

Abstract
Study Design:
Serial dissection of porcine motion segments during robotic control of vertebral kinematics.
Objectives:
To identify which spinal tissues are loaded in response to manual therapy (manipulation and mobilization) and to what magnitude.
Summary of Background Data:
Various theoretical constructs attempt to explain how manual therapies load specific spinal tissues. By using a parallel robot to control vertebral kinematics during serial dissection, it is possible to quantify the loads experienced by discrete spinal tissues undergoing common therapeutic procedures such as manual therapy.
Methods
In nine porcine cadavers, manual therapy was provided to L3 and the kinematic response of L3-4 recorded. The exact kinematic trajectory experienced by L3-4 in response to manual therapy was then replayed to the isolated segment by a parallel robot equipped with a 6 axis load cell. Discrete spinal tissues were then removed and the kinematic pathway replayed. The change in forces and moments following tissue removal were considered to be those applied to that specific tissue by manual therapy.
Results:
In this study, both manual therapies affected spinal tissues. The intervertebral disc experienced the greatest forces and moments arising from both manipulation and mobilization.
Conclusions:
This study is the first to identify which tissues are loaded in response to manual therapy. The observation that manual therapy loads some tissues to a much greater magnitude than others offers a possible explanation for its modest treatment effect; only conditions involving these tissues may be influenced by manual therapy. Future studies are planned to determine if manual therapy can be altered to target (or avoid) specific spinal tissues.
Keywords: Robotics, serial dissection, motion segment, spine, manual therapy
INTRODUCTION
The spine is designed to provide stability during the static and dynamic loads arising from human activity. Because the majority of back pain is considered to be mechanical in nature,1 understanding how loads are carried in spinal tissues is expected provide insight not only into the causes of back pain, but how various mechanically-based interventions may, or may not, exert their therapeutic effects.
Unfortunately, practical limitations frustrate the in vivo measurement of spinal forces and moments.2,3 As a result, in vitro methods of serial dissection have been used toward understanding how specific tissues are loaded during spinal motion. Typically, serial dissection is carried out with one end of a spinal specimen fixed to a stationary load cell while the other end is mobile. The mobile end is moved, an anatomic structure removed, and the difference in loading noted. While this technique provides important information about joint laxity,4-8 the ability to quantify the exact force contribution of a specific spinal tissue is confounded as with each dissection, the constraints on the specimen are altered.
A solution to this problem has been found by employing highly-stable robots capable of repeatedly applying the same three dimensional motion to the mobile end of a specimen no matter what tissues have been removed. As a result, the change in force recorded by the load cell before and after tissue removal is the net force experienced by that tissue.
This technique, based on the principle of superposition, was employed for studying the musculoskeletal system by Fujie et al.9 who removed tissues of interest from an isolated knee joint then replayed the original kinematic path while the force components were re-measured. Since then, others have used this approach to map forces experienced by tissues of the knee10-14, glenohumeral joint15 and human forearm.16
In the spine, robotics have also been used to apply pure translations and rotations to assess internal tissue loads.17-21 While these studies have increased our knowledge of spinal mechanics, the applied motions were not physiologic but artificial constructs meant to isolate motion on, or about, specific orthogonal axes.
To date, the full potential of robotics to reproduce physiologic motions and then quantify the resulting tissue loads has yet to be exploited in spinal research. These motions include passive movements of the spine that occur as the result of mechanically-based treatments. By using robotics, it may be possible to understand if therapeutic interventions apply load to some tissues more than others and in the future, to design new mechanical interventions to isolate (or avoid) specific spinal structures.
Manual therapy, a treatment used frequently for back pain, is a perfect candidate to investigate tissue loads resulting from a therapeutic intervention. Made up of a collection of therapies such as manipulation and mobilization, manual therapies involve a clinician using their hands to apply an external force to a patient with the intent of loading internal tissues of the spine.22 Unfortunately, it is not known presently if these therapies load specific spinal tissues preferentially and to what magnitude.
By using serial dissection of porcine motion segments while employing robotic control of vertebral kinematics, our objective was to identify the spinal tissues loaded in response to manual therapy (manipulation and mobilization).
METHODS
Specimen preparation
Nine porcine cadavers (Duroc × (Large White × Landrace breeds)) of approximately 60 kg were used in this study. In each intact porcine cadaver, the third and fourth lumbar vertebrae (L3, L4) were identified by midline dissection and a pilot hole drilled in each spinous process. Each hole was then dried and glue inserted before screwing in a 3 mm diameter bone pin (Zimmer Spine, Minneapolis, MN). A rectangular flag having four infrared light emitting diode (irLED) markers was then attached to each pin (Figure 1). To identify the left transverse processes of L3, a long needle was used to probe the paravertebral tissues until contact with the transverse process was made. Following the application of manual therapy on the intact porcine cadaver (see below), the spine was removed en bloc by reciprocating saw, the vertebrae superior to L3 and inferior to L4 removed, and the non-ligamentous tissues cleaned away with a water jet dissector (Smith and Nephew, St. Petersburg, FL).
Figure 1.

This image shows two bone pins inserted into the spinous processes of L3 and L4. Attached to each bone pin is a clear plastic flag with four active markers each of which is tethered to a data collection system. The cephalic end of the cadaver is to the reading left.
Manual therapy and kinematic recording
In each porcine cadaver, manipulation and mobilization were applied to the skin overlying the previously identified left transverse process of L3. Spinal manipulation (SMT) is defined as the application of a controlled dynamic thrust applied with high velocity and low force amplitude while mobilization (MOB) is a low velocity, variable amplitude movement applied over a much greater timeframe.23 All manipulations and mobilizations were applied by a single clinician trained in these skills. During the application of SMT (high speed displacement) and MOB (low speed displacement), the resulting motion of each bone pin flag was recorded in three dimensions by an optical tracking system at a rate of 460 Hz (0.01mm system resolution with 0.15mm rigid body resolution; NDI, Waterloo, Canada).
Robotic testing
Pilot holes were drilled in each exposed end of the isolated L3-4 specimen to accommodate three anchor screws per endplate. The specimen was then potted in a vertical orientation using dental stone (Modern Materials, South Bend, IN) with the caudal end fixed to a 6 axis load cell (AMTI MC3A-100, Advanced Mechanical Technology, Inc, Watertown, MA) that in turn was mounted rigidly (Figure 2) to a parallel robot (Parallel Robotics Systems Corporation, Hampton, NH). The robot itself is comprised of a rigid platform suspended by 6 rigid struts of fixed length (Figure 2). Each strut is attached to an electromechanical motor that travels about a circular track. Changes in the position and orientation of the robot platform are achieved by computer-controlled movement of each motor around the track. Therefore, the resolution of the robot is a function of the motor performance (0.05mm with a repeatability of 0.025mm; Mikrolar, Hampton, NH) which translates into a linear resolution of slightly less than 1μm and an angular resolution of approximately 0.001°.
Figure 2.

The left image displays the parallel robot with a potted motion segment attached to the robot's active surface. The motion segment has yet to have its most cranial end (i.e. vertical in this orientation) attached to the rigid cross beam that has been moved into the foreground. The image on the right is a close up view of the potted segment. The caudal end of the specimen is connected to a 6 axis load cell that is then connected rigidly to the robot below. The cranial end of the segment is now attached rigidly to the cross beam located above the sample.
The spinal segment is then potted and the caudal end mounted rigidly to the load cell/robot. A computer is then used to position the robot until the optical markers of the caudal vertebra are in the same position and orientation as was recorded previously from the in vitro neutral pose. From this position, a series of known translations and rotations of the robot platform are performed and then compared to the resulting change in the marker position. With this approach, known mathematical processes24,25 can be used to transpose marker movements caused by SMT and MOB into the robotic frame of reference. The result is two separate robotic trajectory files for SMT and MOB each of which consists of a series of commands that move the robot in displacement control through a sequence of positions and orientations. Once this calibration process is complete, there is no need for the markers to remain in the specimen although they can be retained for quality control tests. Prior experiments have been performed to compare the resulting motion of these markers to the desired robotic trajectory as well as to the actual positions of the strut motors. Results from these experiments (unpublished) indicate that the accuracy in obtaining the requested position is dependent on the time available to reach that position (i.e. relatively fast moves can create position lag). From these experiments, the error caused by position lag was estimated to be less than 5%.
When the calibration procedure is complete, the cranial end of the potted specimen is then fixed to a rigid, stationary cross beam and the segment posed again in its in vivo neutral position.
The robot is then moved through a series of events by a custom computer interface (National Instruments, Austin, TX): initial neutral pose, manipulation trajectory, initial neutral pose, mobilization trajectory. A one minute gap between each event is provided. The gap duration was determined by feasibility tests where the specimen was placed in the neutral pose and the load cell zeroed. The robotic trajectory was then performed and the specimen returned to the neutral pose. The residual loads on the specimen were then recorded and the time noted for these loads to return to the baseline condition. On average, the return to baseline was complete in 30s, therefore, a gap time of 60 seconds was employed. These tests also demonstrated that peak loads in the specimen change with repeated applications of the robotic trajectory, but this phenomenon reaches equilibrium within 2-3 trials – trials that are performed in advance of the testing.
After application of the initial pose, the load cell was zeroed and the loads and moments generated during robotic simulation of SMT and MOB were recorded at 50Hz (x = medial/lateral, y = anterior/posterior and z = superior/inferior). Because the robot accepts commands less frequently than data points generated by the optical system, the robotic command file is normalized to the optical system. After these events were applied by the robot, a single spinal structure was removed and/or transected and the kinematic events re-applied by the robot. In all nine specimens, spinal structures were removed/transected in the following order: interspinous ligament (via scapel), left intertransverse ligament (via scalpel), right intertransverse ligament(via scalpel), left facet capsule (via scalpel), right facet capsule (via scalpel), left fact joint (via rongeur), right fact joint (via rongeur) and intervertebral disc (via scalpel).
Analysis
For each of the nine specimens, the resulting loads and moments were plotted for the intact condition and following the destruction of each anatomical structure (Figure 3). Using customized software (National Instruments, Austin, TX), the baseline load along the x, y, and z axes, as well as the baseline moments about the x, y and z axes, were considered to be those that occurred after the specimen was posed in the neutral position and the load cell zeroed (Figure 3). The peak load or peak moment in or around each axis was determined by software to occur at the point in time where the robotic trajectory reached its greatest translation or rotation (Figure 3). The custom software then determined the change between the peak and baseline forces and moments.
Figure 3.

Typical moment data collected from the load cell during the repeated application of manipulation by parallel robot. Each plot represents moments about the x-axis (shown as unconverted voltages) over time (shown at 0.02 s intervals) following the removal of 8 different spinal tissues. The plot with the highest peak is the intact condition while the plot with the lowest moments was recorded following transection of the intervertebral disc. Vertical cursors describe the common points in time where baseline (left cursor) and peak moment values (right cursor) were obtained.
After each tissue removal, the resulting series of values representing the change in peak force were considered to be a repeated measure. Therefore, a repeated measures analysis of variance (ANOVA) was performed with two addition factors: axis (x, y or z) and treatment type (manipulation or mobilization) (SPSS v17, Chicago, Il). Results for the change in moments following tissue destruction were analyzed in the same manner (two factor repeated measure). The repeated ANOVA procedure also produced observed power for between-subject and within-subject factors along with their test of significance. These powers correspond to the observed effect sizes.
To assess differences from one tissue removal to the next, within-subject contrasts were performed to compare the 1st tissue removal (interspinous ligament) to the 2nd (left intertransverse ligament), the 2nd to the 3rd (left intertransverse ligament) and so on until the 7th tissue removal (right facet joint) was compared to the 8th (intervertebral disc).
RESULTS
Power analysis
A post-hoc power analysis (Table 1) demonstrated that for a sample size of n = 9, the within-subject (repeated) variables of force and moment had an observed power was 0.99 as a result of the large effect size observed. The observed power values for the between-subject variables (main effects) were less (range = 0.23 – 0.27) with the exception of the axis variable when considering moment data (0.99).
Table 1.
Post-hoc power calculations for between-subject and within-subject factors along with their test of significance. These powers correspond to the observed effect sizes.
| Variable | Factor | Observed Power |
|---|---|---|
| Force | Between subject - Manual Therapy (2 levels: SMT, MOB) | 0.27 |
| Between subject - Axis (3 levels: x, y, z) | 0.26 | |
| Within subject (repeated) - Force | 0.99 | |
|
| ||
| Moments | Between subject - Manual Therapy (2 levels: SMT, MOB) | 0.23 |
| Between subject - Axis (3 levels: x, y, z) | 0.99 | |
| Within subject (repeated) - Moment | 0.99 | |
Translations and Forces
Relative translations between vertebrae (as measured by the optical tracking system and recreated by the robot) are displayed in Table 2 by specimen and axis. Peak robotic translations for all specimens were greater than the resolution of the optical tracking system and the robot itself indicating that the peak translations and rotations created for SMT and MOB were above and beyond the system's total error. When compiled as absolute values, the greatest change in the average relative translation (experienced by the segment and simulated by the robot) occurred in the y axis (posterior to anterior translation) in both manipulation and mobilization (Table 2).
Table 2.
Maximal change in displacement (mm) and rotation (degree) created in each cadaveric specimen with the application of manipulation (SMT) and mobilization (MOB) trajectories. These are the same maximal displacements and rotations simulated by the robot.
| Displacement in mm | Rotation in degrees | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| X SMT | Y SMT | Z SMT | X MOB | Y MOB | Z MOB | X SMT | Y SMT | Z SMT | X MOB | Y MOB | Z MOB | |
| Specimen 1 | 2.43 | 1.42 | −0.28 | 1.76 | 3.60 | −0.32 | 0.44 | −0.52 | −0.03 | 1.24 | −0.42 | 0.66 |
| Specimen 2 | 1.30 | 5.27 | 0.47 | 1.24 | 5.40 | 0.46 | 2.05 | −0.21 | −0.26 | 1.88 | −0.41 | 0.09 |
| Specimen 3 | −0.59 | 4.52 | 0.47 | 0.23 | 3.75 | 0.40 | 1.54 | 0.30 | 0.60 | 1.26 | 0.22 | 0.33 |
| Specimen 4 | 2.89 | 10.53 | 0.74 | 2.34 | 10.61 | 0.83 | 3.77 | −1.10 | −0.15 | 3.61 | −0.93 | −0.12 |
| Specimen 5 | −1.00 | 3.86 | 0.60 | −1.09 | 3.80 | 0.48 | 1.83 | −0.08 | −1.28 | 1.22 | 0.17 | −1.15 |
| Specimen 6 | 5.10 | 7.98 | 0.88 | 5.27 | 7.41 | 1.12 | 2.59 | −1.53 | −0.26 | 2.64 | −1.66 | −0.12 |
| Specimen 7 | −1.05 | 5.37 | 0.23 | −0.94 | 6.89 | 0.34 | 1.78 | 0.20 | −0.18 | 2.43 | 0.11 | 0.09 |
| Specimen 8 | 3.06 | 4.25 | 0.39 | 2.63 | 5.97 | 0.63 | 1.91 | −1.05 | 1.12 | 2.14 | −0.78 | 0.13 |
| Specimen 9 | 1.91 | 4.94 | 0.46 | 1.22 | 4.88 | 0.39 | 1.76 | −0.54 | −0.15 | 1.74 | −0.37 | −0.04 |
|
|
||||||||||||
| Displacement in absolute mm | Rotation in absolute degrees | |||||||||||
|
|
||||||||||||
| Average | 2.15(0.47) | 5.35(0.86) | 0.5(0.07) | 1.86(0.49) | 5.81(0.75) | 0.55(0.09) | 1.96(0.29) | 0.61(0.17) | 0.45(0.15) | 2.02(0.26) | 0.56(0.16) | 0.3(0.12) |
For the forces resulting from manual therapy, Table 3, as well as Figures 4 and 5, show the change in peak force for all specimens after each spinal tissue was removed. The repeated measure, 2 factor ANOVA, demonstrated a significant main effect for the between-subject axis factor and none for the between-subject treatment factor. There was no interaction between axis and treatment factors.
Table 3.
Mean ±SE change in peak force and peak moments (for all specimens) caused by removal of a specific tissue during application of manipulation (SMT) and mobilization (MOB) trajectories. SL = spinous ligament. LTVP = left intertransverse ligament. RTVP = right intertransverse ligament. LCAP = left facet joint capsule. RCAP = right facet joint capsule. LFAC = left facet joint. RFAC = right facet joint. Disc = intervertebral disc.
| Change in Peak Force (N) | Change in Peak Moment (Nm) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| X SMT | Y SMT | Z SMT | X MOB | Y MOB | Z MOB | X SMT | Y SMT | Z SMT | X MOB | Y MOB | Z MOB | |
| SL | 1.02(0.2) | 0.56(0.26) | 7.36(2.78) | 0.61(0.17) | 0.95(0.31) | 4.47(1.61) | 3.37(0.75) | 3.84(1.4) | 3.36(1.56) | 1.11(0.22) | 2.35(0.66) | 2.79(1.23) |
| LTVP | 0.44(0.14) | 0.53(0.14) | 6.91(3.88) | 0.43(0.06) | 0.47(0.24) | 3.04(1.11) | 1.03(0.28) | 1.24(0.54) | 1.92(0.53) | 0.83(0.34) | 1.31(0.36) | 1.01(0.3) |
| RTVP | 0.64(0.18) | 0.57(0.16) | 6.35(4.47) | 0.33(0.11) | 0.44(0.27) | 2.32(1.53) | 0.61(0.18) | 1.6(0.55) | 1.88(0.62) | 0.78(0.46) | 1.12(0.3) | 1.69(0.94) |
| LCAP | 0.53(0.13) | 0.55(0.21) | 6.23(4.78) | 0.35(0.1) | 0.3(0.08) | 3.52(1.48) | 2.74(0.77) | 1.93(0.73) | 1.37(0.36) | 2.11(0.69) | 2.76(0.77) | 2.58(1.06) |
| RCAP | 0.46(0.15) | 0.46(0.25) | 7.15(5.16) | 0.29(0.09) | 0.37(0.12) | 2.64(1.72) | 1.25(0.24) | 2.13(0.51) | 1.2(0.33) | 1.87(0.76) | 2.45(0.73) | 2.01(0.55) |
| LFAC | 0.52(0.12) | 0.77(0.17) | 1.65(0.62) | 0.94(0.42) | 0.66(0.21) | 1.7(0.54) | 1.57(0.39) | 3.44(1.25) | 3.94(1.32) | 1.58(0.44) | 3.73(1.39) | 6.53(2.27) |
| RFAC | 0.43(0.12) | 0.5(0.14) | 1.72(0.66) | 0.88(0.35) | 0.47(0.14) | 1.92(0.68) | 1.77(0.59) | 2.19(0.7) | 4.58(1.04) | 1.03(0.46) | 2.02(0.5) | 4.24(1.2) |
| DISC | 4.93(2.13) | 2.75(0.84) | 13.27(4.48) | 2.4(0.74) | 1.86(0.46) | 10.26(2.63) | 26.47(4.44) | 23.45(8.19) | 12.99(4.27) | 21.94(4.31) | 16.14(3.69) | 12.35(4.7) |
|
|
||||||||||||
| Average | 1.12(0.4) | 0.84(0.27) | 6.33(3.35) | 0.4(0.26) | 0.27(0.23) | 3.35(1.41) | 4.85(0.96) | 4.98(1.73) | 3.91(1.25) | 0.96(0.96) | 1.73(1.05) | 1.25(1.53) |
Figure 4.

The average change in peak forces for all cadavers (N ± StErr) following removal of specific tissues. Data are shown separately for manipulation (SMT) and mobilization (MOB) and are stratified by axis. SL = spinous ligament. LTVP = left intertransverse ligament. RTVP = right intertransverse ligament. LCAP = left facet joint capsule. RCAP = right facet joint capsule. LFAC = left facet joint. RFAC = right facet joint. Disc = intervertebral disc.
Figure 5.
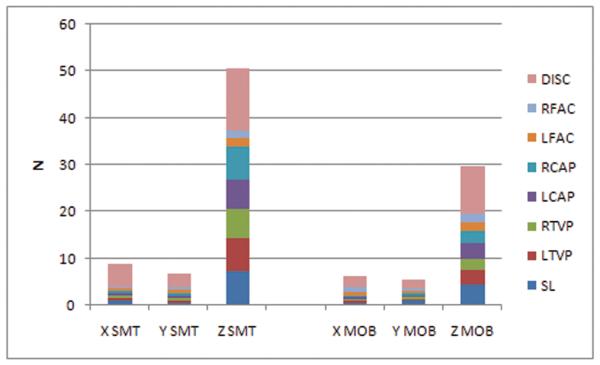
A bar chart showing data from Figure 4 in a different manner. The accumulative increase in the average change in peak force (N) for all cadavers is shown following the removal of specific tissues. Data are shown separately for manipulation and mobilization and are stratified by axis. SL = spinous ligament. LTVP = left intertransverse ligament. RTVP = right intertransverse ligament. LCAP = left facet joint capsule. RCAP = right facet joint capsule. LFAC = left facet joint. RFAC = right facet joint. Disc = intervertebral disc.
For the within-subject (repeated) factor of force, we observed a significant change over the course of serial tissue removal (p < 0.00). A further analysis of within-subject contrasts demonstrated that force does not change significantly until the intervertebral disc is transected (Table 4). In addition, a significant interaction was observed (p < 0.00) between the change in peak force and the axis of translation.
Table 4.
With-in subject contrasts for repeated measures of change in peak force and change in peak moment. SL = spinous ligament. LTVP = left intertransverse ligament. RTVP = right intertransverse ligament. LCAP = left facet joint capsule. RCAP = right facet joint capsule. LFAC = left facet joint. RFAC = right facet joint. Disc = intervertebral disc.
| Within-subject contrast | Change in peak force p value |
Change in peak moment p value |
|---|---|---|
| SP vs. LTVP | 0.544 | 0.000 |
| LTVP vs. RTVP | 0.581 | 0.969 |
| RTVP vs. LCAP | 0.361 | 0.000 |
| LCAP vs. RCAP | 0.924 | 0.127 |
| RCAP vs. LFAC | 0.357 | 0.029 |
| LFAC vs. RFAC | 0.811 | 0.066 |
| RFAC vs. Disc | 0.000 | 0.000 |
Rotations and moments
Relative rotations between vertebrae (as measured by the optical tracking system and recreated by the robot) are displayed in Table 2. When compiled as absolute values, the greatest change in rotation occurred about the x axis (flexion/extension) for both manipulation and mobilization.
For the moments resulting from manual therapy, Table 3, as well as Figures 6 and 7, show the change in peak moment for all specimens after each spinal tissue was removed. The repeated measure, 2 factor ANOVA, demonstrated a significant main effect for the between-subject axis factor and none for the between-subject treatment factor. There was no interaction between axis and treatment factors.
Figure 6.

A bar chart showing the average of change in peak moments for all cadavers (Nm ± StErr) following removal of specific tissues. Data are shown separately for manipulation (SMT) and mobilization (MOB) and are stratified by axis. SL = spinous ligament. LTVP = left intertransverse ligament. RTVP = right intertransverse ligament. LCAP = left facet joint capsule. RCAP = right facet joint capsule. LFAC = left facet joint. RFAC = right facet joint. Disc = intervertebral disc.
Figure 7.
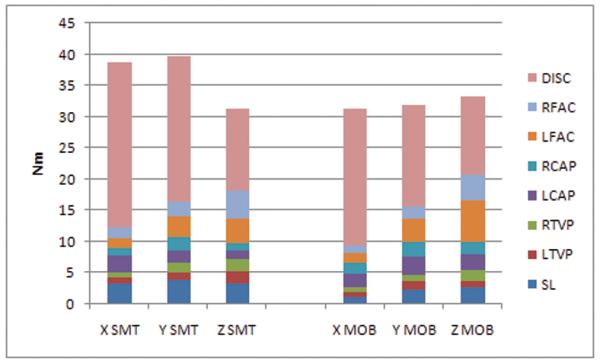
A bar chart showing data from Figure 6 in a different manner. The accumulative increase in the average change in peak moments (Nm) for all cadavers is shown following the removal of specific tissues. Data are shown separately for manipulation and mobilization and are stratified by axis. SL = spinous ligament. LTVP = left intertransverse ligament. RTVP = right intertransverse ligament. LCAP = left facet joint capsule. RCAP = right facet joint capsule. LFAC = left facet joint. RFAC = right facet joint. Disc = intervertebral disc.
For the within-subject (repeated) factor of moment, we observed a significant change with successive tissue destruction (p < 0.00). Within-subject contrasts demonstrated that some tissue removal, but not all tissue removal, resulted in a significant change in peak moment (Table 4). Significant changes in peak moment occurred following removal of the left intertransverse ligament, the left facet capsule, the left facet joint and the intervertebral disc. By comparison of absolute values of the peak moments between each tissue removal, the largest change in segmental moments was experienced after transection of the intervertebral disc. As with force data, there was a significant interaction between the repeated factor (change in peak moment) and the axis of rotation.
DISCUSSION
In this study, a parallel robot was employed to quantify forces and moments arising in spinal tissues as a result of the application of manipulation and mobilization. It was observed that the intervertebral disc was the tissue affected to the greatest extent by both manual therapies. Although various clinical professions have proposed theoretical constructs to explain which spinal tissues may be targeted by various mechanical interventions,26,27 this is the first evidence that a specific tissue can be loaded to a significantly greater extent through the application of manual therapy.
Manual therapy in this study was applied solely to the left transverse process of L3. As might be expected, the resulting displacement of the L3-4 segment from manipulation and mobilization was largest from posterior to anterior as the vertebrae were pushed away from the point of applied force. Similarly, the greatest rotation of the segment in response to both manipulation and mobilization was about the x axis after the contacted vertebra was pushed further anterior than the adjacent, non-contacted vertebra.
Although the greatest displacement of the segment from manual therapy occurred in the y axis, the y axis did not experience the greatest change in force as a result of serial dissection. Similarly, the greatest rotations applied to the segment were about the x axis, however, the change in moment following serial dissection was similar between axes. Presently, we can provide no definitive explanation for why the axes experiencing the greatest displacement or rotation do not result in the greatest force or moments associated with that axis. We speculate that the reason for this observation may be that 1) displacements and rotations applied superficially by manual therapy may not transfer directly into forces and moments along the same axes28,29 and 2) some displacement and rotation may occur through zones of joint laxity where forces and moments may not increase linearly.30
While many consider the therapeutic goals of SMT and MOB to be different, both created substantial forces and moments in the intervertebral disc. While this study was not designed or powered to determine if these two therapies affect the disc similarly, our data suggest that the clinical impact of these therapies may be limited to specific tissues. Interestingly, some smaller tissues other than the disc were also affected by SMT and MOB (left intertransverse ligament, the left facet capsule, the left facet joint), but only with respect to changes in moments. This finding suggests that many more spinal tissues are influenced by the rotational forces created during manual therapy than by translational forces. Presently, it is not known if manual therapies can be altered to preferentially provide linear or rotational forces to underlying spinal tissues.
The observation that the moments created by manual therapy loaded some left sides tissues more than their right sided counterparts suggests the presence of an effect caused by the order in which the tissues were sacrificed. Compared to some serial robots, the increased stiffness available from the parallel robot used in this experiment creates high levels of repeatability in performing a specific kinematic trajectory with a high level of accuracy under changing load conditions. As a result, the robotic trajectories applied to the mobile end of the mounted spinal specimen are unwavering whether the motion segment is completely intact or fully dissociated. This set of conditions allows the principle of superposition10 to be applied which permits the assumption that any change in load following the removal of a spinal tissue is the load carried by the dissected tissue itself. The principle also allows the assumption that the order in which tissues are removed has no effect.20 Therefore, we have assumed that left-sided tissues found to carry greater moments are affected differently due to the unilateral nature of the applied manual therapy. Certainly, this assumption can be problematic if Tissue A shields Tissue B from load. In this case, the order in which Tissue A and B are removed may result in different load values. The possibility of this phenomenon provides further justification for removing tissues from each specimen in the same order as this procedure would standardize shielding affects between all specimens. Future experiments will be conducted to identify the presence of force shielding in spinal tissues impacted by manual therapy. In addition, other factors such as specimen potting and specimen compliance may also affect the forces and moments generated by manual therapy.
These results offer a possible explanation for why manual therapy, like many other back pain therapies, has been reported to have a modest effect;31-33 should interventions such as manual therapy target specific tissues to the exclusion of others, it is unlikely that manual therapy could impact the entire constellation of low back pain conditions and their different etiologies.
Although obvious, it should be emphasized that kinematics other than those applied here do not necessarily affect the disc maximally in spite of its size relative to other spinal ligamentous structures. Gillespie et al.20 demonstrated that when applying pure moments to spinal segments, robotic serial dissection demonstrated that tissues other than the disc experience the majority of load. These results contrast those of this study and emphasize that one cannot assume which spinal tissue may be loaded preferentially with a given kinematic pathway.
It is important to note that although the sample size used in this study could be considered small (n = 9), our post-hoc power analysis (Table 1) described very high observational power scores for our within-subject (repeated) factors due to large effect sizes. As a result, not only can we say that significant differences in forces and moments occurred following removal of certain tissues, but when significant changes did not occur, we are confident in the lack of observed change. Interestingly, our sample size is very similar to prior studies9-11,15-16,18,20-21 using robotic serial dissection (mean n = 10).
Unfortunately, this study did not attempt to alter specific parameters of manual therapy (e.g. application site, application angle) to determine if spinal tissues carrying the largest forces and moments could be changed to other tissues purposefully. Future studies are required to determine if it possible to alter the delivery of manual therapies such that different tissues are loaded preferentially. Even if these therapies cannot be altered to target tissues of choice, the manual therapies tested here still may exert their effect in other ways via tissue systems not represented in this model (e.g. muscular, neurological).
Should future robotic testing determine that the parameters of manual therapy can be altered so that different spinal tissues can be loaded preferentially, it may be possible to create new therapeutic techniques able to target, or conversely avoid, specific spinal tissues. Alternatively, it may not be possible to alter target tissues by changing manual therapy parameters; recent studies suggest that altering the application angle of manipulation acts only to decrease the resulting magnitude of vertebral displacement and not the direction of vertebral displacement.28,29
Key points.
Manual therapy (manipulation and mobilization) was applied to the L3-4 segment of nine pig cadavers and the kinematic response of the vertebrae recorded.
The exact three dimensional kinematics of the L3 and L4 vertebrae resulting from manual therapy were then replayed to the isolated L3-4 segment by a parallel robot.
By using a parallel robot to replay and control vertebral kinematics, any change in the loads and moments experienced by the motion segment after the removal of a specific tissue can be considered to be load and moment experienced by that specific tissue.
In this study, both manual therapies (manipulation and mobilization) affected spinal tissues with the intervertebral disc experiencing the greatest forces and moments.
Precis.
Manual therapy (manipulation and mobilization) was applied to L3-L4 motions segments of porcine cadavers and the resulting kinematics replayed to the isolated segments via parallel robotics. Through serial dissection, it was shown that both manual therapies (manipulation and mobilization) affected spinal tissues with the intervertebral disc experiencing the greatest forces and moments.
ACKNOWLEDGEMENTS
Support for this project was provided by the National Institutes of Health (1R21AT004055-01A2). Support for Greg Kawchuk was provided by the Canada Research Chairs program. The authors would also like to thank Christine Cooke, Stephen Perle and Gina Montgomery for their assistance. This study was approved by the Animal Care and Use Committee of the University of Alberta.
Footnotes
This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- 1.Liang MH. Acute low back pain: diagnosis and management of mechanical back pain. Prim Care. 1988;15:827–847. [PubMed] [Google Scholar]
- 2.Ravary B, Pourcelot P, Bortolussi C, et al. Strain and force transducers used in human and veterinary tendon and ligament biomechanical studies. Clinical biomechanics. 2004;19:433–447. doi: 10.1016/j.clinbiomech.2004.01.008. [DOI] [PubMed] [Google Scholar]
- 3.Fleming BC, Beynnon BD. In vivo measurement of ligament/tendon strains and forces: a review. Ann Biomed Eng. 2004;32:318–328. doi: 10.1023/b:abme.0000017542.75080.86. [DOI] [PubMed] [Google Scholar]
- 4.Heuer F, Schmidt H, Klezl Z, et al. Stepwise reduction of functional spinal structures increase range of motion and change lordosis angle. J Biomech. 2007;40:271–280. doi: 10.1016/j.jbiomech.2006.01.007. [DOI] [PubMed] [Google Scholar]
- 5.Pitzen T, Lane C, Goertzen D, et al. Anterior cervical plate fixation: biomechanical effectiveness as a function of posterior element injury. J Neurosurg. 2003;99:84–90. doi: 10.3171/spi.2003.99.1.0084. [DOI] [PubMed] [Google Scholar]
- 6.Tencer AF, Ahmed AM, Burke DL. Some static mechanical properties of the lumbar intervertebral joint, intact and injured. J Biomech Eng. 1982;104:193–201. doi: 10.1115/1.3138348. [DOI] [PubMed] [Google Scholar]
- 7.Posner I, White AA, Edwards WT, et al. A biomechanical analysis of the clinical stability of the lumbar and lumbosacral spine. Spine. 1982;7:374–389. doi: 10.1097/00007632-198207000-00008. [DOI] [PubMed] [Google Scholar]
- 8.Panjabi MM, White AA, Johnson RM. Cervical spine mechanics as a function of transection of components. J Biomech. 1975;8:327–336. doi: 10.1016/0021-9290(75)90085-8. [DOI] [PubMed] [Google Scholar]
- 9.Fujie H, Livesay GA, Woo SL, et al. The use of a universal force-moment sensor to determine in-situ forces in ligaments: a new methodology. J Biomech Eng. 1995;117:1–7. doi: 10.1115/1.2792266. [DOI] [PubMed] [Google Scholar]
- 10.Li G, Rudy TW, Sakane M, et al. The importance of quadriceps and hamstring muscle loading on knee kinematics and in-situ forces in the ACL. J Biomech. 1999;32:395–400. doi: 10.1016/s0021-9290(98)00181-x. [DOI] [PubMed] [Google Scholar]
- 11.Sakane M, Livesay GA, Fox RJ, et al. Relative contribution of the ACL, MCL, and bony contact to the anterior stability of the knee. Knee Surg Sports Traumatol Arthrosc. 1999;7:93–97. doi: 10.1007/s001670050128. [DOI] [PubMed] [Google Scholar]
- 12.Livesay GA, Fujie H, Kashiwaguchi S, et al. Determination of the in situ forces and force distribution within the human anterior cruciate ligament. Ann Biomed Eng. 1995;23:467–474. doi: 10.1007/BF02584446. [DOI] [PubMed] [Google Scholar]
- 13.Woo SL, Abramowitch SD, Kilger R, et al. Biomechanics of knee ligaments: injury, healing, and repair. J Biomech. 2006;39:1–20. doi: 10.1016/j.jbiomech.2004.10.025. [DOI] [PubMed] [Google Scholar]
- 14.Woo SL, Debski RE, Wong EK, et al. Use of robotic technology for diathrodial joint research. J Sci Med Sport. 1999;2:283–297. doi: 10.1016/s1440-2440(99)80002-4. [DOI] [PubMed] [Google Scholar]
- 15.Debski RE, Wong EK, Woo SL, et al. In situ force distribution in the glenohumeral joint capsule during anterior-posterior loading. J Orthop Res. 1999;17:769–776. doi: 10.1002/jor.1100170523. [DOI] [PubMed] [Google Scholar]
- 16.DeFrate LE, Li G, Zayontz SJ, et al. A minimally invasive method for the determination of force in the interosseous ligament. Clin Biomech. 2001;16:895–900. doi: 10.1016/s0268-0033(01)00092-4. [DOI] [PubMed] [Google Scholar]
- 17.Dickey JP, Gillespie KA. Representation of passive spinal element contributions to in vitro flexion-extension using a polynomial model: illustration using the porcine lumbar spine. J Biomech. 2003;36:883–888. doi: 10.1016/s0021-9290(02)00479-7. [DOI] [PubMed] [Google Scholar]
- 18.Gardner-Morse MG, Stokes IA. Structural behavior of human lumbar spinal motion segments. J Biomech. 2004;37:205–212. doi: 10.1016/j.jbiomech.2003.10.003. [DOI] [PubMed] [Google Scholar]
- 19.Gilbertson LG, Doehring TC, Kang JD. New methods to study lumbar spine biomechanics: Delineation of in vitro load-displacement characteristics by using a robotic/UFS testing system with hybrid control. Operative Techniques in Orthopaedics. 2000;10:246–253. [Google Scholar]
- 20.Gillespie KA, Dickey JP. Biomechanical role of lumbar spine ligaments in flexion and extension: determination using a parallel linkage robot and a porcine model. Spine. 2004;29:1208–1216. doi: 10.1097/00007632-200406010-00010. [DOI] [PubMed] [Google Scholar]
- 21.Thompson RE, Pearcy MJ, Barker TM. The mechanical effects of intervertebral disc lesions. Clinical biomechanics. 2004;19:448–455. doi: 10.1016/j.clinbiomech.2004.01.012. [DOI] [PubMed] [Google Scholar]
- 22.Lederman Eyal. The science and practice of manual therapy. Churchill Livingstone; 2005. [Google Scholar]
- 23.Hurwitz EL, Morgenstern H, Harber P, et al. A randomized trial of chiropractic manipulation and mobilization for patients with neck pain: clinical outcomes from the UCLA neck-pain study. Am J Public Health. 2002;92:1634–1641. doi: 10.2105/ajph.92.10.1634. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Goldsmith P, Wynd S, Kawchuk DG. Robotic Measurement and Control for Chiropractic Research (in press) Applied Bionics and Biomechanics. 2006;2:43–48. [Google Scholar]
- 25.Goldsmith P. Design of a robot for sport shoe testing; Proc.5th Int Conf on Control, Automation, Robotics and Vision; 1998. pp. 105–110. [Google Scholar]
- 26.Haldeman S, editor. Principles and Practices of Chiropractic. McGraw-Hill Medical: 2004. [Google Scholar]
- 27.Boyling J, Palastanga N, Grieve G. Grieve's Modern Manual Therapy: The Vertebral Column. W.B. Saunders Company; 1994. [Google Scholar]
- 28.Bereznick DE, Ross JK, McGill SM. The frictional properties at the thoracic skin-fascia interface: implications in spine manipulation. Clin Biomech. 2002;17:297–303. doi: 10.1016/s0021-9290(02)00014-3. [DOI] [PubMed] [Google Scholar]
- 29.Kawchuk GN, Perle SM. The relation between the application angle of spinal manipulative therapy (SMT) and resultant vertebral accelerations in an in situ porcine model. Man Ther. 2009;14:480–483. doi: 10.1016/j.math.2008.11.001. [DOI] [PubMed] [Google Scholar]
- 30.Panjabi MM. The stabilizing system of the spine. Part II. Neutral zone and instability hypothesis. J Spinal Disord. 1992;5:390–396. doi: 10.1097/00002517-199212000-00002. [DOI] [PubMed] [Google Scholar]
- 31.Assendelft W, Morton S, Yu E, et al. Spinal manipulative therapy for low back pain. Cochrane Database Syst Rev. 2004 doi: 10.1002/14651858.CD000447.pub2. [DOI] [PubMed] [Google Scholar]
- 32.Bronfort G, Haas M, Evans R, et al. Efficacy of spinal manipulation and mobilization for low back pain and neck pain: a systematic review and best evidence synthesis. Spine J. 2004;4:335–356. doi: 10.1016/j.spinee.2003.06.002. [DOI] [PubMed] [Google Scholar]
- 33.van Tulder M, Koes B, Malmivaara A. Outcome of non-invasive treatment modalities on back pain: an evidence-based review. Eur Spine J. 2006;(Suppl 1):S64–S81. doi: 10.1007/s00586-005-1048-6. [DOI] [PMC free article] [PubMed] [Google Scholar]