

Abstract
An increasing number of studies have begun to investigate properties of tissue obtained from patients with osteonecrosis of the jaw (ONJ). Due to the relatively low incidence of ONJ, these studies necessitate the use of specimens from patients who have had ONJ for various durations. The goal of this study was to determine if properties, specifically bone morphology assessed by micro-computed tomography (micro-CT), were influenced by the duration of ONJ. Sequestra from 31 patients with confirmed ONJ for between 3 weeks and 42 months prior to obtaining the tissue were scanned using micro-CT to determine bone volume/tissue volume (BV/TV) and bone surface/volume (BS/TV). There was no significant correlation between the sequestra bone morphology (either BV/TV or BS/TV) and the duration of ONJ. We interpret this as evidence that studies should not be concerned about assessing tissue properties from patients that have had ONJ for different durations. Furthermore, the lack of difference in morphology with continued duration of ONJ suggests that the majority of changes to the bone tissue occur early on in the disease progression.
Keywords: Bisphosphonate, osteonecrosis of the jaw, imaging, sequestrum, morphology
INTRODUCTION
Bisphosphonates (BPs) have significant benefits in the treatment of various metabolic bone diseases and cancers [1, 2]. The side effect of osteonecrosis of the jaw (ONJ), although relatively rare, has received significant attention mostly because of its unknown pathophysiology [3, 4]. Progress toward understanding ONJ has been slow due to numerous difficulties in studying the human condition.
A number of studies have assessed tissue-level changes associated with ONJ in human samples [5–12]. One challenge in the interpretation of these studies is the lack of standardizing key aspects of the patient population from which the tissue is obtained. For example, the samples in these previous reports are from patients that had been treated with BPs, and had exposed bone, for various durations (ranging from a few months to many years). The identification of highly eroded surfaces and osteoclasts in these ONJ specimens could mean that resorption activity drastically changes the specimen characteristics over time. That is, it’s not clear if these highly eroded surfaces are part of the initial pathology that leads to the bone being necrotic or if they are simply a consequence of the piece of bone being dead It would be unrealistic to expect samples to have similar characteristics with respect to duration of bone exposure as the specimens for study are routinely made available when sequestrum is debrided from a patient. As such, future studies are likely to be limited by these same issues. The aim of the current work was to understand if tissue properties are influenced by the duration of ONJ.
One way to assess this question would be to look at the tissue multiple times in the same person using in vivo imaging, yet this technique is currently limited by resolution. We chose an alternative approach - to look at tissue that was removed from patients who had ONJ for various durations of time and determine whether there was any correlation to the bone morphology, assessed by micro-computed tomography. We hypothesized that the duration of ONJ would be negatively correlated to the bone volume (BV/TV) and positively correlated to the ratio of bone surface to bone volume (BS/BV).
MATERIALS AND METHODS
The study of these specimens was approved by the Indiana University Purdue University Indianapolis/Clarian Institutional Review Board (NS0806-04). Sequestra from patients with confirmed ONJ were collected during routine treatment of patients for their condition. A total of 40 bone samples were collected from 31 different patients. Patient age and gender, the specific bisphosphonate, length of bisphosphonate treatment prior to ONJ diagnosis and duration of ONJ prior to sample collection were collected. We did not obtain information about the underlying condition for which the patients were receiving bisphosphonate treatment Samples were fixed in 10% neutral-buffered and then transferred to 70% ethanol.
Samples were obtained from 8 males and 23 females ranging in age from 53 to 85 years old. Patients had been treated with various BPs (Fosamax (n=8), Actonel (n=1), Boniva (n=1), Zometa (n=16), Aredia (n=1), Foxamax/Boniva (n=1) or Aredia/Zometa (n=3)).) The duration of the BP treatment prior to ONJ diagnosis ranged from 3 months to 120 months. The duration of ONJ prior to specimen collection ranged from 3 weeks to 48 months.
A single piece of bone was removed from twenty-seven of the patients. One individual had six different pieces removed, one patient had three pieces removed, and one patient had two pieces removed. For these cases with multiple pieces of bone, the parameters were assessed by combining the raw data (tissue volume, bone volume, bone surface) and then calculating the derived parameters. One individual had a single piece of bone removed at two different times – these two samples were treated as individual data points.
Micro-Computed Tomography
Specimens were scanned using a micro-computed tomography machine (MicroCT, SkyScan 1172; SkyScan, Kontich, Belgium) as previously described [8]. Briefly, samples were wrapped in Parafilm (Brand, Germany) and affixed to the scanning stage. Projection images were attained at 12 µm resolution and then reconstructed using manufacturer-provided software (NRecon; SkyScan). Reconstructed images were analyzed by using manufacturer-supplied software (CTAn; SkyScan). A region of interest was manually traced around the individual 2D images throughout the entire specimen (Figure 1), a threshold applied to separate bone from soft tissue (100–255 range), and then the specimen was analyzed in 3D. Outcome parameters included tissue volume (TV, the size of the sequestrum including bone plus soft tissue), bone volume (BV, the amount of bone within the tissue) and bone surface (BS). These primary parameters were used to calculate bone volume per unit tissue volume (BV/TV, %) and bone surface per unit bone volume (BS/BV, 1/mm). Similar to our previous work, the mean tissue density was also assessed in all samples [8].
Figure 1.
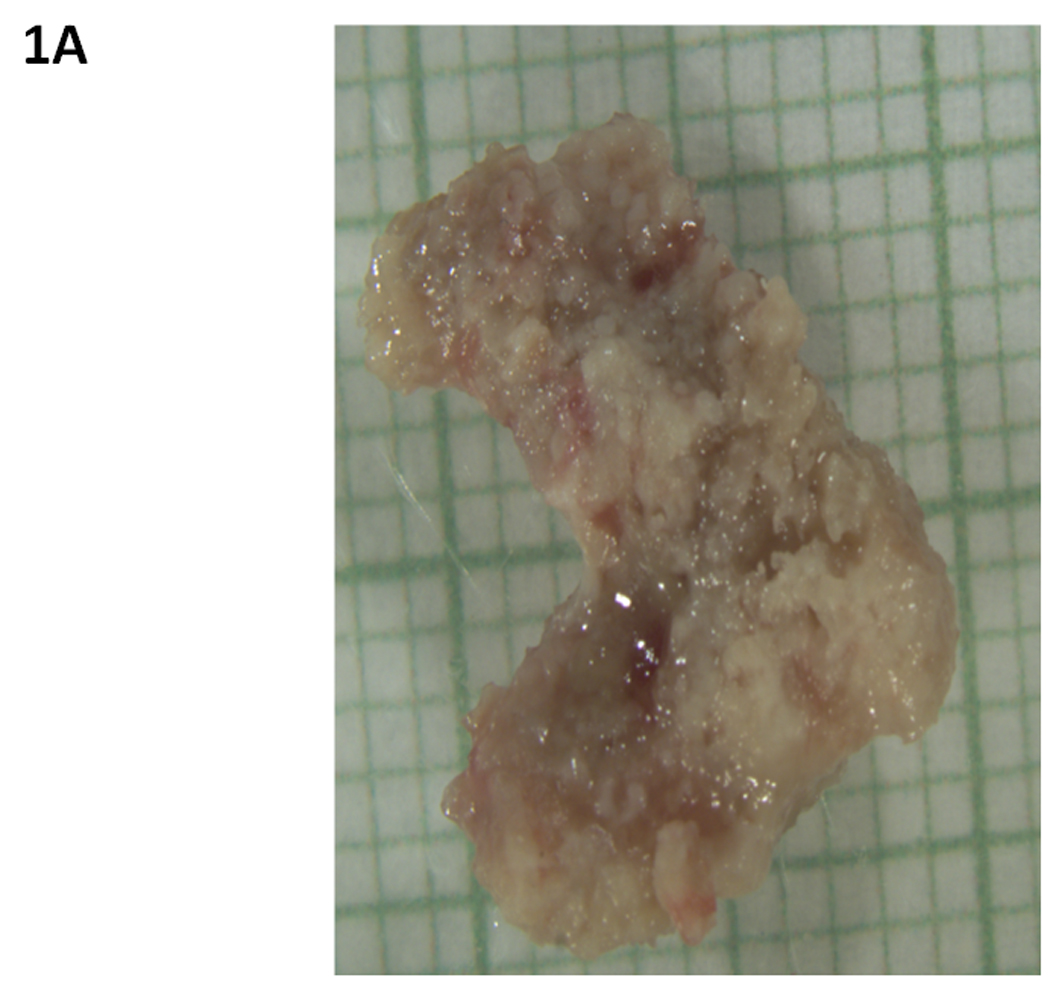
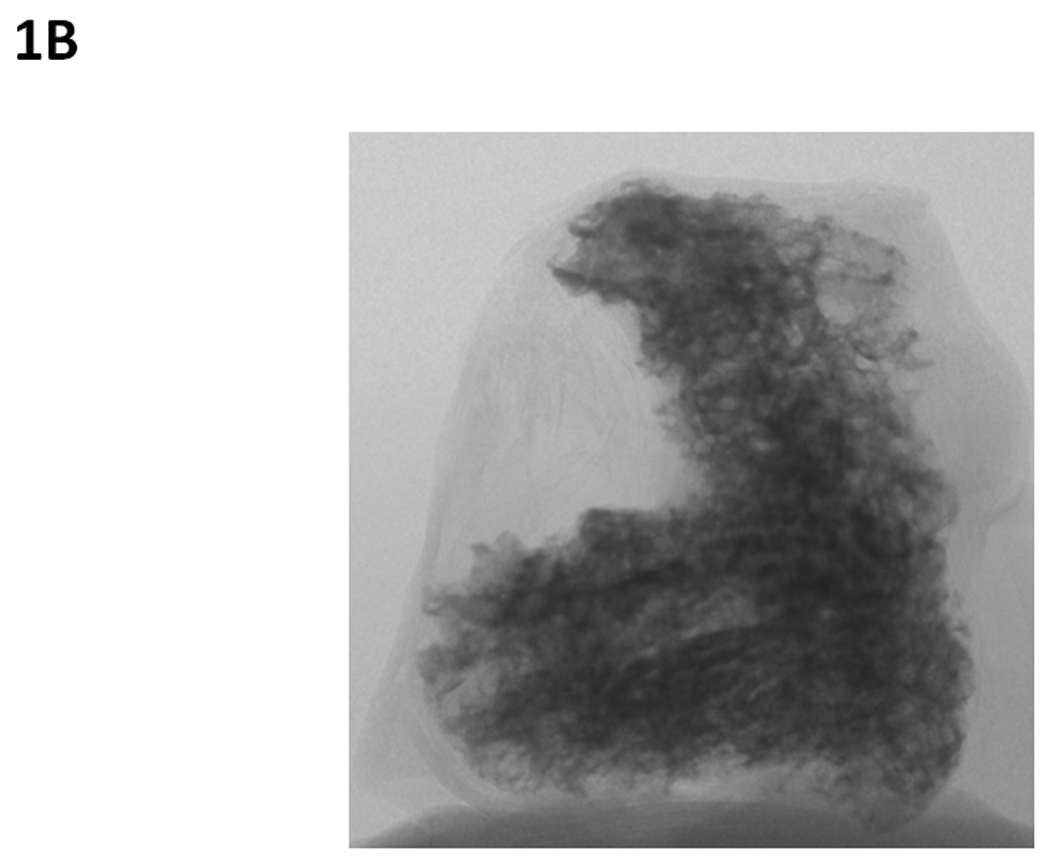
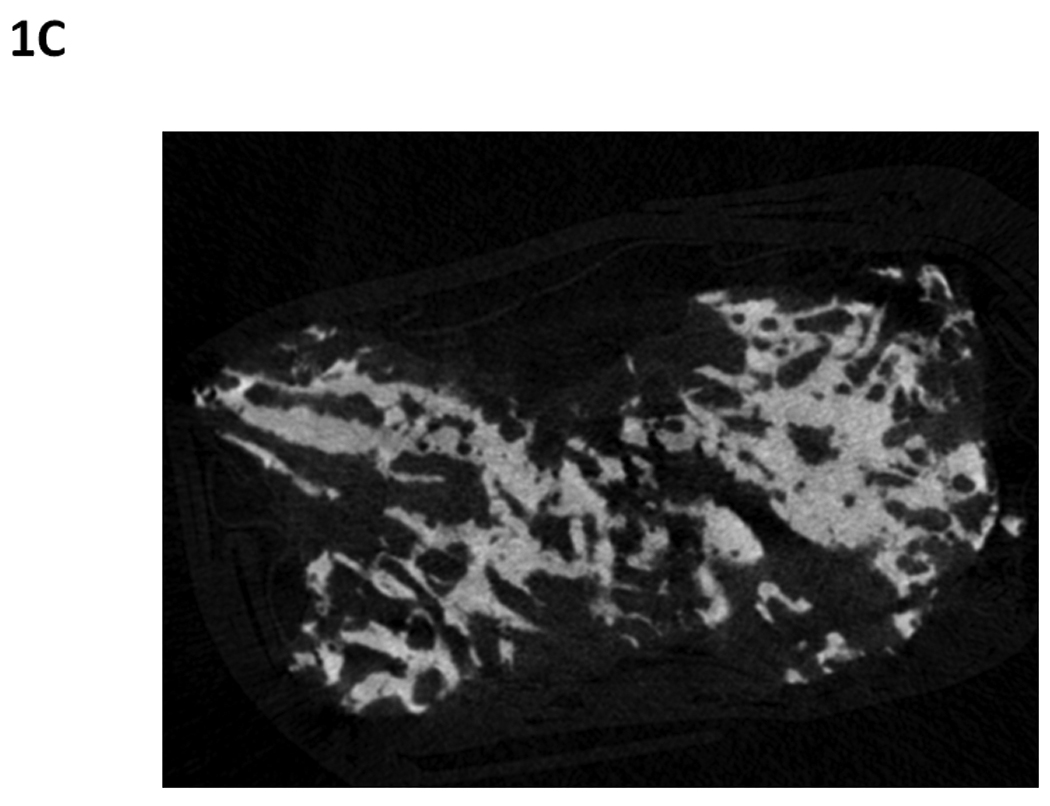
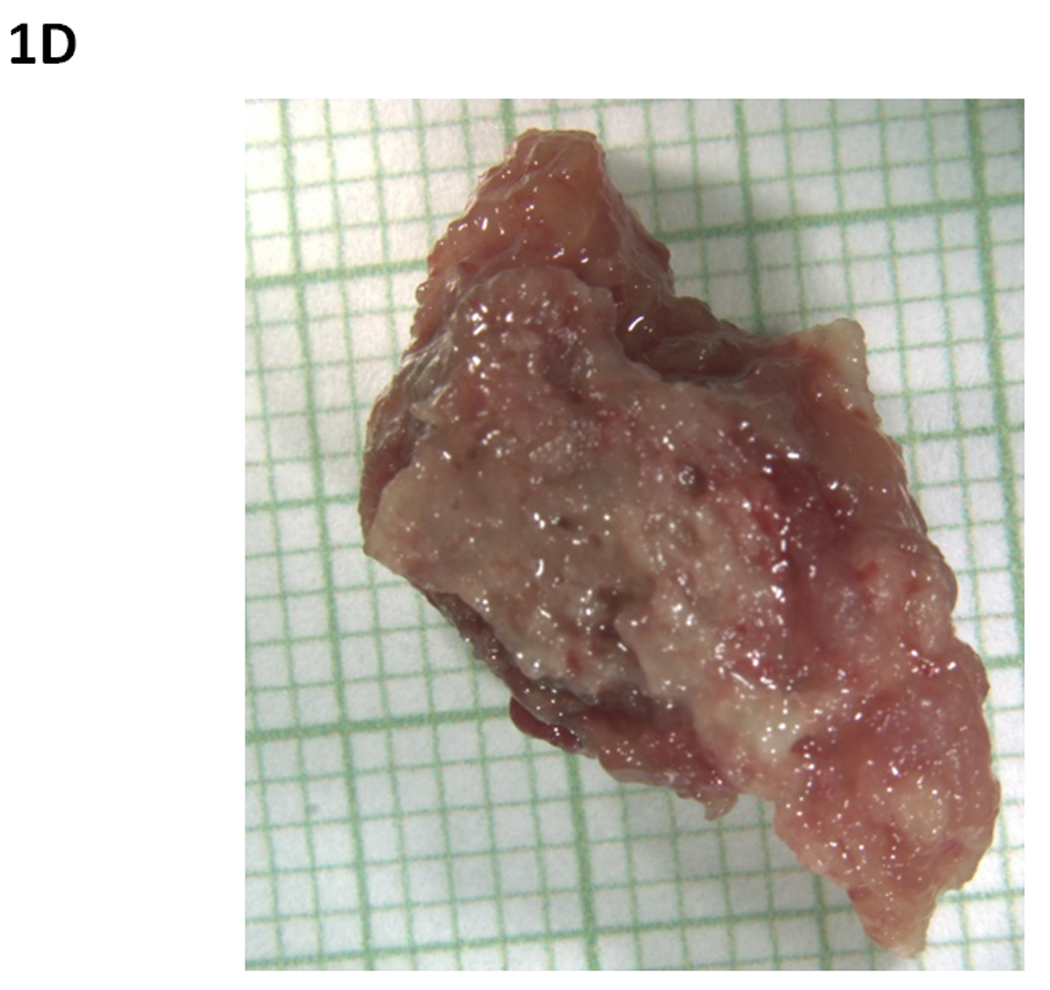
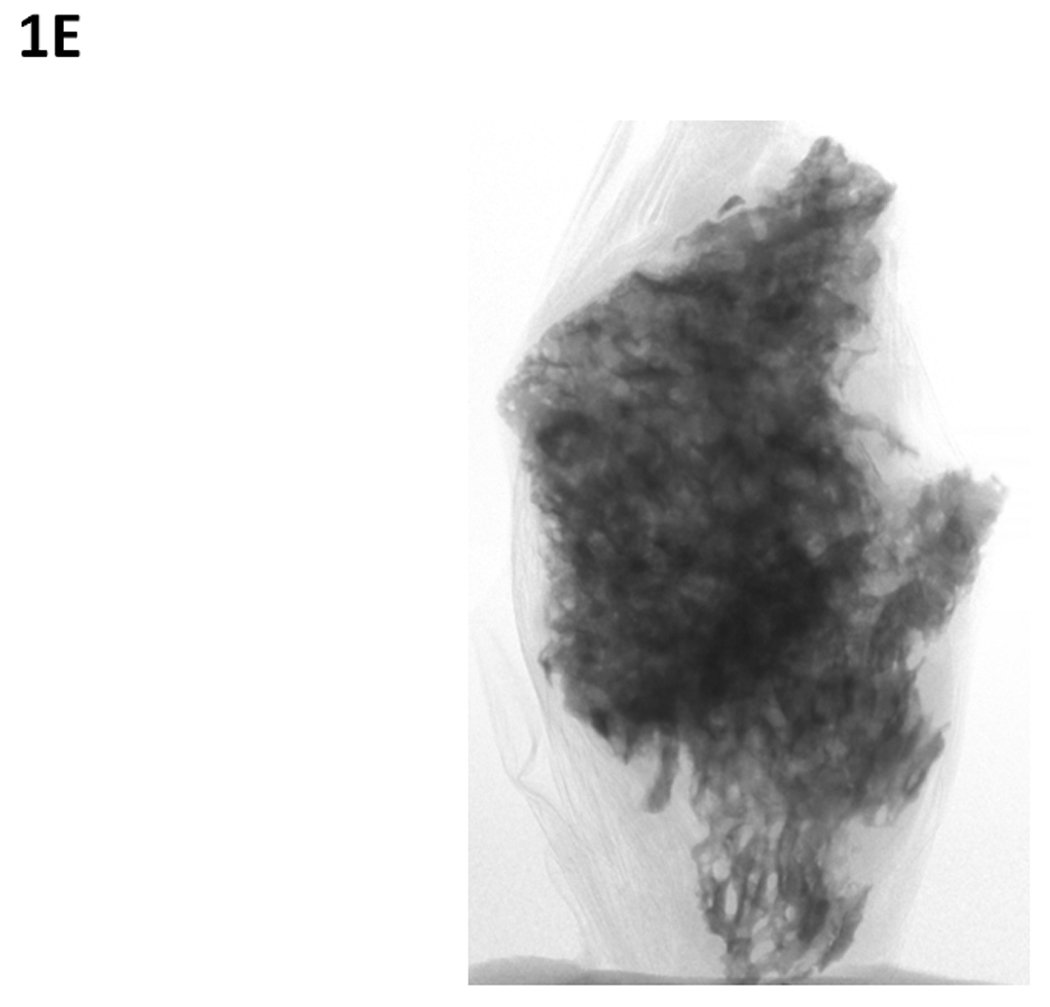
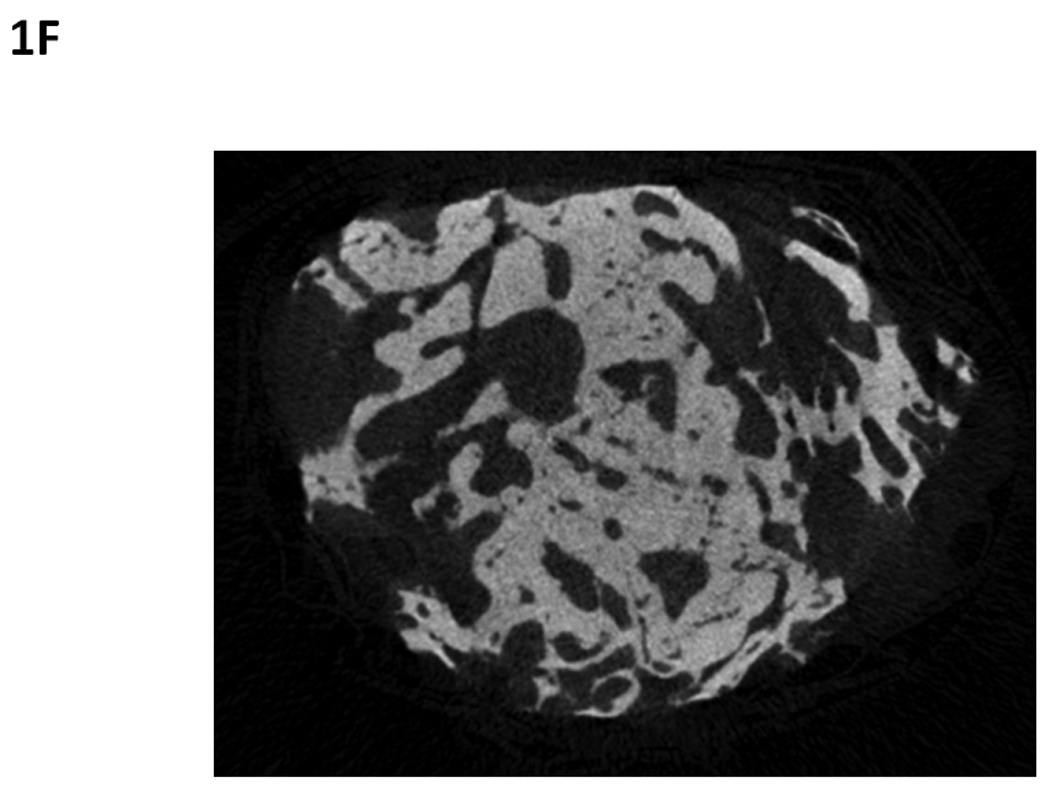
Osteonecrosis of the jaw sequestra from two different patients that had been diagnosed with ONJ for 6 months (A–C) or 48 months (D–F) prior to specimen collection. Specimens were photographed (A and D) and then scanned using micro-computed tomography which provides two dimensional projection (B and E) and cross-sectional (C and F) images. These images illustrate the similarly in the morphological structure of the specimens despite the differing durations of disease. In photographed image, each small square represents 1 mm × 1 mm.
Statistics
Statistical tests were performed with SAS software (SAS Institute, Cary, NC). Pearson correlations were used to determine the relationship between patient characteristics and micro-CT variables. A p-value of < 0.05 was considered statistically significant.
RESULTS
There was no correlation between the duration of ONJ prior to bone tissue removal and either BV/TV or BS/BV. Specifically, the r value for BV/TV was 0.026 (p = 0.887) while the r value for BS/BV was -0.011 (p = 0.950) (Figure 2A and 2B). There was also no correlation between the duration of BP treatment and either BV/TV (r = 0.084, p = 0.650) or BS/BV (r = -0.162, p = 0.383) (Figure 2C and 2D).
Figure 2.
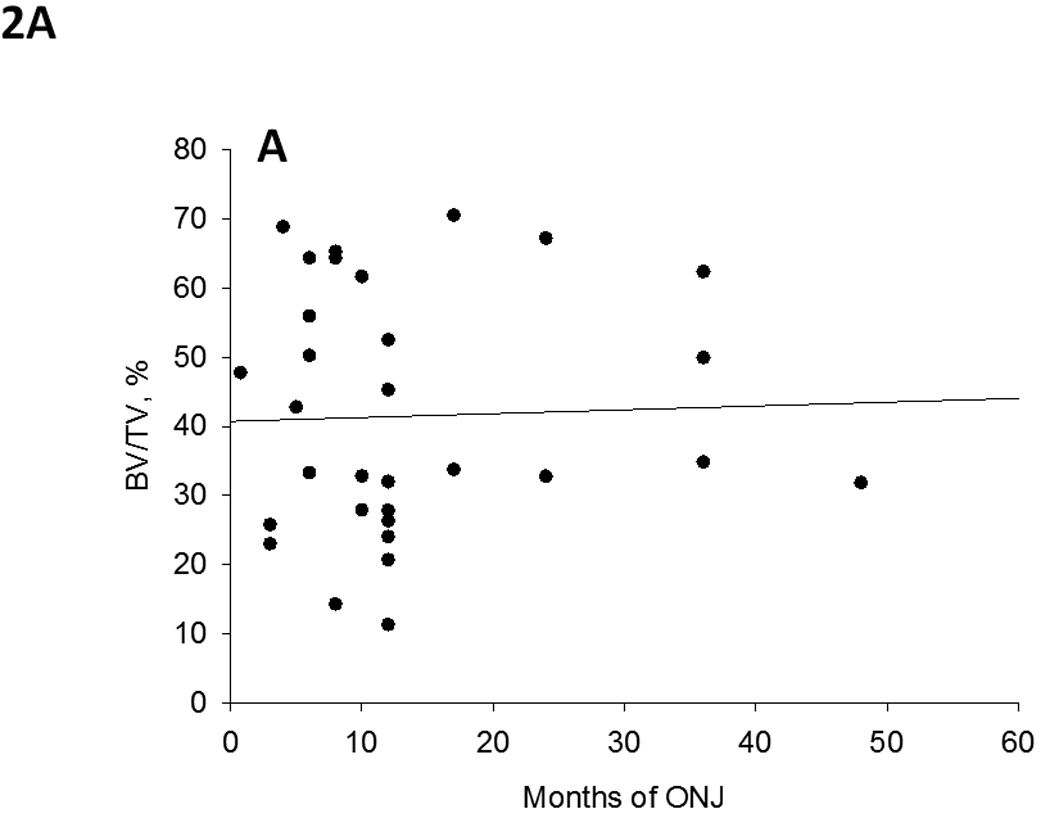
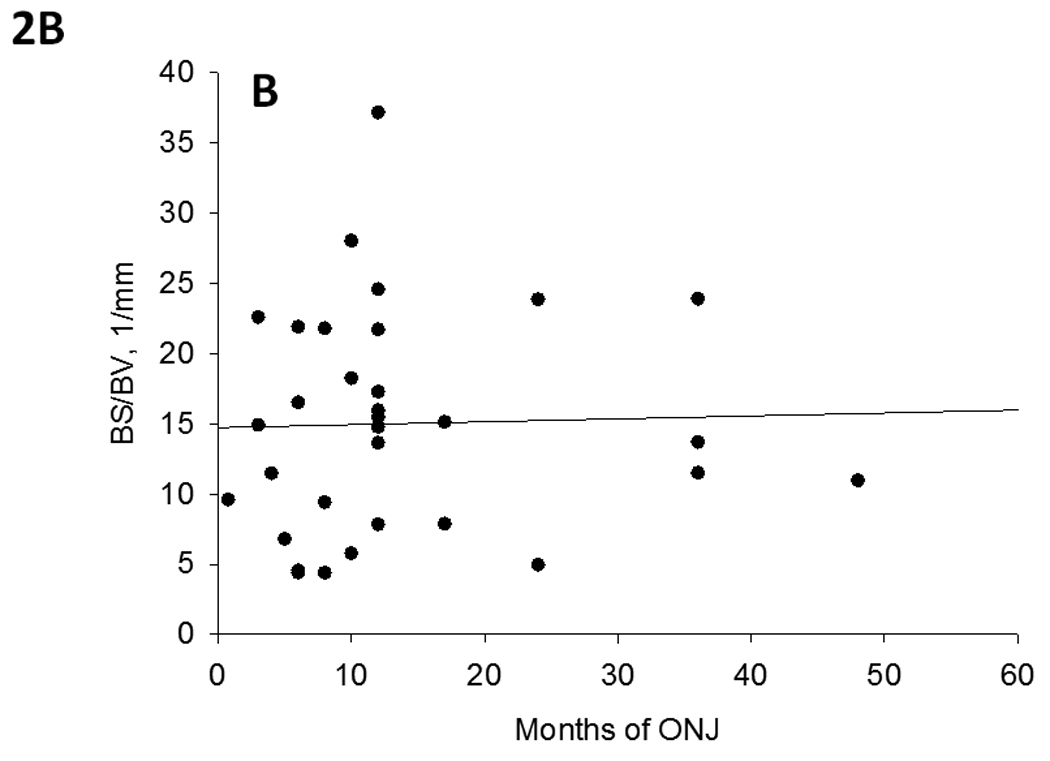
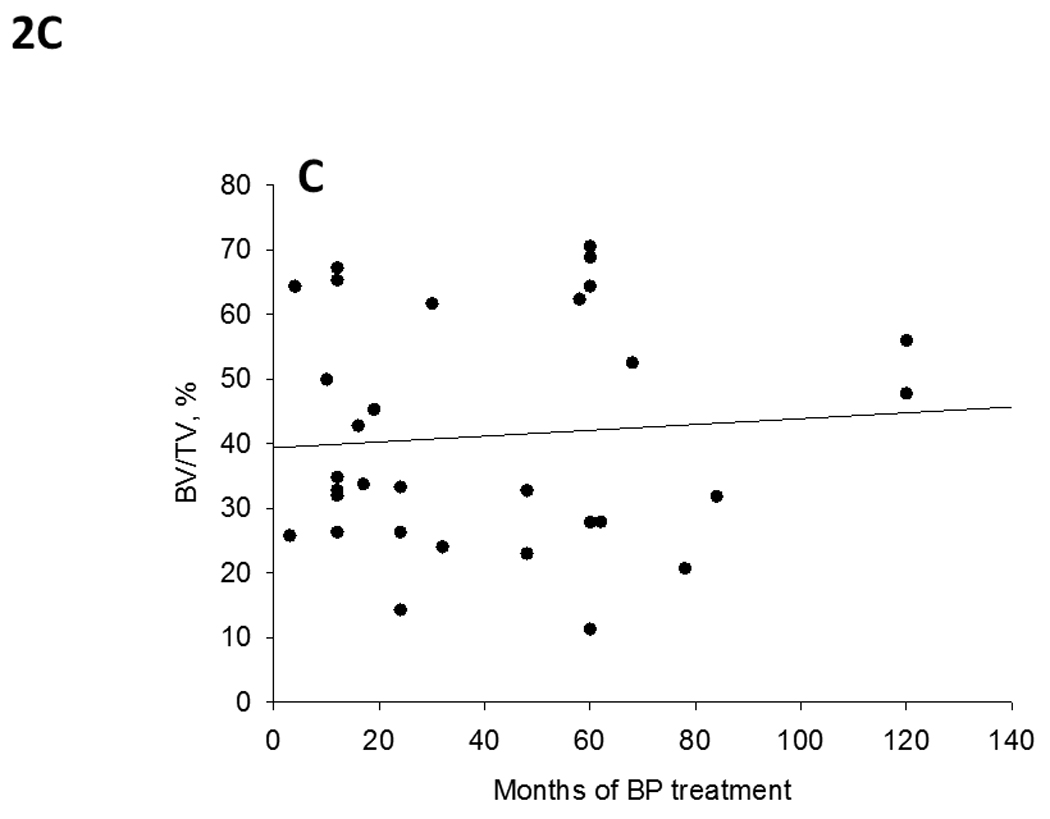
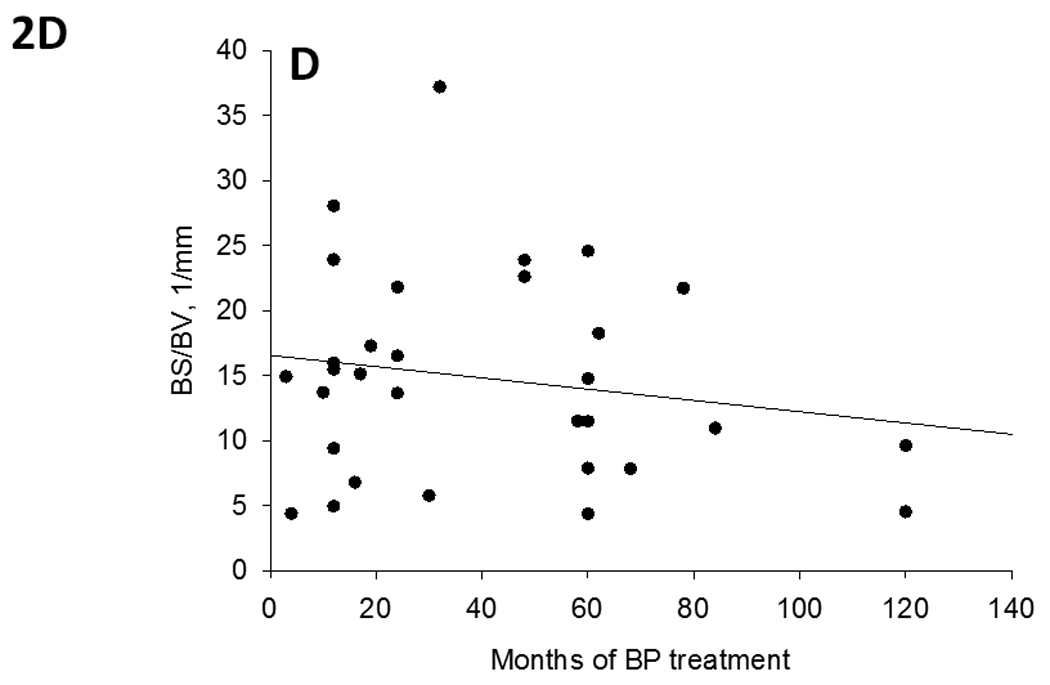
Relationships between sequestra morphology and the duration of ONJ (A and B) or duration of bisphosphonate treatment (C and D). There was no correlation between the duration of ONJ prior to bone tissue removal either BV/TV (r = 0.026, p = 0.887) or BS/BV (r = -0.011, p = 0.950). There was also no correlation between the duration of BP treatment and either BV/TV (r = 0.084, p = 0.650) or BS/BV (r = -0.162, p = 0.383).
In the two specimens collected at two different times (6 months and 8 months post-diagnosis) BV/TV was higher at the first time-point (65%) compared to the second (33%); BS/BV was higher at the second compared to the first. In the case where multiple pieces were obtained at the same time, there was general homogeneity in the morphology among samples. Specifically, the BV/TV in the individual with 6 pieces ranged from 27% to 39%; the patient with three pieces had BV/TV ranging from 14% to 15.8%; the patient with two pieces had BV/TV values of 22.4% and 23.9%.
Mean tissue density was not significantly correlated to either duration of ONJ (r = 0.21 p = 0.25) or duration of BP treatment (BV/TV, r = -0.09, p = 0.61). Consistent with our previous work [8], there was a wide range of mean tissue densities among the specimens (Figure 3). This range includes samples above and below a +/− 2.5 SD range of z-scores calculated from non-ONJ control tissue [8].
Figure 3.
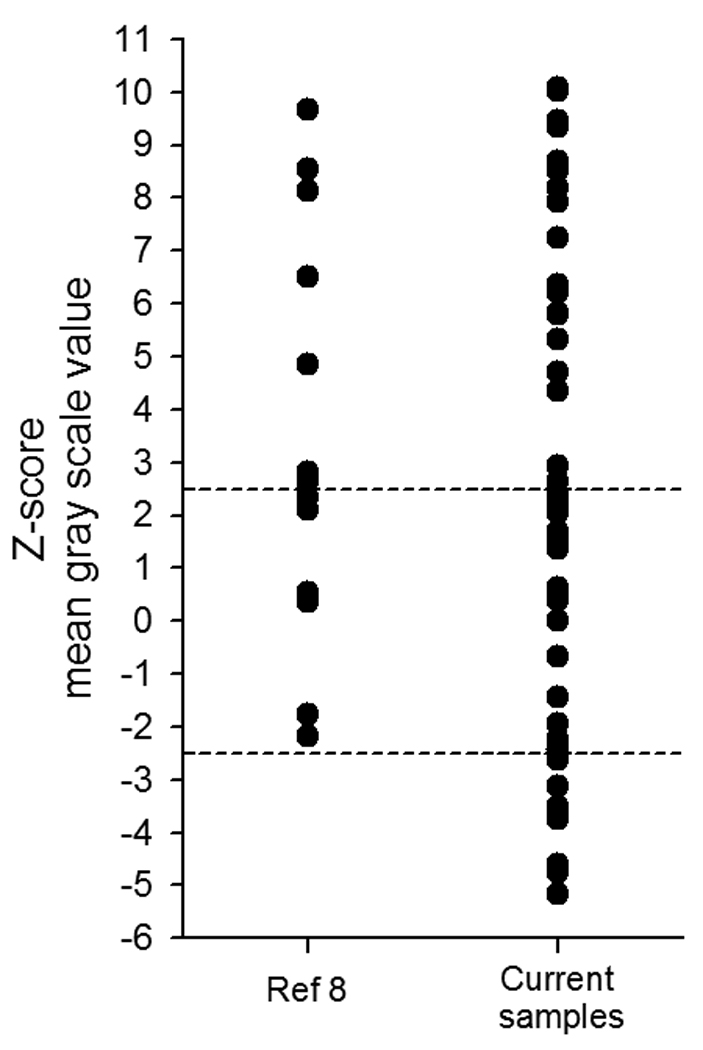
Density heterogeneity of ONJ sequestrum. Using z-score analysis based on non-ONJ mandible tissue from our previous work [8], the density of sequestra is shown to be highly heterogeneous. This heterogeneity is consistent with our previous work, yet in this sample population we found both high and low density specimens (dotted lines represent +/− 2.5 standard deviations).
DISCUSSION
Progress toward understanding osteonecrosis of the jaw (ONJ) necessitates studies of tissue from patients afflicted by this condition. Since the proposed treatment of individuals with ONJ is conservative, tissue samples become available only when the exposed bone is debrided – a procedure that is highly variable with respect to timing post-diagnosis. If the duration of ONJ influences the properties of the tissue, this would result in highly heterogeneous tissue properties among patients making it challenging to draw conclusions about the tissue. As the majority of reports to date that have focused on properties of sequestra have been qualitative, this issue has not been of great concern. However, moving forward the issue will likely become more relevant. Our results, showing no relationship between the duration of ONJ and bone morphology, are encouraging as they provide evidence that interpretation of past studies [5–12] were not likely influenced by differences in disease exposure prior to sample collection. They also suggest that future studies with ONJ tissue specimens can reliably utilize specimens that have had the condition for various durations.
Our data document that the length of ONJ diagnosis prior to sample collection is not correlated to the bone morphology. Although these are correlative data, this finding would suggest that the majority of changes to the tissue occur early in the disease progression, perhaps even before the tissue becomes exposed. Numerous reports have described highly scalloped surfaces and abundant osteoclasts in ONJ specimens [5–12]. Our a priori hypothesis based on these observations was that the longer a patient had ONJ the less bone volume (and greater bone surface/bone volume) would be present in the sequestrum, as bone resorption would be actively removing the tissue. The results of our analysis show otherwise – there is no relationship between duration of disease and bone morphology (Figure 2). We interpret this to mean that despite the presence of osteoclasts in ONJ sequestra, these cells are not sufficiently active to meaningfully alter the morphology once the bone becomes exposed. This makes intuitive sense based on the mechanism of bisphosphonate action, which significantly reduces osteoclast activity although it may not significantly alter the number of osteoclasts that are present.
The duration of BP treatment is significantly associated with the risk of developing ONJ [13]. Based on this, we asked a related question: does the duration of BP treatment prior to diagnosis of ONJ influence the tissue properties? Our results, showing no correlation between these two parameters, suggests the answer to this question is no. This tells us that while the risk of ONJ is increased with increasing duration of BP treatment [13], the properties of the sequestra tissue are independent of BP duration.
We have previously reported a high degree of heterogeneity in the mean tissue density of ONJ sequestra [8]. Using a similar method of analysis, but now in a larger number of specimens, the current work shows a similar degree of heterogeneity. Interestingly we show that a number of specimens had very low levels of mineralization, whereas our previous report showed that extreme values were all in the higher range of density values. As with the morphological parameters, the mean tissue density was not correlated with either duration of ONJ or duration of BP use. Based on these results, we continue to believe that the density heterogeneity proves problematic with respect to the development of imaging methods, based on density, to visualize ONJ lesions prior to their exposure.
Our study lacked assessment of control tissue. As the goal of this study was to understand how the duration of this specific disease affects the morphology of the sequestra, the need for control tissue is lessened. Clearly, to understand whether the properties of the squestra that manifest in ONJ are similar/different than other forms of necrosis, a question that is important yet beyond the scope of the current work, such control tissue is essential,
In conclusion we report a lack of correlation between the duration of ONJ and the bone morphology of sequestra. Such a finding has important implications for the design and interpretation of ONJ studies as it suggests that the heterogeneity in timing of tissue collection is not playing a major role in the tissue properties. It also suggests that much of the change in tissue morphology occurs early in the disease, with little activity during the period which it is exposed in the oral cavity.
ACKNOWLEDGEMENTS
We would like to thank Mark Koivuniemi for assistance with micro-CT scanning. This work was supported in part by grants from the NIH (R21-DE019686 and S10-RR023710).
REFERENCES
- 1.Russell RG, Xia Z, Dunford JE, et al. Bisphosphonates: an update on mechanisms of action and how these relate to clinical efficacy. Ann N Y Acad Sci. 2007;1117:209. doi: 10.1196/annals.1402.089. [DOI] [PubMed] [Google Scholar]
- 2.Rodan GA, Fleisch HA. Bisphosphonates: Mechanisms of action. Journal of Clinical Investigation. 1996;97:2692. doi: 10.1172/JCI118722. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Allen MR, Burr DB. The Pathogenesis of Bisphosphonate-Related Osteonecrosis of the Jaw: So Many Hypotheses, So Few Data. Journal of Oral and Maxillofacial Surgery. 2009;67:61. doi: 10.1016/j.joms.2009.01.007. [DOI] [PubMed] [Google Scholar]
- 4.Khosla S, Burr D, Cauley J, et al. Bisphosphonate-associated osteonecrosis of the jaw: Report of a task force of the American Society for Bone and Mineral Research. Journal of Bone and Mineral Research. 2007;22:1479. doi: 10.1359/jbmr.0707onj. [DOI] [PubMed] [Google Scholar]
- 5.Lesclous P, Abi Najm S, Carrel JP, et al. Bisphosphonate-associated osteonecrosis of the jaw: a key role of inflammation? Bone. 2009;45:843. doi: 10.1016/j.bone.2009.07.011. [DOI] [PubMed] [Google Scholar]
- 6.Sedghizadeh PP, Kumar SK, Gorur A, et al. Identification of microbial biofilms in osteonecrosis of the jaws secondary to bisphosphonate therapy. J Oral Maxillofac Surg. 2008;66:767. doi: 10.1016/j.joms.2007.11.035. [DOI] [PubMed] [Google Scholar]
- 7.Sedghizadeh PP, Kumar SK, Gorur A, et al. Microbial biofilms in osteomyelitis of the jaw and osteonecrosis of the jaw secondary to bisphosphonate therapy. J Am Dent Assoc. 2009;140:1259. doi: 10.14219/jada.archive.2009.0049. [DOI] [PubMed] [Google Scholar]
- 8.Allen MR, Ruggiero SL. Higher Bone Matrix Density Exists in Only a Subset of Patients With Bisphosphonate-Related Osteonecrosis of the Jaw. Journal of Oral and Maxillofacial Surgery. 2009;67:1373. doi: 10.1016/j.joms.2009.03.048. [DOI] [PubMed] [Google Scholar]
- 9.Badros A, Weikel D, Salama A, et al. Osteonecrosis of the jaw in multiple myeloma patients: Clinical features and risk factors. Journal of Clinical Oncology. 2006;24:945. doi: 10.1200/JCO.2005.04.2465. [DOI] [PubMed] [Google Scholar]
- 10.Bedogni A, Blandamura S, Lokmic Z, et al. Bisphosphonate-associated jawbone osteonecrosis: a correlation between imaging techniques and histopathology. Oral Surgery Oral Medicine Oral Pathology Oral Radiology and Endodontology. 2008;105:358. doi: 10.1016/j.tripleo.2007.08.040. [DOI] [PubMed] [Google Scholar]
- 11.Favia G, Pilolli GP, Maiorano E. Histologic and histomorphometric features of bisphosphonate-related osteonecrosis of the jaws: An analysis of 31 cases with confocal laser scanning microscopy. Bone. 2009;45:406. doi: 10.1016/j.bone.2009.05.008. [DOI] [PubMed] [Google Scholar]
- 12.Allegra A, Russo S, Cannavo A, et al. IMMUNOHISTOCHEMICAL EVALUATION OF SARCOGLYCANS AND INTEGRIN IN GINGIVAL EPITHELIUM OF MULTIPLE MYELOMA PATIENTS WITH BISPHOSPHONATE-INDUCED OSTEONECROSIS OF THE JAW. Haematologica-the Hematology Journal. 2009;94 0943. [Google Scholar]
- 13.Hoff AO, Toth BB, Altundag K, et al. Frequency and risk factors associated with osteonecrosis of the jaw in cancer patients treated with intravenous bisphosphonates. Journal of Bone and Mineral Research. 2008;23:826. doi: 10.1359/JBMR.080205. [DOI] [PMC free article] [PubMed] [Google Scholar]