

Abstract
Background
The lower trapezius is an important muscle for normal arthrokinematics of the scapula. In the early stages of rehabilitation, it is generally accepted to perform exercises with the shoulder kept below 90° of elevation in order to minimize risk for shoulder impingement. Few exercises for the lower trapezius have been studied which maintain the shoulder below 90° of humeral elevation.
Objective
To identify therapeutic exercises performed below 90° of humeral elevation that activate marked levels of lower trapezius electromyographic (EMG) activity.
Methods
Surface EMG activity of the lower, middle, upper trapezius, and serratus anterior was collected bilaterally on fifteen healthy subjects during four exercises: the press-up, unilateral scapular retraction with the shoulder positioned at 80° of shoulder flexion, bilateral shoulder external rotation, and unilateral scapular depression.
Results
The press-up exercise elicited marked lower trapezius EMG activity, moderate upper trapezius EMG activity, and a high ratio of lower trapezius to upper trapezius EMG activity. Scapular retraction produced marked EMG activity of both the lower and upper trapezius and moderate activity of the middle trapezius. Bilateral shoulder external rotation generated moderate lower trapezius EMG activity, minimal upper trapezius activity, and the highest ratio of lower trapezius to upper trapezius EMG activity. Scapular depression produced moderate lower trapezius EMG activity, mimimal upper trapezius EMG activity, and a moderately high ratio of lower trapezius to upper trapezius EMG activity.
Discussion and Conclusions
This study identified two exercises performed below 90° of humeral elevation that markedly activated the lower trapezius: the press-up and scapular retraction.
Keywords: lower trapezius, electromyography, scapula
INTRODUCTION
Lower trapezius muscle performance is an essential component to normal scapulohumeral rhythm.1–7 Normal scapulohumeral rhythm requires upward scapular rotation, provided by the force couple of the trapezius and serratus anterior muscles, in order to prevent the rotator cuff tendon from impinging against the anterolateral acromion.6,8–12 During active humeral elevation, upward scapular rotation of the scapula is initiated by the serratus anterior.10 One function of the lower trapezius muscle is to stabilize the scapula against lateral displacement produced by the serratus anterior.10 The serratus anterior and upper trapezius can then exert an upward rotation moment about the scapula.10 A second function of the lower trapezius is to stabilize the scapula against scapular elevation produced by the levator scapulae.10 Therefore, the lower trapezius muscle is an essential component of the trapezius-serratus anterior force couple by maintaining vertical and horizontal equilibrium of the scapula during humeral elevation.10
Research has shown an association between shoulder pathology and abnormal scapular motion or muscle firing patterns of the lower trapezius.3,6,13–27 Increased scapular elevation has been found in subjects with subacromial impingement compared to subjects without shoulder pathology.19,27 Cools et al13 found a decrease in lower trapezius activity during isokinetic scapular protraction-retraction in 19 overhead athletes with subacromial impingement. A delayed onset of lower trapezius muscle activity and over-activity of the upper trapezius was found in a study comparing 30 normal athletes and 39 athletes with subacromial impingement in response to external forces imposed on the arm.14
Although it is not known whether abnormal scapular arthrokinematics precedes or is a consequence of abnormal motor recruitment patterns of the scapular muscles, normal movement and function of the shoulder is dependent upon normal function of the scapular upward rotator muscles.12 Subsequently, it is important to strengthen the lower trapezius muscle during rehabilitation of patients with shoulder pathology. These exercises should be performed below 90° of humeral elevation during the initial stages of shoulder rehabilitation in order to prevent impingement or strain on the rotator cuff tendons and shoulder ligaments.20,28–30 Despite these recommendations, to our knowledge, no exercises performed with the shoulder below 90° of elevation have been identified which markedly recruit the lower trapezius using the standard established by McCann et al.20
Several studies have reported that maximum lower trapezius muscle electromyographic (EMG) activity occurs between 90° and end range of humeral elevation during active motion or therapeutic exercises.1,4,22,31–36 Ekstrom et al32 assessed the EMG activity of the trapezius and serratus anterior muscles in 30 healthy subjects with the use of surface EMG during 10 exercises. The authors found that shoulder elevation while lying prone with the externally rotated shoulder positioned in line with the lower trapezius was the best exercise for the lower trapezius, eliciting 97% of maximum voluntary isometric contraction (MVIC). Prone lying shoulder external rotation and horizontal extension with the arm positioned at 90° of abduction was found to activate 79% MVIC and 74% MVIC respectively. Utilizing indwelling electrodes on 20 healthy subjects, Ballantyne et al31 determined that shoulder external rotation while lying prone with the arm positioned at 90° produced 40% MVIC of the lower trapezius. Mosely et al22 analyzed 16 exercises in nine subjects with the use of indwelling electrodes and concluded that five exercises qualified as optimal for recruiting the lower trapezius: shoulder abduction, rowing, shoulder flexion, shoulder horizontal abduction with external rotation, and shoulder horizontal abduction in neutral rotation. Peak muscle activity for these exercises occurred between 90° and 150° of shoulder elevation and ranged from 56%-68% of MVIC.
All of the exercises cited in the aforementioned studies require the shoulder to be positioned at or greater than 90° of elevation. Subsequently, these exercises may not be appropriate for patients in the initial stage of shoulder rehabilitation with subacromial impingement. Only two previous studies were identified that examined lower trapezius muscle activity during exercises performed while maintaining the shoulder below 90° of humeral elevation.32,34 Ekstrom et al32 found that shoulder abduction performed below 80° in the plane of the scapula activated 50±21% MVIC of the lower trapezius while prone unilateral rowing produced 45±17% MVIC. Lear and Gross34 utilized surface EMG on 16 healthy subjects performing three variations of a push-up: push-up with a plus, push-up with a plus and the feet elevated, and push-up with a plus with the feet elevated and hands placed on a trampoline. All three conditions elicited lower trapezius muscle activity of less than 40% MVIC. The purpose of this study was to identify exercises performed with the shoulder below 90° that elicited marked levels of lower trapezius muscle activity using the standard established by McCann et al 20 (>50% MVIC).
METHODS
Subjects
Subjects for this study consisted of fifteen healthy volunteers (age - 31.7 ± 9.5; height - 1.8 ± .09 meters; 8 females and 7 males; weight - 76.2 ± 14.2 kg.). The ages of the subjects ranged from 18 to 38 years. The inclusion criteria were being at least 18 years of age and being able to communicate in English. Potential subjects were excluded from this study if they reported a recent history (less than one year) of a musculoskeletal injury, condition, or surgery involving either upper extremity or the cervical spine. Subjects were also excluded if they reported a prior history of a neuromuscular condition, pathology, or the presence of numbness or tingling in either upper extremity. The senior author performed the assessment for the inclusion and exclusion criteria through the use of a verbal questionnaire. This study was approved by the Lenox Hill Hospital Institutional Review Board and informed consent was obtained from all subjects prior to participation.
Testing Procedures
Silver/silver-chloride (Ag/AgC1) surface electrodes were placed bilaterally over the serratus anterior and the upper, middle, and lower trapezius muscles of each subject according to the method described by Basmajian and DeLuca37 and as outlined in Table 1. The skin was prepared prior to electrode placement by shaving hair (if necessary), abrading the skin with fine sandpaper, and cleaning the site with isopropyl alcohol. A reference electrode was placed on the olecranon process of each subject.
Table 1.
Muscles tested, electrode position, and maximal voluntary contraction (MVIC) Protocol
| Muscle | Electrode position | MVIC position | MVIC Action |
|---|---|---|---|
| Upper trapezius | At the angle of the neck and shoulder, over the belly of the muscle in line with the muscle fibers. | Sitting with arms relaxed at sides | Resisted maximum shoulder elevation |
| Middle trapezius | Centered vertically between the medial border of the scapula and the spines of the thoracic vertebrae at the same level (T-1 to T-6) | Prone, shoulder abducted to 90° and lateral rotation, elbow flexed 90° | Resisted horizontal arm abduction |
| Lower trapezius | Placed obliquely upward and laterally along a line between the intersection of the spine of the scapula with the vertebral border of the scapula and the seventh thoracic spinous process. | Prone, shoulder in 130° of abduction. | Resisted arm elevation |
| Serratus anterior | Placed vertically below the axilla, anterior to the latissimus, over the 4th-6th ribs | Supine, shoulder in 90° of flexion and elbow in extension | Resisted end range protraction |
An 8-channel Telemyo EMG system (Noraxon USA, Inc., Scottsdale, AZ) was used to acquire surface EMG data. The center to center interelectrode distance was 25 mm. The Telemyo system has a gain of 2000, a common mode rejection ratio (CMRR) of greater than 100 dB at 60 Hz, a bandwidth of 10 to 500 Hz, and a differential input impedance of >10 M. The Telemyo was interfaced with a personal computer via a 16 channel, 12 bit A/D card. Each subject performed one manually resisted sub-maximal voluntary isometric contraction of each muscle according to the methods outlined by Daniels and Worthingham38 in order to verify the quality of the telemetric signal and to ensure that each subject became familiar with the muscle testing procedures. Three manually resisted maximum voluntary isometric contractions (MVICs), each for duration of 3 seconds, were then performed for each muscle. Table 1 displays the electrode placement location, MVIC position, and MVIC action for each of the five muscles during the testing protocol.
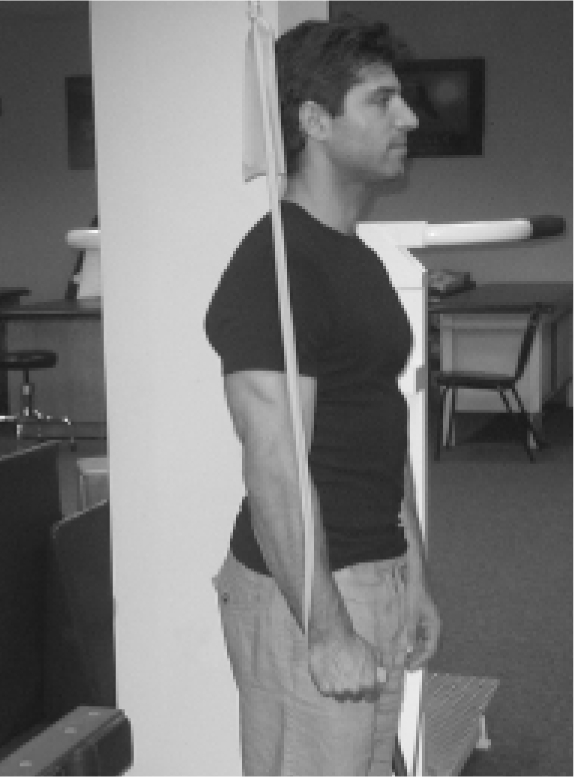
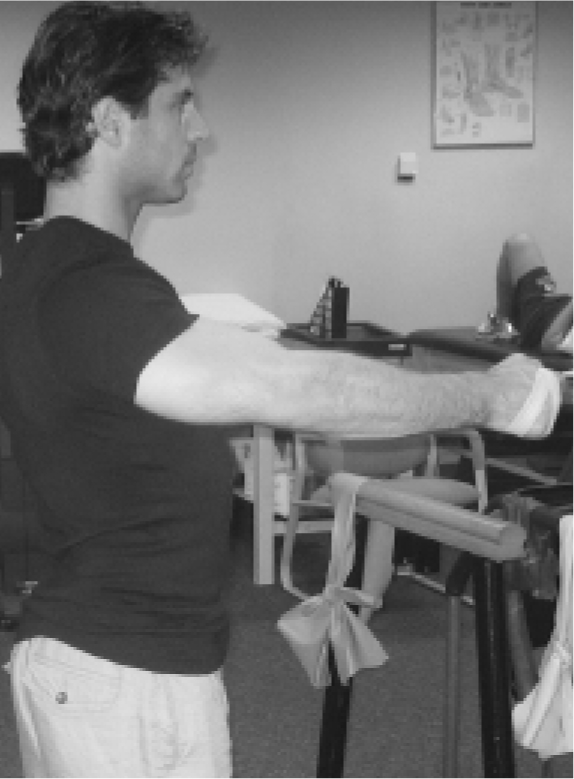
Each subject then performed five repetitions of four selected isotonic therapeutic exercises as illustrated in Figures 1 to 4. The four exercises were as follows: 1) the press-up (Figure 1), 2) unilateral scapular retraction with the shoulder positioned at 80° of shoulder flexion (Figure 2), 3) bilateral shoulder external rotation (Figure 3), and 4) unilateral scapular depression (Figure 4). Exercises two through four were performed with the use of Theraband® (The Hygenic Corporation, Akron, Ohio) to provide resistance. The subjects began the exercises from a position in which the elastic resistance was just taut and permitted them to complete five repetitions with correct form. The level of resistance was adjusted based on the subject reporting a moderate level of effort to complete the five repetitions. All exercises were performed with a 4-second cadence as determined by the senior author (2 seconds for each concentric and eccentric phase). Each testing repetition was separated by a 5 second rest period.
Figure 1.
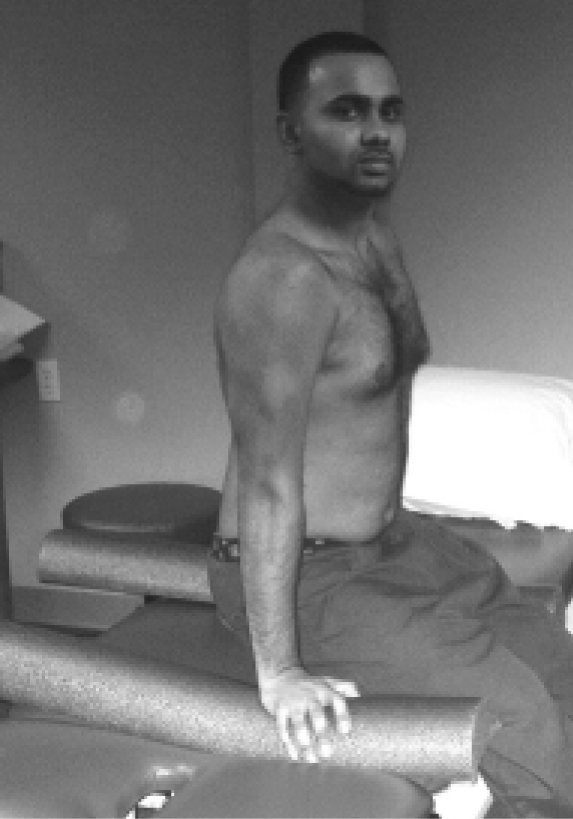
Seated press up
Figure 4.
Unilateral shoulder depression
Figure 2.
Unilateral scapular retraction
Figure 3.

Bilateral shoulder external rotation
All subjects became familiar with the exercises during a pretest session that took place just prior to the testing session. During this pretest session, each subject received instructions regarding proper execution of exercises. Each subject performed 3 to 5 practice repetitions of each exercise to ensure that they executed the exercises with correct biomechanics and rate of movement as determined by the senior author. The exercises were performed in random order to avoid bias from order effects.
Data Processing
The raw EMG data for all MVIC trials and exercise repetitions were full-wave rectified and processed using a root-mean-square algorithm with a 20-ms moving window. All data were low-pass filtered with a fourth order Butterworth filter with a 10Hz cut-off frequency. After processing, the maximum EMG activity recorded for each muscle during the MVICs was determined and used to normalize the trial data. The sampling rate was set at a 1000 Hz per channel. An average of the peak maximum activation values (% MVIC) for the middle three repetitions of each exercise was then calculated for each muscle. Muscle activity during each exercise was categorized according to the criteria proposed by McCann20: minimal (0% to 20% MVIC, moderate (21 to 50% MVIC), or marked (>50% MVIC).
Data Analysis
One-way repeated measures analysis of variance (ANOVA) was applied to the data to determine if significant differences existed in EMG activity between muscles for each exercise. Bonferoni corrections were used for pair-wise comparisons between muscles.
RESULTS
Electromyography Exercise Data
The normalized EMG data, including mean and standard deviation, for each muscle during each exercise is displayed in Table 2. The distribution of the EMG activity for each exercise is shown by box-and-whisker plots in Figures 5 to 8. The EMG data for each muscle during each exercise was found to be normally distributed.
Table 2.
Mean (± SD) EMG activity of the lower trapezius (LT), middle trapezius (MT), upper trapezius (UT), and serratus anterior (SA) muscles expressed as a percentage of maximum voluntary isometric contraction (MVIC) for four selected exercises.
| Exercise | UT %MVIC | MT %MVIC | LT %MVIC | SA %MVIC |
|---|---|---|---|---|
| 1. Press Up | 27 (32) | 32 (16) | 56 (23) †† | 44 (35) |
| 2. Scapular Retraction | 62 (44) | 50 (36) | 51 (29) | 26 (23)§ |
| 3. B/L Shld. ER | 17 (18) ** | 37 (19) * | 40 (12) * | 29 (32) |
| 4. Scapular Depression | 20 (17) | 19 (19) | 21(16) | 41 (38) † |
Significantly greater than UT activity. (p< 0.05)
Significantly less than MT and LT activity, but not significantly different from SA activity. (p< 0.05)
Significantly greater than UT and MT activity, but not significantly different than LT activity. (p< 0.05)
Significantly greater than UT and MT activity, but not significantly greater than SA activity. (p< 0.05)
Significantly less than UT, MT, and LT activity. (p< 0.05)
Figure 5.

Box-and-whisker plot showing muscle activity, as expressed as % MVIC, of the upper trapezius (UT), middle trapezius (MT), lower trapezius (LT), and serratus anterior (SA) during press-up exercise. The boxes in the plots represent the 25th and 75th percentiles. The line in the box represents the 50th percentile. The whiskers represent the highest and lowest values in the data.
Figure 8.

Box-and-whisker plot showing muscle activity, as expressed as % MVIC, of the upper trapezius (UT), middle trapezius (MT), lower trapezius (LT), and serratus anterior (SA) during scapular depression. The boxes in the plots represent the 25th and 75th percentiles. The line in the box represents the 50th percentile. The whiskers represent the highest and lowest values in the data.
Figure 6.

Box-and-whisker plot showing muscle activity, as expressed as % MVIC, of the upper trapezius (UT), middle trapezius (MT), lower trapezius (LT), and serratus anterior (SA) during scapular retraction. The boxes in the plots represent the 25th and 75th percentiles. The line in the box represents the 50th percentile. The whiskers represent the highest and lowest values in the data.
Figure 7.

Box-and-whisker plot showing muscle activity, as expressed as % MVIC, of the upper trapezius (UT), middle trapezius (MT), lower trapezius (LT), and serratus anterior (SA) during bilateral shoulder external rotation. The boxes in the plots represent the 25th and 75th percentiles. The line in the box represents the 50th percentile. The whiskers represent the highest and lowest values in the data.
DISCUSSION
Press-Up
This exercise elicited marked EMG activity of the lower trapezius (56±23% MVIC). Only one other study was identified which found exercises performed below 90° of humeral elevation that produced comparable levels of lower trapezius EMG activity. Ekstrom et al32 determined that shoulder abduction performed below 80° in the plane of the scapula elicited 50±21% MVIC of the lower trapezius while prone unilateral rowing produced 45±17% MVIC. Only moderate upper trapezius muscle activity (27±32% MVIC) was found during the press-up exercise whereas Ekstrom et al32 reported marked upper trapezius activity during shoulder abduction below 80° (72±19% MVIC) and during unilateral rowing (63±17% MVIC). During the press-up, the muscle activity level of lower trapezius (56±23% MVIC) was more than twice (2.07) the level of upper trapezius activity (27±32% MVIC). In cases where excessive scapular elevation is observed, the press-up exercise may be beneficial in promoting scapular depression.
To date, only one prior study reported lower trapezius muscle activity during closed chain exercises performed with the shoulders below 90°. Lear and Gross34 reported that three variations of a push-up activated the lower trapezius to levels of less than 40% MVIC. Since standard deviations of EMG activity were not reported by Lear and Gross34 in this study, no comparisons can be made on the variability of muscle activity levels between the press-up exercise and the push-up exercises. A biomechanical explanation of the muscle activity recorded during the press-up exercise is that an inferior directed moment is imposed on the scapula from the bodyweight of the subjects. The lower trapezius would, theoretically, function to prevent the scapula from being displaced superiorly. Since several authors have advocated the use of closed chain exercises for shoulder rehabilitation,39–46 the press-up exercise is an exercise that clinicians may use as a component of a scapular stabilization program.
Scapular Retraction
Scapular retraction produced marked activity of both the lower trapezius (51±29% MVIC) and upper trapezius (62±44% MVIC) while eliciting moderate activity of the middle trapezius (50±36% MVIC). This exercise elicited lower trapezius %MVIC that was very similar to the exercise in the study by Ekstrom et al32 in which shoulder abduction in the plane of the scapula below 80° was performed (50±21% MVIC). An important function of the scapula is retraction and protraction along the thoracic wall.5 The primary function of the upper and middle trapezius muscles are to pull the scapula posterior and medially during retraction.10 The lower trapezius has an important stabilizing and eccentric role against the laterally directed moment on the scapula created by the serratus anterior.10,47–48 Throwing athletes with posterior glenohumeral tightness may demonstrate excessive scapular protraction at follow-through,49 which is thought to decrease the subacromial space and increase risk for impingement.5 Therefore, the scapular retraction exercise may be more beneficial in cases where such excessive scapular protraction is evident as this exercise involves training the lower trapezius more specifically to promote medial-lateral stabilization of the scapula.
Bilateral Shoulder External Rotation
This exercise elicited moderate levels (40±12% MVIC) and minimal levels of upper trapezius activity (17±18% MVIC). This exercise was expected to elicit greater lower trapezius activity in order to stabilize the scapula against the supero-lateral moments imposed on the scapula by the external rotators. However, this exercise was the most effective in isolating the lower trapezius from the upper trapezius. The ratio of lower trapezius to upper trapezius muscle activity was the highest (2.35) of the four exercises studied. Subsequently, although this bilateral external rotation only elicited moderate lower trapezius activity, this exercise may be particularly useful in isolating the lower trapezius in cases where excessive scapular elevation is noted. A possible reason for the relatively low levels of upper trapezius muscle activity is that this bilateral external rotation was the only exercise that did not require humeral elevation and subsequent upward scapular rotation. A possible benefit is that exercise simultaneously trains the shoulder external rotators, which is a common aim in the rehabilitation of patients with shoulder pathology.
Scapular Depression
This exercise generated moderate muscle activity of the lower trapezius (21±16% MVIC) and a low ratio of lower trapezius to upper trapezius muscle activity (1.05). Subsequently, this exercise was determined to be the least successful of the four exercises in training the lower trapezius.
Limitations
Direct comparisons between previous studies and the present one is limited by methodological differences, including the types of electrodes utilized, the levels and types of resistance used, and the velocity of muscle contraction during exercises. The use of surface electrodes, as used in this study, are more susceptible to cross talk than fine wire electrodes, yet are more reliable and less invasive.50
Because this protocol was chosen to represent low load exercises, such as used in postoperative or post-injury patients, moderate resistance levels were utilized. Conversely, in the study by Ekstrom et al32 exercises were performed at a high level of intensity (85%-90% of maximum lifting capacity). The study involved a mixture of three open chain and one closed chain exercise. For the open chain exercises, a subjectively defined level of moderate resistance was used. The closed chain exercise (press-up) involved the subject raising the body against gravity and subsequently the level of resistance could not be adjusted. The resistance level of this exercise was relatively moderate as subjects felt they could perform several more repetitions of this exercise. However, the lack of standardized resistance levels used in our study limits direct comparison between exercises within this study and to exercises in previous studies. In addition, the mode of resistance differed in our study as compared to previous studies. Three of the four exercises in this study were performed with the use of elastic resistance. Previous studies primarily utilized free weights as the mode of resistance.22,31–32
Another limiting factor that was not totally controlled for was the rate at which each exercise was performed. Although exercises were performed deliberately at a slow cadence of approximately four seconds, a purely objective method to control for the rate at which exercises were performed was not used. Previous research indicates that the relationship between EMG activity and muscle force can be affected by velocity of muscle contraction.51 Sugamoto et al52 determined that scapulohumeral rhythm during shoulder motion is constant at slow speeds and variable at high speeds. Despite the limitations with respect to the level and rate of resistance, the variability of our data is consistent with previous EMG studies.14,22,50,53–55
Future studies are recommended which analyze lower trapezius muscle exercises while objectively controlling for resistance level and rate of movement. In addition, further research on lower trapezius muscle activity during exercises in patients with shoulder pathology is encouraged. The majority of the subjects in this study were young, active individuals who exercised on a regular basis. Since these exercises may be more challenging to perform for older, less active or fit individuals, or patients with shoulder pathologies, generalizing the results of this study to those populations should be taken with caution.
CONCLUSIONS
The results of this study suggest that the lower trapezius muscle is markedly activated by the press-up and scapular retraction exercises. The press-up exercise preferentially recruited the lower trapezius muscle over the middle and upper trapezius muscles, but not the serratus anterior muscle. Scapular retraction elicited marked activity of the lower and upper trapezius, however, this was not significantly greater than middle trapezius activity. Serratus anterior muscle activity was significantly less than the upper, middle, and lower trapezius muscles during scapular retraction. Bilateral shoulder external rotation and scapular depression failed to produce marked muscle activity of the lower trapezius muscle.
ACKNOWLEDGEMENTS
The authors wish to acknowledge Rudi Hiebert, ScM for his assistance with data analysis.
REFERENCES
- 1.Bagg SD, Forrest WF. Electromyographic study of the scapular rotators during arm abduction in the scapular plane. Am J Phys Med. 1986;65:111–124 [PubMed] [Google Scholar]
- 2.Doody SG, Freedman L, Waterland JC. Shoulder movements during abduction in the scapular plane. Arch Phys Med Rehabil. 1970;51:595–604 [PubMed] [Google Scholar]
- 3.Freedman L, Munro RR. Abduction of the arm in the scapular plane: Scapular and glenohumeral movements. A roentgenographic study. J Bone Joint Surg Am. 1966;48:1503–1510 [PubMed] [Google Scholar]
- 4.Inman VT, Saunders JB, Abbott LC. Observations on the function of the shoulder joint. J Bone Joint Surg. 1944;26:1–30 [DOI] [PubMed] [Google Scholar]
- 5.Kibler WB. The role of the scapula in athletic shoulder function. Am J Sports Med. 1998;26:325–337 [DOI] [PubMed] [Google Scholar]
- 6.Ludewig PM, Cook TM. Alterations in shoulder kinematics and associated muscle activity in people with symptoms of shoulder impingement. Phys Ther. 2000;80:276–291 [PubMed] [Google Scholar]
- 7.Poppen NK, Walker PS. Normal and abnormal motion of the shoulder. J Bone Joint Surg Am. 1976;58:195–201 [PubMed] [Google Scholar]
- 8.Harner CD, Fu FH, Klein AH. Shoulder impingement syndrome: New concepts. Fourth Annual Panther Sports Medicine Symposium-Current Concepts of the Shoulder in Throwing Sports Pittsburgh,PA and Raquet: November 29-December 1, 1990 [Google Scholar]
- 9.Jobe CM. Superior glenoid impingement. Current concepts. Clin Orthop Relat Res. 1996;330:98–107 [PubMed] [Google Scholar]
- 10.Johnson G, Bogduk N, Nowitzke A, et al. Anatomy and actions of the trapezius muscle. Clin Biomech. 1994;9:44–50 [DOI] [PubMed] [Google Scholar]
- 11.Kamkar A, Irrgang JJ, Whitney SL. Nonoperative management of secondary shoulder impingement syndrome. J Orthop Sports Phys Ther. 1993;17:212–222 [DOI] [PubMed] [Google Scholar]
- 12.Norkin CC, Levangie PK. Joint Structure and Function. Philadelphia, PA: FA Davis Co; 1992 [Google Scholar]
- 13.Cools AM, Witrouw EE, Declercq GA, et al. Evaluation of isokinetic force production and associated muscle activity in the scapular rotators during a protraction-retraction movement in overhead athletes with impingement syndrome. Br J Sports Med. 2004;38:64–68 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Cools AM, Witrouw EE, Declercq GA, et al. Scapular muscle recruitment patterns: Trapezius muscle latency with and without impingement syndromes. Am J Sports Med. 2003;31:542–549 [DOI] [PubMed] [Google Scholar]
- 15.Glousman R, Jobe F, Tibone J, et al. Dynamic electromyographic analysis of the throwing shoulder with glenohumeral instability. J Bone Joint Surg Am. 1988;70:220–226 [PubMed] [Google Scholar]
- 16.Kibler WB. Role of the scapula in the overhead throwing motion. Contemp Orthop. 1991;22:525–532 [Google Scholar]
- 17.Kuhn JE, Plancher KD, Hawkins RJ. Scapular winging. J Am Acad Orthop Surg. 1995;3:319–325 [DOI] [PubMed] [Google Scholar]
- 18.Ludewig PM, Cook TM, Nawoczenski DA. Three-dimensional scapular orientation and muscle activity at selected positions of humeral elevation. J Orthop Sports Phys Ther. 1996;24:58–63 [DOI] [PubMed] [Google Scholar]
- 19.Lukasiewicz AC, McClure P, Michener L, et al. Comparison of 3-dimensional scapular position and orientation between subjects with and without shoulder impingement. J Orthop Sports Phys Ther. 1999;29:574–586 [DOI] [PubMed] [Google Scholar]
- 20.McCann PD, Wootten ME, Kadaba MP, et al. A kinematic and electromyographic study of shoulder rehabilitation exercises. Clin Orthop Relat Res. 1993;288:179–188 [PubMed] [Google Scholar]
- 21.Morrison DS, Greenbaum BS, Einhorn A. Shoulder impingement. Orthop Clin North Am. 2000;31:285–293 [DOI] [PubMed] [Google Scholar]
- 22.Moseley JB, Jobe FW, Pink M, et al. EMG analysis of the scapular muscles during a shoulder rehabilitation program. Am J Sports Med. 1992;20:28–134 [DOI] [PubMed] [Google Scholar]
- 23.Rowe PA, Pink M, Jobe FW, et al. The normal and the painful shoulders during the breaststroke. Electromyographic and cinematographic analysis of twelve muscles. Am J Sports Med. 1994;22:789–796 [DOI] [PubMed] [Google Scholar]
- 24.Sahrmann SA. Diagnosis and Treatment of Movement Impairment Syndromes. St Louis: Mosby; 2002 [Google Scholar]
- 25.Scovazzo ML, Browne A, Pink M, et al. The painful shoulder during freestyle swimming: an electromyographic cinematographic analysis of twelve muscles. Am J Sports Med. 1991;19:577–582 [DOI] [PubMed] [Google Scholar]
- 26.Wadsworth DJ, Bullock-Saxton JE. Recruitment of the scapular rotator muscles in freestyle swimmers with subacromial impingement. Int J Sports Med. 1997;18:618–624 [DOI] [PubMed] [Google Scholar]
- 27.Warner JP, Micheli LJ, Arslenian LE, et al. Scapulothoracic motion in normal shoulders and shoulders with glenohumeral instability and impingement syndrome. A study using Moire topographic analysis. Clin Orthop Relat Res. 1992;285:191–199 [PubMed] [Google Scholar]
- 28.Kessel L, Watson M. The painful arc syndrome: Clinical classification as a guide to management. J Bone Joint Surg Br. 1977;59:166–172 [DOI] [PubMed] [Google Scholar]
- 29.Pappas AM, Zawacki RM, McCarthy CF. Rehabilitation of the pitching shoulder. Am J Sports Med. 1985;13:223–235 [DOI] [PubMed] [Google Scholar]
- 30.Watson CJ, Schenkman M. Physical therapy management of isolated serratus anterior muscle paralysis. Phys Ther. 1994;75:194–202 [DOI] [PubMed] [Google Scholar]
- 31.Ballantyne BT, O'Hare SJ, Paschall JL, et al. Electromyographic activity of selected shoulder muscles in commonly used therapeutic exercises. Phys Ther. 1993;73:668–677 [DOI] [PubMed] [Google Scholar]
- 32.Ekstrom RA, Donatelli RA, Soderberg GL. Surface electromyographic analysis of exercises for the trapezius and serratus anterior muscles. J Orthop Sports Phys Ther. 2003;33:247–258 [DOI] [PubMed] [Google Scholar]
- 33.Filho JG, Furlani J, De Freitas V. Electromyographic study of the trapezius muscle in free movements of the arm. Electromyogr Clin Neurophysiol. 1991;31:93–98 [PubMed] [Google Scholar]
- 34.Lear LJ, Gross MT. An electromyographical analysis of the scapular stabilizing synergists during a push-up progression. J Orthop Sports Phys Ther. 1998;28:146–157 [DOI] [PubMed] [Google Scholar]
- 35.Saha AK. Studies on electromyographic changes of muscles acting on the shoulder joint complex. Calcutta Med J. 1956;53:409–413 [Google Scholar]
- 36.Wiedenbaurer MM, Mortenson OA. An electromyographic study of the trapezius muscle. Am J Phys Med. 1952;31:363–371 [PubMed] [Google Scholar]
- 37.Basmajian JV, Deluca CJ. Muscles Alive: Their Functions Revealed by Electromyography. (5th Ed), Baltimore: Williams & Wilkins; 1985 [Google Scholar]
- 38.Daniels L, Worthingham C. Muscle Testing Techniques of Manual Examination. (5th Ed), Philadelphia: W.B. Saunders Company; 1986 [Google Scholar]
- 39.Davies GJ, Dickoff-Hoffman S. Neuromuscular testing and rehabilitation of the shoulder complex. J Orthop Sports Phys Ther. 1993;18:449–458 [DOI] [PubMed] [Google Scholar]
- 40.Kibler WB. Biomechanical analysis of the shoulder during tennis activities. Clin Sports Med. 1995;14:79–85 [PubMed] [Google Scholar]
- 41.Lephart SM. Scientific rationale and physiologic effects of closed kinetic chain in upper extremity rehabilitation. Presented at the Closed Kinetic Chain in Sports Rehabilitation: Scientific Basis and Functional Application Conference, Sponsored by the National Athletic Trainer's Association, American Physical Therapy Association and United States Olympic Committee, Birmingham, AL, Feb 4-5,1995 [Google Scholar]
- 42.Stone JA, Partin NB, Leuken JS, et al. Upper extremity proprioceptive training. J Athl Train. 1994;29:15–18 [PMC free article] [PubMed] [Google Scholar]
- 43.Stone JA, Leuken JS, Partin NB, et al. Closed kinetic chain rehabilitation for the glenohumeral joint. J Athl Train. 1993;28:34–37 [PMC free article] [PubMed] [Google Scholar]
- 44.Tippett SR. Closed chain exercise. Orthop Phys Ther Clinic North Am. 1992;1:253–267 [Google Scholar]
- 45.Wilk KE. Closed and open kinetic chain exercise and testing for the upper extremity. Presented at the Closed Kinetic Chain in Sports Rehabilitation: Scientific Basis and Functional Application Conference, Sponsored by the National Athletic Trainer's Association, American Physical Therapy Association and United States Olympic Committee, Birmingham, AL, Feb 4-5, 1995 [Google Scholar]
- 46.Wilk KE, Arrigo C. Current concepts in the rehabilitation of the athletic shoulder. J Orthop Sports Phys Ther. 1993;19:365–378 [DOI] [PubMed] [Google Scholar]
- 47.Arroyo JS, Hershon SJ, Bigliani LU. Special considerations in the athletic throwing shoulder. Orthop Clin North Am. 1997;28:69–78 [DOI] [PubMed] [Google Scholar]
- 48.Wilk KE, Meister K, Andrews JR. Current concepts in the rehabilitation of the overhead Athlete. Am J Sports Med. 2002;30:136–151 [DOI] [PubMed] [Google Scholar]
- 49.Flesig GS, Dillman CJ, Andrews JR. Biomechanics of the shoulder during throwing. In: Andrews JR, Wilk KE. The Athlete's Shoulder. New York, Churchill Livingstone; 1994: 355–368 [Google Scholar]
- 50.Hintermeister RA, Lange GW, Schultheis JM, et al. Electromyographic activity and applied loads during shoulder rehabilitation exercises using elastic resistance. Am J Sports Med. 1998;26:210–220 [DOI] [PubMed] [Google Scholar]
- 51.Soderberg GL. Selected Topics in Surface Electromyography for Use in the Occupational Setting: Expert Perspectives. U.S. Department of Health and Human Services, Public Health Service, Centers for Disease Control, National Institute of Occupational Safety and Health. Washington DC: Government Printing Office, 1992(DHHS/NIOSH). Publication NO. 91-100 [Google Scholar]
- 52.Sugamoto K, Hareda T, Machida A, et al. Scapulohumeral rhythm: Relationship between motion velocity and rhythm. Clin Orthop Rel Res. 2002;401:119–124 [DOI] [PubMed] [Google Scholar]
- 53.Decker MJ, Hintermeister RA, Faber KJ, et al. Serratus anterior muscle activity during selected rehabilitation exercises. Am J Sports Med. 1999;27:784–791 [DOI] [PubMed] [Google Scholar]
- 54.Kelly BT, Backus SI, Russell WF, et al. Electromyographic analysis and phase definition of the overhead football throw. Am J Sports Med. 2003;30:837–844 [DOI] [PubMed] [Google Scholar]
- 55.Reinold MM, Wilk KE, Flesig GS, et al. Electromyographic analysis of the rotator cuff and deltoid musculature during common shoulder external rotation exercises. J Orthop Sports Phys Ther. 2004;34:385–394 [DOI] [PubMed] [Google Scholar]