

Abstract
Heavy snowfall, cold temperatures, and low atmospheric pressure during the winter months have been associated with increased adverse cardiovascular events. However, only a few cases of the “snow -shoveler’s infarction ” have been reported. We present our experience with 6 patients presenting with ST elevation myocardial infarction all within a 24-hour period during an unprecedented snowfall (4 of whom were shoveling snow), and provide a detailed review of previously reported cases of snow-shoveler’s infarction. Consistent with other reports, the majority of our patients had the traditional cardiac risk factors of hypertension, hyperlipidemia, diabetes mellitus, tobacco use, and were habitually sedentary. Unique to our case series, however, was that the four patients who had a history of coronary artery disease and prior coronary artery stenting, all presented with subacute stent thrombosis documented on the coronary angiography performed emergently. Moreover, these patients constituted 25% of all the subacute stent thromboses diagnosed in our cardiac catheterization laboratory over the preceding 12 months. In conclusion, our findings suggest that in typically sedentary individuals with cardiac risk factors or a history of coronary artery disease, snow shoveling may trigger ST elevation myocardial infarction and, therefore, should be avoided. This may be most critical in patients with a history of coronary stent placement since our findings suggest that snow shoveling may precipitate subacute stent thrombosis.
Keywords: Snow-shoveling, STEMI, Snow-shoveler’s infarction
Introduction
Adverse cardiac events, including acute myocardial infarction and sudden cardiac death, may be triggered during and after major snowstorms by colder temperatures and the physical exertion expended with snow shoveling 1–8. We present a case series of 6 patients who presented with an acute ST elevation myocardial infarction (STEMI) all within a 24-hour period during an unprecedented snowfall: 4 patients experienced symptoms while shoveling snow. Patients with a history of coronary artery disease and previous coronary stent placement, all presented with subacute stent thrombosis; a unique presentation which has not been previously described in other cases of “snow - shoveler’s infarction” 9–12.
Patients
In one 24-hour period, from Saturday, December 19, 2009 to Sunday, December 20, 2009, 6 patients were taken emergently to the cardiac catheterization laboratory at the University of Virginia, Charlottesville, Virginia with the diagnosis of STEMI; 4 underwent primary percutaneous coronary intervention (PCI), and 2 underwent rescue PCI following failed thrombolysis. Medical history, medications on admission, laboratory values, 12-lead electrocardiographic results, treatment delay, angiographic findings, procedural details, and in-hospital outcomes for all patients were recorded.
Methods
We searched the literature for reported cases of “snow -shoveler’s infarction ”. We review ed the MEDLINE database (Nation al Library of Medicine, Bethesda, MD) from 1970 to 2010. The following key words were used in the search: ST elevation myocardial infarction, acute coronary syndrome, infarction, snow, snow shoveling, snow blowing, snow removal. We reviewed only articles written in English. We also gathered meteorological data from the McCormick Observatory located on the campus of the University of Virginia, for the time period of December 18, 2009 to December 20, 2009 (data from previous months was reviewed for comparison). Lastly, we searched our cardiac catheterization laboratory database to determine: (1) the daily number of patients with STEMI referred for primary PCI, and (2) the daily number of STEMIs that were a result of subacute stent thrombosis from December 2008 to December 2009.
Results
The baseline characteristics of the patients are listed in Table 1. Of the 6 patients, 4 had a history of previous stent placement (2 with drug-eluting stents, and 2 with bare metal stents) (Table 1); all 4 patients presented with subacute stent thrombosis, and all but one were on chronic dual anti-platelet therapy. Symptom onset to arrival in the emergency department ranged from 40 minutes 6 to 264 minutes. The infarct-related artery was the left anterior descending artery in 3 patients and the right coronary artery in 3 patients; all patients underwent intervention of the infarct related artery, and one patient required an intra-aortic balloon pump. New congestive heart failure was diagnosed in 3 patients, and 1 patient died of cardiogenic shock.
Table 1.
Characteristics of 6 patients presenting with ST segment elevation myocardial infarction during a snow storm
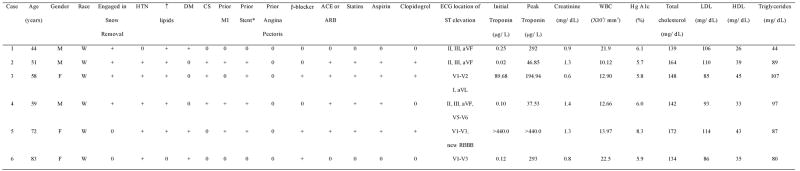 |
ACE = angiotensin converting enzyme inhibitor; ARB = angiotensin receptor blocker; CS = cigarette smoker; DM = diabetes mellitus; HDL = high -density lipoprotein; Hg = hemoglobin; HTN = hypertension; LDL = low-density lipoprotein; MI = myocardial infarction; RBBB = right bundle branch block; WBC = white blood cell count.
Case #2 had a bare metal stent placed in the right coronary artery in 2007; Case #3 had a drug-eluting stent placed in the left anterior descending coronary artery in 2006; Case #4 had a bare metal stent placed in the right coronary artery in 2000; Case #5 had a d rug-eluting stent placed in the left anterior descending coronary artery 9 days prior.
Data obtained from the University of Virginia cardiac catheterization laboratory database revealed a doubling of STEMI cases within a single 24-hour period compared to any other 24-hour period over the past year (Figure 1). Moreover, there was a sharp increase in the incidence of subacute stent thrombosis on December 20, 2009 (diagnosed in 4 of the 6 patients), compared t o daily rates seen over the past year. The spike in the STEMI rate correlated with greater snowfall (Figure 1), as well as colder temperatures, lower atmospheric pressure, and higher wind gusts (Figure 2). A total of 20.5 inches of snow was recorded, the largest single-storm snowfall total for the month of December in the Charlottesville, Virginia area since December 1969 when 16 inches was recorded.
Figure 1.
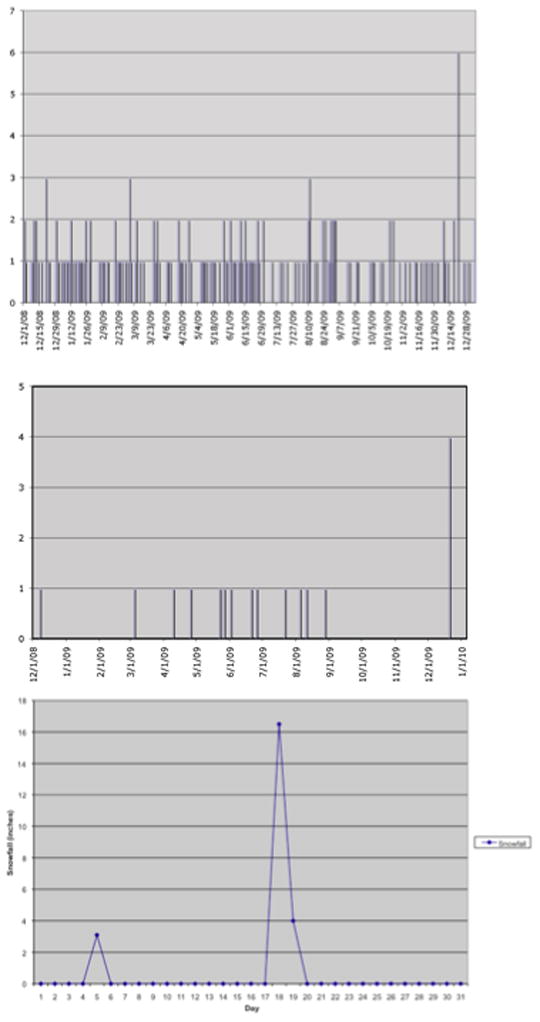
Daily number of patients with ST elevation myocardial infarction undergoing primary percutaneous coronary intervention at the University of Virginia from December 1, 2008 to December 31, 2009 (top panel), and daily number of patients with subacute stent thrombosis presenting with ST elevation myocardial infarction over the same time period (middle panel). The abrupt spike in the number of STEMI patients correlated with the large snowfall (inches) from December 18, 2009 to December 20, 2009, as recorded by the McCormick Observatory on the campus of the University of Virginia, Charlottesville, Virginia.
Figure 2.
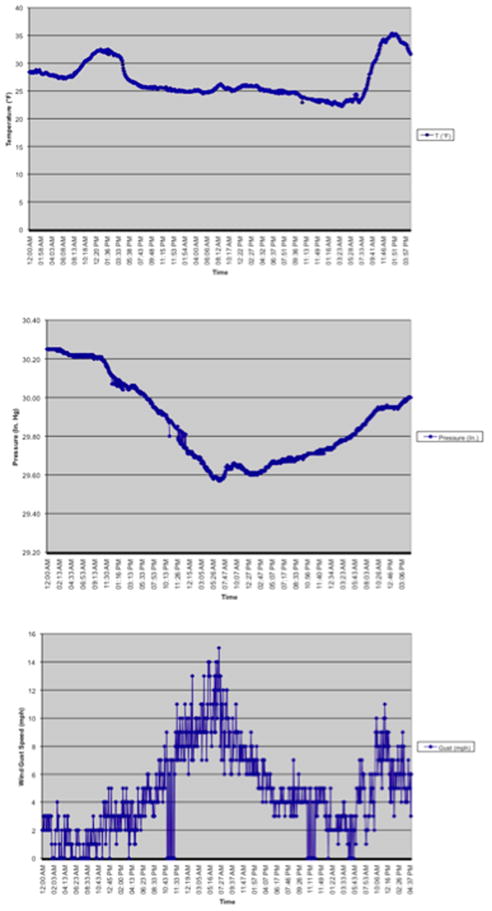
Hourly meteorological data as recorded by the McCormick Observatory on the campus of the University of Virginia, Charlottesville, Virginia. Temperature (top panel) in degrees Fahrenheit (°F) from 12 am December 18, 2009 to 3:57 pm, December 20, 2009; atmospheric pressure (middle panel) in inches of mercury (in Hg) from 12 am December 18, 2009 to 3:06 pm, December 20, 2009; wind gusts (bottom panel) in miles per hour (mph) from 12 am December 18, 2009 to 4:37 pm, December 20, 2009.
Our review of published reports resulted in a total of 4 case series that fulfilled our search restrictions 9–12. These articles were reviewed by 2 of the authors (RJ and ECK). Pertinent information including year and location of the snowstorm, maximum snowfall recorded (inches), number of patients, cardiac history and whether symptoms were preceded by snow shoveling were collected for these studies and summary data, including our series, is shown in Table 2.
Table 2.
Summary of case series of patients presenting with myocardial infarction during or after a heavy snowfall
| Case series | Total Number of Patients | Number of Patients Shoveling Snow | Year of Snow storm | Location | Snow fall (inches) | Cardiac Risk factors | History of Myocardial Infarction | Prior Angina Pectoris |
|---|---|---|---|---|---|---|---|---|
| Franklin et al 9 | 20* | 5 | 1999 | Detroit, Michigan | 11 | + | 1 | 1 |
| Glass et al 10 | 60† | NA | 1979 | Chicago, Illinois | 20 | + | 16 | 6 |
| Hammoudeh et al 11 | 9 | 9 | 1996 | Edison, New Jersey | 32 | + | NA§ | NA§ |
| Heppel et al 12 | 5 | 4 | 1990 | Sheffield, England | 14 | + | 0 | 0 |
| Janardhanan et al | 6 | 4 | 2009 | Charlottesville, Virginia | 20.5 | + | 4 | 0 |
5 patients developed symptoms while shoveling snow, 2 were diagnosed with ST elevation, and 3 with non-ST elevation myocardial infarction
not specified how many patients presented with ST elevation versus non -ST elevation myocardial infarction
3 patients were reported to have known coronary artery disease but this was not further defined
NA = data not available
Discussion
The phenomenon of increased rates of adverse cardiac events occurring during the cold winter months was originally described more than 60 years ago 13; patients with pre-existing coronary artery disease are especially vulnerable 14. Temperature changes and seasonal variations have been associated with an increase in the incidence of myocardial infarction and sudden cardiac death 2,6,7,15, and have also been associated with infarct size 16. Numerous studies have suggested that strenuous exertion (such as snow shoveling) in the days following heavy snowfalls is associated with increased cardiac events 1,2,8,10,17–21. In fact, strenuous exercise of other types has been associated with plaque rupture and subsequent thrombosis 22,23.
Snow shoveling results in significant increases in heart rate, systolic blood pressure, and rate–pressure product 5, and is often undertaken in the early morning hours when circadian changes may play a role 24. Moreover, strenuous exercise and colder temperatures have been associated with changes in blood rheology including increased platelet activation, increased fibrinogen, and increased blood viscosity 25,26, and a hazardous effect on blood pressure 27. It is possible that a combination of these factors may trigger an acute cardiac event, particularly in those with underlying coronary artery disease who are habitually sedentary 28–30. Thus, patients with known coronary artery disease (particularly those with a history of coronary stenting) and sedentary persons with cardiac 8 risk factors, should be cautioned regarding the increased myocardial demands of snow shoveling.
Our study has limitations. First, because of the inherent nature of a case series, ours was descriptive and limited by lack of a control group. Second, complete demographic data was not available for many of the patients previously reported in the literature. Third, we do not have blood test results for levels of fibrinogen, platelet activation, or blood viscosity since these are not routinely measured as part of standard of care.
Acknowledgments
Funding: This work was supported by the National Institutes of Health [HL097074 to E.C.K.]
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- 1.Auliciems A, Frost D. Temperature and cardiovascular deaths in Montreal. Int J Biometeorol. 1989;33:151–156. doi: 10.1007/BF01084599. [DOI] [PubMed] [Google Scholar]
- 2.Baker-Blocker A. Winter weather and cardiovascular mortality in Minneapolis - St. Paul. Am J Public Health. 1982;72:261–265. doi: 10.2105/ajph.72.3.261. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Franklin BA, Bonzheim K, Gordon S, Timmis GC. Snow shoveling: a trigger for acute myocardial infarction and sudden coronary death. Am J Cardiol. 1996;77:855–858. doi: 10.1016/S0002-9149(97)89181-3. [DOI] [PubMed] [Google Scholar]
- 4.Persinger MA, Ballance SE, Moland M. Snow fall and heart attacks. J Psychol. 1993;127:243–252. doi: 10.1080/00223980.1993.9915559. [DOI] [PubMed] [Google Scholar]
- 5.Franklin BA, Hogan P, Bonzheim K, Bakalyar D, Terrien E, Gordon S, Timmis GC. Cardiac demands of heavy snow shoveling. JAMA. 1995;273:880–882. [PubMed] [Google Scholar]
- 6.Gerber Y, Jacobsen SJ, Killian JM, Weston SA, Roger VL. Seasonality and daily weather conditions in relation to myocardial infarction and sudden cardiac death in Olmsted County, Minnesota, 1979 to 2002. J Am Coll Cardiol. 2006;48:287–292. doi: 10.1016/j.jacc.2006.02.065. [DOI] [PubMed] [Google Scholar]
- 7.Thakur CP, Anand MP, Shahi MP. Cold weather and myocardial infarction. Int J Cardiol. 1987;16:19–25. doi: 10.1016/0167-5273(87)90266-x. [DOI] [PubMed] [Google Scholar]
- 8.Chowdhury PS, Franklin BA, Boura JA, Dragovic LJ, Kanluen S, Spitz W, Hodak J, O’Neill WW. Sudden cardiac death after manual or automated snow removal. Am J Cardiol. 2003;92:833–835. doi: 10.1016/s0002-9149(03)00894-4. [DOI] [PubMed] [Google Scholar]
- 9.Franklin BA, George P, Henry R, Gordon S, Timmis GC, O’Neill WW. Acute myocardial infarction after manual or automated snow removal. Am J Cardiol. 2001;87:1282–1283. doi: 10.1016/s0002-9149(01)01520-x. [DOI] [PubMed] [Google Scholar]
- 10.Glass RI, Wiesenthal AM, Zack MM, Preston M. Risk factors for myocardial infarction associated with the Chicago snowstorm of jan 13- 15, 1979. JAMA. 1981;245:164–165. [PubMed] [Google Scholar]
- 11.Hammoudeh AJ, Haft JI. Coronary-plaque rupture in acute coronary syndromes triggered by snow shoveling. N Engl J Med. 1996;335:2001. doi: 10.1056/NEJM199612263352617. [DOI] [PubMed] [Google Scholar]
- 12.Heppell R, Hawley SK, Channer KS. Snow shoveller’s infarction. BMJ. 1991;302:469–470. doi: 10.1136/bmj.302.6774.469-c. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Masters AM. Factors and events associated with onset of coronary artery thrombosis. JAMA. 1937;109:546–549. [Google Scholar]
- 14.van Rossum CT, Shipley MJ, Hemingway H, Grobbee DE, Mackenbach JP, Marmot MG. Seasonal variation in cause-specific mortality: are there high-risk groups? 25-year follow-up of civil servants from the first Whitehall study. Int J Epidemiol. 2001;30:1109–1116. doi: 10.1093/ije/30.5.1109. [DOI] [PubMed] [Google Scholar]
- 15.Ebi KL, Exuzides KA, Lau E, Kelsh M, Barnston A. Weather changes associated with hospitalizations for cardiovascular diseases and stroke in California, 1983–1998. Int J Biometeorol. 2004;49:48–58. doi: 10.1007/s00484-004-0207-5. [DOI] [PubMed] [Google Scholar]
- 16.Kloner RA, Das S, Poole WK, Perrit R, Muller J, Cannon CP, Braunwald E. Seasonal variation of myocardial infarct size. Am J Cardiol. 2001;88:1021–1024. doi: 10.1016/s0002-9149(01)01981-6. [DOI] [PubMed] [Google Scholar]
- 17.Anderson TW, Rochard C. Cold snaps, snowfall and sudden death from ischemic heart disease. Can Med Assoc J. 1979;121:1580–1583. [PMC free article] [PubMed] [Google Scholar]
- 18.Rogot E, Padgett SJ. Associations of coronary and stroke mortality with temperature and snowfall in selected areas of the United States, 1962–1966. Am J Epidemiol. 1976;103:565–575. doi: 10.1093/oxfordjournals.aje.a112261. [DOI] [PubMed] [Google Scholar]
- 19.Faich G, Rose R. Blizzard morbidity and mortality: Rhode Island, 1978. Am J Public Health. 1979;69:1050–1052. doi: 10.2105/ajph.69.10.1050. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Blindauer KM, Rubin C, Morse DL, McGeehin M. The 1996 New York blizzard: impact on noninjury emergency visits. Am J Emerg Med. 1999;17:23–27. doi: 10.1016/s0735-6757(99)90008-6. [DOI] [PubMed] [Google Scholar]
- 21.Spitalnic SJ, Jagminas L, Cox J. An association between snowfall and ED presentation of cardiac arrest. Am J Emerg Med. 1996;14:572–573. doi: 10.1016/S0735-6757(96)90102-3. [DOI] [PubMed] [Google Scholar]
- 22.Ciampricotti R, el Gamal MI, Bonnier JJ, Relik TH. Myocardial infarction and sudden death after sport: acute coronary angiographic findings. Cathet Cardiovasc Diagn. 1989;17:193–197. doi: 10.1002/ccd.1810170402. [DOI] [PubMed] [Google Scholar]
- 23.Black A, Black MM, Gensini G. Exertion and acute coronary artery injury. Angiology. 1975;26:759–783. doi: 10.1177/000331977502601101. [DOI] [PubMed] [Google Scholar]
- 24.Muller JE. Morning increase of onset of myocardial infarction. Implications concerning triggering events. Cardiology. 1989;76:96–104. doi: 10.1159/000174480. [DOI] [PubMed] [Google Scholar]
- 25.Kestin AS, Ellis PA, Barnard MR, Errichetti A, Rosner BA, Michelson AD. Effect of strenuous exercise on platelet activation state and reactivity. Circulation. 1993;88:1502–1511. doi: 10.1161/01.cir.88.4.1502. [DOI] [PubMed] [Google Scholar]
- 26.Woodhouse PR, Khaw KT, Plummer M, Foley A, Meade TW. Seasonal variations of plasma fibrinogen and factor VII activity in the elderly: winter infections and death from cardiovascular d isease. Lancet. 1994;343:435–439. doi: 10.1016/s0140-6736(94)92689-1. [DOI] [PubMed] [Google Scholar]
- 27.Jehn M, Appel LJ, Sacks FM, Miller ER., 3rd The effect of ambient temperature and barometric pressure on ambulatory blood pressure variability. Am J Hypertens. 2002;15:941–945. doi: 10.1016/s0895-7061(02)02999-0. [DOI] [PubMed] [Google Scholar]
- 28.Marchant B, Donaldson G, Mridha K, Scarborough M, Timmis AD. Mechanisms of cold intolerance in patients with angina. J Am Coll Cardiol. 1994;23:630–636. doi: 10.1016/0735-1097(94)90747-1. [DOI] [PubMed] [Google Scholar]
- 29.Mittleman MA, Maclure M, Tofler GH, Sherwood JB, Gold berg RJ, Muller JE. Triggering of acute myocardial infarction by heavy physical exertion. Protection against triggering by regular exertion. Determinants of Myocardial Infarction Onset Study Investigators. N Engl J Med. 1993;329:1677–1683. doi: 10.1056/NEJM199312023292301. [DOI] [PubMed] [Google Scholar]
- 30.Willich SN, Maclure M, Mittleman M, Arntz HR, Muller JE. Sudden cardiac death. Support for a role of triggering in causation. Circulation. 1993;87:1442–1450. doi: 10.1161/01.cir.87.5.1442. [DOI] [PubMed] [Google Scholar]