

A 49-year-old woman from Kazakhstan, who had immigrated to Germany ~5 years before, developed acute abdominal pain of the right upper quadrant. Cholecystolithiasis was suspected clinically. White blood count showed 7,130 leukocytes/µL with 10% eosinophils. C-reactive protein level was elevated (19 mg/dL), and liver function tests showed a raised gamma-GT of 59 U/L. Cholecystectomy was performed, however, no gallstones were found. Histopathological examination of the removed gallbladder revealed a slight chronic inflammation of the lamina propria. In a Luschka's duct, helminth parasites consistent with hepatic trematodes of the genus Opisthorchis were found (Figures 1 and 2). The eggs seen in the trematode's uterus were much smaller than those of the cosmopolitan liver fluke Fasciola hepatica. Stool examination for helminth ova was not performed. Treatment with praziquantel (75 mg/kg/d in 3 doses) was advised. Opisthorchiasis is caused by the small liver flukes Opisthorchis felineus in the Russian Federation, Ukraine, and Kazakhstan, and Opisthorchis viverrini in Thailand, Lao, Cambodia, and Vietnam.2 Approximately 1.2 million people are infected by O. felineus, the most likely parasite in the case described here, and 12.5 million people are at risk.3 The infection is acquired by eating raw or undercooked cyprinoid fish, which contains metacercariae of the trematodes.2 Not only humans, but also cats, dogs, and possibly many fish-eating mammals, act as definitive hosts. Adult flukes reside in small- and medium-sized intrahepatic bile ducts, and occasionally also in the gallbladder, extrahepatic bile ducts, and in the pancreatic duct.2 In contrast to infection with O. viverrini, a group 1 carcinogen,4 many patients infected by O. felineus suffer from fever and hepatitis-like symptoms in the early stage of infection,5 and no association with cholangiocarcinoma formation has been established. In chronic infections, patients may present with cholangitis and liver abscess because of biliary obstruction.2 Diagnosis is achieved by detection of eggs in feces, however, species-specific diagnosis on the basis of egg morphology is difficult.5 Polymerase chain reaction detecting DNA of the adult parasite in stool may be helpful2 and sometimes the parasites are detected histopathologically in situ, as in the case described here.
Figure 1.
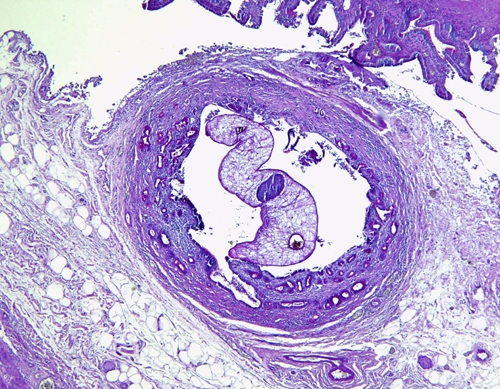
Opisthorchis sp. in Luschka's duct from an immigrant from Kazakhstan. Cross section through posterior third of the parasite. In the center of the trematode the ovary is visible, whereas laterally the paired ceca can be seen. Note absence of vitellaria (compared with Figure 2) in this section plane, which favors the diagnosis of Opisthorchis felineus over the very similar Opisthorchis viverrini.1 Periodic acid-Schiff stain, original magnification ×40. This figure appears in color at www.ajtmh.org.
Figure 2.
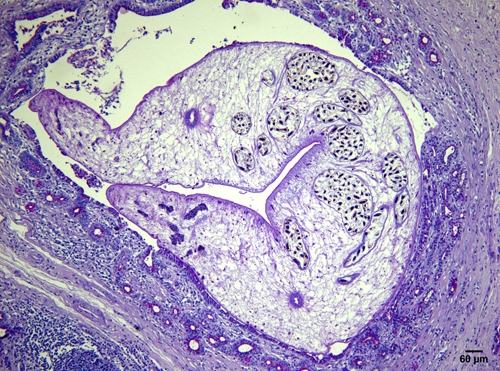
Close-up of Opisthorchis sp. Multiple branches of the egg-filled uterus are visible, flanked by the paired ceca on this cross section through the midbody of the aspinous fluke. Eggs measure 32 × 14 µm on average (length: width ratio of 2.28) and are thus consistent with Opisthorchis felineus.1 Sparse vitellaria are found on the lateral extremes of the parasite on this section. Slight chronic inflammation of the hosts's lamina propria without marked eosinophilic infiltrate can be seen. Periodic acid-Schiff stain, original magnification ×100. This figure appears in color at www.ajtmh.org.
Footnotes
Authors' addresses: Dennis Tappe, Institute of Hygiene and Microbiology, University of Würzburg, Josef-Schneider-Str.2, 97080 Würzburg, Germany, E-mail: dtappe@hygiene.uni-wuerzburg.de. Ralph Triefenbach, Institute for Pathology and Cytology, Limburg, Germany, E-mail: triefenbach@patho-limburg.de.
References
- 1.Mas-Coma S, Bargues Castello MD, Marty AM, Neafie RC. In: Pathology of Infectious Diseases, Volume 1, Helminthiases. Meyers WM, Neafie RC, Marty AM, Wear DJ, editors. Washington, DC: Armed Forces Institute of Pathology, American Registry of Pathology; 2000. pp. 69–92. (Hepatic trematodiases). [Google Scholar]
- 2.Marcos LA, Terashima A, Gotuzzo E. Update on hepatobiliary flukes: fascioliasis, opisthorchiasis and clonorchiasis. Curr Opin Infect Dis. 2008;21:523–530. doi: 10.1097/QCO.0b013e32830f9818. [DOI] [PubMed] [Google Scholar]
- 3.Keiser J, Utzinger J. Emerging foodborne trematodiasis. Emerg Infect Dis. 2005;11:1507–1514. doi: 10.3201/eid1110.050614. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Bouvard V, Baan R, Straif K, Grosse Y, Secretan B, El Ghissassi F, Benbrahim-Tallaa L, Guha N, Freeman C, Galichet L, Cogliano V. A review of human carcinogens–Part B: biological agents. Lancet Oncol. 2009;10:321–322. doi: 10.1016/s1470-2045(09)70096-8. WHO International Agency for Research on Cancer Monograph Working Group. [DOI] [PubMed] [Google Scholar]
- 5.Keiser J, Utzinger J. Food-borne trematodiases. Clin Microbiol Rev. 2009;22:466–483. doi: 10.1128/CMR.00012-09. [DOI] [PMC free article] [PubMed] [Google Scholar]