

Abstract
HIV-associated cognitive neurological disorders (HAND) prevail in the antiretroviral therapy era. Proteomics analysis of CSF revealed expression of Cu/Zn superoxide dismutase (Cu/Zn SOD) in Hispanic women with cognitive impairment (CI). We tested the hypothesis that there is reduced capacity of antioxidant enzymes in CI by measures of expression and activity of Cu/Zn SOD, catalase, and Se-glutathione peroxidase in HAND. Our results showed that the function of these antioxidants was decreased in the CSF and monocytes of women with CI. These findings have important implications regarding their possible contribution to oxidative stress and in the diagnosis and therapy for HAND.
Keywords: Antioxidant enzymes, Cu/Zn SOD, HIV-associated cognitive impairment, HAART, Women
1. Introduction
HIV-associated neurocognitive disorders (HAND) have remained prevalent after introduction of combined antiretroviral therapy (highly active antiretroviral therapy, HAART) (Brew, 2004; Kolson, 2002; Antinori et al., 2007; Wojna et al., 2006; Meléndez et al., 2008). Motor and cognitive deficiencies often manifest as mild conditions and persist as patients live longer (Kolson, 2002; Wojna et al., 2006; Fisher-Smith and Rappaport, 2005). High levels of immunological markers such as tumor necrosis factor-α (TNF-α), interleukin-1, interleukin-6, metalloproteinases, neopterin (Brew et al., 1990), quinolinic acid (Heyes et al., 1991), glycoprotein 41 (gp 41) (Adamson et al., 1999), and macrophage chemotactic protein-1 (MCP-1)(Conant et al., 1998), in brain tissue or cerebrospinal fluid (CSF) have been regarded as risk factors for neurological decline in the pre-HAART era (Griffin, 1997). Of these, MCP-1 and TNF alpha are associated with the time to HIV dementia (Sevigny et al., 2004), or with genetics (MCP-1) in the post-HAART era (Gonzalez et al., 2002; Letendre et al., 2004; Monteiro de Almeida et al., 2005). However, routinely measured blood tests such as CD4 counts and viral RNA that have been linked to improvement in psychomotor speed performance (Sacktor et al., 2003), were not associated with the time to HIV dementia in patients receiving HAART (Sevigny et al., 2004). Since many of these biomarkers are common to other inflammatory diseases, the search for new and combined molecular biomarkers continues to be an objective of active research (Sacktor et al., 2004; Price et al., 2007).
The neuropathogenesis of HIV infection stems from disrupted cellular networks between peripheral monocytes, tissue macrophages, endothelium, and glia. Increased numbers of peripheral CD14+/CD16+ monocytes have been associated with HAD (Pulliam et al., 1997). In an animal model of AIDS, invading monocytes from circulation settle into the perivascular space of the brain (Clay et al., 2007; Kim et al., 2006). Williams et al. (2001) and Fischer-Smith et al. (2001) demonstrated that perivascular macrophages accumulated in SIV and HIVE, respectively. These cells promote pathogenesis by perpetuating the inflammatory process and virus replication in the central nervous system (CNS) (Nath, 1999; Williams and Hickey, 2002).
Our research focuses on the mechanism of HIV neuropathogenesis in a cohort of Hispanic women characterized for cognitive impairment (CI) while using combined antiretroviral therapy. Differences in the macrophage proteome of women with CI, as compared to that of women with no such impairment, have been reported (Luo et al., 2003). Our recent CSF proteomics profiling study from the Hispanic cohort revealed unique proteins associated with CI (Laspiur et al., 2007). Proteins involved in cell signaling, structural function, and antioxidant activities were identified. The cytosolic isoform of Cu/Zn superoxide dismutase (Cu/Zn SOD) was identified from the CSF of 18 women with CI and found with increased expression by immunoblot in 6 patients. Cu/Zn SOD is an important antioxidant enzyme that maintains normal redox status with the dismutation of the superoxide radical into hydrogen peroxide. Hydrogen peroxide is further detoxified by the intervention of either selenium-dependent glutathione peroxidase (GPx) or catalase (Fig. 1). GPx keeps cellular lipids free of harmful peroxides. More importantly, Cu/Zn SOD has a role in signaling and inflammation that depends on the cell redox status and experimental conditions (Marikovsky et al., 2003). This enzyme was identified in the secretome of in vitro HIV-1-infected monocyte-derived macrophages (Ciborowski et al., 2007).
Fig. 1.
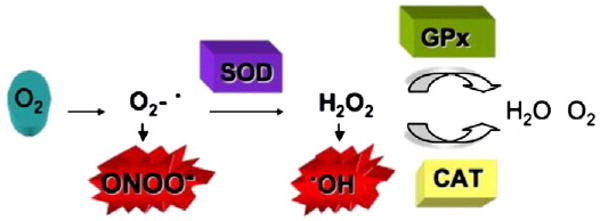
Cellular antioxidant enzyme system.
Oxidative stress is one of the hallmarks of neurodegenerative conditions including HAND, and we found increased Cu/Zn SOD in the CSF of patients with CI. On this basis we hypothesized that the function of Cu/Zn SOD, catalase, and GPx was dysregulated in HIV-infected Hispanic women with CI. We tested these enzymes in blood and CSF compartments, as well as the effect of zidovudine and protease inhibitor therapy on antioxidant enzyme function. Our data support the premise that in the CSF and monocytes there is decreased antioxidant enzyme function that may contribute to oxidative stress and CI. This study has important implications for future diagnosis and therapy of HAND.
2. Materials and methods
2.1. Study patients
A longitudinal cohort study of HIV-seropositive Hispanic women has been followed since 2002 as part of a Specialized Neuroscience Research Program, at the University of Puerto Rico, Medical Sciences Campus (Institutional Review Board Approved Protocol). Forty-three (43) women from this cohort were selected for this study. Inclusion and exclusion criteria have been described previously (Luo et al., 2003; Wojna et al., 2006). Briefly, inclusion criteria were nadir CD4+ T-cell count less than 500 cells/mm3 or a viral load equal to or greater than 1000 copies/mL. Patients with a history of neuropsychiatric disorders, neuroinfectious diseases, hepatitis C, or with a positive toxicology report were excluded. Viral and immune parameters were evaluated at an AIDS Clinical Trial Group (ACTG) certified laboratory. All patients were evaluated with a macro neurological exam and a battery of neuropsychological tests as described previously (Wojna et al., 2006). Cognitive function was determined by the Memorial Sloan Kettering (MSK) dementia scale and the patients were grouped as normal cognition (NC; MSK=0), asymptomatic (A; MSK=0.5), or symptomatic (CI; MSK≥1) (Marder et al., 2003). Asymptomatics have substandard neuropsychological results with average neurological performance and in the study represent a group with early cognitive impairment.
2.2. Blood and CSF samples
Peripheral blood from 43 patients and seropositive subjects was collected in four tubes containing acid citrate dextrose (ACD) anticoagulant and centrifuged to obtain plasma for storage in 0.5 mL aliquots at −80 °C. Peripheral blood mononuclear cells (PBMC) were isolated from the remaining blood in Lymphosep medium (MP Biomedicals, Solon, OH). Monocytes were separated using magnetic cell sorting columns and CD14+ microbeads (Miltenyi Biotech, Auburn, CA). Cells were lysed (5 mM Tris–HCl/0.1% Triton X-100, pH 8.0) and treated with protease inhibitors from Sigma-Aldrich (St. Louis, MO). CSF was collected from the patients using an atraumatic Sprotte needle. CSF was placed in sterile tubes on ice, centrifuged to remove cells and added protease inhibitors (20%). The 0.5 mL aliquots were stored at −80 °C until analysis.
2.3. Cu/Zn SOD expression
Cytosolic Cu/Zn SOD expression was measured by enzyme-linked immunoabsorbent assay (ELISA) (Calbiochem, San Diego, CA), following the manufacturer's instructions. A dilution of 1:200 was selected for plasma, monocyte, and CSF samples after titration. The concentration of Cu/Zn SOD was measured in nanograms per mL (ng/mL). Duplicate samples from each patient were tested and read in a Dynex MRX Revelation Microplate Reader (Chantilly, VA) at 450/620 nm.
2.4. Cu/Zn SOD function
Cu/Zn SOD function was determined by testing enzyme activity using the Superoxide Dismutase Assay Kit II (Calbiochem, San Diego, CA). The assay is based on the reaction between xanthine oxidase and hypoxanthine. Tetrazolium salt was used to detect the superoxide formed in the reaction. Superoxide dismutase present in patient samples degrades the superoxide and a change in absorbance is read at 450 nm. One unit is defined as 50% dismutation of superoxide anion produced. Units in the sample were extrapolated from the standard curve. A 1:30 dilution was used for all samples and tested in triplicate. The kit is sensitive to all 3 SOD isoforms: Cu/Zn (cytosolic and extracellular), Mn (mitochondrial), and Fe SOD (prokaryotes). However, the use of 3 mM potassium cyanide as inhibitor to Cu/Zn SOD helped us to distinguish its activity from the Mn SOD.
2.5. Catalase function
Catalase function was measured using the catalase assay kit from Cayman Chemical (Ann Arbor, MI), which reports activity as the enzyme detoxifies hydrogen peroxide in the presence of methanol. Oxidation of aldehyde that has been formed will cause a change in absorbance, detected at 540 nm. One unit represents the amount of enzyme necessary to produce 1 nmol of aldehyde/minute at 25 °C. A 1:10 dilution was used for monocytes and plasma samples; CSF was undiluted. All samples were assayed in duplicate.
2.6. Glutathione peroxidase function
Selenium-GPx activity was measured with an assay kit from Stressgen (Ann Arbor, MI) based on the scavenging of peroxide with oxidation of glutathione. Glutathione reductase then reduces glutathione and oxidizes nicotinamide adenine dinucleotide phosphate (NADPH). One unit of GPx will cause oxidation of 1 nmol of NADPH. A decrease in absorbance from this reaction is measured at 340 nm. Samples at 1:5 to 1:10 dilution were tested in triplicate.
2.7. Statistical analysis
Two-sided hypothesis testing with a Type I error threshold for significance of 0.05 was used to address the goals of the project. To test the assumption of normality, we used the Shapiro–Wilk test. Since this test indicated that the variables were normally distributed, we reported means and standard deviation (SD) and tested our hypotheses using parametric statistical analysis. The primary goal was to study the expression and/or function of Cu/Zn SOD, catalase, and glutathione peroxidase in cells and fluids from HIV-seropositive Hispanic women as a function of cognitive impairment. To address this goal, enzymes were measured in several compartments: CSF, plasma, and monocytes. Mean differences across groups were tested using analysis of variance (ANOVA). In the event of overall differences, post-hoc analyses were used to test for between-group differences. The secondary goal was to test for differences in Cu/Zn SOD according to antiretroviral therapy. Mean differences in therapy, adjusted across groups, were tested using ANOVA. Data were analyzed using SAS version 8.02 (SAS Institute, Cary, NC).
3. Results
3.1. Study patients
Table 1A summarizes the cognitive status and viral-immune parameters for the patient groups. Samples from 43 HIV-seropositive women were used. Some of them change in MSK classification from one visit to another and we may have used sample from patients representing more than one cognitive group. The mean age for the patients in the study was 37±7 years. CD4 counts were 366±234 cells/mm3. Mean viral load in the CSF was 2.05±0.71 log10 copies/ml and 2.92±1.22 log10 copies/ml in plasma. More than 70% of patients in the cohort are on combined antiretroviral therapy. The average duration of therapy was 1.81 (SD 2.45) years. The range of duration of therapy was 0.02 years to 11.00 years. For those on HAART, the average duration of therapy was 1.55 (SD 1.99) years. Only ten (10) of the 43 individuals (23.2%) have been on their current regiment for less than 3 months. CSF viral load was 2.68 (SD 1.02) among those with ≤3 months duration and was 2.23 (SD 0.55) among those with >3 months duration (p=.127). Plasma viral load was 3.04 (SD 0.86) among those with ≤3 months duration and was 2.87 (SD 1.13) among those with >3 months duration (p=.706). There were no differences in CSF viral load (p=.328) or plasma viral load (p=.612) when stratified by MSK. After stratifying for cognitive status, there were no differences in Cu/Zn SOD expression (p=.812) as a function of duration of therapy. Statistical analysis did not reveal significant differences among the groups for any of these parameters. The number of samples varied according to protein concentration. There were a limited number of samples from normal cognition compared to the other cognitive groups (Table 1B).
Table 1.
| Table 1A: Cognitive status and viral-immune parameters in the three patient groups | ||||||||
|---|---|---|---|---|---|---|---|---|
| MSK1 | n | Age (years) | CD4 (cells/mm3) | Viral load (log 10 copies/ml) | Treatment* | |||
| CSF | Plasma | ART2 | HAART3 | |||||
| Normal cognition | 0 | 11 | 37.4±5.0 | 281.4±121.4 | 2.15±1.00 | 2.85±1.21 | 18% (2) | 72.7% (8) |
| Asymptomatic | 0.5 | 25 | 37.0±6.4 | 374.0±255.3 | 2.21±0.77 | 3.13±1.41 | 16% (4) | 84% (21) |
| Symptomatic CI | ≥1 | 21 | 37.4±7.3 | 408.3±253.6 | 1.79±0.29 | 2.75±1.03 | 19% (4) | 80.9% (17) |
| Table 1B: Number of patient samples used in the study | ||||
|---|---|---|---|---|
| Group | Assay | Monocyte | CSF | Plasma |
| Normal cognition | ELISA | 2 | 7 | 9 |
| Activity | 4 | 11 | 11 | |
| Asymptomatic | ELISA | 6 | 18 | 17 |
| Activity | 6 | 16 | 19 | |
| Symptomatic CI | ELISA | 3 | 16 | 19 |
| Activity | 5 | 17 | 19 | |
Values represent mean±standard deviation.
MSK: Memorial Sloan Kettering,
ART: antiretroviral therapy (two antiviral drugs),
HAART: highly active antiretroviral therapy.
One patient naïve for therapy in the NC group. Statistical analyses for these parameters showed no differences among the groups: Age (p=0.973), CD4 (p=0.353), viral load CSF (p=0.218), viral load plasma (p=0.590) and therapy (p=0.359).
3.2. Cu/Zn SOD expression
An independent analysis of Cu/Zn SOD expression in the monocytes, CSF, and plasma compartments was done by comparing the enzyme concentration in the 3 groups—NC, A, and CI. Expression was significantly lower in monocytes of the CI group than the A (p<0.05) or NC (p<0.001) group. The mean concentration of Cu/Zn SOD in the CI group was 163.5±52 ng/mL (Fig. 2A). Cu/Zn SOD expression in CSF of the A group was 136.8±32.5 ng/mL, but there was a significant increase in the CI group (188.4±78.2 ng/mL, p<0.05). No differences were found in the CI and A groups as compared to patients in the NC group (Fig. 2B). We did not find significant differences in Cu/Zn SOD expression in plasma between women with NC and CI (Fig. 2C). The average concentration of Cu/Zn SOD in plasma was higher than in monocytes and CSF (248.2±171.2 ng/mL).
Fig. 2.
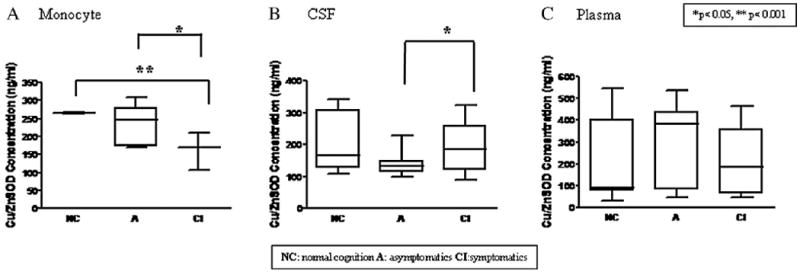
Cu/Zn SOD Expression in women with HIV-1 associated cognitive impairment. Monocytes from women with NC (n=2) and cognitive impairment, A (n=5) and CI (n=3), were tested by ELISA (Calbiochem) in duplicates. (A) Monocytes from CI showed a decrease in expression compared to A (*p<0.05) and to patients with NC (**p<0.001). (B) Increase in Cu/Zn SOD concentration in CSF of CI (n=16) compared to A (n=18) (*p<0.05). No differences were found in the CSF Cu/Zn SOD between A or CI women compared to those with NC. (C) Cu/Zn SOD expression in plasma showed no significant differences between the groups.
3.3. Cu/Zn SOD function
The Cu/Zn SOD function was determined in monocytes, CSF, and plasma by comparing the activity obtained in the 3 different patient categories. There was lower monocyte Cu/Zn SOD activity in CI than in NC (p<0.001) and A women (p<0.05) with an average activity for CI of 0.74±0.53 U/mL (Fig. 3A). Cu/Zn SOD activity in CSF was significantly lower in CI (0.65±0.34 U/ml, p<0.05) than in A (0.87±0.37 U/mL) (Fig. 3B). Cu/Zn SOD activity in plasma was similar among the NC (1.92±0.73 U/mL), A (2.13±1.06 U/mL), and CI (2.46±1.65 U/mL) groups (Fig. 3C).
Fig. 3.
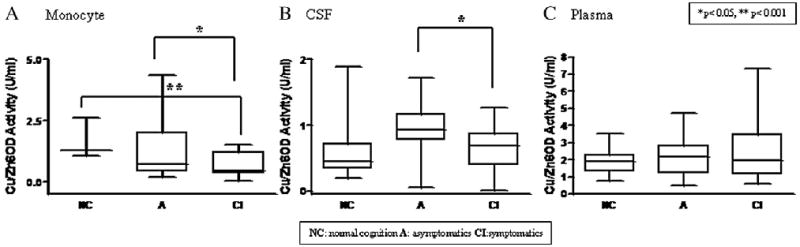
Cu/Zn SOD Function in women with HIV-1 associated cognitive impairment. Cu/Zn SOD function was measured in patient samples by enzymatic activity assay (Calbiochem). (A) Monocytes showed decreased Cu/Zn SOD activity in CI (n=3) compared to NC (n=1) (**p<0.001) and to A (n=3) (*p<0.05). (B) Cu/Zn SOD activity in CSF was measured in women with NC (n=7), A (n=13), and CI (n=10). Decrease activity was found in the CSF of CI compared to A (*p<0.05). (C) There were no differences in plasma Cu/Zn SOD activity among the groups.
3.4. Catalase and Se-GPx function
Catalase activity was lower in monocytes from CI (36.5±28.6 nmol/min/mL, p<0.05) than from patients with NC (67.2±16.7 nmol/min/mL) (Fig. 4A). Catalase did not change in either CSF or plasma of NC and CI patients (Fig. 4B and C). GPx function was lower in monocytes from CI (46.2±52.7 U/mL) than from NC (113.5±44.9 U/mL, p<0.05) or A (94.3±11.1 U/mL p<0.05) (Fig. 5A). There was also lower GPx activity in the CSF from CI than from NC and A (p<0.05) (Fig. 5B). There was greater GPx activity in plasma from A and CI than from NC (p<0.05) (Fig. 5C).
Fig. 4.
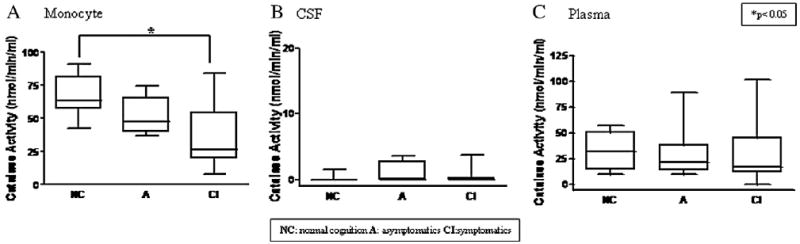
Catalase function and cognitive impairment. Catalase activity was measured in the CSF, plasma and monocyte samples using an indirect method of hydrogen peroxide processing with aldehyde oxidation (Cayman Chemical). (A) A decrease in catalase activity was found in monocytes of CI (n=4) compared to patients with NC (n=4) (*p<0.05). No differences were found in (B) CSF or (C) plasma among the groups.
Fig. 5.
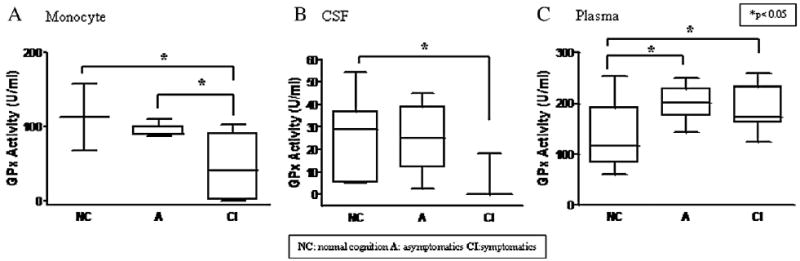
GPx function and cognitive impairment. GPx activity was evaluated through oxidation of NADPH read at A340 nm (Stressgen). (A) GPx activity was decreased in monocytes of CI (n=4), compared to women with NC (n=3) (*p<0.05) (B) Activity decreased in the CSF of CI (n=11) (*p<0.05) compared to patients with NC (n=8) and A (n=11). (C) GPx activity was higher in plasma of patients with cognitive impairment (As n=11, CI n=11) (*p<0.05) compared to the NC group (n=8).
3.5. Antiretroviral therapy in Cu/Zn SOD expression and function
Combined antiretroviral therapy was used by most patients (72.1%; 31/43). Side effects of some of the compounds are due to disruption of important cellular processes. A sub-analysis into the effect of zidovudine (AZT) and protease inhibitors (PI) on Cu/Zn SOD expression and activity was conducted examining data from women with or without AZT in their medication regimen. Although it has been reported that AZT affects Cu/Zn SOD expression (D'Andrea et al., 2006), no significant differences were found between the use of AZT or PI among the 3 groups of cognitive performance.
4. Discussion
This study was designed to determine the role of antioxidant enzymes in HAND. Specifically, we determined the expression and activity of Cu/Zn SOD, catalase, and Se-GPx in HAND with 43 HIV-seropositive Hispanic women who used combined antiretroviral therapy. In our previous study, immunoblot analysis revealed an increase of Cu/Zn SOD in women with cognitive impairment as compared to those with normal cognition. In the present study when we stratified cognitive function between asymptomatic women and those with cognitive impairment, we confirmed that the increase was mainly in the latter group. This increased expression of Cu/Zn SOD in CI was accompanied by a significantly decreased Cu/Zn SOD function in the CSF. This compartment contains molecules that are byproducts of processes occurring in the CNS. Increased Cu/Zn SOD expression in the CSF of CI could be a compensatory mechanism for decreased enzyme function. In contrast to CI women, the A group had low enzyme concentration with elevated activity. This may indicate modulation of function in the initial stages of neurological disease. High levels of Cu/Zn SOD mRNA were reported in brain tissue of patients with HIV-associated dementia in the pre-HAART era (Boven et al., 1999). Cu/Zn SOD abundance was increased in microglia and brain macrophages as compared with non-demented and control subjects (Boven et al., 1999). Our data support previous studies and indicate that Cu/Zn SOD abundance in the CSF is linked to decreased function independent of the duration of HAART.
In addition to decreased Cu/Zn SOD activity, GPx activity was also lower in the CSF of patients with CI. With Cu/Zn SOD activity being decreased, less hydrogen peroxide is produced and less GPx is needed for conversion of hydrogen peroxide into water and oxygen (Fig. 1). Our results could indicate that defects in Cu/Zn SOD function affect the other enzymes in the antioxidant pathway.
Activated monocytes are increased in HIV dementia (Pulliam et al., 1997). Cu/Zn SOD activity decreases in mononuclear cells with progression of HIV infection (Treitinger et al., 2000). In our studies we found that Cu/Zn SOD expression and activity were both lower in the monocytes of patients with CI than in those with NC. This low activity combined with oxidative stress in the CNS may promote peroxynitrite formation and neuronal damage (Mollace et al., 2001). Another aspect of low Cu/Zn SOD function is altered monocyte chemotaxis. Cu/Zn SOD controls up-regulation of adhesion proteins by HIV-1 Tat-mediated reactive oxygen species (ROS) release in monocytes (Song et al., 2007). Moreover, unrestricted ROS production may facilitate NF-κβ induction, subsequent HIV long terminal repeat transactivation, and chronic viral replication upon cell maturation into macrophages (Israel and Gougerot-Pocidalo, 1997).
Monocytes of CI had low catalase activity. Studies prior to HAART reported increased catalase activity in serum with advanced HIV infection (Leff et al., 1992). Another study found low expression of catalase in T-lymphocytes from HIV-seropositive individuals (Yano et al.,1998). To our knowledge, there is no previous evidence of catalase expression or activity in HIV-associated cognitive impairment (Mollace et al., 2001).
GPx, the counterpart of catalase, showed significant decreased activity in monocytes of women with CI (p<0.05). Viral proteins, gp120 and Tat, can decrease levels of GPx in brain endothelial cells where oxidative stress contributes to blood-brain barrier disruption (Price et al., 2005). Lower activity of catalase and GPx may promote peroxidation and neuronal apoptosis in HAND.
We determined the expression and activity of these antioxidants in plasma from women with CI to compare their effect in the periphery with that of CSF. We found similar expression and activity of Cu/Zn SOD and catalase in plasma of women with HAND. In contrast to our findings for CSF, we found increased GPx activity in the plasma of patients with CI. There is a plasma-specific selenocysteine isoform, distinct from the intracellular GPx, and its contribution to the observed increase in activity cannot be ruled out in our results.
We found important dysregulation of the antioxidant enzyme sysem in more than one compartment studied. There is evidence of modifications relating to neurological disorders and HIV. Established factors altering Cu/Zn SOD function are mutations (Emerit et al., 2004), oxidation (Ezzi et al., 2007), high levels of nitric oxide (Boven et al., 1999), temperature, and copper depletion (Lombardo et al., 2003). Regarding GPx, decreased levels of reduced glutathione, an intermediary in the GPx reaction, affect HIV-seropositive patients (Israel and Gougerot-Pocidalo, 1997). The glutathione precursor, cysteine, is also low and may have an adverse effect on the overall immune suppression characteristic of the infection (Dröge, 2002). Selenium is required as a cofactor in GPx active sites and decreases in HIV infection (Ogunro et al., 2006).
In general our findings indicate that monocytes and CSF from the Hispanic cohort with HIV-associated cognitive impairment demonstrate a parallel decline in antioxidant enzyme function independent of the antiretroviral therapy. One question remains unanswered: Is decreased enzyme activity a protective mechanism of innate immunity or a negative consequence of failed control in the inflammatory response after HIV infection? Research initiatives in this area are ongoing at our laboratories. One limitation of our study is the number of monocyte samples from patients with intact neurological function. Efforts to expand this sample group are in progress. Finally, it is essential to verify expression and activity of these antioxidant enzymes in samples from other cohorts, such as the North Eastern AIDS Dementia (NEAD) or Hawaii Aging groups, that are well characterized for HAND.
The knowledge gained from this study conveys a need for therapies directed at normalizing functional levels of enzymes, such as Cu/Zn SOD and GPx, to control unfavorable production of ROS. Such an approach may have a synergistic effect with better CNS-penetrating antiretroviral therapy in further suppressing the onset of neurological complications associated with HIV infection. Advances could also be relevant to other disorders where oxidative stress is present, such as ALS, Down syndrome, asthma, and Parkinson and Alzheimer's disease.
Acknowledgments
This work was supported by grants NIH-SNRP 1 U54NS430, NIH-MBRS-SCORE-SO6GMO822 and NIH-RCMI-CRC P20RR11126. We thank the patients of the SNRP-NeuroAIDS Hispanic Women Cohort. Ms. Tania Ginebra and Dr. Tania de la Torre provided patient outreach. Ms. Elizabeth Maldonado organized patient demographics. We thank Dr. Rosa Hechavarría and Dr. Raul Mayo for neuropsychological testing. We thank Dr. Carmen Zorrilla and Dr. Hermes García, directors of the Centro de Estudios Materno Infantil (CEMI) and Centro Latinoamericano de Enfermedades de Transmisión Sexual (CLETS) respectively, who referred patients to the study. We thank Dr. Edmundo Kraiselburd, director of the SNRP-NeuroAIDS Program for his support in this study. We thank Dr. Howard Gendelman and Dr. Dale Benos for careful review of this manuscript.
References
- Adamson DC, McArthur JC, Dawson TM, Dawson VL. Rate and severity of HIV-associated dementia (HAD): correlations with Gp41 and iNOS. Mol Med. 1999;5:98–109. [PMC free article] [PubMed] [Google Scholar]
- Antinori A, Arendt G, Becker JT, Brew BJ, Byrd DA, Cherner M, Clifford DB, Cinque P, Esptein LG, Goodkin K, Gisslen M, Grant I, Heaton RK, Joseph J, Marder K, Marra CM, McArthur JC, Nunn M, Price RW, Pulliam L, Robertson KR, Sacktor N, Valcour V, Wojna V. Updated research nosology for HIV-associated neurocognitive disorders. Neurology. 2007;69:1789–1799. doi: 10.1212/01.WNL.0000287431.88658.8b. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Boven LA, Gomes L, Hery C, Gray F, Verhoef J, Portergeis P, Tardieu M, Nottet HSLM. Increased peroxynitrate activity in AIDS dementia complex: implications for the neuropathogenesis of HIV-1 infection. J Immunol. 1999;162:4319–4327. [PubMed] [Google Scholar]
- Brew BJ. Evidence for a change in AIDS dementia complex in the era of highly active antiretroviral therapy and the possibility of new forms of AIDS dementia complex. AIDS. 2004;18(suppl 1):S75–S78. [PubMed] [Google Scholar]
- Brew BJ, Bhalla RB, Morris P, Gallardo H, McArthur JC, Schwartz MK, Price RW. Cerebrospinal fluid neopterin in human immunodefiency virus type 1 infection. Ann Neurol. 1990;28:556–560. doi: 10.1002/ana.410280413. [DOI] [PubMed] [Google Scholar]
- Ciborowski P, Kadiu I, Rozek W, Smith L, Bernhardt K, Fladseth M, Ricardo-Dukelow M, Gendelman HE. Investigating the human immunodeficiency virus type 1-infected monocyte-derived macrophage secretome. Virology. 2007;363:198–209. doi: 10.1016/j.virol.2007.01.013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Clay CC, Rodrigues DS, Ho YS, Fallert BA, Janatpour K, Reinhart TA, Esser U. Neuroinvasion of fluorescein-positive monocytes in acute simian immunodeficiency virus infection. J Virol. 2007;81:12040–12048. doi: 10.1128/JVI.00133-07. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Conant K, Garzino-Demo A, Nath A, McArthur JC, Halliday W, Power C, Gallo RC, Major EO. Induction of monocyte chemoattractant protein-1 in HIV-1 Tat-stimulated astrocytes and elevation in AIDS dementia. PNAS. 1998;17:3117–3121. doi: 10.1073/pnas.95.6.3117. [DOI] [PMC free article] [PubMed] [Google Scholar]
- D'Andrea G, Lizzi AR, Venditti S, Di Francesco L, Giorgi A, Mignogna G, Oratore A, Bozzi A. Proteins pattern alteration in AZT-treated K562 cells detected by two-dimensional gel electrophoresis and peptide mass fingerprinting. Proteome Sci. 2006;4(4) doi: 10.1186/1477-5956-4-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dröge W. Free radicals in the physiological control of cell function. Physiol Rev. 2002;82:47–95. doi: 10.1152/physrev.00018.2001. [DOI] [PubMed] [Google Scholar]
- Emerit J, Edeas M, Bricaire F. Neurodegenerative diseases and oxidative stress. Biomed Pharmacother. 2004;58:39–46. doi: 10.1016/j.biopha.2003.11.004. [DOI] [PubMed] [Google Scholar]
- Ezzi SA, Urushitani M, Julien JP. Wild-type superoxide dismutase acquires binding and toxic properties of ALS-linked mutant forms through oxidation. J Neurochem. 2007;102:170–178. doi: 10.1111/j.1471-4159.2007.04531.x. [DOI] [PubMed] [Google Scholar]
- Fisher-Smith T, Rappaport J. Evolving paradigms in the pathogenesis of HIV-associated dementia. Expert Rev Mol Med. 2005;7:1–26. doi: 10.1017/S1462399405010239. [DOI] [PubMed] [Google Scholar]
- Fischer-Smith T, Croul S, Sverstiuk AE, Capini C, L'Heureux D, Regulier EG, Richardson MW, Amini S, Morgello S, Khalili K, Rappaport J. CNS invasion by CD14+/CD16+ peripheral blood-derived monocytes in HIV dementia: perivascular accumulation and reservoir of HIV infection. J Neurovirol. 2001;7:528–541. doi: 10.1080/135502801753248114. [DOI] [PubMed] [Google Scholar]
- Gonzalez E, Rovin BH, Sen L, Cooke G, Dhanda R, Mummidi S, Kulkarni H, Bamshad MJ, Telles V, Anderson SA, Walter EA, Stephan KT, Deucher M, Mangano A, Bologna R, Ahuja SS, Dolan MJ, Ahuja SK. HIV-1 infection and AIDS dementia are influenced by a mutant MCP-1 allele linked to increased monocyte infiltration of tissues and MCP-1 levels. PNAS. 2002;99(21):13795–13800. doi: 10.1073/pnas.202357499. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Griffin DE. Cytokines in the brain during viral infection. Clues to HIV-associated dementia. J Clin Invest. 1997;100:2948–2951. doi: 10.1172/JCI119847. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Heyes MP, Brew BB, Martin A, Price RW, Salazar A, Sidtis JJ, Yergey JA, Mouradian MM, Sadler AE, Keilp J, Rubinow R, Markey SP. Quinolinic acid in cerebrospinal fluid and serum in HIV-1 infection: relationship to clinical and neurological status. Ann Neurol. 1991;29:202–209. doi: 10.1002/ana.410290215. [DOI] [PubMed] [Google Scholar]
- Israel N, Gougerot-Pocidalo MA. Oxidative stress in human immunodeficiency virus infection. CMLS Cell Mol Life Sci. 1997;53:864–870. doi: 10.1007/s000180050106. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kim WK, Alvarez X, Fisher J, Bronfin B, Westmoreland S, McLaurin J, Williams K. CD163 identifies perivascular macrophages in normal and viral encephalitic brains and potential precursors to perivascular macrophages in blood. Am J Pathol. 2006;168(3):822–834. doi: 10.2353/ajpath.2006.050215. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kolson DL. Neuropathogenesis of central nervous system HIV-1 infection. Clin Lab Med. 2002;22:703–717. doi: 10.1016/s0272-2712(02)00009-4. [DOI] [PubMed] [Google Scholar]
- Laspiur JP, Anderson ER, Ciborowsky P, Wojna V, Rozek W, Duan F, Mayo R, Rodríguez E, Plaud-Valentín M, Rodríguez-Orengo J, Gendelman HE, Meléndez LM. CSF proteomics fingerprints for HIV-associated cognitive impairment. J Neuroimmunol. 2007;192:157–170. doi: 10.1016/j.jneuroim.2007.08.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Leff JA, Oppegard MA, Curiel TJ, Brown KS, Schooley RT, Repine JE. Progressive increases in serum catalase activity in advancing human immunodeficiency virus infection. Free Radic Biol Med. 1992;13:143–149. doi: 10.1016/0891-5849(92)90076-s. [DOI] [PubMed] [Google Scholar]
- Letendre S, Marquie-Beck J, Singh KK, de Almeida S, Zimmerman J, Spector SA, Grant I, Ellis R, HNRC Group The monocyte chemotactic protein-1–2578G allele is associated with elevated MCP-1 concentrations in cerebrospinal fluid. J Neuroimmunol. 2004;157:193–196. doi: 10.1016/j.jneuroim.2004.08.028. [DOI] [PubMed] [Google Scholar]
- Lombardo MF, Ciriolo MR, Rotilio G, Rossi L. Prolonged copper depletion induces expression of antioxidants and triggers apoptosis in SH-SY5Y neuroblastoma cells. CMLS Cell Mol Life Sci. 2003;60:1733–1743. doi: 10.1007/s00018-003-3153-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Luo X, Carlson KA, Wojna W, Mayo R, Biskup TM, Stoner J, Anderson J, Gendelman HE, Meléndez LM. Macrophage proteomic fingerprinting predicts HIV-1 associated cognitive impairment. Neurology. 2003;60:1931–1937. doi: 10.1212/01.wnl.0000064396.54554.26. [DOI] [PubMed] [Google Scholar]
- Marder K, Albert SM, McDermott MP, McArthur JC, Schifitto G, Selnes OA, Sacktor N, Stern Y, Palumbo D, Kieburtz K, Cohen B, Orme C, Epstein LG. Inter-rater reliability of a clinical staging of HIV-associated cognitive impairment. Neurology. 2003;60:1467–1473. doi: 10.1212/01.wnl.0000064172.46685.82. [DOI] [PubMed] [Google Scholar]
- Marikovsky M, Ziv Vered, Nevo N, Harris-Cerruti C, Mahler O. Cu/Zn superoxide dismutase plays important role in immune response. J Immunol. 2003;170:2993–3001. doi: 10.4049/jimmunol.170.6.2993. [DOI] [PubMed] [Google Scholar]
- Meléndez LM, Mayo-Santana R, Luciano C, Wojna V. Ethnicity and Neuro-AIDS conditions in the HAART Era. In: Goodkin K, Shapshak P, Verma A, editors. Spectrum of Neuro-AIDS Disorders: Pathophysiology, Diagnosis, and Treatment. ASM; Washington, DC: 2008. [Google Scholar]
- Mollace V, Nottet HSLM, Clayette P, Turco MC, Muscoli C, Salvemini D, Perno CF. Oxidative stress and neuroAIDS: triggers, modulators and novel antioxidants. Trends Neurosci. 2001;24:411–416. doi: 10.1016/s0166-2236(00)01819-1. [DOI] [PubMed] [Google Scholar]
- Monteiro de Almeida S, Letendre S, Zimmerman J, Lazzaretto D, Mc Cuthcan A, Ellis R. Dynamics of monocyte chemoattractant protein type one (MCP-1) and HIV viral load in human cerebrospinal fluid and plasma. J Neuroimmunol. 2005;169:144–152. doi: 10.1016/j.jneuroim.2005.07.012. [DOI] [PubMed] [Google Scholar]
- Nath A. Pathobiology of human immunodeficiency virus dementia. Semin Neurol. 1999;19:113–127. doi: 10.1055/s-2008-1040830. [DOI] [PubMed] [Google Scholar]
- Ogunro PS, Ogungbamigbe TO, Elemie PO, Egbewale BE, Adewole TA. Plasma selenium concentration and glutathione peroxidase activity in HIV-1/AIDS infected patients: a correlation with the disease progression. Niger Postgrad Med J. 2006;13:1–5. [PubMed] [Google Scholar]
- Price TO, Ercal N, Nakaoke R, Banks WA. HIV-1 viral proteins gp120 and Tat induce oxidative stress in brain endothelial cells. Brain Res. 2005;1045:57–63. doi: 10.1016/j.brainres.2005.03.031. [DOI] [PubMed] [Google Scholar]
- Price RW, Epstein LG, Becker JT, Cinque P, Gisslen M, Pulliam L, McArthur JC. Biomarkers of HIV-1 CNS infection and injury. Neurology. 2007;69:1781–1788. doi: 10.1212/01.wnl.0000278457.55877.eb. [DOI] [PubMed] [Google Scholar]
- Pulliam L, Gascon R, Stubblebine M, McGuire D, McGrath MS. Unique monocyte subset in patients with AIDS dementia. Lancet. 1997;349:692–695. doi: 10.1016/S0140-6736(96)10178-1. [DOI] [PubMed] [Google Scholar]
- Sacktor N, Skolasky RL, Tarwater PM, McArthur JC, Selnes OA, Becker J, Cohen B, Visscher B, Miller EN, Multicenter AIDS Cohort Study (MACS) Response to systemic HIV viral load suppression correlates with psychomotor speed performance. Neurology. 2003;26:567–569. doi: 10.1212/01.wnl.0000076477.71313.6e. [DOI] [PubMed] [Google Scholar]
- Sacktor N, Haughey N, Cutler R, Tamara A, Turchan J, Pardo C, Vargas D, Nath A. Novel markers of oxidative stress in actively progressive HIV dementia. J Neuroimmunol. 2004;157:176–184. doi: 10.1016/j.jneuroim.2004.08.037. [DOI] [PubMed] [Google Scholar]
- Sevigny JJ, Albert SM, McDermott MP, McArthur JC, Sacktor N, Conant K, Schifitto G, Selnes OA, Stern Y, McClernon DR, Palumbo D, Kieburtz K, Riggs G, Cohen B, Epstein LG, Marder K. Evaluation of HIVRNA and markers of immune activation as predictors of HIV-associated dementia. Neurology. 2004;63:2084–2090. doi: 10.1212/01.wnl.0000145763.68284.15. [DOI] [PubMed] [Google Scholar]
- Song HY, Ju SM, Lee JA, Kwon H, Eum WS, Jang SH, Choi SY, Park J. Suppression of HIV-1 Tat-induced monocyte adhesiveness by a cell-permeable superoxide dismutase in astrocytes. Exp Mol Med. 2007;39:778–786. doi: 10.1038/emm.2007.84. [DOI] [PubMed] [Google Scholar]
- Treitinger A, Spada C, Verdi JC, Miranda AF, Oliveira OV, Silveira MV, Moriel P, Abdalla DS. Decreased antioxidant defence in individuals infected by the human immunodeficiency virus. Eur J Clin Invest. 2000;30:454–459. doi: 10.1046/j.1365-2362.2000.00642.x. [DOI] [PubMed] [Google Scholar]
- Williams KC, Hickey WF. Central nervous system damage, monocytes and macrophages and neurological disorders in AIDS. Annu Rev Neurosci. 2002;25:537–562. doi: 10.1146/annurev.neuro.25.112701.142822. [DOI] [PubMed] [Google Scholar]
- Williams KC, Corey S, Westmoreland SV, Pauley D, Knight H, De Bakker C, Alvarez X, Lackner AA. Perivascular macrophages are the primary cell type productively infected by simian immunodeficiency virus in the brains of macaques: implications for the neuropathogenesis of AIDS. J Exp Med. 2001;193:905–915. doi: 10.1084/jem.193.8.905. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wojna V, Skolasky RL, Hechevarría R, Mayo R, Selnes O, MacArthur JC, Meléndez LM, Maldonado E, Zorrilla CD, García H, Kraiselburd E, Nath A. Prevalence of human immunodeficiency virus-associated cognitive impairment in a group of Hispanic women at risk for neurological impairment. J NeuroVirol. 2006;12:356–364. doi: 10.1080/13550280600964576. [DOI] [PubMed] [Google Scholar]
- Yano S, Yano N, Rodriguez N, Baek JH, Que X, Yamamura Y, Kim SJ. Suppression of intracellular hydrogen peroxide generation and catalase levels in CD8+ T-lymphocytes from HIV+ individuals. Free Radic Biol Med. 1998;24:349–359. doi: 10.1016/s0891-5849(97)00275-x. [DOI] [PubMed] [Google Scholar]