

Abstract
Background
Many sports involve movements during which the lower extremity functions as a closed kinetic chain, requiring weight-bearing (WB) range of motion (ROM). Assessment of the capacity for internal and external rotation motion at the hip is typically performed with the individual in a prone, supine, or seated position. Such measurements represent ROM in a non-weight bearing (NWB) position, and, as a result, may not appropriately assess the capacity of the joint to meet the demands of the athlete's sport. To date, no research exists which documents WB hip ROM in golfers relative to the ROM demands of the golf swing or the symmetry of weight-bearing hip rotation ROM in female golfers.
Objectives
Weight-bearing hip rotation ROM was measured in female golfers and compared to the actual hip rotation ROM that occurred during a full golf swing.
Methods
Fifteen right-handed, female collegiate golfers participated in the study. The WB hip rotation ROM was measured during three different stance conditions and during full golf swings using a custom-built testing device. These actions were captured using a 3-D motion analysis system.
Results
The golfers WB ROM was symmetrical for external rotation and internal rotation, p = 0.648 and p = 0.078, respectively. During the backswing, the golfers used approximately 20-25% of their available WB right internal rotation, and 50-75% of their available WB left external rotation. For the downswing, the golfers used approximately 34-37% of their available WB right external rotation and 84-131% of their available WB left internal rotation. The golfers used significantly more external and internal hip rotation ROM on the left (lead) hip during both phases of the full golf swing (p < 0.001), demonstrating an asymmetrical movement pattern.
Discussion
In general, golfers did not exceed the measured WB ROM limits during the golf swing but did demonstrate decreased WB internal rotation on the lead hip.
Conclusion
Clinicians need to pay special attention to functional (WB) hip rotation ROM in female golfers in order to assess injury risk related to the rotational hip asymmetry present during the golf swing.
Keywords: golf, hip rotation ROM, symmetry
INTRODUCTION
Several studies1–8 have examined hip range of motion (ROM) in athletes and other healthy adults, but the normative values that they report appear to be somewhat different. Part of the reason for such discrepancies may be that there have been different methodologies employed regarding the type of motion measured (active vs. passive), as well as in the position used during the measurement (prone, supine, or seated). Despite this variability, common agreement exists that passive ROM is greater than active ROM.9
Interestingly, most activities of daily living, as well as sports, occur with a majority of the time spent in weight-bearing (WB). However, when assessing available joint ROM, measurements are frequently performed in non weight-bearing (NWB). Currently, no published normative data exists regarding available WB hip rotation ROM's. For the athlete, a more functional assessment in the WB position may be required to determine if there is an adequate amount of hip rotation ROM necessary for a particular sport, skill, or motion.
Golf is a non-contact sport; however, injuries do occur. The leading site of injury among both professional and amateur golfers is the spine.10–12 Interestingly, of the available injury survey studies, very few report hip injuries.12–18 Although a small number of reported cases of hip injuries in golfers exist, Cibulka3 has described an association between low back pain and hip rotation ROM asymmetry in the non-golfing population. Currently, the normal or typical amount of hip rotation the lead and trail hip each undergo during the full golf swing is unknown.
If the repetitive motion of the golf swing occurs in an asymmetrical movement pattern, then asymmetrical hip rotation ROM may develop. Thus, a critical link may exist between golfers' available hip rotation ROM and their susceptibility to low back pain.
One recent investigation examined the association between low back pain and hip rotation ROM in Professional Golf Association (PGA) golfers.19 The authors found a decreased amount of internal rotation on the lead hip in those with low back pain and a similar, although non-significant trend, in healthy golfers. As a result of that study, whether playing golf repetitively alters side-to-side hip rotation ROM symmetry or if low back pain creates the asymmetrical measurement is unknown. But, due to the fact that there was a similar trend in healthy golfers, this may suggest that playing golf repetitively could alter side-to-side hip rotation ROM. Further support for side to side asymmetry exists in a recent study published by Gulgin et al.20 They found almost one-fourth of a group of Ladies' Professional Golf Association (LPGA) golfers showed a side-to-side asymmetry of more than five degrees in IR. Thus, these previous investigations provide an indication that a golfer's hip rotation ROM may adapt to the demands placed upon the hip.
Currently, no data exist documenting WB hip rotation in golfers or data that illustrates the actual amount of hip rotation ROM that occurs during the full golf swing. Thus, the purpose of this study was to measure WB hip rotation ROM in female golfers during the full golf swing and compare this to their available WB hip rotation ROM as measured in varied stance positions.
METHODS
Fifteen female golfers (mean age 19.6 ± 1.4 yrs; ht. 163.3 ± 6.5 cm; wt. 59.5 ± 6.6 kg; hdcp 5.2 ± 3.3) participated in the study. All subjects were right-hand dominant, played right-handed, and were screened to exclude those with a history of any hip or back pain within the past six months. Prior to participation, subjects signed a written consent form as approved by the University of Toledo Human Subjects Research Review Committee.
The subjects reported to the laboratory on one occasion. Prior to the WB ROM measurements, all subjects pedaled for five minutes on a stationary bicycle as a general warm-up. The available WB ROM of hip rotation was measured under three stance conditions, and then subjects performed approximately ten full golf swings with a driver. Video data of all the trials (WB ROM and golf swing) was collected. A three-dimensional (3D) motion capture system (Motion Analysis Corporation, Santa Rosa, CA) was used to quantify the hip rotation movements of each subject (Figure 1). The EVa 7.0 and KinTrak software (Motion Analysis Corporation, Santa Rosa, CA) were used for all data acquisition and processing. Eight Falcon High Resolution cameras (Motion Analysis Corporation, Santa Rosa, CA), sampling at 120 Hz were used for capturing the movement of the retroflective markers on each subject. The various markers were placed on all subjects by the same investigator over the anatomical landmarks listed in Table 1. For obtaining WB hip rotation measurements, subjects stood on a custom-built wooden base so that one foot was fixed (stable), while the other foot (the involved leg used for measurement) was free to rotate on the moveable circular disk (Figure 2, Table 1). The subjects were asked to maintain equal weight distribution on the right and left lower extremities during the measurement. All subjects were measured in three different WB conditions. For Condition A (WBa), the subject stood erect (hips and knees extended) with the stance width equal to the distance between the greater trochanters. Reliability for repeated measurements of hip rotation ROM measured in Condition A (WBa) was 0.819 (Cronbach's Alpha), and thus, the set up was used for the remainder of conditions as well. For Condition B (WBb), the subjects stood erect (hips and knees extended) with stance width equal to the distance between the lateral border of feet when using a self-selected golf set-up position (for a driver). For Condition C (WBc), subjects were positioned in the same stance width as Condition B, but also with the amount of hip and knee flexion used during the self-selected golf set-up position (for a driver). For each condition, the rotating foot was aligned on the center of the board (with a tape line down for a l i g n m e n t ) . However, the starting angle of the entire rotating board was positioned to represent the subject's natural toe-in or toe-out position.Depending on which direction was being measured, the subject was asked to rotate the foot externally (or internally) as far as possible, and then return to the start position. Measurements of maximum hip IR and ER were performed bilaterally, repeating the full movement six times in each direction. In order to maintain the level of flexion in the hip and knees during data collection (WBc), the subject's initial start position was reset (using a goniometer) after every two trials. The three trials that required the least editing to produce complete marker paths were selected, tracked, processed, analyzed and the ensemble was averaged to examine the available WB hip rotation ROM. When processing the available WB ROM, any pelvic movement (ASIS vector) that occurred during the trial was subtracted from the maximum amount of foot rotation.
Figure 1.

High-speed camera set-up with full body marker set.
Table 1.
Anatomical landmarks for marker placement
| Marker Location | WB ROM Trials | Full Golf Swing Trials |
|---|---|---|
| (B) anterior superior iliac spine | Yes | Yes |
| sacrum | Yes | Yes |
| (B) greater trochanter | Yes | Yes |
| (B) anterior thigh (mid) | Yes | Yes |
| (B) lateral femoral condyle | Yes | Yes |
| (B) tibial tuberosity | Yes | Yes |
| (B) mid tibia (medial) | Yes | Yes |
| (B) low tibia (lateral) | Yes | Yes |
| (B) lateral malleolus | Yes | Yes |
| (B) calcaneus | Yes | Yes |
| (B) 5th metatarsal | Yes | Yes |
| (B) 3rd toe | Yes | Yes |
| (B) acromion | Yes | |
| (B) lateral humeral epicondyle | Yes | |
| (B) wrist (dorsum) | Yes | |
| C7 | Yes | |
| anterior forehead | Yes | |
| clubhead | Yes | |
| club shaft (distal to grip) | Yes | |
| ball | Yes |
B = bilateral
Figure 2.
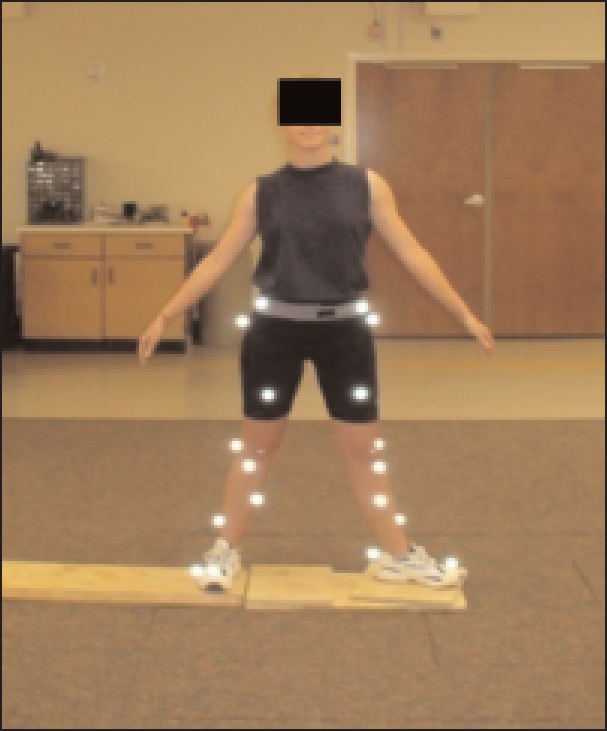
WB ROM trial.
For the assessment of the golf swing, an expanded marker set (Figure 3, Table 1) was placed on each golfer (by the same investigator), and ten golf swings were recorded. Practice swings were allowed for warm-up, as well as to allow the subject to feel comfortable performing a golf swing with the marker set in place. Each golfer assumed their natural stance width (as measured previously) and performed the swing with a standard 45″ driver. As with the WB ROM trials, the full golf swings were captured at 120 Hz. For each subject, the three trials were selected (all by same investigator) in the same manner as previously mentioned to determine for each hip the maximum internal rotation and external rotation that occurred during the golf swing.
Figure 3.
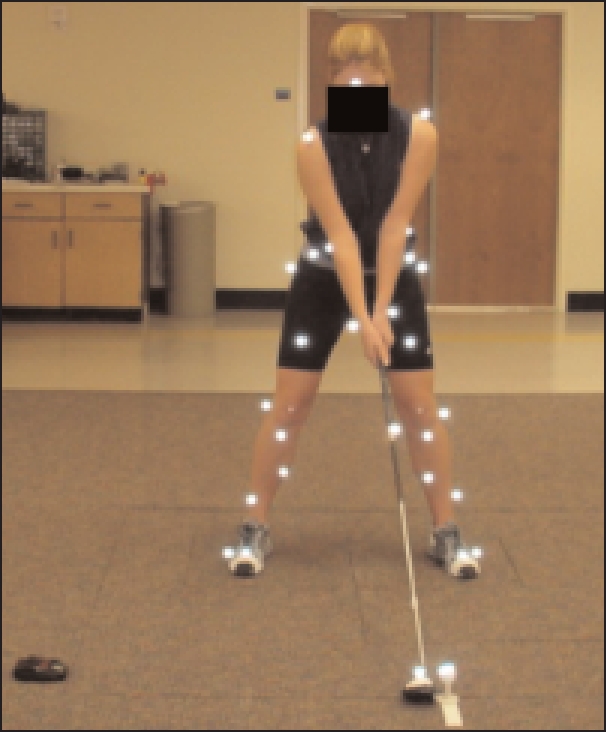
Full body marker set up.
Statistical data analysis was performed using Statistical package SPSS version 14.0 (SPSS Inc., Chicago, IL). The significance level was set at an alpha level of 0.05. Two separate two way (side x condition) repeated measures ANOVA's were utilized, one for internal rotation and one for external rotation. A post-hoc analysis was performed to verify where significant differences occurred across the conditions. For comparison of rotational hip motion ROM during the backswing and downswing phases a two way ANOVA (side x rotation) was run to test for a difference in the amount of rotation present in each hip.
RESULTS
The means and standard deviations for subject demographics are shown in Table 2. The mean stance width for WBa was less than WBb & WBc (43.0 ± 2.6 cm vs. 59.5 ± 4.6 cm respectively, Table 3). The mean hip and knee flexion used in WBc was 38.7 ± 6.0 degrees and 24.7 ± 7.0 respectively (Table 3).
Table 2.
Subject demographics.
| Descriptives | Mean ± SD (n = 15) |
|---|---|
| Age (yrs) | 19.7 ±1.4 |
| Height (cm) | 163.3 ±6.5 |
| Weight (kg) | 59.6 ±6.6 |
| Handicap | 5.2 ±3.3 |
Table 3.
WB ROM Measurement Stance Descriptions
| Stance Description | Mean ± SD (n=15) |
|---|---|
| WBa - stance width (cm) | 43.0 ± 2.6 |
| WBb - stance width (cm) | 59.5 ± 4.6 |
| WBc - stance width (cm) | 59.5 ±4.6 |
| WBc hip flexion (deg) | 38.7 ± 6.0 |
| WBc knee flexion (deg) | 24.7 ± 7.0 |
For external rotation WB ROM, no significant difference occurred between sides (p = 0.648), a non-significant interaction (p = 0.908), but a significant difference existed between conditions (p < 0.001). Post-hoc analysis reveals that WBb ROM was significantly greater than WBa in the right hip (p = 0.013, Table 4) and was approaching a significant difference in the left hip (p = 0.055, Table 4). The ER rotation measured in the WBc was significantly greater than that measured in WBb in the right hip (p < 0.001, Table 4), but was not significantly greater in the left hip (p = 0.12, Table 4). The right and left hip demonstrated symmetrical WB external rotation. However, the external rotation increased significantly in the right hip (and not the left hip) by first increasing stance width, and increased even more by adding hip and knee flexion into the measurement posture. Although the left hip experienced the same amount of increase in external rotation ROM across the three stance conditions, the standard deviations were larger on this side, potentially keeping them from the significant finding on the left hip.
Table 4.
WB ROM - Mean maximum rotation (all conditions)
| WBROM (n=15) | WBa | WBb | WBc |
|---|---|---|---|
| Right ER | 40.7 ±6.5* | 48.8 ±6.6* | 60.7 ±8.6* |
| Left ER | 39.5 ±8.3† | 48.2 ±9.4 | 59.0 ±11.1† |
| Right IR | 29.8 ±9.1 | 29.9 ±9.5 | 43.4 ±10.9** |
| Left IR | 26.5 ±9.8 | 27.2 ±10.2 | 41.1 ±8.3†† |
indicates significant difference at 0.05 level for right ER
Indicates significant difference at 0.05 level for right IR
Indicates significant difference at 0.05 level for left ER
Indicates significant difference at 0.05 level for left IR
For internal rotation WB ROM, no significant difference existed between sides (p = 0.078), a non-significant interaction (p = 0.890), but significant difference existed between conditions (p < 0.001). The means and standard deviations (Table 4) revealed that the left hip has approximately two degrees less internal rotation ROM in all conditions which is not statistically nor clinically significant. Post-hoc analysis revealed that WBa ROM was not significantly different from WBb in either the right hip, p = 1.0 or the left hip, p = 1.0 (Table 4). However, the WBc group was significantly greater than WBb in the right hip, p = 0.002 and the left hip, p = 0.001 (Table 4). Thus, for WB internal rotation, widening the stance did not significantly alter available ROM, but adding hip and knee flexion did.
When examining the amount of WB ROM the golfers used during the full golf swing compared to the WB values obtained during the three WB conditions, they did not exceed the available internal rotation or external rotation WB ROM on the right (trail) hip at any point during the golf swing (Table 5). However, during the downswing, the mean left (lead) hip internal rotation was 34.8 ± 11.7 degrees, which exceeded the golfers WB ROM available as measured during two of the WB stance conditions (WBa, WBb, Table 5). But, when the golfer's WB ROM was measured in a similar position to that used during the golf swing (condition WBc), the golfers did not exceed the available internal rotation WB ROM (Table 5).
Table 5.
Mean maximum WB ROM in comparison to WB hip ROM used during the golf swing
| WB ROM | WBa (deg) | WBb (deg) | WBc (deg) | Golf Swing ROM | % of WBa | % of WBb | % of WBc |
|---|---|---|---|---|---|---|---|
| Right TR | 29.8 ± 9.1 | 29.9 ± 9.5 | 43.4 ± 10.9 | 8.9 ±4.8 | 29.8 | 29.7 | 20.5 |
| Left ER | 39.5 ± 8.3 | 48.2 ± 9.4 | 59.0 ± 11.1 | 29.7 ±11.3* | 75.1 | 61.6 | 50.3 |
| Right ER | 40.7 ± 6.5 | 48.8 ± 6.6 | 60.7 ± 8.6 | 14.9 ± 9.6 | 36.6 | 30.5 | 24.5 |
| Left lR | 26.5 ± 9.8 | 27.2 ± 10.2 | 41.1 ± 8.3 | 34.8 ±11,7* | 131.3 | 127.9 | 84.6 |
n=15
Indicates significant difference at 0.05 level
During the backswing phase of the golf swing, the maximum right hip internal rotation was 8.9 ± 4.8 degrees, which was significantly less than maximum external rotation, 29.7 ± 11.3 degrees; p < 0.001 (Table 5), of the left hip that was occurring at the same time. During the down-swing, the subjects demonstrated the same pattern, as right hip external rotation of 14.9 ± 9.6 degrees was significantly less than left hip IR, 34.8 ± 11.7 degrees; p < 0.001 (Table 5). Thus, it would appear that the left (lead) hip experienced more rotation than the trailing hip throughout the backswing and downswing phases of the golf swing, demonstrating an asymmetrical movement pattern.
DISCUSSION
Since the position of the hip joint during measurement influences the results,7 it may be inferred that tension on the hip capsule affects this measurement. When the hip is flexed, the capsule and ligaments have more laxity, which should allow for more movement relative to a neutral hip joint (more taut hip capsule and ligaments). However, the literature refutes this line of thought, showing more hip rotation in a prone position when compared to measurements taken in a seated position.2,7 These hip rotation ROM values may then suggest that muscle length, as a result of the joint position, could be the limiting factor.
The current study revealed that less WB ROM occurred when standing erect or in hip neutral (WBa & WBb) than when hip and knee flexion were added, which places the joint capsule on slack. Thus, the results of the current study conflict with Bierma-Zienstra et al2 and Simoneau et al,7 in that, when in WB, the tautness of the hip capsule and ligament structures appear to have more of a limiting role than when measured in non-weight bearing (NWB). The studies by Bierma-Zienstra et al2 and Simoneau et al7 measured hip rotation ROM actively (NWB), which was similar to this study, as the WB measurement required active ROM. However, several factors contribute to joint ROM, such as the capsule, ligaments, surrounding muscle length, and bony congruency, making it difficult to identify the factor that was the greatest contributor to the rotational limitation.
In order to further examine the role that muscle length might play in hip rotation ROM, altered stance positions were used during data collection. Among the three stance conditions used in this study, there was variation in length of the surrounding hip musculature. For example, comparing WBa to WBb, an increase in stance width occurred in WBb, resulting in greater hip abduction. This increase in hip abduction shortens the abductors and lengthens the adductors, which may have limited the active tension that these muscles could generate to contribute to internal rotation or external rotation, limiting the WB ROM. For example, the gracilis muscle is considered an internal rotator of the hip and becomes stretched in condition WBb as hip abduction is increased. The gluteus minimus muscle can contribute to internal rotation when the hip is abducted, which could make up for the lengthened gracilis muscle. No change in WB internal rotation occurred between condition WBa and WBb on either hip (Table 4).
As for WB external rotation, a significant difference in ROM existed between condition WBa and WBb (increase in hip abduction) for the right hip, while for the left hip the difference approached a significant difference (p = 0.055). The WBb stance condition was associated with approximately 8-9 degrees more of external hip rotation than when measured in WBa condition (Table 4). When increasing the stance width and hip abduction, the gluteus medius, gluteus minimus, and tensor fascia latae muscles (all capable of producing external rotation) become shortened. But, the adductor brevis, adductor magnus, and pectineus muscles (all capable of external rotation) are lengthened. For WB external rotation, the change in muscle length of the involved musculature appeared to allow for more external rotation.
When going from a stance with an erect posture (WBa and WBb) to a stance with added hip and knee flexion (WBc), an 11-12 degree increase in WB external rotation and a 13-14 degree increase in WB internal rotation occurred (Table 4). In addition to the increased laxity in the hip capsule, most of the internal rotators are put on slack in the position of hip flexion (anterior gluteus medius, and tensor fascia latae muscles) and thus are not limiting the measurement, allowing for such an increase. However, the external rotators would be lengthened with the additional hip flexion, but not at such a length that would limit the significant increase in WB external rotation.
Prior to this study, the characteristics of weight bearing internal and external hip rotations during a golf swing had not been documented. The results of the current study demonstrate that significantly more external and internal rotation occurs on the left (lead) hip during both the back-swing and downswing phases (Table 5) than on the right (trail) hip. Thus, the golf swing necessitates an asymmetrical pattern of internal rotation and external rotation between the two hips. Previous research19–20 has shown that golfers do present with side-to-side differences in their hip internal rotation ROM, which would appear to be linked to this repetitive movement pattern. When examining golfers in a prone, NWB condition, Vad et al19 found a significant difference in side-to-side internal rotation in a sample of professional golfers. In that study, the lead hip demonstrated less internal rotation than the trail hip. Although the significant difference was only evident in the golfers with low back pain, the trend was present for healthy golfers as well. Further supporting Vad et al19, was the recent study by Gulgin et al20 that found almost one-fourth of a sample of female professional golfers had side-to-side asymmetry between the lead and trail hip of more than five degrees in internal rotation. Vad et al19 measured active hip rotation ROM and Gulgin et al20 measured passive hip rotation ROM. Although these previous investigations measured hip rotation ROM in a NWB condition, it appears that golfer's hip rotation ROM adapts to the demands placed on it by the dynamic asymmetry of the golf swing. In the current study, WB internal rotation was approximately two degrees less, although not significant, on the left (lead) hip in comparison to the right (trail) hip (Table 4). This result adds to the body of evidence of the adaptation in the golfer's lead hip internal rotation ROM, regardless of the measurement technique (NWB or WB) used.
The clinical relevance for asymmetrical hip rotation ROM between the right and left hip is that the function of the body's kinetic chain may be altered. In particular, there is a link with the spine, pelvis, and hip. When ROM is limited in one of the movement regions, the others may also be affected. In order to maintain function, when ROM is limited in one of these segments, adaptation in the movement of others is generally necessitated. The investigation of Cibulka et al3 have shown that an association exists with asymmetrical hip rotation ROM and low back pain. This finding suggests that golfers who development asymmetrical hip ROM as a result of the mechanics of the swing may be at an increased risk for low back pain over the course of their career. Interestingly, low back conditions have been reported to be the leading injury complaint among both professional and amateur golfers.10–18
Another important clinical consideration involving hip ROM is that involving the influence of hip ROM on excessive stress on the surrounding soft-tissue of the hip, which would appear to be of particular concern when the available WB ROM is not adequate to accommodate the demands of a full golf swing. The results revealed that the golfers tested did not exceed their available WB external rotation ROM on either the backswing or downswing phases (Table 5). However, the golfers averaged 34.8 ± 11.7 degrees of internal rotation on the left (lead) hip during the downswing, which exceeded their available WB ROM as measured in condition WBa and WBb. For WBa condition, the golfers required 131.3% of their available internal rotation WB ROM on the lead (left) hip, and for condition WBb, they required 127.9% of their available internal rotation WB ROM (Table 5). However, when the internal rotation WB ROM used during the golf swing is compared to a condition most similar to that used during the golf swing (WBc), the subjects did not exceed their available internal rotation WB hip rotation ROM on the lead (left) hip (Table 5). Thus, if golfers become fatigued or change their address posture (do not set up with enough flexion in the hip and knees) during a round of golf, they may begin to exceed their available WB internal rotation ROM and risk injury.
While this study provides important information about WB hip ROM and the associated hip ROM during the golf swing, several limitations exist that should be considered. First, the amount of the subject's hip torsion (anteversion or retroversion) was not taken into consideration. Participants who have a greater anteversion or retroversion angle might show limitations in one of the hip rotation measurements, while possibly having more in the opposite rotational direction. Second, tibial motion, or other kinematic contributors, may have acted differently when the knee was flexed (condition WBc) compared to when the knee was not flexed (condition WBa). The transverse plane movements of the knee or foot was not measured, because this study only focused on hip motion; thus, the influence of these other factors cannot be directly assessed for their relative contributions. The separate contributions of the lower extremity joints and anatomic factors during a transverse plane movement are areas that need to be addressed in future research. Third, the WB ROM measurements were assessed while each subject maintained equal weight distribution between the right and left sides. During the golf swing, weight shifts to the right (trail) hip during the backswing and toward the left (lead) hip during the down-swing. Alterations in weight distribution may influence hip joint kinematics.
CONCLUSION
The female golfers demonstrated symmetrical WB hip rotation ROM for IR and ER, but did demonstrate a slight decrease in WB internal rotation on the lead hip. In general, golfers did not exceed the measured WB ROM limits during the golf swing, but used significantly more hip rotation ROM on the lead hip, creating an asymmetrical movement pattern. Thus, for the athlete, WB assessment of hip ROM may be more functionally relevant than traditional NWB or more appropriate for the determination of adequate ROM for a particular sport task. Future research should focus on examination of the association between the required ROM demands of a specific sport and the amount of WB ROM available in athletes who participate in those sports. An athlete who does not have the available WB ROM needed for their sport movement may increase their risk of injury by placing excessive stresses on the relevant soft-tissues associated with the involved joint.
REFERENCES
- 1. Barbee-Ellison J, Rose S, Sahrmann S. Patterns of hip rotation range of motion: a comparison between healthy subjects and patients with low back pain. Phys Ther. 1990;70:537–541 [DOI] [PubMed] [Google Scholar]
- 2. Bierma-Zeinstra SMA, Bohnen AM, Ramlal R, et al. Comparison between two devices for measuring hip joint motions. Clin Rehabil. 1998;12:497–505 [DOI] [PubMed] [Google Scholar]
- 3. Cibulka MT, Sinacore DR, Cromer GS, et al. Unilateral hip rotation range of motion asymmetry in patients with sacroiliac joint regional pain. Spine. 1998;23:1009–1015 [DOI] [PubMed] [Google Scholar]
- 4. Ellenbecker TS, Ellenbecker GA, Roetert EP, et al. Descriptive profile of hip rotation range of motion in elite tennis players and professional baseball pitchers. Am J Sport Med. 2007;35:1371–1376 [DOI] [PubMed] [Google Scholar]
- 5. Roaas A, Andersson G. Normal range of motion of the hip, knee and ankle joints in male subjects, 30-40 years of age. Acta Orthop Scand. 1982;53:205–208 [DOI] [PubMed] [Google Scholar]
- 6. Roach KE, Miles TP. Normal hip and knee active range of motion: the relationship to age. Phys Ther. 1991;71:656–665 [DOI] [PubMed] [Google Scholar]
- 7. Simoneau GG, Hoenig KJ, Lepley JE, et al. Influence of hip position and gender on active hip internal and external rotation. J Orthop Sport Phys. 1998;28:158–164 [DOI] [PubMed] [Google Scholar]
- 8. Svenningsen S, Terjesen T, Auflem M, et al. Hip motion related to age and sex. Acta Orthop Scand. 1989;60:97–100 [DOI] [PubMed] [Google Scholar]
- 9. Norkin C, White D. Measurement of Joint Motion. A Guide to Goniometry. 3rd ed. Philadelphia, PA: F.A. Davis Company, 2003 [Google Scholar]
- 10. Grimshaw PN, Burden AM. Case report: reduction of low back pain in a professional golfer. Med Sci Sport Exer. 2000; 32:1667–1673 [DOI] [PubMed] [Google Scholar]
- 11. Lindsay DM, Horton JF, Vandervoort AA. A review of injury characteristics, aging factors and prevention programmes for the older golfer. Sports Med. 2000;30:89–103 [DOI] [PubMed] [Google Scholar]
- 12. McCarroll J. The frequency of golf injuries. Clin Sport Med. 1996;15:1–7 [PubMed] [Google Scholar]
- 13. Batt M. A survey of golf injuries in amateur golfers. Brit J Sport Med. 1992;26:63–65 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Gosheger G, Liem D, Ludwig K, et al. Injuries and overuse syndromes in golf. Am J Sport Med. 2003;31:438–443 [DOI] [PubMed] [Google Scholar]
- 15. Grimshaw P, Giles A, Tong R, et al. Lower back and elbow injuries in golf. Sports Med. 2002;32:655–666 [DOI] [PubMed] [Google Scholar]
- 16. McCarroll J, Rettig A, Shelbourne K. Injuries in the amateur golfer. Physician Sports Med. 1990;18:122–126 [DOI] [PubMed] [Google Scholar]
- 17. McCarroll J, Gioe T. Professional golfers and the price they pay. Physician Sports Med. 1982;10:64–70 [DOI] [PubMed] [Google Scholar]
- 18. Theriault G, Lachance P. Golf injuries. An overview. Sports Med. 1998;26:43–57 [DOI] [PubMed] [Google Scholar]
- 19. Vad VB, Bhat AL, Basrai D, et al. Low back pain in professional golfers. The role of associated hip and low back range-of-motion deficits. American J Sport Med. 2004;32:494–497 [DOI] [PubMed] [Google Scholar]
- 20. Gulgin H, Armstrong A, Gribble P. Passive hip rotation range of motion in LPGA golfers. Clinical Kinesiology. 2008;62:9–15 [Google Scholar]