

Abstract
Purpose
Presented here is a retrospective clinical audit of clubfoot patients to determine the value of the Pirani clubfoot scoring system at initial presentation in the estimation of subsequent relapse.
Methods
All clubfoot patients treated by the same surgeon from 2002 to 2006 were included. The treatment adhered to the standard protocol, involving weekly stretching and casting until the foot was corrected, followed by Achilles tenotomy and plasters for 3 weeks. Thereafter, the child was placed in a foot abduction splint. The severity of clubfoot was assessed using the Pirani scoring system, consisting of two sub-scores—the midfoot contracture score (MFCS) and the hindfoot contracture score (HFCS). The MFCS and HFCS can each be 0.0–3.0, giving rise to a total Pirani score (TPS) of 0.0–6.0. Any recurrent deformity was classed as a relapse.
Results
Sixty-one clubfoot patients were treated. Five patients were lost to follow-up and six patients were excluded due to the presence of identified syndromes or having had primary treatment elsewhere. A total of 80 clubfeet were included. There were 17 relapses. The average interval between the initiation of foot abduction splint and relapse was 23 months. The median TPS was 3.5 in the no relapse group and 5.0 in the relapse group. The median MFCS was 1.5 in the no relapse group and 2.0 in the relapse group. The median HFCS was 2.0 in the no relapse group and 3.0 in the relapse group. Higher TPS and HFCS were statistically significant when the relapse group was analysed against the no relapse group (P = 0.05 × 10−4 and 0.02 × 10−4, respectively).
Conclusions
Higher Pirani scores were associated with the late relapse group. The TPS and HFCS were shown to be statistically significant predictors of potential relapse. Closer follow-up is advised for patients at risk of relapse.
Keywords: Clubfoot, Relapse, Pirani score, Ponseti treatment method
Introduction
The clubfoot deformity is characterised by equinus, varus and internal rotation of the os calcis beneath the talus with adductus, cavus and supination of the mid- and forefoot [1] (Fig. 1). There exists a spectrum of severity in terms of both the magnitude and the flexibility of the foot and the most severe deformity usually affects the hind part of the foot [1]. Although extensive operative soft tissue releases were performed to correct the deformity in the past, the current conventionally accepted management is serial stretching and casting described by Ponseti [1]. It is not straightforward to predict the foot’s longer term outcome following manipulations, as this is not only linked to the initial severity of the deformity, but also to the accuracy of reduction and the compliance with the abduction brace [2]. Regardless of the degree of initial correction, the deformity may relapse up until the age of 7 years [1] and there is a 10–56% relapse rate quoted in the literature [3–5]. Therefore, with meticulous management and diligent use of foot abduction orthoses, there is an opportunity to minimise relapses. Integral to this management is the knowledge gained from classification at the initial presentation and the continued long-term follow-up to identify those factors which may be associated with a higher chance of relapse and, therefore, the potential to prevent its occurrence.
Fig. 1.
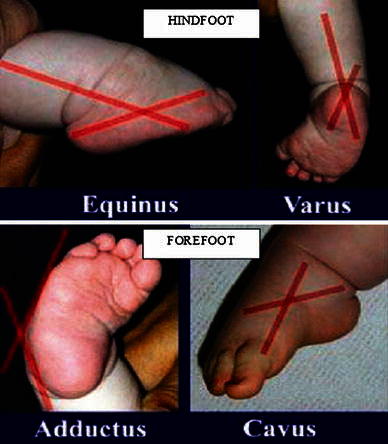
Demonstration of deformities present in clubfoot
The severity of clubfoot may be assessed with a variety of methods, although the Pirani and Diméglio scoring systems are more commonly used [6, 7]. The Pirani score was found to have an excellent record of inter-observer reliability, with a significant correlation coefficient of 0.90 [8] and has been utilised for this study. The Pirani score has been assessed in relation to the number of serial casts required and the need for Achilles tenotomy [9–11] in achieving complete deformity correction. It is well recognised that the more stiff the deformity at the outset, the higher the likelihood of relapse occurring, but we could not find any previous work investigating the association of an initial Pirani score and the rate of subsequent relapse. Therefore, the objective of our study was to determine if the initial Pirani score can be used as a predictor of subsequent relapse.
Materials and methods
This study was part of an ongoing prospective study of all clubfoot patients being treated by the senior author. All patients beginning treatment for clubfoot from 2002 to 2006 were included, with follow-up of 2–6 years (average 57 months). All clubfeet were assessed by the senior author in accordance with the Pirani scoring system on the initial presentation to our institution and annually thereafter. The treatment was conducted by the same surgeon following the standard Ponseti protocol [1].
This involved weekly stretching and long-leg casting until the foot was corrected or until no further correction was possible (Fig. 2). At this stage, either the foot was fully corrected or an Achilles tenotomy under local anaesthetic cream was required to achieve complete correction to at least 15° of dorsiflexion.
Fig. 2.

Serial gentle foot stretches and castings to correct the deformity in a stepwise fashion. First, the cavus deformity is corrected by supination of the forefoot. Then, the adductus deformity of the forefoot is corrected, which simultaneously drives the calcaneus into external rotation in relation to the talus. The varus and equinus posture similarly improves with forefoot correction. No pronation force is applied but the forefoot naturally aligns to the hindfoot. Lastly, the equinus at the ankle is corrected by dorsiflexion of the foot with the heel in valgus and forefoot abducted to 70°. If full dorsiflexion is not possible with stretching alone, an Achilles tenotomy is performed
Occasionally, especially in cases of an atypical clubfoot, a tenotomy is required before the hindfoot corrects to the neutral position to ‘unlock’ the os calcis from beneath the talus [12], followed by further stretching and casting to achieve complete correction. However, in routine cases, the tenotomy enables the final position to be achieved, allowing application of the final cast.
If this approach does not result in complete correction of all components of the deformity, then further intervention is necessary. This involves an assessment of the Achilles tendon to ensure complete transaction has been performed, as in some patients, especially those that have ample fatty tissue, partial section can occur or aberrant fibrous bands have been described [13]. On occasion, a limited posterior ankle capsule release or, rarely, subtalar release may be required to achieve a complete correction. In bilateral clubfeet of different severity, the castings continued until both feet were ready for simultaneous Achilles tenotomy. Once the final position was achieved, a cast was retained for 3 weeks and this final cast was not applied until complete correction was obtained. This can be assessed by accurate clinical examination to ensure that the os calcis has rotated completely beneath the talus by digital palpation beneath the lateral side of the talar head, the tuberosity has filled the heel pad and the ankle dorsiflexion is at least 15°. Full correction equates to a Pirani score of zero and was achieved in all cases. Arguably, there may be a posterior skin crease still visible but nothing more than superficial. The final cast is removed after 3 weeks and, thereafter, the child was placed in a foot abduction brace (FAB) for 23 h daily for 3 months and then at night only for 4 years (Fig. 3). The boots were set at 70° of external rotation on a fixed bar and the distance between the heels matched the distance between the outside of the child’s shoulders.
Fig. 3.

Foot abduction orthosis. The length of the bar is equal to the width of the child’s shoulders. The boot is attached at the end of the bar at 70° external rotation on the affected side and at 40° external rotation on the normal side
Any recurrent deformity occurring after commencement of the foot abduction orthosis that required further active treatment was classed as a relapse. The recurrence was associated with a Pirani score rising above 0. Thus, two groups of patients were identified; those with no relapse and those with relapse requiring treatment. The latter group included even minor loss of position that required further casting, as well as any more interventional procedures. This approach ensures that the foot is placed into the fully corrected position as early as possible once detected to prevent more significant degrees of relapse. Care is needed when comparing other published rates of relapse to ensure that the assessment of relapse is considered in the same way. Re-casting for 2 or 3 weeks with or without Achilles tenotomy to return the foot to normal is far different to surgery for relapse, but the authors believe that this level of vigilance in identifying minor loss of position and classifying it as relapse ensures less intervention in the longer term. This remains the subject of the on-going prospective review from this institution.
The initial severity of clubfoot was assessed using Pirani’s scoring system consisting of two sub-scores—the midfoot contracture score (MFCS) and the hindfoot contracture score (HFCS). The principle of scoring is as follows: 0—no abnormality, 0.5—moderate abnormality, 1—severe abnormality. The MFCS and HFCS can each be 0.0–3.0, giving a total Pirani score (TPS) of 0.0–6.0.
All patients are followed up every 4 months for the first 2 years and every 6 months thereafter. Compliance is important to the success of the treatment protocol, but is notoriously difficult to record accurately [5, 11]. Use of the FAB is encouraged until the child is 4 years of age and to improve compliance, at each visit, the device is checked by a specialist orthotist and any adjustments are made. We believe that this approach gives the best opportunity for maximum use of the FAB. No formal attempt was made to record the exact use of each FAB, as it was considered likely to be too inaccurate to be reliable. The practice of re-casting feet that are showing the initial signs of relapsing minimises the effect of incomplete compliance with the FAB and provides a renewed focus to the parents of the importance of bracing. In some series, these feet may not be classed as having a true relapse and the comparison of data must be made with appropriate attention to this detail.
The statistical method involved directly comparing the two groups using the Wilcoxon two-sample test, as our data was non-parametric with unequal samples. The median was used as a result of our data being of ordinal non-parametric type.
Results
A total of 61 patients with clubfoot were reviewed. Five patients were lost to follow-up and five additional patients had identified syndromes and were excluded. One patient was referred at the age of 6 months having undergone previous treatment elsewhere, and was also excluded. This left a cohort of 50 patients with idiopathic clubfoot (40 male and nine female), 30 of which were bilateral, giving a total of 80 clubfeet. Bilateral clubfeet had the same severity on either side in 21 patients and different severities in nine patients. In the latter group, the maximum difference in severity as assessed by the Pirani score was 1.0. The average age at presentation was 23.2 days, ranging from 2 to 152 days. Five patients (seven clubfeet) were referred from other hospitals, with the average age at presentation being 137 days (range 87–171 days).
Of the 80 feet, 28 (35%) were successfully treated with serial casting alone, 51 (64%) required a primary Achilles tenotomy and one foot needed a limited posterior release to achieve complete correction. Four feet required a further manipulation following Achilles tenotomy. Primary Achilles tenotomy was required in association with a higher TPS and HFCS. Of 51 Achilles tenotomies performed, 18 were in clubfeet with TPS ≥ 5, 17 with TPS ≥ 4 and 16 with TPS < 4. Similarly, the procedure was carried out in 33 clubfeet with HFCS ≥ 2, 12 with HFCS ≥ 1 and six with HFCS < 1. Therefore, TPS ≥ 4 introduces an 83% risk of requiring tenotomy, while HFCS ≥ 2 introduces an 85% risk. There were 17 (21%) relapses. The average interval between the initiation of boot on a bar and the diagnosis and initiation of treatment of relapse was 23 months, ranging from 9 to 43 months.
The primary Achilles tenotomy was required in 10 of 17 feet (59%) that subsequently experienced a relapse, and in 41 of 63 feet (65%) that did not relapse (P > 0.05). The number of casts required to achieve full correction (including the final cast following Achilles tenotomy) ranged between three and nine. The number of casts required was also related to the initial severity. The clubfeet whose TPS was 2–4 required a median of four casts, while those scoring 4–6 required a median of seven casts (P < 0.01). Similarly, an HFCS of 1–2 was associated with a median of five casts, while an HFCS of 2–3 required a median of seven casts (P < 0.05).
An initial attempt was made to correct the recurrent deformity with recasting in all cases, but if unsuccessful, surgical corrections were undertaken and were required in seven feet. Of ten relapsed feet that had been previously treated with primary Achilles tenotomy, four feet required further corrective surgery after relapse (58%), while six feet where treated with casting with or without repeat Achilles tenotomy (60%). Achilles tenotomy for relapse was required in nine feet, including five revision Achilles tenotomies performed in clubfeet that had previously underwent primary tenotomies. Therefore, only one relapsed foot that had been treated with primary Achilles tenotomy could be managed with recasting alone after the relapse. Of seven feet requiring surgery, one (1%) foot underwent tibialis anterior transfer, one (1%) required a subtalar release and one (2.5%) had a cuboid recession. Two feet (2.5%) required a medial release and one (1%) a posterior release. All feet were recasted post-operatively. Three feet relapsed for a second time and required a further repeat procedure, including two tibialis anterior transfers and one gradual correction using a Taylor spatial frame. This patient’s foot is behaving more like a syndromic or teratologic foot, but there is no evidence to identify a specific condition and the patient, therefore, remains in this cohort. Overall, three (4%) feet required a tibialis anterior transfer.
The median initial TPS was 3.5 in the no relapse group and 5.0 in the relapse group. The median MFCS was 1.5 in the no relapse group and 2.0 in the relapse group. The median HFCS was 2.0 in the no relapse group and 3.0 in the relapse group (Fig. 4).
Fig. 4.

This chart demonstrates that, while the median midfoot contracture scores (MFCS) are similar in both groups, the median total Pirani scores (TPS) and hindfoot contracture scores (HFCS) are higher in the relapse group
There was no significant difference discovered between the two groups on the basis of the MFCS (P = 0.13). However, when analysed against the no relapse group, both the TPS and HFCS were statistically significant in predicting the relapse (P = 0.05 × 10−4 and 0.02 × 10−4, respectively).
Discussion
It is widely accepted that the non-surgical management of a clubfoot deformity using the Ponseti method should be the first line of treatment. What is less widely accepted is the value of classification in the routine management of idiopathic clubfoot. Several authors have shown the benefit of using the Pirani score in predicting the likely number of casts required to correct the deformity and the likely chance of requiring an Achilles tenotomy. The data presented in this study has shown a strong link between the severity of the initial Pirani score, especially that of the hindfoot score (HFCS), and the rate of subsequent relapse. In the relapse group, no patient had a TPS of 0–3.0, five had a TPS of 3.5–4.5 and 12 had a TPS of 5.0–6.0. This correlation is equally statistically convincing for HFCS, where all 17 patients in the relapse group had an HFCS of 2.5–3.0 (Fig. 5).
Fig. 5.

a The percentage of clubfeet with higher TPS is greater in the relapse compared to the no relapse group. b The percentage of clubfeet with higher MFCS, but especially HFCS, is also greater in the relapse compared to the no relapse group
It is essential to correct the deformity completely before placing the feet in a foot abduction orthosis. If the correction fails to progress with successive casts, an invasive intervention may be necessary. Usually, this will be in the form of an Achilles tenotomy, but, on occasion, it may be necessary to perform a limited posterior release of the ankle capsule. The foot must be corrected before the orthosis is applied in order to maximise the fit and comfort of the device. Additionally, there is a risk of a rocker-bottom deformity occurring or the persistence of an equinus heel [1, 14]. A well-fitting foot abduction orthosis with the boots externally rotated to 70° and the distance between the heels matching the outer width of the child’s shoulders will increase compliance.
The Ponseti method is based on the idea that “the successful non-operatively treated club foot has a better outcome than the successful surgically treated foot.” The goal of this treatment is a functional, pain-free, plantigrade foot, with good mobility and without calluses, that does not require modified shoes [1]. The outcomes of the treatment reported by Ponseti from the University of Iowa include correction in 98% of clubfeet with no requirement for extensive corrective surgery in >95% cases [5] and a high rate of functionally satisfactory results in 89% of cases [1], even after revision treatment. All but one foot (99%) in our study attained full correction after the initial serial manipulations and castings, which compares favourably with the current prevailing overall initial correction rate of 94.8% in pooled data from about 10,000 cases [15].
Dobbs et al. [2] suggested that non-compliance was one of the most significant factors predicting relapse. They found that the mean age of relapse due to non-compliance was 6 months, with the mean duration of follow-up being 27 months. Therefore, the subsequent potential relapses in their study could have been missed, as, according to our data, the average interval from the completion of Ponseti castings to relapse is 23 months. The minimum follow-up in our study is 2 years, and the rate of relapse may, therefore, increase with time as the cohort matures and will be reported fully once the youngest patients reach 10 years of age and again at maturity. The majority (65%) of our patients had a follow-up period of longer than 4 years.
The reported rate of relapse in this cohort of idiopathic clubfeet was 21%. After the initial attempt to treat these cases with repeat cast applications, all but one of our relapses were ultimately treated operatively. The lowest relapse rate following non-operative management quoted in the literature is 10% in idiopathic clubfeet, with 4% of relapses requiring surgery [5]. Another study reported that one-third of relapse cases can be salvaged with repeat castings [16]. All of our clubfoot cases are continually followed up, allowing for early diagnosis and the re-instigation of treatment for recurrence. However, comparisons with other authors are difficult unless a scoring system is adopted universally to identify which feet are relapsing and how these feet respond to further interventions. From our data, there is clear evidence that a higher hindfoot score, and, consequently, total score, are associated with a greater chance of relapse. To compare appropriately with other series, classification of the initial deformity is essential but also the long-term assessment of outcome to understand fully the effect of further interventions on the different grades of feet encountered. We have also demonstrated that the higher initial TPS and HFCS are associated with a higher rate of Achilles tenotomy and a higher number of casts needed to achieve full initial correction. This is consistent with previously published findings [9, 10]. However, according to our findings, the cases requiring Achilles tenotomy did not appear to significantly correlate with subsequent relapse. Therefore, Achilles tenotomy remains a necessity in obtaining full correction, but is unlikely to affect the potential risk of relapse. Primary Achilles tenotomy also does not appear to render a protective quality against a more invasive procedure required to achieve deformity correction after a relapse. Of ten clubfeet that had undergone primary Achilles tenotomies, equal proportions subsequently required corrective surgery versus recasting with or without Achilles tenotomies after the relapse (58 vs. 60%).
In summary, we have identified that higher initial Pirani scores were associated with a statistically significant increased rate of subsequent relapse. Compared to the MFCS, both the TPS and the HFCS were shown to be the stronger predictors for relapse. The implication of the establishment of this link is that, in order to identify progressive deformity as early as possible to allow timely intervention, a more vigilant follow-up schedule is advised for the patients that are more likely to relapse.
Conflict of interest
No external funding or support was received.
References
- 1.Ponseti IV. Current concepts review: treatment of congenital club foot. J Bone J Surg Am. 1992;74(3):448–454. [PubMed] [Google Scholar]
- 2.Dobbs MB, Rudzki JR, Purcell DB, et al. Factors predictive of outcome after use of the Ponseti method for the treatment of idiopathic clubfeet. J Bone J Surg Am. 2004;86-A(1):22–27. doi: 10.2106/00004623-200401000-00005. [DOI] [PubMed] [Google Scholar]
- 3.Laaveg SJ, Ponseti IV. Long-term results of treatment of congenital club foot. J Bone J Surg Am. 1980;62-A:23–31. [PubMed] [Google Scholar]
- 4.Ponseti IV, Smoley EN. Congenital club foot: the results of treatment. J Bone J Surg Am. 1963;45-A:261–275. [Google Scholar]
- 5.Morcuende JA, Dolan LA, Dietz FR, et al. Radical reduction in the rate of extensive corrective surgery for clubfoot using the Ponseti method. Pediatrics. 2004;113:376–380. doi: 10.1542/peds.113.2.376. [DOI] [PubMed] [Google Scholar]
- 6.Pirani S, Outerbridge HK, Sawatzky B et al (1999) A reliable method of clinically evaluating a virgin clubfoot evaluation. In: Proceedings of the 21st SICOT World Congress, Sydney, Australia
- 7.Diméglio A, Bensahel H, Souchet P, et al. Classification of clubfoot. J Pediatr Orthop B. 1995;4:129–136. doi: 10.1097/01202412-199504020-00002. [DOI] [PubMed] [Google Scholar]
- 8.Flynn JM, Donohoe M, Mackenzie WG. An independent assessment of two clubfoot-classification systems. J Pediatr Orthop. 1998;18(3):323–327. [PubMed] [Google Scholar]
- 9.Scher DM, Feldman DS, van Bosse HJP, et al. Predicting the need for tenotomy in the Ponseti method for correction of clubfeet. J Pediatr Orthop. 2004;24:349–352. doi: 10.1097/01241398-200407000-00001. [DOI] [PubMed] [Google Scholar]
- 10.Dyer PJ, Davis N. The role of the Pirani scoring system in the management of club foot by the Ponseti method. J Bone J Surg Br. 2006;88-B(8):1082–1084. doi: 10.1302/0301-620X.88B8.17482. [DOI] [PubMed] [Google Scholar]
- 11.Bor N, Coplan JA, Herzenberg JE. Ponseti treatment for idiopathic clubfoot: minimum 5-year followup. Clin Orthop Relat Res. 2009;467(5):1263–1270. doi: 10.1007/s11999-008-0683-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Ponseti IV, Zhivkov M, Davis N, et al. Treatment of the complex idiopathic clubfoot. Clin Orthop Relat Res. 2006;451:171–176. doi: 10.1097/01.blo.0000224062.39990.48. [DOI] [PubMed] [Google Scholar]
- 13.Jerome JTJ, Varghese M, Sankaran B et al (2009) Aberrant tendo-Achilles tendon in club foot: a case report. The Foot and Ankle Online Journal. Available online at: http://faoj.files.wordpress.com/2009/02/aberrant_tendo-achilles.pdf. Accessed 25 July 2010
- 14.Simons GW. Correspondence. J Bone Joint Surg. 1986;68-A:151–152. [Google Scholar]
- 15.Morcuende JA (2007) Personal communication. In: Richards S (ed). Dallas, TX
- 16.Richards BS, Faulks S, Rathjen KE, et al. A comparison of two nonoperative methods of idiopathic clubfoot correction: the Ponseti method and the French functional (physiotherapy) method. J Bone J Surg Am. 2008;90(11):2313–2321. doi: 10.2106/JBJS.G.01621. [DOI] [PubMed] [Google Scholar]