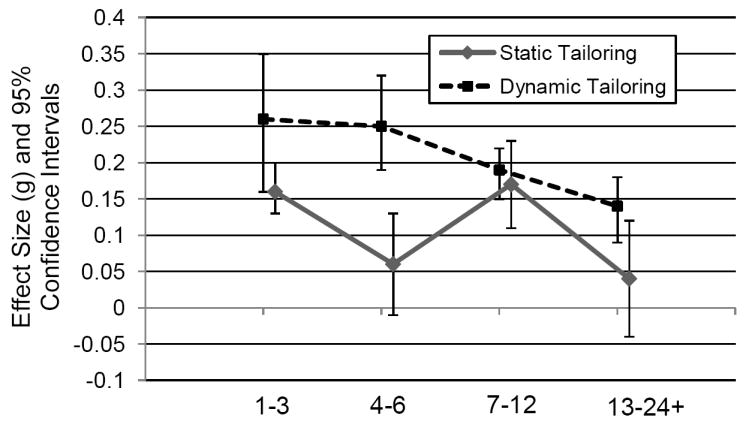
Trends in effect size over outcome time point by tailoring method
Table 3.
Comparison of Effect Sizes for Static and Dynamic Tailoring Method by Outcome Time Point (Studies published 1988-2009)
| Time Point | Static |
Dynamic |
p-value* | ||||
|---|---|---|---|---|---|---|---|
| k | g | 95% CI | k | g | 95% CI | ||
| 1-3 months | 30 | 0.16 | 0.13-0.20 | 9 | 0.26 | 0.16-0.35 | .05 |
| 4-6 months | 14 | 0.06 | -0.01-0.13 | 17 | 0.25 | 0.19-0.32 | < .001 |
| 7-12 months | 13 | 0.17 | 0.11-0.23 | 23 | 0.19 | 0.15-0.22 | .61 |
| 13-24 months | 7 | 0.04 | -0.04-0.12 | 14 | 0.14 | 0.09-0.18 | .03 |
Mean intervention length was 4.5 months (range = 0-18).
If studies reported outcomes at more than one time point, they were entered once into each category. Comparisons between static and dynamic methods are thus independent within time point category.
In terms of communication channel (i.e. print, computer, telephone, etc), effect sizes ranged from 0.16-0.21 with no significant difference noted (p = .89). A trend was found for increasing effect sizes across studies that intervened on one (g = 0.15), two (g = 0.21), and three (g = 0.24) behaviors, but this trend did not continue with the one study at intervened on four behaviors (g = 0.12).
Recruitment Strategies
No differences were found between studies employing proactive (g = 0.18) and reactive (g = 0.17) recruitment strategies (p = .85). A nonsignificant trend (p = .10) was found favoring studies that recruited participants who were currently not engaging in a particular behavior (g = 0.18) versus studies that did not screen out participants who may be already engaging in the behavior (g = 0.15).
Demographic Moderators
Studies conducted in the U.S. (g = 0.18) did not differ from those based in other countries (g = 0.14), p = .12. When regressed on mean effect size, no significant relationships were found by age, proportion of non-White participants, and gender after controlling for the relationship between gender and behavior by excluding mammography studies (see Table 2).
Study Quality and Design
Study quality (B = 0.01, p = .07) and retention rate (B = 0.06, p = .33) were not related to mean effect size (see Table 2). Overall, 49 studies compared a tailored intervention to a minimal intervention and 39 compared tailoring to an assessment-only group, but effect sizes between study designs did not differ significantly (g = 0.18 vs. g = 0.15, p = .20).
Discussion
This study computed a mean effect size for 88 studies that provided computer-tailored feedback based on individual assessments using computer, print, or telephone communication channels. We also examined moderators that were hypothesized to influence the effects of tailored interventions. A significant effect size (g = 0.17) was found for tailored interventions averaged across four health behaviors. The overall effect for tailored interventions represents a small to medium-size effect for population-based interventions (Rossi, 2003) (where g = 0.15, 0.20, and 0.25 for small, medium and large effects) and a 36% increase (OR = 1.36) over the control conditions to which the interventions were compared. In addition, significant effects were found for each of the behaviors examined individually. It appears that systematic differences in tailoring methods is an unlikely explanation for the range of effect sizes across behaviors since the same research groups conducted interventions for each behavior and many tailoring techniques were shared across groups. Other possibilities are base rates and differences in the nature of the behaviors. Population rates of mammography (the lowest effect size reported) are the highest (>66%) compared to the other behaviors, which may produce a ceiling effect. Each behavior also presents a unique set of barriers to adherence and it is difficult to make conclusions regarding the relative difficulty of changing distinct behaviors.
These data show that computer-tailored interventions would have clinically significant impact on rates of behavioral risk factors. First, in terms of smoking cessation, the average point prevalence abstinence was 20% at final follow-up versus 14% in the comparison group, a clinically significant absolute increase of 6% in quit rates, and a rate comparable to that observed with 4-8 individual in-person counseling sessions (Fiore, 2008). Second, for physical activity, 43% of participants receiving computer-tailored communications were adherent to physical activity recommendations (World Health Organization, 2002) at follow-up versus only 34% in the comparison groups. With up to 40% of people in industrialized countries not engaging in any regular physical activity (Bauman, et al., 2009), increasing rates of physical activity by the rate produced by these interventions would have an important impact on health outcomes. Third, since an estimated 27% of people eat five or more fruits or vegetables per day (Centers for Disease Control and Prevention, 2007), increasing this rate by the effect size found in this study for fruit and vegetable intake (OR = 1.36) would increase the absolute rate of fruit and vegetable consumption to 37%, a meaningful change that is highly recommended to prevent and control obesity and multiple chronic diseases (Centers for Disease Control and Prevention, 2009). Finally, for receipt of least bi-annual mammography screening, computer-tailored interventions resulted in 56% adherence versus 50% in control groups, an important difference given that a secular trend reflecting a reduction of 4% in mammography screening rates existed during the period in which most of these studies were conducted (Breen, et al., 2007).
In terms of moderators of effect size, dynamically-tailored interventions outperformed statically-tailored interventions, especially upon examination of longitudinal effects. The larger effect size for dynamically tailored interventions could be explained by increased number of overall contacts that dynamic tailoring necessitates, and indeed static tailoring with more than one contact showed similar effects (g = .20) compared to dynamic tailoring (g = .19). When examined longitudinally, however, greater intervention effects for dynamic tailoring as compared to static tailoring with multiple contacts were seen in three of four outcome time point categories (1-3, 4-6, and 13-24 months) and only dynamic tailoring remained significant at long-term follow up, an important finding in terms of intervention maintenance. These results suggest that more than just providing additional contact, updating feedback to reflect a person’s changes may increase information relevance and depth of processing (Petty and Elster, 1981). The addition of systematic qualitative data as a complement to studies of dynamically tailored interventions would help to clarify the processes involved in this observed effect.
No significant differences were found by communication channel (print, computer, or automated phone). While conclusions cannot be drawn regarding automated phone intervention delivery with only three studies, the lack of difference between print and computer terminal-based feedback channels suggests that both channels can be effective means of health communication.
It also appears that intervening on up to three multiple behaviors at the same time does not negatively impact behavioral outcomes, with suggestion of a trend for larger effects as number of behaviors increased from one to three. Individual studies also support the feasibility of multiple behavior interventions (Vandelanotte, et al., 2008). The effectiveness of multiple behavior change could reflect an underlying general health orientation that influences engagement in behaviors (Noar, et al., 2008, Prochaska, et al., 2008). Common change patterns have also been found across behaviors for both decisional balance (Hall and Rossi, 2008) and self-efficacy (Grembowski, et al., 1993) constructs, suggesting that similar principles can be applied to changing distinct behaviors.
In terms of study design characteristics, a nominally significant (p = .10) trend was found suggesting that including only participants not engaging in a behavior may mitigate intervention effects. It was also predicted that reactive recruitment would result in larger effect sizes under the assumption that participants responding to ads and actively volunteering would be more ready to change. This hypothesis was not upheld, possibly because studies using reactive strategies made efforts to recruit people who were less ready to change (Hageman, et al., 2005, Prochaska, et al., 1993). Results did not favor non-U.S based studies as previously found by Noar. Whereas their sample of studies conducted outside the U.S. used shorter follow up time points, which likely explained this difference, our samples were similar in that non-U.S. studies followed up at 8.9 months on average and U.S. studies did so at 9.3 months. Study quality was also not related to effect size, which may be due to restricted range for the measure given a standard deviation of 1.6 on the 22-point scale. Differences in effect size were not found for mean age, percentage of minority participants, or gender likely attributable to efforts in most studies to randomize by demographic characteristics.
Study Strengths and Limitations
This study has a number of strengths that enhance its contribution to the study of computer-tailored interventions. First, it is the most representative and current review of studies that employed computer tailoring. We included studies using three different communication channels and searched multiple databases drawing from over 20 years of research. While publication bias has been cited as a problem in meta-analysis, it is likely minimal given that almost all intervention studies were large-scale funded projects. The fail-safe N suggests that a large number of studies would be needed to lower the average effect size to clinical nonsignificance. Second, this study distinguishes tailoring methodology from communication channels as has not been done previously. Third, we employed well-established meta-analytic techniques for effect size estimation and moderator analysis. Finally, we conducted novel moderator analyses not covered in previous reviews, examining effect sizes across outcome time points, intervention channels, multiple behaviors, design characteristics, and study quality.
On the other hand, methodological considerations necessarily limit the conclusions able to be drawn from the present work. First, given that effects decrease after intervention completion, using the final assessment from each study may underestimate the potential of tailored-interventions. If participant contact can be maintained, intervention effects may be higher than found here. Second, this study reported primary analyses of computer-tailored interventions and more work is needed to examine the relationship between effect size and additional intervention variables. We are currently preparing an analysis that focuses on the utility of tailoring options such as tailoring using specific constructs, use of theory, depth of tailoring, cultural tailoring, etc. (Rimer and Kreuter, 2006).
Conclusion
The current analysis of computer tailoring indicates that this intervention technique can be effective for supporting health-related changes across a number of behaviors linked to chronic diseases. Dynamic tailoring using iterative assessment and feedback is an important intervention strategy, and print, telephone, and computer-based communication channels are all effective for delivering intervention content. In addition, results demonstrate that multiple behaviors can be targeted simultaneously without hindering intervention effectiveness.
This study also highlights areas for improvement with regard to intervention design as well as study reporting. Regardless of tailoring method, intervention effects overall were found to decline after intervention completion, suggesting the need for innovative techniques to help participants maintain changes. In addition, while these programs produce clinically significant effects, little data is available as to whether the interventions themselves are being sustained, as would be necessary to decrease disease burden among populations. Further work needs to analyze their cost-effectiveness and possibly investigate methods for integrating these methods into clinical care systems in ways that they will be maintained over time and available to the populations that would most benefit from them (Stellefson, et al., 2008). In addition, few studies sufficiently reported methods for how assessments and feedback were integrated and no study examined or even mentioned graphic/visual and human factors design issues, which may be important moderators of effect in these communication modalities.
This study demonstrates that computer-tailored interventions have the potential to impact health behaviors to a meaningful extent and suggests strategies that may lead to greater effectiveness of these techniques. Further work is needed to improve intervention maintenance and to define specific mechanisms, such as content and depth of tailoring, that promote optimal effectiveness of computer-tailored interventions.
Supplementary Material
Acknowledgments
This research was supported by grant T32CA009461-25 from the National Cancer Institute. We thank Syncia Sabain for her assistance with review and coding of articles and Dr. Jamie Ostroff for valuable comments on earlier versions of this manuscript.
Footnotes
Conflict of Interest Statement James O. Prochaska is founder of and consultant to ProChange Behavior Systems, Inc., which develops and disseminates tailored interventions.
Preliminary findings were presented as a podium presentation at the Society of Behavioral Medicine Annual Conference, in Montreal, Canada, April 22-25, 2009.
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- Bauman A, Bull F, Chey T, Craig CL, Ainsworth BE, Sallis JF, Bowles HR, Hagstromer M, Sjostrom M, Pratt M, Díaz CG, Bazan N, Kunic H, Merom D, Smith B, De Bourdeaudhuij I, Lefevre J, Philippaerts R, Matsudo SM, Matsudo VR, Cameron C, Yang L, Hua F, Gómez LF, Fromel K, Mitas J, Macfarlane D, Bacon-Shone J, Reddy SK, Joshi P, Goenka S, Prabhakaran D, Katsumura T, Murase N, Volbekiene V, Baubliene R, McLean G, Carr H, Tomten H, Anderssen SA, Sardinha L, Mota J, Al-Hazzaa HM, Serra Majem L, Roman B, Sjöström M, Hagströmer M, Bergman P, Yiing ML, Yung-Tai H, Hipp D. The international prevalence study on physical activity: Results from 20 countries. Int J Behav Nutr Phys Act. 2009;6 doi: 10.1186/1479-5868-6-21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Biostat. Comprehensive meta-analysis. Englewood, NJ: 2006. [Google Scholar]
- Borenstein M, Hedges L, Higgins J, Rothstein H. Introduction to meta-analysis. Wiley; Chichester, UK: 2009. [Google Scholar]
- Boutron I, Moher D, Altman DG, Schulz KF, Ravaud P. Extending the consort statement to randomized trials of nonpharmacologic treatment: Explanation and elaboration. Ann Intern Med. 2008;148:295–309. doi: 10.7326/0003-4819-148-4-200802190-00008. [DOI] [PubMed] [Google Scholar]
- Breen N, Cronin KA, Meissner HI, Taplin SH, Tangka FK, Tiro JA, McNeel TS. Reported drop in mammography: Is this cause for concern? Cancer. 2007;109:2405–2409. doi: 10.1002/cncr.22723. [DOI] [PubMed] [Google Scholar]
- Brug J, Campbell M, van Assema P. The application and impact of computer-generated personalized nutrition education: A review of the literature. Patient Educ Couns. 1999;36:145–156. doi: 10.1016/s0738-3991(98)00131-1. [DOI] [PubMed] [Google Scholar]
- Centers for Disease Control. Chronic disease prevention and health promotion. CDC; Atlanta, GA: 2008. [Google Scholar]
- Centers for Disease Control and Prevention. Fruit and vegetable consumption among adults --- united states, 2005. MMWR. 2007;56:213–217. [PubMed] [Google Scholar]
- Centers for Disease Control and Prevention. Overweight and obesity 2009 [Google Scholar]
- Duval S, Tweedie R. Trim and fill: A simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics. 2000;56:455–463. doi: 10.1111/j.0006-341x.2000.00455.x. [DOI] [PubMed] [Google Scholar]
- Fiore M, Jaen CR, Baker TB, et al. Treating tobacco use and dependence: 2008 update. In: Fiore MC, editor. Clinical Practice Guideline. U.S Department of Health and Human Services. Public Health Service; Rockville, MD: 2008. [Google Scholar]
- Grembowski D, Patrick D, Diehr P, Durham M, Beresford S, Kay E, Hecht J. Self-efficacy and health behavior among older adults. J Health Soc Behav. 1993;34:89–104. [PubMed] [Google Scholar]
- Hageman PA, Walker SN, Pullen CH. Tailored versus standard internet-delivered interventions to promote physical activity in older women. J Geriatr Phys Ther. 2005;28:28–33. doi: 10.1519/00139143-200504000-00005. [DOI] [PubMed] [Google Scholar]
- Hall KL, Rossi JS. Meta-analytic examination of the strong and weak principles across 48 health behaviors. Prev Med. 2008;46:266–274. doi: 10.1016/j.ypmed.2007.11.006. [DOI] [PubMed] [Google Scholar]
- Heimendinger J, O’Neill C, Marcus AC, Wolfe P, Julesburg K, Morra M, Allen A, Davis S, Mowad L, Perocchia RS, Ward JD, Strecher V, Warnecke R, Nowak M, Graf I, Fairclough D, Bryant L, Lipkus I. Multiple tailored messages are effective in increasing fruit and vegetable consumption among callers to the cancer information service. J Health Commun. 2005;10:65–82. doi: 10.1080/10810730500263646. [DOI] [PubMed] [Google Scholar]
- Higgins J, Green S. Cochrane handbook for systematic reviews of interventions version 5.0.2. The Cochrane Collaboration; 2009. [Google Scholar]
- Hughes JR, Keely JP, Niaura RS, Ossip-Klein DJ, Richmond RL, Swan GE. Measures of abstinence in clinical trials: Issues and recommendations. Nicotine Tob Res. 2003;5:13–25. [PubMed] [Google Scholar]
- Institute of Medicine. Health and behavior. National Academies Press; 2001. p. 377. [Google Scholar]
- Kreuter MW, Skinner CS. Tailoring: What’s in a name? Health Educ Res. 2000;15:1–4. doi: 10.1093/her/15.1.1. [DOI] [PubMed] [Google Scholar]
- Kroeze W, Werkman A, Brug J. A systematic review of randomized trials on the effectiveness of computer-tailored education on physical activity and dietary behaviors. Ann Behav Med. 2006;31:205–223. doi: 10.1207/s15324796abm3103_2. [DOI] [PubMed] [Google Scholar]
- Lancaster T, Stead LF. Telephone counselling for smoking cessation. Cochrane Database of Systematic Reviews. 2006;3:CD002850. doi: 10.1002/14651858.CD002850.pub2. [DOI] [PubMed] [Google Scholar]
- Lipsey M, Wilson DB. Practical meta-analysis. Sage; Thousand Oaks, CA: 2001. [Google Scholar]
- Moher D, Cook DJ, Eastwood S, Olkin I, Rennie D, Stroup DF. Improving the quality of reports of meta-analyses of randomised controlled trials: The quorom statement. Lancet. 1999;354:1896–1900. doi: 10.1016/s0140-6736(99)04149-5. [DOI] [PubMed] [Google Scholar]
- Moher D, Pham B, Jones A, Cook DJ, Jadad AR, Moher M, Tugwell P, Klassen TP. Does quality of reports of randomised trials affect estimates of intervention efficacy reported in meta-analyses? Lancet. 1998;352:609–613. doi: 10.1016/S0140-6736(98)01085-X. [DOI] [PubMed] [Google Scholar]
- Noar SM, Benac CN, Harris MS. Does tailoring matter? Meta-analytic review of tailored print health behavior change interventions. Psychol Bull. 2007;133:673–693. doi: 10.1037/0033-2909.133.4.673. [DOI] [PubMed] [Google Scholar]
- Noar SM, Chabot M, Zimmerman RS. Applying health behavior theory to multiple behavior change: Considerations and approaches. Prev Med. 2008;46:275–280. doi: 10.1016/j.ypmed.2007.08.001. [DOI] [PubMed] [Google Scholar]
- Norman GJ. A review of ehealth interventions for physical activity and dietary behavior change. Am J Prev Med. 2007;33:336–345. e316. doi: 10.1016/j.amepre.2007.05.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Petty K, Elster A. Attitudes and persuasion: Classical and contemporary approaches. Brown; Dubuque, IA: 1981. [Google Scholar]
- Portnoy DB, Scott-Sheldon LA, Johnson BT, Carey MP. Computer-delivered interventions for health promotion and behavioral risk reduction: A meta-analysis of 75 randomized controlled trails, 1988-2007. Prev Med. 2008;47:3–16. doi: 10.1016/j.ypmed.2008.02.014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Prochaska JJ, Spring B, Nigg CR. Multiple health behavior change research: An introduction and overview. Prev Med. 2008;46:181–188. doi: 10.1016/j.ypmed.2008.02.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Prochaska JO, DiClemente CC, Velicer WF, Rossi JS. Standardized, individualized, interactive, and personalized self-help programs for smoking cessation. Health Psychol. 1993;12:399–405. doi: 10.1037//0278-6133.12.5.399. [DOI] [PubMed] [Google Scholar]
- Rimer BK, Kreuter MW. Advancing tailored health communication: A persuasion and message effects perspective. J Commun. 2006;56 [Google Scholar]
- Rossi JS. Comparison of the use of significance testing and effect sizes in theory-based health promotion research. 43rd Annual Meeting of the Society for Multivariate Experimental Psychology, Keystone, CO; Keystone, CO. 2003. [Google Scholar]
- Ryan P, Lauver DR. The efficacy of tailored interventions. J Nurs Scholarsh. 2002;34:331–337. doi: 10.1111/j.1547-5069.2002.00331.x. [DOI] [PubMed] [Google Scholar]
- Skinner CS, Campbell MK, Rimer BK, Curry S, Prochaska JO. How effective is tailored print communication? Ann Behav Med. 1999;21:290–298. doi: 10.1007/BF02895960. [DOI] [PubMed] [Google Scholar]
- Sohl SJSJ. Tailored interventions to promote mammography screening: A meta-analytic review. Prev Med. 2007;45:252–261. doi: 10.1016/j.ypmed.2007.06.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stellefson ML, Hanik BW, Chaney BH, Chaney JD. Challenges for tailored messaging in health education. Am J Health Educ. 2008;39:303–311. [Google Scholar]
- Strecher VJ. Computer-tailored smoking cessation materials: A review and discussion. Patient Educ Couns. 1999;36:107–117. doi: 10.1016/s0738-3991(98)00128-1. [DOI] [PubMed] [Google Scholar]
- Strecher VJ, Shiffman S, West R. Randomized controlled trial of a web-based computer-tailored smoking cessation program as a supplement to nicotine patch therapy. Addiction. 2005;100:682–688. doi: 10.1111/j.1360-0443.2005.01093.x. [DOI] [PubMed] [Google Scholar]
- Thompson BT, Schoenfeld D. Usual care as the control group in clinical trials of nonpharmacologic interventions. Proc Am Thorac Soc. 2007;4:577–582. doi: 10.1513/pats.200706-072JK. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tunis SR, Stryer DB, Clancy CM. Practical clinical trials: Increasing the value of clinical research for decision making in clinical and health policy. JAMA. 2003;290:1624–1632. doi: 10.1001/jama.290.12.1624. [DOI] [PubMed] [Google Scholar]
- Vandelanotte C, Reeves MM, Brug J, De Bourdeaudhuij I. A randomized trial of sequential and simultaneous multiple behavior change interventions for physical activity and fat intake. Prev Med. 2008;46:232–237. doi: 10.1016/j.ypmed.2007.07.008. [DOI] [PubMed] [Google Scholar]
- Velicer WF, Prochaska JO. A comparison of four self-report smoking cessation outcome measures. Addict Behav. 2004;29:51–60. doi: 10.1016/s0306-4603(03)00084-4. [DOI] [PubMed] [Google Scholar]
- World Health Organization. Move for health. World Health Organization; Geneva: 2002. [Google Scholar]
Studies Included for Analysis
- Anderson ES, Winett RA, Wojcik JR, Winett SG, Bowden T. A computerized social cognitive intervention for nutrition behavior: Direct and mediated effects on fat, fiber, fruits and vegetables, self-efficacy and outcome expectations among food shoppers. Ann Behav Med. 2001;23:88–100. doi: 10.1207/S15324796ABM2302_3. [DOI] [PubMed] [Google Scholar]
- Armitage CJ, Conner M. Efficacy of a minimal intervention to reduce fat intake. Soc Sci Med. 2001;52:1517–1524. doi: 10.1016/s0277-9536(00)00265-3. [DOI] [PubMed] [Google Scholar]
- Ausems M, Mesters I, van Breukelen G, de Vries H. Effects of in-school and tailored out-of-school smoking prevention among Dutch vocational school students. Health Educ Res. 2004;19:51–63. doi: 10.1093/her/cyg001. [DOI] [PubMed] [Google Scholar]
- Aveyard P, Griffin C, Lawrence T, Cheng KK. A controlled trial of an expert system and self-help manual intervention based on the stages of change versus standard self-help materials in smoking cessation. Addiction. 2003;98:345–354. doi: 10.1046/j.1360-0443.2003.00302.x. [DOI] [PubMed] [Google Scholar]
- Bastani R, Maxwell AE, Bradford C, Das IP, Yan KX. Tailored risk notification for women with a family history of breast cancer. Prev Med. 1999;29:355–364. doi: 10.1006/pmed.1999.0556. [DOI] [PubMed] [Google Scholar]
- Becona E, Velazquez FL. Effectiveness of personalized written feedback through a mail intervention for smoking cessation: A randomized-controlled trial in Spanish smokers. J Consult Clin Psychol. 2001;69:33–40. [PubMed] [Google Scholar]
- Block G, Wakimoto P, Metz D, Fujii ML, Feldman N, Mandel R, Sutherland B. A randomized trial of the Little by Little CD-ROM: demonstrated effectiveness in increasing fruit and vegetable intake in a low-income population. Prev Chronic Dis. 2004;1:A08. [PMC free article] [PubMed] [Google Scholar]
- Bock BC, Marcus BH, Pinto BM, Forsyth LH. Maintenance of physical activity following an individualized motivationally tailored interention. Ann Behav Med. 2001;23:79–87. doi: 10.1207/S15324796ABM2302_2. [DOI] [PubMed] [Google Scholar]
- Borland R, Balmford J, Hunt D. The effectiveness of personally tailored computer-generated advice letters for smoking cessation. Addiction. 2004;99:369–377. doi: 10.1111/j.1360-0443.2003.00623.x. [DOI] [PubMed] [Google Scholar]
- Borland R, Balmford J, Segan C, Livingston P, Owen N. The effectiveness of personalized smoking cessation strategies for callers to a Quitline service. Addiction. 2003;98:837–846. doi: 10.1046/j.1360-0443.2003.00389.x. [DOI] [PubMed] [Google Scholar]
- Brug J, Glanz K, van Assema P, Kok G, van Breukelen GJP. The impact of computer-tailored feedback and iterative feedback on fat, fruit, and vegetable intake. Health Educ Behav. 1998;25:517–531. doi: 10.1177/109019819802500409. [DOI] [PubMed] [Google Scholar]
- Brug J, Steenhaus I, van Assema P, de Vries J. The impact of computer-tailored nutrition intervention. Prev Med. 1996;25:236–242. doi: 10.1006/pmed.1996.0052. [DOI] [PubMed] [Google Scholar]
- Brug J, Steenhuis I, van Assema P, Glanz K, de Vries H. Computer-tailored nutrition education: Differences between two interventions. Health Educ Res. 1999;14:249–256. doi: 10.1093/her/14.2.249. [DOI] [PubMed] [Google Scholar]
- Bull FC, Jamrozik K, Blanksby BA. Tailored advice on exercise: Does it make a difference? Am J Preventive Med. 1999;16:230–239. doi: 10.1016/s0749-3797(98)00160-3. [DOI] [PubMed] [Google Scholar]
- Bull FC, Kreuter MW, Scharff DP. Effects of tailored, personalized and general health messages on physical activity. Patient Educ Couns. 1999;36:181–192. doi: 10.1016/s0738-3991(98)00134-7. [DOI] [PubMed] [Google Scholar]
- Burnett KF, Magel PE, Harrington S, Taylor CB. Computer-assisted behavioral health counseling for high school students. J Counsel Psychol. 1989;36:63–67. [Google Scholar]
- Campbell MK, Bernhardt JM, Waldmiller M, Jackson B, Potenziani D, Weathers B, Demissie S. Varying the message source in computer-tailored nutrition education. Patient Educ Couns. 1999;36:157–169. doi: 10.1016/s0738-3991(98)00132-3. [DOI] [PubMed] [Google Scholar]
- Campbell MK, Carbone E, Honess-Morreale L, Heisler-Mackinnon J, Demissie S, Farrell D. Randomized trial of a tailored nutrition education CD-ROM program for women receiving food assistance. J Nutr Educ Behav. 2004;36:58–66. doi: 10.1016/s1499-4046(06)60134-6. [DOI] [PubMed] [Google Scholar]
- Campbell MK, DeVellis BM, Strecher VJ, Ammerman AS. Improving dietary behavior: The effectiveness of tailored messages in primary care settings. Am J Public Health. 1994;84:783–787. doi: 10.2105/ajph.84.5.783. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Campbell MK, Honess-Morreale L, Farrell D, Carbone E, Brasure M. A tailored multimedia nutrition education pilot program for low-income women receiving food assistance. Health Educ Res. 1999;14:257–267. doi: 10.1093/her/14.2.257. [DOI] [PubMed] [Google Scholar]
- Campbell MK, James A, Hudson MA, Carr C, Jackson E, Oates V, Demissie S, Tessaro I, Farrell D. Improving multiple behaviors for colorectal cancer prevention among African American church members. Health Psychol. 2004;23:492–502. doi: 10.1037/0278-6133.23.5.492. [DOI] [PubMed] [Google Scholar]
- Campbell MK, Tessaro I, DeVellis B, Benedict S, Kelsey K, Belton L, Sanhueza A. Effects of a tailored health promotion program for female blue-collar workers: Health Works for Women. Prev Med. 2002;34:313–323. doi: 10.1006/pmed.2001.0988. [DOI] [PubMed] [Google Scholar]
- Cardinal BJ, Sachs ML. Prospective analysis of stage-of-exercise movement following mail-delivered, self-instructional exercise packets. Am J Health Promot. 1995;9:430–432. doi: 10.4278/0890-1171-9.6.430. [DOI] [PubMed] [Google Scholar]
- Champion V, Skinner CS, Hui S, Monahan P, Juliar B, Daggy J, Menon U. The effect of telephone versus print tailoring for mammography adherence. Patient Educ Couns. 2007;65:416–423. doi: 10.1016/j.pec.2006.09.014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Champion VL, Skinner CS, Menon U, Seshadri R, Anzalone DC, Rawl SM. Comparisons of tailored mammography interventions at two months postintervention. Ann Behav Med. 2002;24:211–218. doi: 10.1207/S15324796ABM2403_06. [DOI] [PubMed] [Google Scholar]
- Clark MA, Rakowski W, Ehrich B, Rimer BK, Velicer WF, Dube CE, Pearlman DN, Peterson KK, Goldstein M. The effect of a stage-matched and tailored intervention on repeat mammography. Am J Prev Med. 2002;22:1–7. doi: 10.1016/s0749-3797(01)00406-8. [DOI] [PubMed] [Google Scholar]
- Curry SJ, McBride C, Grothaus LC, Louie D, Wagner EH. A randomized trial of self-help materials, personalized feedback, and telephone counseling with nonvolunteer smokers. J Consult Clin Psychol. 1995;63:1005–1014. doi: 10.1037//0022-006x.63.6.1005. [DOI] [PubMed] [Google Scholar]
- Curry SJ, Wagner EH, Grothaus LC. Evaluation of intrinsic and extrinsic motivation interventions with a self-help smoking cessation program. J Consult Clin Psychol. 1991;59:318–324. doi: 10.1037//0022-006x.59.2.318. [DOI] [PubMed] [Google Scholar]
- Delichatsios HK, Friedman RH, Glanz K, Tennstedt S, Smigelski C, Pinto BM, Kelley H, Gillman MW. Randomized trial of a “talking computer” to improve adults’ eating habits. Am J Health Promot. 2001;15:215–224. doi: 10.4278/0890-1171-15.4.215. [DOI] [PubMed] [Google Scholar]
- Demark-Wahnefried W, Clipp EC, Lipkus IM, Lobach D, Snyder DC, Sloane R, Peterson B, Macri JM, Rock CL, McBride CM, Kraus WE. Main outcomes of the FRESH START trial: a sequentially tailored, diet and exercise mailed print intervention among breast and prostate cancer survivors. J Clin Oncol. 2007;25:2709–2718. doi: 10.1200/JCO.2007.10.7094. [DOI] [PubMed] [Google Scholar]
- Di Noia J, Contento IR, Prochaska JO. Computer-mediated intervention tailored on transtheoretical model stages and processes of change increases fruit and vegetable consumption among urban African-American adolescents. Am J Health Promot. 2008;22:336–341. doi: 10.4278/ajhp.22.5.336. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dijkstra A. Working mechanisms of computer-tailored health education: Evidence from smoking cessation. Health Educ Res. 2005;20:527–539. doi: 10.1093/her/cyh014. [DOI] [PubMed] [Google Scholar]
- Dijkstra A, de Vries H, Roijackers J. Long-term effectiveness of computer-generated tailored feedback in smoking cessation. Health Education Research. 1998;13:207–214. doi: 10.1093/her/13.2.207. [DOI] [PubMed] [Google Scholar]
- Dijkstra A, de Vries H, Roijackers J. Targeting smokers with low readiness to change with tailored and nontailored self-help materials. Prev Med. 1999;28:203–211. doi: 10.1006/pmed.1998.0407. [DOI] [PubMed] [Google Scholar]
- Elder JP, Ayala GX, Campbell NR, Arredondo EM, Slymen DJ, Baquero B, Zive M, Ganiats TG, Engelberg M. Long-term effects of a communication intervention for Spanish-dominant Latinas. Am J Prev Med. 2006;31:159–166. doi: 10.1016/j.amepre.2006.04.001. [DOI] [PubMed] [Google Scholar]
- Etter J-F, Perneger TV. Post-intervention effect of a computer tailored smoking cessation programme. J Epidemiol Community Health. 2004;58:849–851. doi: 10.1136/jech.2003.017103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Etter J. Comparing the efficacy of two internet-based, computer-tailored smoking cessation programs: A randomized trial. J Med Internet Res. 2005;7 doi: 10.2196/jmir.7.1.e2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Frenn M, Malin S, Brown RL, Greer Y, Fox J, Greer J, Smyczek S. Changing the tide: an Internet/video exercise and low-fat diet intervention with middle-school students. Appl Nurs Res. 2005;18:13–21. doi: 10.1016/j.apnr.2004.04.003. [DOI] [PubMed] [Google Scholar]
- Greaney ML, Riebe D, Garber CE, Rossi JS, Lees FD, Burbank PA, Nigg CR, Ferrone CL, Clark PG. Long-term effects of a stage-based intervention for changing exercise intentions and behavior in older adults. Gerontologist. 2008;48:358–367. doi: 10.1093/geront/48.3.358. [DOI] [PubMed] [Google Scholar]
- Haerens L, Deforche B, Maes L, Brug J, Vandelanotte C, De Bourdeaudhuij I. A computer-tailored dietary fat intake intervention for adolescents: Results of a randomized controlled trial. Ann Behav Med. 2007;34:253–262. doi: 10.1007/BF02874550. [DOI] [PubMed] [Google Scholar]
- Hageman PA, Walker SN, Pullen CH. Tailored versus standard internet-delivered interventions to promote physical activity in older women. J Geriatr Phys Ther. 2005;28:28–33. doi: 10.1519/00139143-200504000-00005. [DOI] [PubMed] [Google Scholar]
- Heimendinger J, O’Neill C, Marcus AC, Wolfe P, Julesburg K, Morra M, Allen A, Davis S, Mowad L, Perocchia RS, Ward JD, Strecher V, Warnecke R, Nowak M, Graf I, Fairclough D, Bryant L, Lipkus I. Multiple tailored messages are effective in increasing fruit and vegetable consumption among callers to the cancer information service. J Health Commun. 2005;10:65–82. doi: 10.1080/10810730500263646. [DOI] [PubMed] [Google Scholar]
- Irvine AB, Ary DV, Grove DA, Gilfillan-Morton L. The effectiveness of an interactive multimedia program to influence eating habits. Health Educ Res. 2004;19:290–305. doi: 10.1093/her/cyg027. [DOI] [PubMed] [Google Scholar]
- Johnson SS, Driskell MM, Johnson JL, Prochaska JM, Zwick W, Prochaska JO. Efficacy of a transtheoretical model-based expert system for antihypertensive adherence. Dis Manag. 2006;9:291–301. doi: 10.1089/dis.2006.9.291. [DOI] [PubMed] [Google Scholar]
- Johnson SS, Paiva AL, Cummins CO, Johnson JL, Dyment SJ, Wright JA, Prochaska JO, Prochaska JM, Sherman K. Transtheoretical Model-based multiple behavior intervention for weight management: Effectiveness on a population basis. Prev Med. 2008;46:238–246. doi: 10.1016/j.ypmed.2007.09.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jones H, Edwards L, Vallis TM, Ruggiero L, Rossi SR, Rossi JS, Greene G, Prochaska JO, Zinman B. Changes in diabetes self-care behaviors make a difference in glycemic control: The diabetes stages of change (DiSC) study. Diabetes Care. 2003;26:732–737. doi: 10.2337/diacare.26.3.732. [DOI] [PubMed] [Google Scholar]
- King AC, Friedman R, Marcus B, Castro C, Napolitano M, Ahn D, Baker L. Ongoing Physical Activity Advice by Humans Versus Computers: The Community Health Advice by Telephone (CHAT) Trial. Health Psychol. 2007;26:718–727. doi: 10.1037/0278-6133.26.6.718. [DOI] [PubMed] [Google Scholar]
- Kosma M, Cardinal BJ, McCubbin JA. A pilot study of a web-based physical activity motivational program for adults with physical disabilities. Disabil Rehabil. 2005;27:1435–1442. doi: 10.1080/09638280500242713. [DOI] [PubMed] [Google Scholar]
- Kreuter MW, Strecher VJ. Do tailored behavior change messages enhance the effectiveness of health risk appraisal? Results from a randomized trial. Health Educ Res. 1996;11:97–105. doi: 10.1093/her/11.1.97. [DOI] [PubMed] [Google Scholar]
- Kreuter MW, Sugg-Skinner C, Holt CL, Clark EM, Haire-Joshu D, Fu Q, Booker AC, Steger-May K, Bucholtz D. Cultural tailoring for mammography and fruit and vegetable intake among low-income African-American women in urban public health centers. Prev Med. 2005;41:53–62. doi: 10.1016/j.ypmed.2004.10.013. [DOI] [PubMed] [Google Scholar]
- Kristal AR, Curry SJ, Shattuck AL, Feng Z, Li S. A randomized trial of a tailored, self-help dietary intervention: The Puget Sound eating patterns study. Prev Med. 2000;31:380–389. doi: 10.1006/pmed.2000.0711. [DOI] [PubMed] [Google Scholar]
- Kypri K, McAnally HM. Randomized controlled trial of a web-based primary care intervention for multiple health risk behaviors. Prev Med. 2005;41:761–766. doi: 10.1016/j.ypmed.2005.07.010. [DOI] [PubMed] [Google Scholar]
- Lennox AS, Osman LM, Reiter E, Robertson R, Friend J, McCann I, Skatun D, Donnan PT. Cost effectiveness of computer tailored an non-tailored smoking cessation letters in general practice: Randomised controlled trial. BMJ. 2001;322:1396–1400. doi: 10.1136/bmj.322.7299.1396. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lipkus IM, Lyna PR, Rimer BK. Using tailored interventions to enhance smoking cessation among African-Americans at a community health center. Nicotine Tob Res. 1999;1:77–85. doi: 10.1080/14622299050011181. [DOI] [PubMed] [Google Scholar]
- Lipkus IM, Rimer BK, Halabi S, Strigo TS. Can tailored interventions increase mammography use among HMO women? Am J Prev Med. 2000;18:1–10. doi: 10.1016/s0749-3797(99)00106-3. [DOI] [PubMed] [Google Scholar]
- Lutz SF, Ammerman AS, Atwood JR, Campbell MK, DeVellis RF, Rosamond WD. Innovative newsletter interventions improve fruit and vegetable consumption in healthy adults. J Am Diet Assoc. 1999;99:705–709. doi: 10.1016/S0002-8223(99)00169-8. [DOI] [PubMed] [Google Scholar]
- Marcus BH, Bock BC, Pinto BM, Forsyth LH, Roberts MB, Traficante RM. Efficacy of an individualized, motivationally-tailored physical activity intervention. Ann Behav Med. 1998;20:174–180. doi: 10.1007/BF02884958. [DOI] [PubMed] [Google Scholar]
- Marcus BH, Napolitano MA, King AC, Lewis BA, Whiteley JA, Albrecht A, Parisi A, Bock B, Pinto B, Sciamanna C, Jakicic J, Papandonatos GD. Telephone versus print delivery of an individualized motivationally tailored physical activity intervention: Project STRIDE. Health Psychol. 2007;26:401–409. doi: 10.1037/0278-6133.26.4.401. [DOI] [PubMed] [Google Scholar]
- McKay HG, King D, Eakin EG, Seeley JR, Glasgow RE. The diabetes network internet-based physical activity intervention: a randomized pilot study. Diabetes Care. 2001;24:1328–1334. doi: 10.2337/diacare.24.8.1328. [DOI] [PubMed] [Google Scholar]
- Meyer C, Ulbricht S, Baumeister SE, Schumann A, Ru?ge J, Bischof G, Rumpf HJ, John U. Proactive interventions for smoking cessation in general medical practice: A quasi-randomized controlled trial to examine the efficacy of computer-tailored letters and physician-delivered brief advice. Addiction. 2008;103:294–304. doi: 10.1111/j.1360-0443.2007.02031.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Napolitano MA, Fotheringham M, Tate D, Sciamanna C, Leslie E, Owen N, Bauman A, Marcus B. Evaluation of an Internet-based physical activity intervention: A preliminary investigation. Ann Behav Med. 2003;25:92–99. doi: 10.1207/S15324796ABM2502_04. [DOI] [PubMed] [Google Scholar]
- Nitzke S, Kritsch K, Boeckner L, Greene G, Hoerr S, Horacek T, Kattelmann K, Lohse B, Oakland MJ, Phillips B, White A. A stage-tailored multi-modal intervention increases fruit and vegetable intakes of low-income young adults. Am J Health Promot. 2007;22:6–14. doi: 10.4278/0890-1171-22.1.6. [DOI] [PubMed] [Google Scholar]
- Oenema A, Tan F, Brug J. Short-Term Efficacy of a Web-Based Computer-Tailored Nutrition Intervention: Main Effects and Mediators. Ann Behav Med. 2005;29:54–63. doi: 10.1207/s15324796abm2901_8. [DOI] [PubMed] [Google Scholar]
- Owen N, Ewins A-L, Lee C. Smoking cessation by mail: A comparison of standard and personalized correspondence course formats. Addict Behav. 1989;14:355–363. doi: 10.1016/0306-4603(89)90023-3. [DOI] [PubMed] [Google Scholar]
- Papadaki A, Scott JA. The Mediterranean eating in Scotland experience project: evaluation of an Internet-based intervention promoting the Mediterranean diet. Br J Nutr. 2005;94:290–298. doi: 10.1079/bjn20051476. [DOI] [PubMed] [Google Scholar]
- Patrick K, Sallis JF, Prochaska JJ, Lydston DD, Calfas KJ, Zabinski MF, Wilfley DE, Saelens BE, Brown DR. A multicomponent program for nutrition and physical activity change in primary care: PACE+ for adolescents. Arch Pediatr Adolesc Med. 2001;155:940–946. doi: 10.1001/archpedi.155.8.940. [DOI] [PubMed] [Google Scholar]
- Peterson TR, Aldana SG. Improving exercise behavior: An application of the stages of change model in a worksite setting. Am J Health Promot. 1999;13:229–232. doi: 10.4278/0890-1171-13.4.229. [DOI] [PubMed] [Google Scholar]
- Pinto B, Friedman R, Marcus BH, Kelley H, Tennstedt S, Gillman MW. Effects of a computer-based, telephone-counseling system on physical activity. Am J Prev Med. 2002;23:113–120. doi: 10.1016/s0749-3797(02)00441-5. [DOI] [PubMed] [Google Scholar]
- Prochaska JJ, Sallis JF. A randomized controlled trial of single versus multiple health behavior change: Promoting physical activity and nutrition among adolescents. Health Psychol. 2004;23:314–318. doi: 10.1037/0278-6133.23.3.314. [DOI] [PubMed] [Google Scholar]
- Prochaska JO, DiClemente CC, Velicer WF, Rossi JS. Standardized, individualized, interactive, and personalized self-help programs for smoking cessation. Health Psychol. 1993;12:399–405. doi: 10.1037//0278-6133.12.5.399. [DOI] [PubMed] [Google Scholar]
- Prochaska JO, Velicer WF, Fava JL, Rossi JS, Tsoh JY. Evaluating a population-based recruitment approach and a stage-based expert system intervention for smoking cessation. Addict Behav. 2001;26:583–602. doi: 10.1016/s0306-4603(00)00151-9. [DOI] [PubMed] [Google Scholar]
- Prochaska JO, Velicer WF, Fava JL, Ruggiero L, Laforge RG, Rossi JS, Johnson SS, Lee PA. Counselor and stimulus control enhancements of a stage-matched expert system intervention for smokers in a managed care setting. Prev Med. 2001;32:23–32. doi: 10.1006/pmed.2000.0767. [DOI] [PubMed] [Google Scholar]
- Prochaska JO, Velicer WF, Redding C, Rossi JS, Goldstein M, DePue J, Greene GW, Rossi SR, Sun X, Fava JL, Laforge R, Rakowski W, Plummer BA. Stage-based expert systems to guide a population of primary care patients to quit smoking, eat healthier, prevent skin cancer, and receive regular mammograms. Prev Med. 2005;41:406–416. doi: 10.1016/j.ypmed.2004.09.050. [DOI] [PubMed] [Google Scholar]
- Prochaska JO, Velicer WF, Rossi JS, Redding CA, Greene GW, Rossi SR, Sun X, Fava JL, Laforge R, Plummer BA. Multiple risk expert systems interventions: Impact of simultaneous stage-matched expert system interventions for smoking, high-fat diet, and sun exposure in a population of parents. Health Psychol. 2004;23:503–516. doi: 10.1037/0278-6133.23.5.503. [DOI] [PubMed] [Google Scholar]
- Rakowski W, Ehrich B, Goldstein MG, Rimer BK, Pearlman DN, Clark MA, Velicer WF, Woolverton H., III Increasing mammography among women aged 40-74 by use of a stage-matched, tailored intervention. Prev Med. 1998;27:748–756. doi: 10.1006/pmed.1998.0354. [DOI] [PubMed] [Google Scholar]
- Rakowski W, Lipkus IM, Clark MA, Rimer BK, Ehrich B, Lyna PR, Kornguth PJ. Reminder letter, tailored stepped-care, and self-choice comparison for repeat mammography. Am J Prev Med. 2003;25:308–314. doi: 10.1016/s0749-3797(03)00215-0. [DOI] [PubMed] [Google Scholar]
- Rimer BK, Halabi S, Skinner CS, Lipkus IM, Strigo TS, Kaplan EB, Samsa GP. Effects of a mammography decision-making intervention at 12 and 24 months. Am J Prev Med. 2002;22:247–257. doi: 10.1016/s0749-3797(02)00417-8. [DOI] [PubMed] [Google Scholar]
- Saywell RM, Jr, Champion VL, Skinner CS, Menon U, Daggy J. A cost-effectiveness comparison of three tailored interventions to increase mammography screening. J Women’s Health. 2004;13:909–918. doi: 10.1089/jwh.2004.13.909. [DOI] [PubMed] [Google Scholar]
- Schumann A, John U, Baumeister S, Ulbricht S, Rumpf HJ, Meyer C. Computer-tailored smoking cessation intervention in a general population setting in Germany: Outcome of a randomized controlled trial. Nicotine Tob Res. 2008;10:371–379. doi: 10.1080/14622200701825767. [DOI] [PubMed] [Google Scholar]
- Shiffman S, Paty JA, Rohay JM, Di Marino ME, Gitchell JG. The efficacy of computer-tailored smoking cessation material as a supplement to nicotine patch therapy. Drug Alcohol Dep. 2001;64:35–46. doi: 10.1016/s0376-8716(00)00237-4. [DOI] [PubMed] [Google Scholar]
- Skinner CS, Strecher VJ, Hospers H. Physicians’ recommendations for mammography: do tailored messages make a difference? Am J Public Health. 1994;84:43–49. doi: 10.2105/ajph.84.1.43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Smeets T, Brug J, de Vries H. Effects of tailoring health messages on physical activity. Health Educ Res. 2008;23:402–413. doi: 10.1093/her/cyl101. [DOI] [PubMed] [Google Scholar]
- Strecher VJ, Kreuter M, Den Boer D-J, Kobrin S. The effects of computer-tailored smoking cessation messages in family practice settings. J Fam Pract. 1994;39:262–270. [PubMed] [Google Scholar]
- Strecher VJ, Marcus A, Bishop K, Fleisher L, Stengle W, Levinson A, Fairclough DL, Wolfe P, Morra M, Davis S, Warnecke R, Heimendinger J, Nowak M. A randomized controlled trial of multiple tailored messages for smoking cessation among callers to the cancer information service. J Health Commun. 2005;10:105–118. doi: 10.1080/10810730500263810. [DOI] [PubMed] [Google Scholar]
- Strecher VJ, Shiffman S, West R. Randomized controlled trial of a web-based computer-tailored smoking cessation program as a supplement to nicotine patch therapy. Addiction. 2005;100:682–688. doi: 10.1111/j.1360-0443.2005.01093.x. [DOI] [PubMed] [Google Scholar]
- Velicer WF, Friedman RH, Fava JL, Gulliver SB, Keller S, Sun X, Ramelson H, Prochaska JO. Evaluating nicotine replacement therapy and stage-based therapies in a population-based effectiveness trial. J Consult Clin Psychol. 2006;74:1162–1172. doi: 10.1037/0022-006X.74.6.1162. [DOI] [PubMed] [Google Scholar]
- Velicer WF, Prochaska JO, Fava JL, Laforge RG, Rossi JS. Interactive versus noninteractive interventions and dose-response relationships for stage-matched smoking cessation programs in a managed care setting. Health Psychol. 1999;18:21–28. doi: 10.1037//0278-6133.18.1.21. [DOI] [PubMed] [Google Scholar]
References for Excluded Studies
- 1.Blalock SJ, DeVellis BM, Patterson CC, Campbell MK, Orenstein DR, Dooley MA. Effects of an osteoporosis prevention program incorporating tailored educational materials. Am J Health Promot. 2002;16:146–156. doi: 10.4278/0890-1171-16.3.146. [DOI] [PubMed] [Google Scholar]
- 2.Brinberg D, Axelson ML. Increasing the consumption of dietary fiber: A decision theory analysis. Health Educ Res. 1990;5:409–420. [Google Scholar]
- 3.Brinberg D, Axelson ML, Price S. Changing food knowledge, food choice, and dietary fiber consumption by using tailored messages. Appetite. 2000;35:35–43. doi: 10.1006/appe.2000.0335. [DOI] [PubMed] [Google Scholar]
- 4.Brug J, van Assema P. Differences in use and impact of computer-tailored dietary fat-feedback according to stage of change and education. Appetite. 2000;34:285–293. doi: 10.1006/appe.2000.0322. [DOI] [PubMed] [Google Scholar]
- 5.Brug J, Glanz K, Kok G. The relationship between self-efficacy, attitudes, intake compared to others, consumption, and stages of change related to fruit and vegetables. Am J Health Promot. 1997;12:25–30. doi: 10.4278/0890-1171-12.1.25. [DOI] [PubMed] [Google Scholar]
- 6.De Bourdeaudhuij I, Brug J, Vandelanotte C, Van Oost P. Differences in impact between a family- versus an individual-based tailored intervention to reduce fat intake. Health Educ Res. 2002;17:435–449. doi: 10.1093/her/17.4.435. [DOI] [PubMed] [Google Scholar]
- 7.de Vet E, de Nooijer J, de Vries NK, Brug J. Testing the transtheoretical model for fruit intake: Comparing web-based tailored stage-matched and stage-mismatched feedback. Health Educ Res. 2008;23:218–227. doi: 10.1093/her/cym019. [DOI] [PubMed] [Google Scholar]
- 8.Esters ON, Boeckner LS, Hubert M, Horacek T, Kritsch KR, Oakland MJ, Lohse B, Greene G, Nitzke S. Educator and participant perceptions and cost analysis of stage-tailored educational telephone calls. J Nutr Educ Behav. 2008;40:258–264. doi: 10.1016/j.jneb.2007.05.005. [DOI] [PubMed] [Google Scholar]
- 9.Glanz K, Murphy S, Moylan J, Evensen D, Curb JD. Improving dietary self-monitoring and adherence with hand-held computers: A pilot study. Am J Health Promot. 2006;20:165–170. doi: 10.4278/0890-1171-20.3.165. [DOI] [PubMed] [Google Scholar]
- 10.Glasgow RE, Toobert DJ, Hampson SE, Strycker LA. Implementation, generalization and long-term results of the “choosing well” diabetes self-management intervention. Patient Educ Couns. 2002;48:115–122. doi: 10.1016/s0738-3991(02)00025-3. [DOI] [PubMed] [Google Scholar]
- 11.Gould SM, Anderson J. Economic analysis of bilingual interactive multimedia nutrition education. J Nutr Educ Behav. 2002;34:273–278. doi: 10.1016/s1499-4046(06)60106-1. [DOI] [PubMed] [Google Scholar]
- 12.Jantz C, Anderson J, Gould SM. Using computer-based assessments to evaluate interactive multimedia nutrition education among low-income predominantly Hispanic participants. J Nutr Educ Behav. 2002;34:252–260. doi: 10.1016/s1499-4046(06)60103-6. [DOI] [PubMed] [Google Scholar]
- 13.King DK, Estabrooks PA, Strycker LA, Toobert DJ, Bull SS, Glasgow RE. Outcomes of a multifaceted physical activity regimen as part of a diabetes self-management intervention. Ann Behav Med. 2006;31:128–137. doi: 10.1207/s15324796abm3102_4. [DOI] [PubMed] [Google Scholar]
- 14.Oenema A, Brug J. Feedback strategies to raise awareness of personal dietary intake: Results of a randomized controlled trial. Prev Med. 2003;36:429–439. doi: 10.1016/s0091-7435(02)00043-9. [DOI] [PubMed] [Google Scholar]
- 15.Oenema A, Brug J, Lechner L. Web-based tailored nutrition education: Results of a randomized controlled trial. Health Edu Res. 2001;16:647–660. doi: 10.1093/her/16.6.647. [DOI] [PubMed] [Google Scholar]
- 16.Sorensen G, Thompson B, Glanz K, Feng Z, Kinne S, DiClemente C, Emmons K, Heimendinger J, Probart C, Lichtenstein E. Work site-based cancer prevention: primary results from the Working Well Trial. Am J Public Health. 1996;86:939–947. doi: 10.2105/ajph.86.7.939. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Stevens VJ, Glasgow RE, Toobert DJ, Karanja N, Smith KS. Randomized trial of a brief dietary intervention to decrease consumption of fat and increase consumption of fruits and vegetables. Am J Health Promot. 2002;16:129–134. doi: 10.4278/0890-1171-16.3.129. [DOI] [PubMed] [Google Scholar]
- 18.Stevens VJ, Glasgow RE, Toobert DJ, Karanja N, Smith KS. One-year results from a brief, computer-assisted intervention to decrease consumption of fat and increase consumption of fruits and vegetables. Prev Med. 2003;36:594–600. doi: 10.1016/s0091-7435(03)00019-7. [DOI] [PubMed] [Google Scholar]
- 19.Veverka DV, Anderson J, Auld GW, Coulter GR, Kennedy C, Chapman PL. Use of the stages of change model in improving nutrition and exercise habits in enlisted Air Force men. Mil Med. 2003;168:373–379. [PubMed] [Google Scholar]
- 20.Winett RA, Wagner JL, Moore JF, Walker WB, Hite LA, Leahy M, Neubauer T, Arbour D, Walberg J, Geller ES, et al. An experimental evaluation of a prototype public access nutrition information system for supermarkets. Health Psychol. 1991;10:75–78. doi: 10.1037//0278-6133.10.1.75. [DOI] [PubMed] [Google Scholar]
- 21.Kreuter MW, Bull FC, Clark EM, Oswald DL. Understanding how people process health information: A comparison of tailored and nontailored weight-loss materials. Health Psychol. 1999;18:487–494. doi: 10.1037//0278-6133.18.5.487. [DOI] [PubMed] [Google Scholar]
- 22.Tate DF, Wing RR, Winett RA. Using Internet technology to deliver a behavioral weight loss program. JAMA. 2001;285:1172–1177. doi: 10.1001/jama.285.9.1172. [DOI] [PubMed] [Google Scholar]
- 23.Tate DF, Jackvony EH, Wing RR. Effects of Internet behavioral counseling on weight loss in adults at risk for type 2 diabetes: a randomized trial. JAMA. 2003;289:1833–1836. doi: 10.1001/jama.289.14.1833. [DOI] [PubMed] [Google Scholar]
- 24.Glasgow RE, Boles SM, McKay HG, Feil EG, Barrera M., Jr The D-Net diabetes self-management program: Long-term implementation, outcomes, and generalization results. Prev Med. 2003;36:410–419. doi: 10.1016/s0091-7435(02)00056-7. [DOI] [PubMed] [Google Scholar]
- 25.Clark M, Hampson SE, Avery L, Simpson R. Effects of a tailored lifestyle self-management intervention in patients with Type 2 diabetes. Br J Health Psychol. 2004;9:365–379. doi: 10.1348/1359107041557066. [DOI] [PubMed] [Google Scholar]
- 26.Booth AO, Nowson CA, Matters H. Evaluation of an interactive, Internet-based weight loss program: A pilot study. Health Educ Res. 2008;23:371–381. doi: 10.1093/her/cyn007. [DOI] [PubMed] [Google Scholar]
- 27.Plotnikoff RC, McCargar LJ, Wilson PM, Loucaides CA. Efficacy of an E-mail intervention for the promotion of physical activity and nutrition behavior in the workplace context. Am J Health Promot. 2005;19:422–429. doi: 10.4278/0890-1171-19.6.422. [DOI] [PubMed] [Google Scholar]
- 28.Vandelanotte C, Reeves MM, Brug J, De Bourdeaudhuij I. A randomized trial of sequential and simultaneous multiple behavior change interventions for physical activity and fat intake. Prev Med. 2008;46:232–237. doi: 10.1016/j.ypmed.2007.07.008. [DOI] [PubMed] [Google Scholar]
- 29.Vandelanotte C, De Bourdeaudhuij I, Sallis JF, Spittaels H, Brug J. Efficacy of sequential or simultaneous interactive computer-tailored interventions for increasing physical activity and decreasing fat intake. Ann Behav Med. 2005;29:138–146. doi: 10.1207/s15324796abm2902_8. [DOI] [PubMed] [Google Scholar]
- 30.Allen B, Jr, Bazargan-Hejazi S. Evaluating a tailored intervention to increase screening mammography in an urban area. J Natl Med Assoc. 2005;97:1350–1360. [PMC free article] [PubMed] [Google Scholar]
- 31.Champion V, Maraj M, Hui S, Perkins AJ, Tierney W, Menon U, Skinner CS. Comparison of tailored interventions to increase mammography screening in nonadherent older women. Prev Med. 2003;36:150–158. doi: 10.1016/s0091-7435(02)00038-5. [DOI] [PubMed] [Google Scholar]
- 32.Gustafson DH, McTavish F, Stengle W, Ballard D, Hawkins R, Shaw BR, Jones E, JulÃs̈berg K, McDowell H, Chen WC, Volrathongchai K, Landucci G. Use and impact of eHealth system by low-income women with breast cancer. Journal of Health Communication Special Issue: The national cancer institute’s cancer information service: a new generation of service and research to the nation. 2005;10:195–218. doi: 10.1080/10810730500263257. [DOI] [PubMed] [Google Scholar]
- 33.Jibaja-Weiss ML, Volk RJ, Kingery P, Smith QW, Holcomb JD. Tailored messages for breast and cervical cancer screening of low-income and minority women using medical records data. Annual Meeting of the North American Primary Care Research Group; 28th Nov 2000; Amelia Island, FL, US. 2003. pp. 123–132. Presented in part at the aforementioned meeting. [DOI] [PubMed] [Google Scholar]
- 34.McCaul KD, Wold KS. The effects of mailed reminders and tailored messages on mammography screening. J Community Health. 2002;27:181–190. doi: 10.1023/a:1015249906674. [DOI] [PubMed] [Google Scholar]
- 35.Meldrum P, Turnbull D, Dobson HM, Colquhoun C, Gilmour WH, McIlwaine GM. Tailored written invitations for second round breast cancer screening: a randomised controlled trial. J Med Screen. 1994;1:245–248. doi: 10.1177/096914139400100412. [DOI] [PubMed] [Google Scholar]
- 36.Rimer BK, Halabi S, Skinner CS, Kaplan EB, Crawford Y, Samsa GP, Strigo TS, Lipkus IM. The short-term impact of tailored mammography decision-making interventions. Patient Educ Couns. 2001;43:271–287. doi: 10.1016/s0738-3991(00)00172-5. [DOI] [PubMed] [Google Scholar]
- 37.Stoddard AM, Fox SA, Costanza ME, Lane DS, Andersen MR, Urban N, Lipkus I, Rimer BK. Effectiveness of telephone counseling for mammography: Results from five randomized trials. Prev Med. 2002;34:90–99. doi: 10.1006/pmed.2001.0960. [DOI] [PubMed] [Google Scholar]
- 38.Williams-Piehota P, Pizarro J, Schneider TR, Mowad L, Salovey P. Matching health messages to monitor-blunter coping styles to motivate screening mammography. Health Psychol. 2005;24:58–67. doi: 10.1037/0278-6133.24.1.58. [DOI] [PubMed] [Google Scholar]
- 39.Ryan GL, Skinner CS, Farrell D, Champion VL. Examining the boundaries of tailoring: The utility of tailoring versus targeting mammography interventions for two distinct populations. Health Educ Res. 2001;16:555–556. doi: 10.1093/her/16.5.555. [DOI] [PubMed] [Google Scholar]
- 40.Brownson RC, Hagood L, Lovegreen SL, Britton B, Caito NM, Elliott MB, Emery J, Haire-Joshu D, Hicks D, Johnson B, McGill JB, Morton S, Rhodes G, Thurman T, Tune D. A multilevel ecological approach to promoting walking in rural communities. Prev Med. 2005;41:837–842. doi: 10.1016/j.ypmed.2005.09.004. [DOI] [PubMed] [Google Scholar]
- 41.Castro CM, King AC, Brassington GS. Telephone versus mail interventions for maintenance of physical activity in older adults. Health Psychol. 2001;20:438–444. [PubMed] [Google Scholar]
- 42.Demark-Wahnefried W, Clipp EC, McBride C, Lobach DF, Lipkus I, Peterson B, Clutter Snyder D, Sloane R, Arbanas J, Kraus WE. Design of FRESH START: A randomized trial of exercise and diet among cancer survivors. Med Sci Sports Exer. 2003;35:415–424. doi: 10.1249/01.MSS.0000053704.28156.0F. [DOI] [PubMed] [Google Scholar]
- 43.Hurling R, Fairley BW, Dias MB. Internet-based exercise intervention systems: Are more interactive designs better? Psychol Health. 2006;21:757–772. [Google Scholar]
- 44.Jacobs AD, Ammerman AS, Ennett ST, Campbell MK, Tawney KW, Aytur SA, Marshall SW, Will JC, Rosamond WD. Effects of a tailored follow-up intervention on health behaviors, beliefs, and attitudes. J Womens Health. 2004;13:557–568. doi: 10.1089/1540999041281016. [DOI] [PubMed] [Google Scholar]
- 45.Marshall AL, Leslie ER, Bauman AE, Marcus BH, Owen N. Print versus website physical activity programs: a randomized trial. Am J Prev Med. 2003;25:88–94. doi: 10.1016/s0749-3797(03)00111-9. [DOI] [PubMed] [Google Scholar]
- 46.Marcus BH, Emmons KM, Simkin-Silverman LR, Linnan LA, Taylor ER, Bock BC, Roberts MB, Rossi JS, Abrams DB. Evaluation of motivationally tailored vs. standard self-help physical activity interventions at the workplace. Am J Health Promot. 1998;12:246–253. doi: 10.4278/0890-1171-12.4.246. [DOI] [PubMed] [Google Scholar]
- 47.Marcus BH, Lewis BA, Williams DM, Whiteley JA, Albrecht AE, Jakicic JM, Parisi AF, Hogan JW, Napolitano MA, Bock BC. Step into Motion: A randomized trial examining the relative efficacy of Internet vs. print-based physical activity interventions. Contemp Clin Trials. 2007;28:737–747. doi: 10.1016/j.cct.2007.04.003. [DOI] [PubMed] [Google Scholar]
- 48.Purath J, Miller AM, McCabe G, Wilbur J. A brief intervention to increase physical activity in sedentary working women. Can J Nurs Res. 2004;36:76–91. [PubMed] [Google Scholar]
- 49.Van Sluijs EMF, Van Poppel MNM, Twisk JWR, Brug J, Van Mechelen W. The positive effect on determinants of physical activity of a tailored, general practice-based physical activity intervention. Health Educ Res. 2005;20:345–356. doi: 10.1093/her/cyg129. [DOI] [PubMed] [Google Scholar]
- 50.Burling TA, Marotta J, Gonzalez R, Moltzen JO. Computerized smoking cessation program for the worksite: Treatment outcome and feasibility. J Consult Clin Psychol. 1989;57:619–622. doi: 10.1037//0022-006x.57.5.619. [DOI] [PubMed] [Google Scholar]
- 51.Carpenter KM, Watson JM, Raffety B, Chabal C. Teaching brief interventions for smoking cessations via an interactive computer-based tutorial. J Health Psychol. 2003;8:149–160. doi: 10.1177/1359105303008001450. [DOI] [PubMed] [Google Scholar]
- 52.Chouinard M-C, Robichaud-Ekstrand S. The effectiveness of a nursing inpatient smoking cessation program in individuals with cardiovascular disease. Nurs Res. 2005;54:243–254. doi: 10.1097/00006199-200507000-00006. [DOI] [PubMed] [Google Scholar]
- 53.Cobb NK, Graham AL, Bock BC, Papandonatos G, Abrams DB. Initial evaluation of a real-world Internet smoking cessation system. Nicotine Tob Res. 2005;7:207–216. doi: 10.1080/14622200500055319. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Gilbert H, Nazareth I, Sutton S, Morris R, Godfrey C. Effectiveness of computer-tailored smoking cessation advice in primary care (ESCAPE): A randomised trial. Trials. 2008;9 doi: 10.1186/1745-6215-9-23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Klesges RC, DeBon M, Vander Weg MW, Haddock CK, Lando HA, Relyea GE, Peterson AL, Talcott GW. Efficacy of a tailored tobacco control program on long-term use in a population of U.S. military troops. J Consult Clin Psychol. 2006;74:295–306. doi: 10.1037/0022-006X.74.2.295. [DOI] [PubMed] [Google Scholar]
- 56.Lenert L, Munoz RF, Perez JE, Bansod A. Automated e-mail messaging as a tool for improving quit rates in an internet smoking cessation intervention. J Am Med Inform Assoc. 2004;11:235–240. doi: 10.1197/jamia.M1464. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Levinson AH, Glasgow RE, Gaglio B, Smith TL, Cahoon J, Marcus AC. Tailored behavioral support for smoking reduction: Development and pilot results of an innovative intervention. Health Educ Res. 2008;23:335–346. doi: 10.1093/her/cym046. [DOI] [PubMed] [Google Scholar]
- 58.Orleans CT, Boyd NR, Bingler R, Sutton C, Fairclough D, Heller D, McClatchey M, Ward J, Graves C, Fleisher L, Baum S. A self-help intervention for African American smokers: Tailoring Cancer Information Service counseling for a special population. Prev Med. 1998;27:S61–S70. doi: 10.1006/pmed.1998.0400. [DOI] [PubMed] [Google Scholar]
- 59.Pallonen UE, Velicer WF, Prochaska JO, Rossi JS, Bellis JM, Tsoh JY, Migneault JP, Smith NF, Prokhorov AV. Computer-based smoking cessation interventions in adolescents: Description, feasibility, and six-month follow-up findings. Subst Use Misuse. 1998;33:935–965. doi: 10.3109/10826089809056250. [DOI] [PubMed] [Google Scholar]
- 60.Rimer BK, Orleans CT, Fleisher L, Cristinzio S. Does tailoring matter? The impact of a tailored guide on ratings and short-term smoking-related outcomes for older smokers. Health Educ Res. 1994;9:69–84. doi: 10.1093/her/9.1.69. [DOI] [PubMed] [Google Scholar]
- 61.Shegog R, McAlister AL, Hu S, Ford KC, Meshack AF, Peters RJ. Use of interactive health communication to affect smoking intentions in middle school students: A pilot test of the “Headbutt” risk assessment program. Am J Health Promot. 2005;19:334–338. doi: 10.4278/0890-1171-19.5.334. [DOI] [PubMed] [Google Scholar]
- 62.Shiffman S, Rolf CN, Hellebusch SJ, Gorsline J, Gorodetzky CW, Chiang Y-K, Schleusener DS, Di Marino ME. Real-world efficacy of prescription and over-the-counter nicotine replacement therapy. Addiction. 2002;97:505–516. doi: 10.1046/j.1360-0443.2002.00141.x. [DOI] [PubMed] [Google Scholar]
- 63.Stoddard JL, Delucchi KL, Munoz RF, Collins NM, Perez Stable EJ, Augustson E, Lenert LL. Smoking cessation research via the internet: A feasibility study. J Health Commun. 2005;10:27–41. doi: 10.1080/10810730590904562. [DOI] [PubMed] [Google Scholar]
- 64.Wang J, Etter J-Fo. Administering an effective health intervention for smoking cessation online: The international users of Stop-Tabac. Prev Med. 2004;39:962–968. doi: 10.1016/j.ypmed.2004.03.038. [DOI] [PubMed] [Google Scholar]
- 65.Webb MS, Simmons VN, Brandon TH. Tailored interventions for motivating smoking cessation: Using placebo tailoring to examine the influence of expectancies and personalization. Health Psychol. 2005;24:179–188. doi: 10.1037/0278-6133.24.2.179. [DOI] [PubMed] [Google Scholar]
- 66.Wiggers LCW, Oort FJ, Dijkstra A, de Haes JCJM, Legemate DA, Smets EMA. Cognitive changes in cardiovascular patients following a tailored behavioral smoking cessation intervention. Prev Med. 2005;40:812–821. doi: 10.1016/j.ypmed.2004.09.028. [DOI] [PubMed] [Google Scholar]
- 67.Velicer WF, Prochaska JO. An expert system intervention for smoking cessation. Patient Educ Couns. 1999;36:119–129. doi: 10.1016/s0738-3991(98)00129-3. [DOI] [PubMed] [Google Scholar]
- 68.Butler SF, Chiauzzi E, Bromberg JI, Budman SH, Buono DP. Computer-assisted screening and intervention for alcohol problems in primary care. J Technol Human Serv. 2003;21:1–19. [Google Scholar]
- 69.Kypri K, Saunders JB, Williams SM, McGee RO, Langley JD, Cashell-Smith ML, Gallagher SJ. Web-based screening and brief intervention for hazardous drinking: A double-blind randomized controlled trial. Addiction. 2004;99:1410–1417. doi: 10.1111/j.1360-0443.2004.00847.x. [DOI] [PubMed] [Google Scholar]
- 70.McDonald EM, Solomon B, Shields W, Serwint JR, Jacobsen H, Weaver NL, Kreuter M, Gielen AC. Evaluation of kiosk-based tailoring to promote household safety behaviors in an urban pediatric primary care practice. Patient Educ Couns. 2005;58:168–181. doi: 10.1016/j.pec.2004.08.015. [DOI] [PubMed] [Google Scholar]
- 71.Nansel TR, Weaver N, Donlin M, Jacobsen H, Kreuter MW, Simons-Morton B. Baby, Be Safe: The effect of tailored communications for pediatric injury prevention provided in a primary care setting. Patient Educ Couns. 2002;46:175–190. doi: 10.1016/s0738-3991(01)00211-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Reubsaet A, Brug J, Kitslaar J, van Hooff JP, van den Borne HW. The impact and evaluation of two school-based interventions on intention to register an organ donation preference. Health Educ Res. 2004;19:447–456. doi: 10.1093/her/cyg060. [DOI] [PubMed] [Google Scholar]
- 73.Nicholson R, Nash J, Andrasik F. A self-administered behavioral intervention using tailored messages for migraine. Headache. 2005;45:1124–1139. doi: 10.1111/j.1526-4610.2005.00236.x. [DOI] [PubMed] [Google Scholar]
- 74.Wilkie DJ, Huang H-Y, Berry DL, Schwartz A, Lin Y-C, Ko N-Y, Chen A, Gralow J, Lindsley SK, Fitzgibbon D. Cancer symptom control: Feasibility of a tailored, interactive computerized program for patients. Fam Community Health. 2001;24:48–62. [PubMed] [Google Scholar]
- 75.Kreuter MW, Strecher VJ. Changing inaccurate perceptions of health risk: Results from a randomized trial. Health Psychol. 1995;14:56–63. doi: 10.1037//0278-6133.14.1.56. [DOI] [PubMed] [Google Scholar]
- 76.Emmons KM, Wong M, Puleo E, Weinstein N, Fletcher R, Colditz G. Tailored computer-based cancer risk communication: Correcting colorectal cancer risk perception. J Health Commun. 2004;2 doi: 10.1080/10810730490425295. [DOI] [PubMed] [Google Scholar]
- 77.Kreuter MW, Skinner CS, Steger-May K, Holt CL, Bucholtz DC, Clark EM, Haire-Joshu D. Responses to behaviorally vs culturally tailored cancer communication among African American women. Am J Health Behav. 2004;28:195–197. doi: 10.5993/ajhb.28.3.1. [DOI] [PubMed] [Google Scholar]
- 78.Marcus AC, Mason M, Wolfe P, Rimer BK, Lipkus I, Strecher V, Warneke R, Morra ME, Allen AR, Davis SW, Gaier A, Graves C, Julesberg K, Nguyen L, Perocchia R, Speyer JB, Wagner D, Thomsen C, Bright MA. The efficacy of tailored print materials in promoting colorectal cancer screening: Results from a randomized trial involving callers to the national cancer institute’s cancer information service. J Health Commun. 2005;10:83–104. doi: 10.1080/10810730500257754. [DOI] [PubMed] [Google Scholar]
- 79.de Nooijer J, Lechner L, de Vries H. Tailored versus general information on early detection of cancer: A comparison of the reactions of Dutch adults and the impact on attitudes and behaviors. Health Educ Res. 2002;17:239–252. doi: 10.1093/her/17.2.239. [DOI] [PubMed] [Google Scholar]
- 80.Bellis JM, Grimley DM, Alexander LR. Feasibility of a tailored intervention targeting STD-related behaviors. Am J Health Behav. 2002;26:378–385. doi: 10.5993/ajhb.26.5.6. [DOI] [PubMed] [Google Scholar]
- 81.Chesney MA, Koblin BA, Barresi PJ, Husnik MJ, Celum CL, Colfax G, Mayer K, McKirnan D, Judson FN, Huang Y, Coates TJ. An individually tailored intervention for HIV prevention: Baseline data from the EXPLORE study. Am J Pub Health. 2003;93:933–938. doi: 10.2105/ajph.93.6.933. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82.Scholes D, McBride CM, Grothaus L, Civic D, Ichikawa LE, Fish LJ, Yarnall KSH. A tailored minimal self-help intervention to promote condom use in young women: Results from a randomized trial. AIDS. 2003;17:1547–1556. doi: 10.1097/00002030-200307040-00016. [DOI] [PubMed] [Google Scholar]
- 83.Evers KE, Prochaska JO, Johnson JL, Mauriello LM, Padula JA, Prochaska JM. A randomized clinical trial of a population- and transtheoretical model-based stress-management intervention. Health Psychol. 2006;25:521–529. doi: 10.1037/0278-6133.25.4.521. [DOI] [PubMed] [Google Scholar]
- 84.Bernhardt JM. Tailoring messages and design in a web-based skin cancer prevention intervention. Internat Electr J Health Educ. 2001;4:290–297. [Google Scholar]
- 85.Hornung RL, Lennon PA, Garrett JM, DeVellis RF, Weinberg PD, Strecher VJ. Interactive computer technology for skin cancer prevention targeting children. Am J Prev Med. 2000;18:69–76. doi: 10.1016/s0749-3797(99)00115-4. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.