

Abstract
With aging, individuals' gaits become slower and their steps shorter; both are thought to improve stability against balance threats. Recent studies have shown that shorter step lengths, which bring the center of mass (COM) closer to the leading foot, improve stability against slip-related falls. However, a slower gait, hence lower COM velocity, does the opposite. Due to the inherent coupling of step length and speed in spontaneous gait, the extent to which the benefit of shorter steps can offset the slower speed is unknown. The purpose of this study was to investigate, through decoupling, the independent effects of gait speed and step length on gait stability and the likelihood of slip-induced falls. Fifty-seven young adults walked at one of three target gait patterns, two of equal speed and two of equal step length; at a later trial, they encountered an unannounced slip. The results supported our hypotheses that faster gait as well as shorter steps each ameliorates fall risk when a slip is encountered. This appeared to be attributable to the maintenance of stability from slip initiation to liftoff of the recovery foot during the slip. Successful decoupling of gait speed from step length reveals for the first time that, although slow gait in itself leads to instability and falls (a one-standard-deviation decrease in gait speed increases the odds of fall by 4 fold), this effect is offset by the related decrease in step length (the same one-standard-deviation decrease in step length lowers fall risk by 6 times).
Keywords: spontaneous gait, decoupling, audiovisual cuing, foot landing orientation, gait parameters
Introduction
Falls often lead to injuries, declines in mobility, and self imposed limitations on daily activities and socialization [1, 2]. Among older adults, falls resulting from slipping are associated with hip fractures [3] and their accompanying complications and mortality [4]. Aging related changes in various systems involved in perturbation response have been implicated in the higher rates and severity of falls among the elderly. Examples include age related changes in coordination [5, 6], increased onset times for various muscle groups [7, 8], increases in joint stiffness, and decreases in isometric muscle strength [9].
With age, gait speed becomes slower and step lengths shorter [10]. It is not clear whether these changes result from the aging process or from a fear of falling, or both [11]. The evidence is contradictory as to whether either gait modification is in fact safer or more stable. Slower gaits have been shown to be directly associated with an increased fall risk [12, 13], and are correlated with lower scores on clinical balance scales [14]. Several lines of research have proposed that a more quickly moving center of mass (COM), due to faster gait, may travel forward more effectively to “catch up” with the slipping base of support (BOS) [15, 16]. Young and older adults spontaneously shorten their step lengths in response to a known slippery floor [17], and longer steps have been associated with a greater slip probability [18]. Findings indicate that shorter steps should be more stable because the COM is closer to the moving BOS [15]. However, Menz et al suggested that, “step length shortening may be maladaptive” [19].
Stability can be measured as the shortest distance between the COM motion state (i.e., its position and velocity relative to the BOS) and a mathematically derived stability threshold [20]. Negative stability values (below the threshold) predict a backward balance loss [21] and are associated with falls [22]. Both a more anterior COM position, through forward leaning of the trunk and/or shortened steps [21], and a faster COM velocity, from increased gait speed, move the motion state toward the boundary, improving stability. Hence, shorter step lengths and faster gait speeds should enhance stability. This appears to be true only in the early instances of a slip. In a slip induced during self-selected fast, natural, or slow gaits, velocity was strongly correlated with stability at slipping foot touchdown (TD), such that faster gaits had higher stability; however, these differences diminished through the recovery response [15]. The degree to which this recovery response depends upon the gait parameters prior to slip onset is unknown [15].
The independent influence of speed and step length on control of stability by liftoff of the recovery step (LO), and their impact on fall risk cannot be ascertained in spontaneous gait because of their inherent coupling: slower speeds have shorter steps and faster gaits have longer steps. It is necessary to “decouple” these parameters by controlling both. Although there is precedence for modulating one gait parameter at a time during walking, it is rare that two parameters are controlled simultaneously [23], particularly in the context of stability or fall risk.
The purpose of this study was to investigate, through decoupling, the independent effects of gait speed and step length on gait stability and the likelihood of slip-induced falls. In order to decouple spontaneous gait, our experimental design was to control two gait parameters simultaneously, whereby the third would be determined per force. Such manipulation would enable us to test the hypothesis that increasing gait speed or decreasing step length would each, independently, positively influence stability from slipping foot touchdown to liftoff of the recovery foot, and hence lessen the likelihood of a fall.
Methods
Subjects
Fifty-seven subjects, 19–45 years old, were randomly assigned to one of three target groups (Table 1). Subjects were screened for systemic disorders which might affect their participation and gave informed consent as approved by the local Institutional Review Board.
Table 1.
Subject demographics, and target and resultant gait parameters, by group.
| Group | N | Female | Age (yrs) Mean (SD) |
Height (m) Mean (SD) |
Weight (kg) Mean (SD) |
Target Step Length (/bh) | Resultant Step Length (/bh) Mean (SD) |
Target Gait Speed* | Resultant Gait Speed* Mean (SD) |
|---|---|---|---|---|---|---|---|---|---|
| A | 19 | 8 | 28.9 (6.9) | 1.7 (0.1) | 69.2 (14.9) | 0.434 | .433 (.035) | 0.4** | .396 (.039) |
| B | 18 | 11 | 24.3 (4.9) | 1.7 (0.1) | 65.4 (13.5) | 0.301 | .309 (.027) | 0.2 | .203 (.017) |
| C | 20 | 14 | 24.9 (5.1) | 1.7 (0.2) | 68.0 (12.6) | 0.434 | .422 (.027) | 0.2 | .204 (.013) |
This is a dimensionless measure: sacral velocity normalized by where g is the acceleration due to gravity and bh is the subject's body height.
Target for the initial 8 subjects was 0.47; analysis revealed that the subjects could not consistently reach this target, so the target was adjusted to 0.4 for the remaining 11 subjects.
Experimental set up and protocol
Subjects matched, simultaneously, their walking speed to target flags along a moving rope loop and their steps to an audible metronome (Fig. 1, [24]). The rope loop was driven at the target speed by a DC motor (Model 4Z248D, Dayton Electric, Niles, IL). Since gait speed is the product of step length and cadence, this targeted the desired step length as well. Subjects were informed before beginning that they may be slipped “later”. At right touchdown (TD) of selected trials, data from the sacral marker and the heel markers were used to estimate gait speed and step length respectively. These were used to provide verbal error feedback and to assess target matching, deemed successful if subjects were within 10% of the target value [24]. All subjects wore a safety harness attached by shock absorbing ropes to a low friction trolley on an I-beam above the walkway. A load cell recorded forces exerted through the ropes at 600 Hz. Within two trials of target matching, an unannounced slip was induced under the right foot by pre-releasing a movable, locking platform embedded in the walkway. This platform could slide freely up to 150 cm (coefficient of friction < 0.05) and was supported by force plates (AMTI, Newton, MA) recording ground reaction forces (GRF) at 600 Hz.
Figure 1.
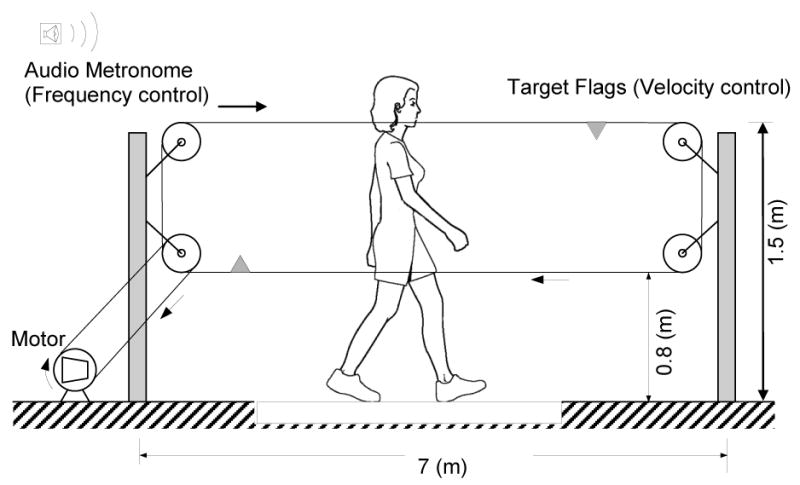
Experimental set up for target presentation during walking. Subjects matched gait speed (V) and step frequency (SF) targets simultaneously while walking along a 7 m walkway. Gait speed target was provided by flags attached to a rope loop running parallel to the length of the walkway and being driven at a constant velocity by a motor. Step frequency was provided by an audible metronome. Step length (SL) was also constrained because V = SL*SF.
Three sets of gait parameters were designed so that groups B and C should have the same gait speed but different step lengths, and A and C should have the same step length, but different gait speeds; C comprised the theoretically least stable combination, to serve as a comparison against the parameters of A and B (Table 1). These targets were designed such that the predicted resultant COM motion states of all three would lie below the stability threshold at slipping limb TD [20, 24].
Data analyses
The kinematics of 27 markers attached to body segment landmarks and the platform were recorded by a motion capture system at 120 Hz (Motion Analysis Corporation, Santa Rosa, CA). Marker paths were low-pass filtered at marker-specific frequencies (range 4.5-9 Hz) using zero-lag, fourth-order Butterworth filters. Locations of joint centers were computed from the marker paths based on anthropometric data and the COM kinematics were computed using known sex-dependent segmental parameters in a 13-segment representation of the body [25]. Slipping step TD and recovery foot liftoff (LO) were identified from the vertical GRF. For each first slip TD, step length and gait speed, normalized to body height, were calculated as above. The COM position (XCOM/BOS) and forward velocity (VCOM/BOS) relative to the base of support (BOS, the slipping heel), at TD and LO, were expressed as a fraction of foot length (lBOS) and , respectively, where g is the acceleration of gravity and bh the subject's height. Stability was calculated as the shortest distance from the instantaneous COM motion state (XCOM/BOS and VCOM/BOS) to the stability threshold [26] at both gait events, TD and LO. One subject in group A was excluded from analyses derived from motion data due to missing markers.
A recovery step was one in which the trailing heel landed behind the slipping heel; an aborted step was characterized by unloading, then re-loading the trailing foot, after slip initiation but before complete unloading [15]. Both constituted a backward balance loss. For an aborted step, LO time was taken as the instant of the minimum vertical GRF during the unload/re-load period. A fall occurred if the maximum force exerted on the load cell exceeded 30% body weight after slip onset [22].
The extent to which the gait parameters of each group met the design criteria was tested using one way analysis of variance (ANOVA). Changes in stability (Δs) from TD to LO (event) were examined using a 3 (groups, inter-subject factor) × 2 (events, intra-subject factor) repeated measures ANOVA. Post hoc analyses were done by Tukey's HSD statistics and paired t-tests with appropriate Bonferroni corrections. Linear regression, with gait speed and step length entered stepwise as factors, was used to assess the impact of the gait parameters on Δs. Differences in loss of balance and falls incidence among the groups were assessed with Chi square (χ2). Logistic regression with gait speed and step length as factors was used to assess the impact of each on falls outcomes; odds ratios for falls were calculated based on this. Post hoc analysis was performed to examine whether pre-slip joint angles of the slipping limb would increase the predictive value for falls of this logistic regression. Statistics were performed with SPSS 17.0 (Chicago, IL) with α of 0.05, unless otherwise noted.
Results
Changes from TD to LO
The resultant mean gait speeds and step lengths of the three groups met the design criteria (Table 2). The COM stability differed significantly among the 3 groups at TD and LO (main effect: F2,53=89.38, P<.001, Fig 2). Group A was more stable than B, which was more stable than C at TD (all P<.001), and at LO (all P<.001). There was a significant event (TD vs. LO) effect (F1,53=23.27, P<.001) and group by event interaction effect for stability (F2,53=6.24, P=.004). Stability for groups A and B remained nearly unchanged from TD to LO (P>0.10 for both). In contrast, group C's stability deteriorated significantly during this period (P<.001) (Fig. 2). Regression analysis predicting change in stability from step length and gait speed [Δs=.229GS-.901SL+.127 (R2=.266, P<.001)], showed that a decrease of one unit in normalized step length resulted in an increase in Δs during the initial slip response by .901, whereas a one unit increase in normalized gait speed yielded an increase of only .229.
Table 2.
Step length, gait speed, and ratio of step length to gait speed for the three experimental groups and for groups with selected characteristics, reported in the literature.
| Sample | Step Length/bh | Gait Speed/bh | Gait Speed/Step length |
|---|---|---|---|
| Group A | .433 (.035)† | .949 (.107)** | 2.18 |
| Group B | .309 (.027)** | .493 (.047)† | 1.59 |
| Group C | .422(.027)† | .490 (.035)† | 1.16 |
| Fearful [11] §§ | 0.301 | 0.545 | 1.81 |
| Fearless [11] §§ | 0.403 | 0.78 | 1.94 |
| Fallers [30] | 0.297 | 0.539 | 1.82 |
| Non-fallers [30] | 0.374 | 0.742 | 1.98 |
| Disabled [31] | 0.347 | 0.65 | 1.87 |
| Healthy [31] | 0.366 | 0.706 | 1.93 |
| Transition to Frail [32] | 0.345 | 0.602 | 1.75 |
Step length is the distance between the heel markers and gait speed is the velocity of the sacral marker, both at slipping foot touchdown and both normalized to body height. Gait speed is the ratio of gait speed to step length.
B vs. A (P<.001) and B vs. C (P<.001) for step length, or A vs. B (P<.001) and A vs. C (P<.001) for speed.
C vs. A (P=.443) and B vs. C (P=.999)
For references in which gait parameters had been presented in absolute terms, the absolute values were divided by the stated average body height for that group.
In this study, no anthropometrics were available; body height of 1.624 m (average among these other studies) was used for normalization.
Figure 2.

Left Panel Mean center of mass (COM) motion state values (XCOM/BOS and VCOM/BOS) for groups A, B, and C at slipping foot touchdown (TD) (solid shapes), relative to stability threshold for backward loss of balance (thick black curve), and at trailing foot liftoff (LO) (open shapes) with error bars showing ±1 SD. Thin lines trace one representative COM motion state trajectory from TD to LO for each group.
Right panel: Mean stability value of each target group at TD (solid symbols) and LO (open symbols). Error bars in both panels represent ±1 SD.
Outcomes
The incidence of backward balance loss was similar among the 3 groups (χ2=2.036, P=.580): all subjects in groups B and C and 18 of 19 in A lost their balance. However, group C experienced more falls (χ2=9.218, P=.01): 6 of 20 in group C fell versus 1 of 19 in A, (χ2=4.048,P=.044), or 0 of 18 in B, (χ2=6.413,P=.011). Logistic regression analysis revealed that gait speed (χ2=4.214, P=.04) and step length (χ2=4.651, P=.031) were each strongly associated with falls. The ability of this regression model to predict falls (89.3%) was improved by only 2% with the addition of the slipping limb foot orientation and hip, knee, and ankle angle. A one-standard-deviation increase in step length conferred a 6.05 times higher odds of fall (95% CI=12.03 to 4.2E+22); while a one-standard-deviation decrease in gait speed increased the odds of fall by only 4.06 fold (95% CI=.000 to .754).
Discussion
The successful decoupling of gait speed from step length has enabled us to investigate the independent influence of each on fall risk and stability during an initial slip recovery response. Notably, step length shortening and increasing gait speed each resulted in maintenance of stability from slip onset to recovery step liftoff. More importantly, each reduced subsequent fall risk, with step length modification having at the very least a comparable if not stronger influence.
Stability typically deteriorates from the onset of an unannounced, novel slip to recovery foot liftoff in gait [15, 21]. The stability of all three groups in this study remained negative from slip onset (about 25 ms after touchdown) to liftoff, but only group C experienced a decline in stability during this period. Groups A and B, each with a different more stable component to bring the COM motion state closer to the stability limits, avoided rapid deterioration of stability. In slips during regular, self-selected gait, speed and step length appeared to affect stability differently through the recovery response: faster gait had the advantage at slip onset; however, short step lengths both moved the COM closer to the slipping base of support, and partially compensated for the slow speed related instability from onset to recovery foot liftoff through a reduced push-off and resulting shorter recovery step [15].
Studies have shown that the response to an unannounced slip, particularly at recovery foot liftoff, is crucial to balance recovery [15, 16]. The deterioration in stability by liftoff provides an important clue about the higher incidence of falls in Group C. Later in the recovery response, prior to recovery foot touchdown, instability combined with poor limb support accounted for nearly 90% of falls in gait-slip, and 100% in sit-to-stand-slip [22]. Recovery step length is often scaled to the overall gait step length, with a longer step during unperturbed walking leading to a longer recovery step upon a novel slip [21], likely bringing the recovery foot landing more closely behind the COM, hence causing a small base of support with worse stability against backward balance loss. Finally, longer step lengths in regular gait would lead to lower hip heights at recovery liftoff, adding additional support challenges for the slipping limb against collapse during that period [22].
In addition to the three primary global gait parameters, speed, step length and cadence, other parameters, such as step width and its variability have been associated with differences in fall risk or fall history [27]. Various pre-slip, local gait parameters such as hip, knee or ankle angles, and particularly foot orientation at heel strike, have also been shown to be associated with perturbation intensity and slip outcomes [21]. In the present study, these local parameters of unperturbed gait did little (∼2%) to improve fall risk prediction beyond the three primary gait parameters.
A wide range of spontaneous gait parameter values are reported for various groups of older adults (Fig. 3, Table 2). In anticipation of a slip, for instance in icy weather, people may intentionally alter their gait pattern to one they perceive as safer [17]. However, the results of this study indicate that the shortened step length inherent in the spontaneous gait of older adults must ameliorate fall risk rather than contribute to it. Based on the present study, the shorter step lengths that accompany aging, and even more so many typical impairments, would lower the odds of falling in response to a slip, but the slower speed would have the opposite effect against slip-induced falls. In some cases, the advantage of the shortened steps can outweigh the heightened risk of the slower speed. For instance, adaptation to slips was better represented by reductions in step length than in gait speed, which remained mostly unchanged [21]. However, for the groups cited here, the ratio of gait speed to step length was less than that of the healthy older adults (Table 2). These groups have reduced their gait speed proportionally more than their step length versus their healthier counterparts, thus increasing their fall risk overall.
Figure 3.

Normalized (to body height) gait speeds and step lengths as reported in the literature for elderly adults with various sample characteristics (open and/or line shapes) and target gait parameter results for the three experimental groups of this study (solid shapes). For references in which only absolute gait parameter values were given, results were divided by the stated average body height for that group. * In this case, no anthropometrics were given; a value of 1.624 (average of body heights reported among these other studies) was used to normalize the absolute parameters. Data presented are from the following studies: fearful and fearless [11, Chamberlin ME, Fulwider BD, Sanders SL, Medeiros JM: Does fear of falling influence spatial and temporal gait parameters in elderly persons beyond changes associated with normal aging? J Gerontol A Biol Sci Med Sci 2005;60:1163-1167.], fallers and non-fallers [30, Kerrigan DC, Lee LW, Nieto TJ, Markman JD, Collins JJ, Riley PO: Kinetic alterations independent of walking speed in elderly fallers. Arch Phys Med Rehabil 2000;81:730-735.], disabled and healthy [31, McGibbon CA, Krebs DE: Discriminating age and disability effects in locomotion: neuromuscular adaptations in musculoskeletal pathology. J Appl Physiol 2004;96:149-160.], frail [32, Kressig RW, Gregor RJ, Oliver A, Waddell D, Smith W, O'Grady M, Curns AT, Kutner M, Wolf SL: Temporal and spatial features of gait in older adults transitioning to frailty. Gait Posture 2004;20:30-35.]
Age-related differences and the artificial nature of the gait patterns of this study mandate caution in generalizing these findings. Nonetheless, these slower speeds (groups B and C) and shorter step lengths (B), and faster velocity (A) and longer step lengths (A and C) do encompass the range of gait parameters observed among older adults (Fig. 3). Further, among young adults, intentionally walking at much slower than typical speeds induces changes similar to those seen in aging gait [28]. The potentially disruptive nature of walking at slower than normal speeds may predispose individuals to difficulty maintaining balance [29]; thus, groups B and C may theoretically have had a greater risk of loss of balance. Yet, despite having similar, very slow walking speeds, group B had no falls, while group C did. Based on the COM motion state derived stability measure, group B was more stable and group C less so, which is primarily attributable to a shorter step, as revealed by this set of experiments [24].
Other limitations of the study include the possibility that simultaneous matching of two targets constitutes a high cognitive load secondary task which could have impacted the subjects' slip responses in unforeseen ways. However, this confounding variable was imposed on all subjects, so its effect would have been similar across groups. Finally, this study represents an attempt to address the dilemma that spontaneous gait patterns are coupled and, therefore, not suitable to decipher the independent impact of each parameter. Inevitably, decoupled gait patterns are, by design, different from those that would be chosen spontaneously; these results are artificial in this respect.
In summary, successful decoupling of gait speed from step length reveals that, although slow gait in itself leads to instability and falls, this is offset by the related decrease in step length. These findings are indicative of an intervention strategy focusing on modulation of gait speed (faster) without necessarily increasing step length, and they provide empirical evidence for further studies to verify these observations in each population and for computer simulations in which the confounding factors associated with the spontaneous coupling between gait parameters could be controlled mathematically.
Acknowledgments
This work was funded by NIH 2R01-AG16727 (YCP). The authors thank Junyi Sun and Ting-yun Wang for assisting in data collection and processing, and Edward Wang, PhD, for statistical consultation.
Footnotes
Conflict of Interest Statement: The study sponsors had no involvement in the study design, execution, or manuscript preparation. There is no conflict of interest for any of the authors.
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- 1.Li F, Fisher KJ, Harmer P, McAuley E, Wilson NL. Fear of falling in elderly persons: association with falls, functional ability, and quality of life. J Gerontol B Psychol Sci Soc Sci. 2003;58:P283–290. doi: 10.1093/geronb/58.5.p283. [DOI] [PubMed] [Google Scholar]
- 2.Hausdorff JM, Edelberg HK, Mitchell SL, Goldberger AL, Wei JY. Increased gait unsteadiness in community-dwelling elderly fallers. Arch Phys Med Rehabil. 1997;78:278–283. doi: 10.1016/s0003-9993(97)90034-4. [DOI] [PubMed] [Google Scholar]
- 3.Smeesters C, Hayes WC, McMahon TA. Disturbance type and gait speed affect fall direction and impact location. J Biomech. 2001;34:309–317. doi: 10.1016/s0021-9290(00)00200-1. [DOI] [PubMed] [Google Scholar]
- 4.Englander F, Hodson TJ, Terregrossa RA. Economic dimensions of slip and fall injuries. J Forensic Sci. 1996;41:733–746. [PubMed] [Google Scholar]
- 5.McGibbon CA, Krebs DE. Age-related changes in lower trunk coordination and energy transfer during gait. J Neurophysiol. 2001;85:1923–1931. doi: 10.1152/jn.2001.85.5.1923. [DOI] [PubMed] [Google Scholar]
- 6.Byrne JE, Stergiou N, Blanke D, Houser JJ, Kurz MJ, Hageman PA. Comparison of gait patterns between young and elderly women: an examination of coordination. Percept Mot Skills. 2002;94:265–280. doi: 10.2466/pms.2002.94.1.265. [DOI] [PubMed] [Google Scholar]
- 7.Lockhart TE, Kim S. Relationship between hamstring activation rate and heel contact velocity: factors influencing age-related slip-induced falls. Gait Posture. 2006;24:23–34. doi: 10.1016/j.gaitpost.2005.06.016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Tirosh O, Sparrow WA. Age and walking speed effects on muscle recruitment in gait termination. Gait Posture. 2005;21:279–288. doi: 10.1016/j.gaitpost.2004.03.002. [DOI] [PubMed] [Google Scholar]
- 9.Goldberg EJ, Neptune RR. Compensatory strategies during normal walking in response to muscle weakness and increased hip joint stiffness. Gait Posture. 2007;25:360–367. doi: 10.1016/j.gaitpost.2006.04.009. [DOI] [PubMed] [Google Scholar]
- 10.Laufer Y. Effect of age on characteristics of forward and backward gait at preferred and accelerated walking speed. J Gerontol A Biol Sci Med Sci. 2005;60:627–632. doi: 10.1093/gerona/60.5.627. [DOI] [PubMed] [Google Scholar]
- 11.Chamberlin ME, Fulwider BD, Sanders SL, Medeiros JM. Does fear of falling influence spatial and temporal gait parameters in elderly persons beyond changes associated with normal aging? J Gerontol A Biol Sci Med Sci. 2005;60:1163–1167. doi: 10.1093/gerona/60.9.1163. [DOI] [PubMed] [Google Scholar]
- 12.Cromwell RL, Newton RA. Relationship between balance and gait stability in healthy older adults. J Aging Phys Act. 2004;12:90–100. doi: 10.1123/japa.12.1.90. [DOI] [PubMed] [Google Scholar]
- 13.Ness KK, Gurney JG, Ice GH. Screening, education, and associated behavioral responses to reduce risk for falls among people over age 65 years attending a community health fair. Phys Ther. 2003;83:631–637. [PubMed] [Google Scholar]
- 14.Coppin AK, Shumway-Cook A, Saczynski JS, Patel KV, Ble A, Ferrucci L, Guralnik JM. Association of executive function and performance of dual-task physical tests among older adults: analyses from the InChianti study. Age Ageing. 2006;35:619–624. doi: 10.1093/ageing/afl107. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Bhatt T, Wening JD, Pai YC. Influence of gait speed on stability: recovery from anterior slips and compensatory stepping. Gait Posture. 2005;21:146–156. doi: 10.1016/j.gaitpost.2004.01.008. [DOI] [PubMed] [Google Scholar]
- 16.You J, Chou Y, Lin C, Su F. Effect of slip on movement of body center of mass relative to base of support. Clin Biomech (Bristol, Avon) 2001;16:167–173. doi: 10.1016/s0268-0033(00)00076-0. [DOI] [PubMed] [Google Scholar]
- 17.Cham R, Redfern MS. Changes in gait when anticipating slippery floors. Gait Posture. 2002;15:159–171. doi: 10.1016/s0966-6362(01)00150-3. [DOI] [PubMed] [Google Scholar]
- 18.Moyer BE, Chambers AJ, Redfern MS, Cham R. Gait parameters as predictors of slip severity in younger and older adults. Ergonomics. 2006;49:329–343. doi: 10.1080/00140130500478553. [DOI] [PubMed] [Google Scholar]
- 19.Menz HB, Lord SR, Fitzpatrick RC. Acceleration patterns of the head and pelvis when walking on level and irregular surfaces. Gait Posture. 2003;18:35–46. doi: 10.1016/s0966-6362(02)00159-5. [DOI] [PubMed] [Google Scholar]
- 20.Pai YC, Patton J. Center of mass velocity-position predictions for balance control. J Biomech. 1997;30:347–354. doi: 10.1016/s0021-9290(96)00165-0. [DOI] [PubMed] [Google Scholar]
- 21.Bhatt T, Wening JD, Pai YC. Adaptive control of gait stability in reducing slip-related backward loss of balance. Exp Brain Res. 2006;170:61–73. doi: 10.1007/s00221-005-0189-5. [DOI] [PubMed] [Google Scholar]
- 22.Yang F, Bhatt T, Pai YC. Role of stability and limb support in recovery against a fall following a novel slip induced in different daily activities. J Biomech. 2009;42:1903–1908. doi: 10.1016/j.jbiomech.2009.05.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Danion F, Varraine E, Bonnard M, Pailhous J. Stride variability in human gait: the effect of stride frequency and stride length. Gait Posture. 2003;18:69–77. doi: 10.1016/s0966-6362(03)00030-4. [DOI] [PubMed] [Google Scholar]
- 24.Espy DD, Yang F, Pai YC. Control of center-of-mass motion state through cuing and decoupling of spontaneous gait parameters in level walking. J Biomech. 2010 doi: 10.1016/j.jbiomech.2010.05.015. in press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.de Leva P. Adjustments to Zatsiorsky-Seluyanov's segment inertia parameters. J Biomech. 1996;29:1223–1230. doi: 10.1016/0021-9290(95)00178-6. [DOI] [PubMed] [Google Scholar]
- 26.Pai YC. Movement termination and stability in standing. Exerc Sport Sci Rev. 2003;31:19–25. doi: 10.1097/00003677-200301000-00005. [DOI] [PubMed] [Google Scholar]
- 27.Brach JS, Berlin JE, VanSwearingen JM, Newman AB, Studenski SA. Too much or too little step width variability is associated with a fall history in older persons who walk at or near normal gait speed. J Neuroeng Rehabil. 2005 Jul 26;2:21. doi: 10.1186/1743-0003-2-21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Ferrandez AM, Pailhous J, Durup M. Slowness in elderly gait. Exp Aging Res. 1990 Spring-Summer;16(1-2):79–89. doi: 10.1080/07340669008251531. [DOI] [PubMed] [Google Scholar]
- 29.Brach JS, Berthold R, Craik R, VanSwearingen JM, Newman AB. Gait variability in community-dwelling older adults. J Am Geriatr Soc. 2001 Dec;49(12):1646–50. doi: 10.1046/j.1532-5415.2001.t01-1-49274.x. [DOI] [PubMed] [Google Scholar]
- 30.Kerrigan DC, Lee LW, Nieto TJ, Markman JD, Collins JJ, Riley PO. Kinetic alterations independent of walking speed in elderly fallers. Arch Phys Med Rehabil. 2000;81:730–735. doi: 10.1016/s0003-9993(00)90101-1. [DOI] [PubMed] [Google Scholar]
- 31.McGibbon CA, Krebs DE. Discriminating age and disability effects in locomotion: neuromuscular adaptations in musculoskeletal pathology. J Appl Physiol. 2004;96:149–160. doi: 10.1152/japplphysiol.00422.2003. [DOI] [PubMed] [Google Scholar]
- 32.Kressig RW, Gregor RJ, Oliver A, Waddell D, Smith W, O'Grady M, Curns AT, Kutner M, Wolf SL. Temporal and spatial features of gait in older adults transitioning to frailty. Gait Posture. 2004;20:30–35. doi: 10.1016/S0966-6362(03)00089-4. [DOI] [PubMed] [Google Scholar]