

Abstract
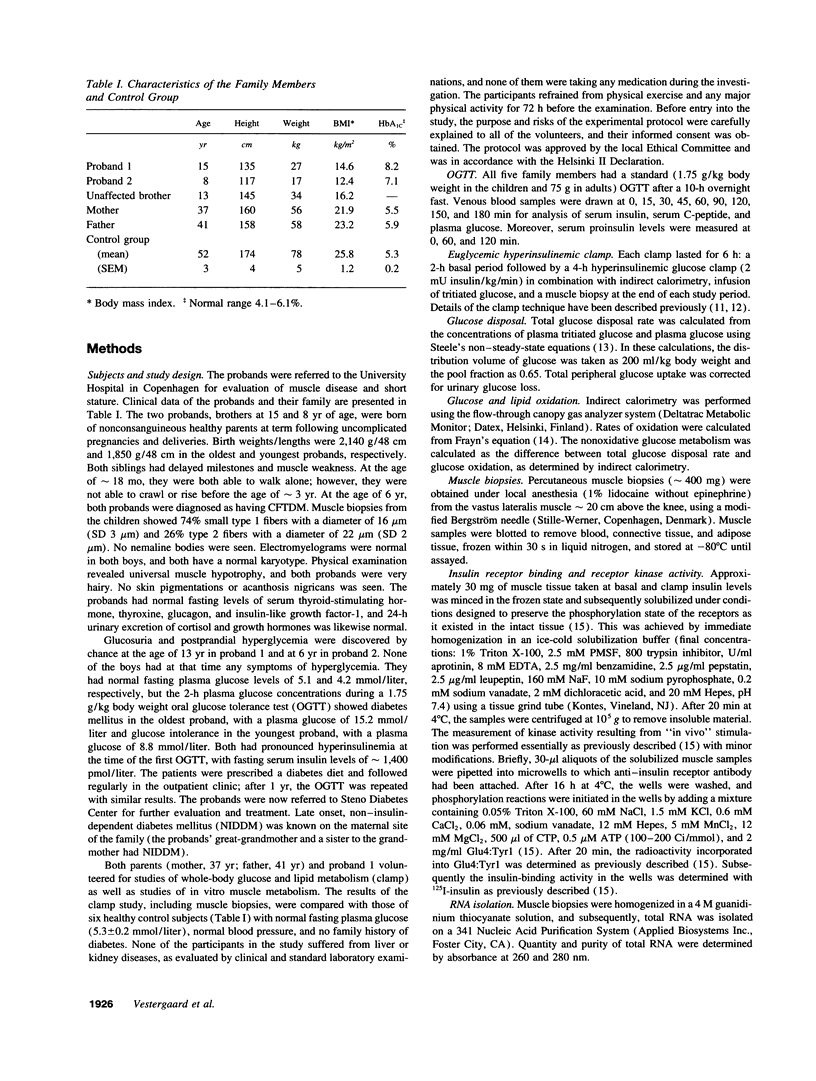
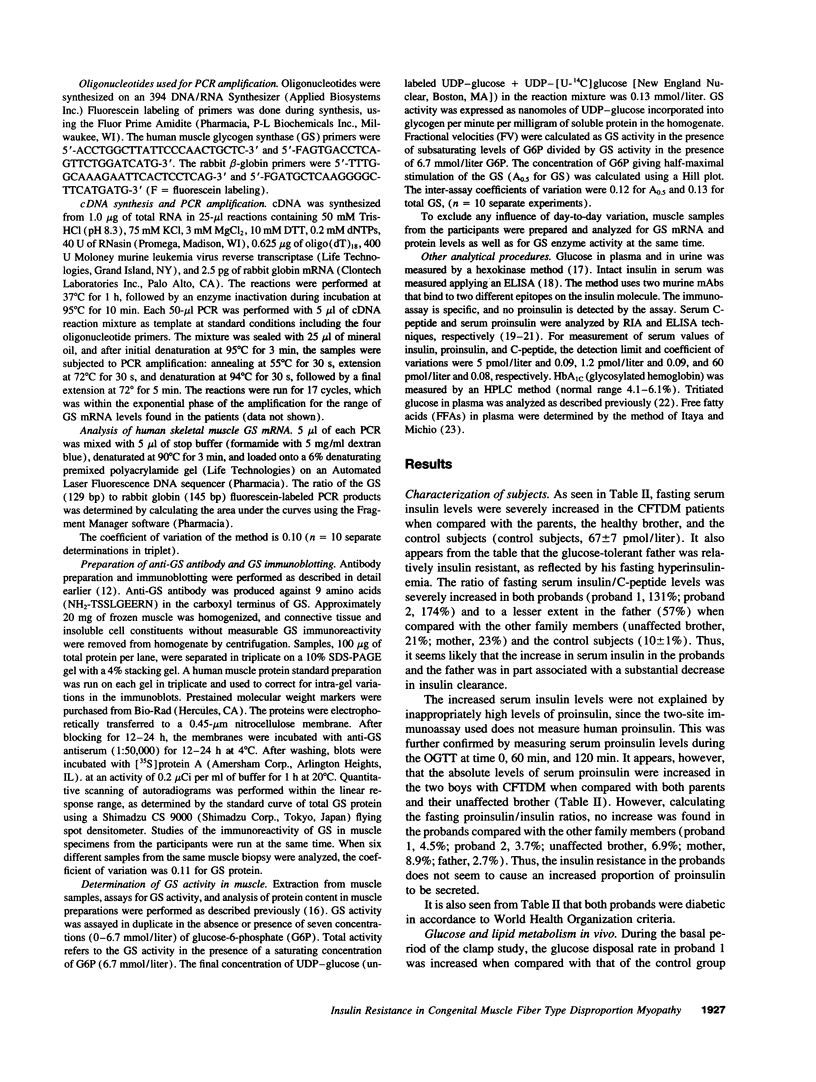
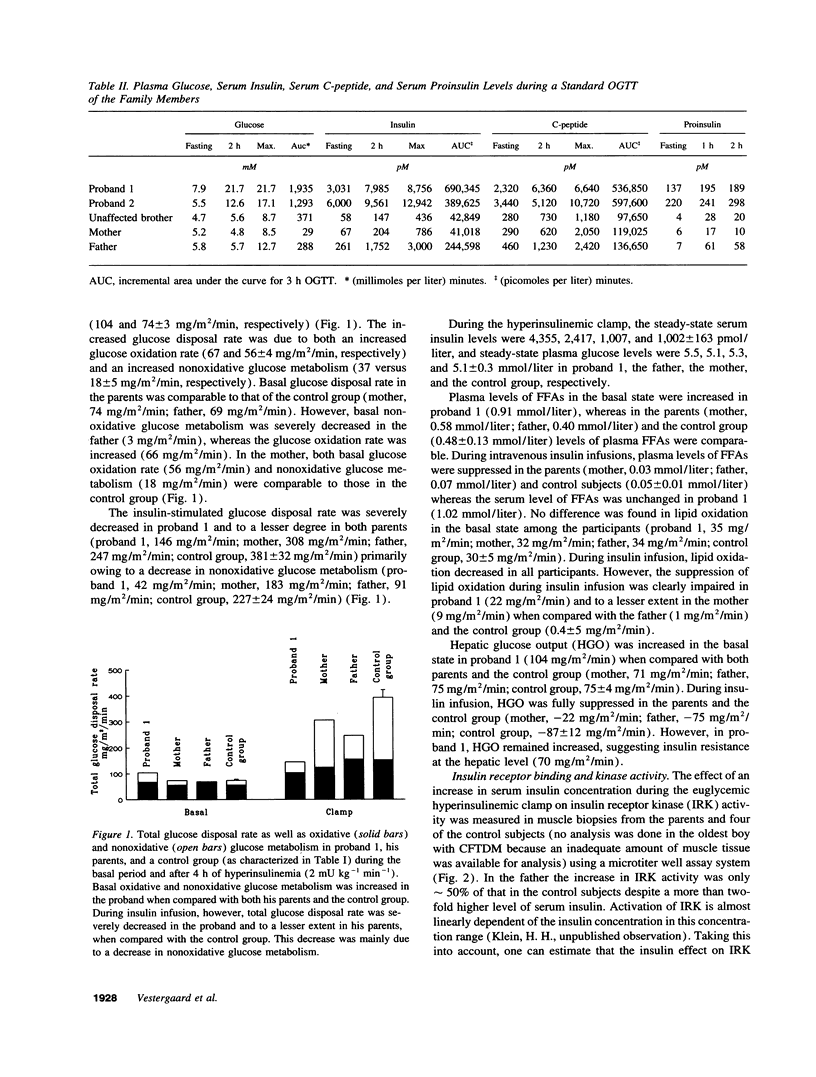
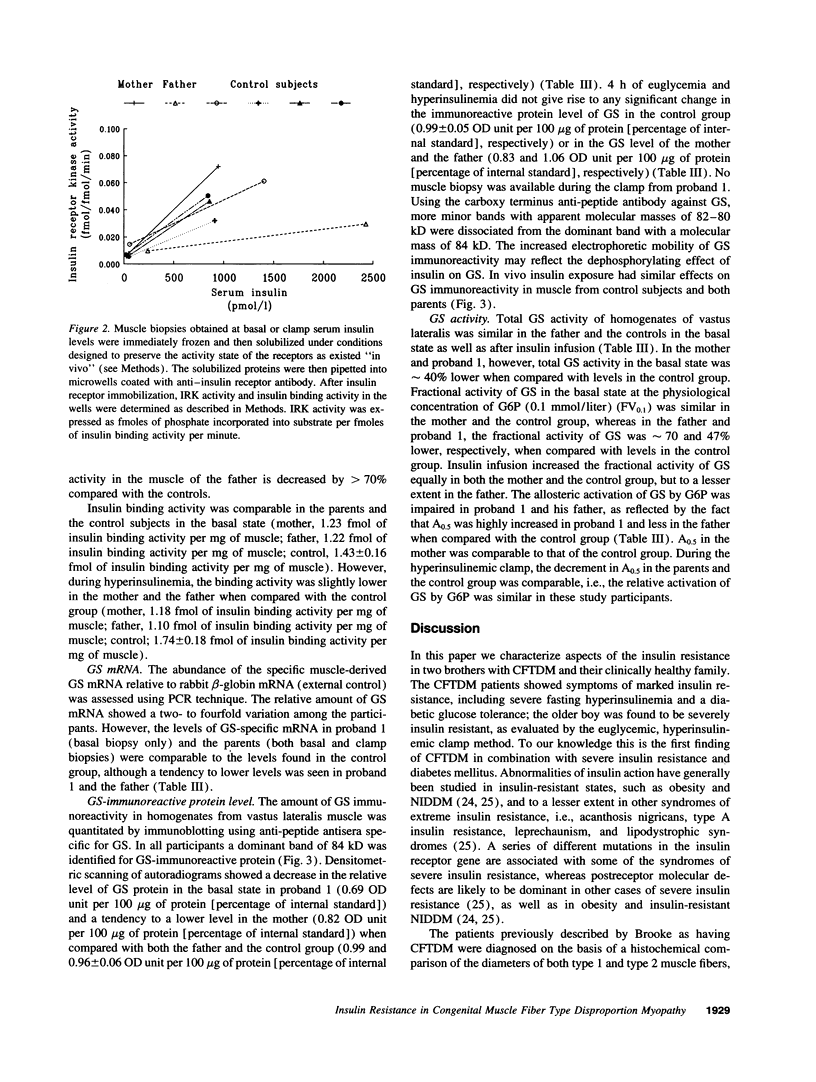
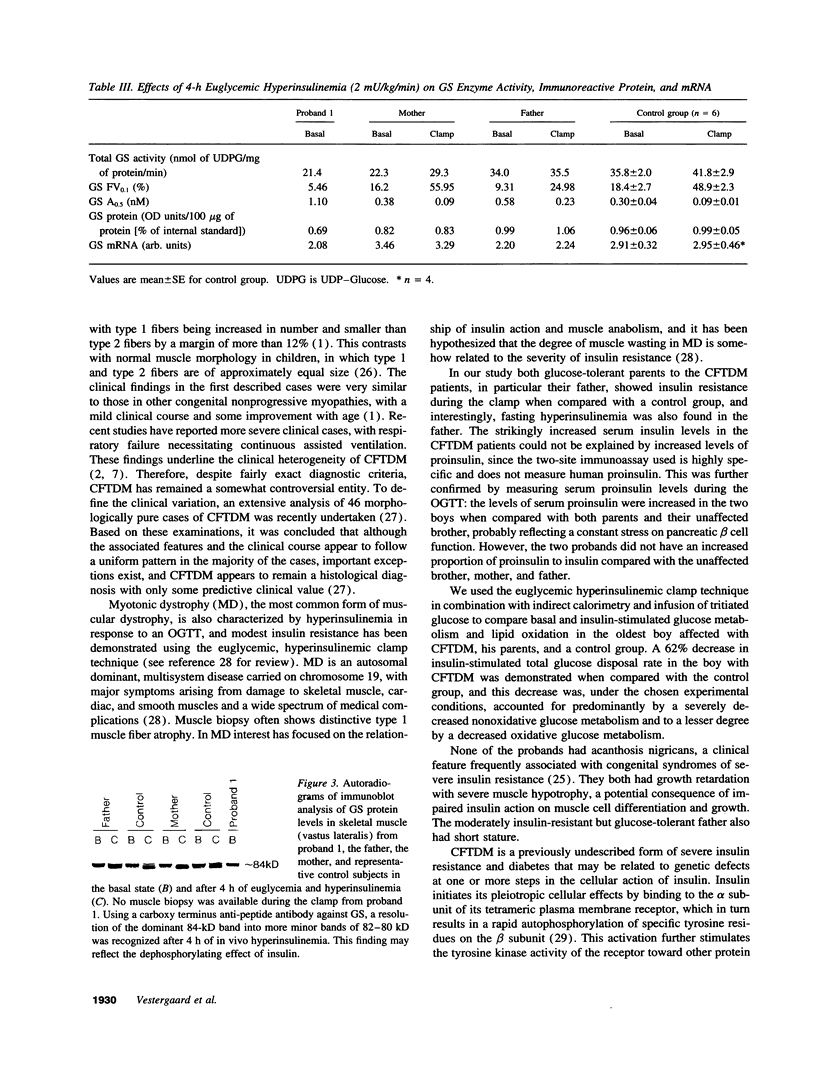
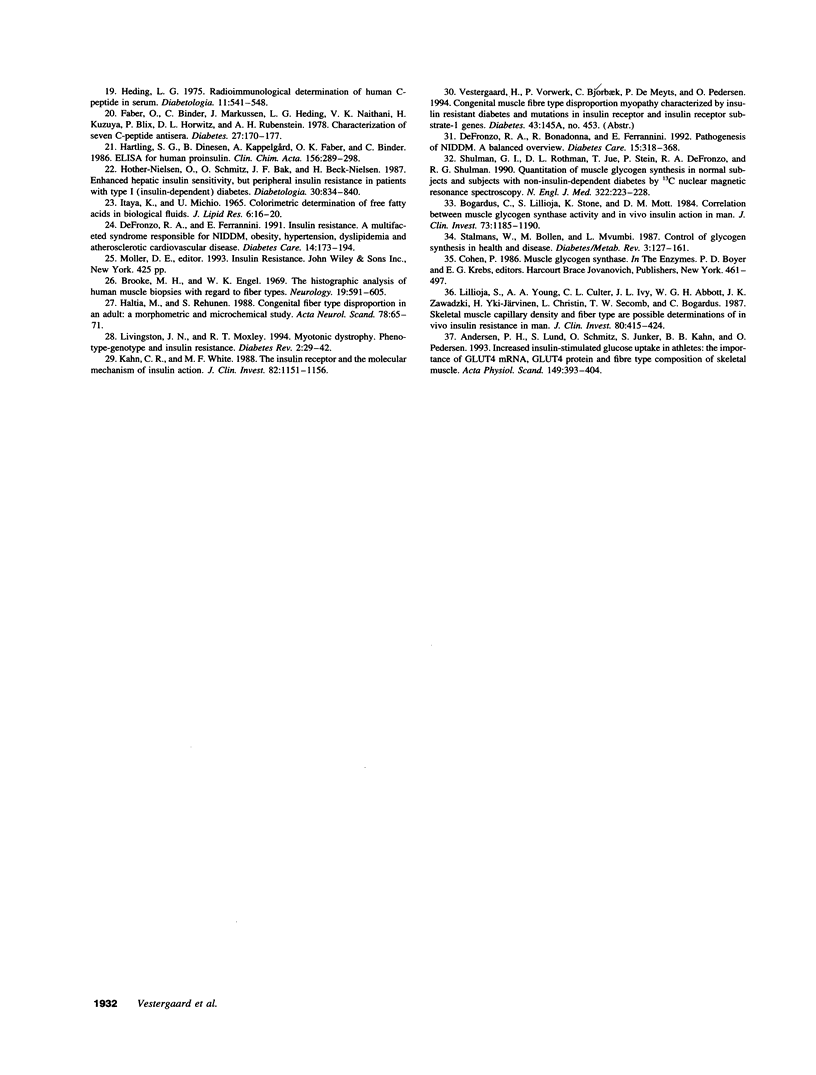
Congenital muscle fiber type disproportion myopathy (CFTDM) is a chronic, nonprogressive muscle disorder characterized by universal muscle hypotrophy and growth retardation. Histomorphometric examination of muscle shows a preponderance of smaller than normal type 1 fibers and overall fiber size heterogeneity. Concomitant endocrine dysfunctions have not been described. We report the findings of altered insulin secretion and insulin action in two brothers affected with CFTDM and glucose intolerance as well as in their nonconsanguineous glucose-tolerant parents. Results are compared with those of six normoglycemic control subjects. All study participants underwent an oral glucose tolerance test to estimate insulin secretion. The oldest boy and his parents volunteered for studies of whole-body insulin sensitivity consisting of a 4-h euglycemic hyperinsulinemic clamp in combination with indirect calorimetry. Insulin receptor function and glycogen synthase (GS) activity and expression were examined in biopsies of vastus lateralis muscle. Despite a 45-90-fold increase in both fasting and postprandial serum insulin levels, both CFTDM patients had diabetes mellitus. Clamp studies revealed that the oldest boy had severe insulin resistance of both liver and peripheral tissues. The impaired insulin-stimulated glucose disposal to peripheral tissues was primarily due to reduced nonoxidative glucose metabolism. These changes were paralleled by reduced basal values of muscle GS total activity, allosterical activation of GS by glucose-6-phosphate, GS protein, and GS mRNA. The father expressed a lesser degree of insulin resistance, and studies of muscle insulin receptor function showed a severe impairment of receptor kinase activity. In conclusion, CFTDM is a novel form of severe hyperinsulinemia and insulin resistance. Whether insulin resistance is causally related to the muscle disorder awaits to be clarified.
Full text
PDF

Images in this article
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Andersen L., Dinesen B., Jørgensen P. N., Poulsen F., Røder M. E. Enzyme immunoassay for intact human insulin in serum or plasma. Clin Chem. 1993 Apr;39(4):578–582. [PubMed] [Google Scholar]
- Andersen P. H., Lund S., Schmitz O., Junker S., Kahn B. B., Pedersen O. Increased insulin-stimulated glucose uptake in athletes: the importance of GLUT4 mRNA, GLUT4 protein and fibre type composition of skeletal muscle. Acta Physiol Scand. 1993 Dec;149(4):393–404. doi: 10.1111/j.1748-1716.1993.tb09635.x. [DOI] [PubMed] [Google Scholar]
- Bak J. F., Pedersen O. Exercise-enhanced activation of glycogen synthase in human skeletal muscle. Am J Physiol. 1990 Jun;258(6 Pt 1):E957–E963. doi: 10.1152/ajpendo.1990.258.6.E957. [DOI] [PubMed] [Google Scholar]
- Bogardus C., Lillioja S., Stone K., Mott D. Correlation between muscle glycogen synthase activity and in vivo insulin action in man. J Clin Invest. 1984 Apr;73(4):1185–1190. doi: 10.1172/JCI111304. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brooke M. H., Engel W. K. The histographic analysis of human muscle biopsies with regard to fiber types. 4. Children's biopsies. Neurology. 1969 Jun;19(6):591–605. doi: 10.1212/wnl.19.6.591. [DOI] [PubMed] [Google Scholar]
- Cavanagh N. P., Lake B. D., McMeniman P. Congenital fibre type disproportion myopathy. A histological diagnosis with an uncertain clinical outlook. Arch Dis Child. 1979 Oct;54(10):735–743. doi: 10.1136/adc.54.10.735. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chang J. F., Jong Y. J., Mak S. C., Chiang C. H. Congenital fiber type disproportion: report of one case. Zhonghua Min Guo Xiao Er Ke Yi Xue Hui Za Zhi. 1990 Nov-Dec;31(6):366–372. [PubMed] [Google Scholar]
- Curless R. G., Nelson M. B. Congenital fiber type disproportion in identical twins. Ann Neurol. 1977 Dec;2(6):455–459. doi: 10.1002/ana.410020603. [DOI] [PubMed] [Google Scholar]
- DeFronzo R. A., Bonadonna R. C., Ferrannini E. Pathogenesis of NIDDM. A balanced overview. Diabetes Care. 1992 Mar;15(3):318–368. doi: 10.2337/diacare.15.3.318. [DOI] [PubMed] [Google Scholar]
- DeFronzo R. A., Ferrannini E. Insulin resistance. A multifaceted syndrome responsible for NIDDM, obesity, hypertension, dyslipidemia, and atherosclerotic cardiovascular disease. Diabetes Care. 1991 Mar;14(3):173–194. doi: 10.2337/diacare.14.3.173. [DOI] [PubMed] [Google Scholar]
- DeFronzo R. A., Tobin J. D., Andres R. Glucose clamp technique: a method for quantifying insulin secretion and resistance. Am J Physiol. 1979 Sep;237(3):E214–E223. doi: 10.1152/ajpendo.1979.237.3.E214. [DOI] [PubMed] [Google Scholar]
- Faber O. K., Binder C., Markussen J., Heding L. G., Naithani V. K., Kuzuya H., Blix P., Horwitz D. L., Rubenstein A. H. Characterization of seven C-peptide antisera. Diabetes. 1978;27 (Suppl 1):170–177. doi: 10.2337/diab.27.1.s170. [DOI] [PubMed] [Google Scholar]
- Frayn K. N. Calculation of substrate oxidation rates in vivo from gaseous exchange. J Appl Physiol Respir Environ Exerc Physiol. 1983 Aug;55(2):628–634. doi: 10.1152/jappl.1983.55.2.628. [DOI] [PubMed] [Google Scholar]
- Haltia M., Somer H., Rehunen S. Congenital fiber type disproportion in an adult: a morphometric and microchemical study. Acta Neurol Scand. 1988 Jul;78(1):65–71. doi: 10.1111/j.1600-0404.1988.tb03621.x. [DOI] [PubMed] [Google Scholar]
- Hartling S. G., Dinesen B., Kappelgård A. M., Faber O. K., Binder C. ELISA for human proinsulin. Clin Chim Acta. 1986 May 15;156(3):289–297. doi: 10.1016/0009-8981(86)90072-0. [DOI] [PubMed] [Google Scholar]
- Heding L. G. Radioimmunological determination of human C-peptide in serum. Diabetologia. 1975 Dec;11(6):541–548. doi: 10.1007/BF01222104. [DOI] [PubMed] [Google Scholar]
- Hother-Nielsen O., Schmitz O., Bak J., Beck-Nielsen H. Enhanced hepatic insulin sensitivity, but peripheral insulin resistance in patients with type 1 (insulin-dependent) diabetes. Diabetologia. 1987 Nov;30(11):834–840. doi: 10.1007/BF00274790. [DOI] [PubMed] [Google Scholar]
- ITAYA K., UI M. COLORIMETRIC DETERMINATION OF FREE FATTY ACIDS IN BIOLOGICAL FLUIDS. J Lipid Res. 1965 Jan;6:16–20. [PubMed] [Google Scholar]
- Kahn C. R., White M. F. The insulin receptor and the molecular mechanism of insulin action. J Clin Invest. 1988 Oct;82(4):1151–1156. doi: 10.1172/JCI113711. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Klein H. H., Kowalewski B., Drenckhan M., Neugebauer S., Matthaei S., Kotzke G. A microtiter well assay system to measure insulin activation of insulin receptor kinase in intact human mononuclear cells. Decreased insulin effect in cells from patients with NIDDM. Diabetes. 1993 Jun;42(6):883–890. doi: 10.2337/diab.42.6.883. [DOI] [PubMed] [Google Scholar]
- Lillioja S., Young A. A., Culter C. L., Ivy J. L., Abbott W. G., Zawadzki J. K., Yki-Järvinen H., Christin L., Secomb T. W., Bogardus C. Skeletal muscle capillary density and fiber type are possible determinants of in vivo insulin resistance in man. J Clin Invest. 1987 Aug;80(2):415–424. doi: 10.1172/JCI113088. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marolda M. Congenital fiber type disproportion in two sisters. A clinical and histopathological study. Acta Neurol (Napoli) 1992 Aug-Dec;14(4-6):398–407. [PubMed] [Google Scholar]
- STEELE R. Influences of glucose loading and of injected insulin on hepatic glucose output. Ann N Y Acad Sci. 1959 Sep 25;82:420–430. doi: 10.1111/j.1749-6632.1959.tb44923.x. [DOI] [PubMed] [Google Scholar]
- Santoro L., Del Giudice E., Francica D., Romano A., Vita G., Barbieri F. Congenital fiber type disproportion myopathy. Report of a case with late onset and myalgia. Clin Pediatr (Phila) 1985 Apr;24(4):219–220. doi: 10.1177/000992288502400410. [DOI] [PubMed] [Google Scholar]
- Shulman G. I., Rothman D. L., Jue T., Stein P., DeFronzo R. A., Shulman R. G. Quantitation of muscle glycogen synthesis in normal subjects and subjects with non-insulin-dependent diabetes by 13C nuclear magnetic resonance spectroscopy. N Engl J Med. 1990 Jan 25;322(4):223–228. doi: 10.1056/NEJM199001253220403. [DOI] [PubMed] [Google Scholar]
- Stalmans W., Bollen M., Mvumbi L. Control of glycogen synthesis in health and disease. Diabetes Metab Rev. 1987 Jan;3(1):127–161. doi: 10.1002/dmr.5610030107. [DOI] [PubMed] [Google Scholar]
- Sulaiman A. R., Swick H. M., Kinder D. S. Congenital fibre type disproportion with unusual clinico-pathologic manifestations. J Neurol Neurosurg Psychiatry. 1983 Feb;46(2):175–182. doi: 10.1136/jnnp.46.2.175. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vestergaard H., Lund S., Larsen F. S., Bjerrum O. J., Pedersen O. Glycogen synthase and phosphofructokinase protein and mRNA levels in skeletal muscle from insulin-resistant patients with non-insulin-dependent diabetes mellitus. J Clin Invest. 1993 Jun;91(6):2342–2350. doi: 10.1172/JCI116466. [DOI] [PMC free article] [PubMed] [Google Scholar]
- ter Laak H. J., Jaspar H. H., Gabreëls F. J., Breuer T. J., Sengers R. C., Joosten E. M., Stadhouders A. M., Gabreëls-Festen A. A. Congenital fibre type disproportion. Clin Neurol Neurosurg. 1981;83(2):67–79. doi: 10.1016/0303-8467(81)90004-4. [DOI] [PubMed] [Google Scholar]