

Abstract
The social acceptability and durability of two house screening interventions were addressed using focus group discussions, questionnaires, indoor climate measurements, and durability surveys. Participants recognized that screening stopped mosquitoes (79–96%) and other insects (86–98%) entering their houses. These and other benefits were appreciated by significantly more recipients of full screening than users of screened ceilings. Full screened houses were 0.26°C hotter at night (P = 0.05) than houses with screened ceilings and 0.51°C (P < 0.001) hotter than houses with no screening (28.43°C), though only 9% of full screened house users and 17% of screened ceiling users complained about the heat. Although 71% of screened doors and 85% of ceilings had suffered some damage after 12 months, the average number of holes of any size was < 5 for doors and < 7 for ceilings. In conclusion, house screening is a well-appreciated and durable vector control tool.
Introduction
Historically, malaria has been controlled in many parts of the tropics by mosquito-proofing houses with screens,1–4 but since the 1950s this technology has been largely ignored. To assess whether house screening could be reintroduced as an effective malaria control strategy this century, a three-arm randomized controlled trial was conducted near the Medical Research Council Laboratories at Farafenni in The Gambia.5 Two different types of screening were compared with houses that received no protection, other than untreated bed nets for the residents: 1) full screening, in which doors and windows were screened with polyvinyl chloride (PVC)-coated fiberglass netting and eaves sealed with a mortar of sand, rubble, cement, and water; and 2) screened ceilings, in which the same netting material was stretched from wall to wall below the eave gap. Over two years 188 full screened homes, 178 with screened ceilings, and 96 controls completed the trial. It was found that houses with full screening had 59% fewer Anopheles gambiae sensu lato, the major African malaria vector, indoors at night, and screened ceiling houses 47% fewer, than unscreened houses.6 More importantly, the effect of these reductions was evident in the clinical data collected. Anemia prevalence was reduced by about half among children in full screened houses and among those in screened ceiling houses compared with those in unscreened houses.6 Because severe anemia is a major cause of mortality in young African children,7,8 house screening is likely to save lives.
This evidence alone is compelling, but the argument for advocating screening use would be even stronger if it could be demonstrated that occupiers of screened houses appreciated the positive health impacts the intervention introduced into their domestic environment. It has often been argued that human behavior, and social, cultural, and economic contexts should be integrated into the conception of research and intervention programs.9 Understanding the context into which an intervention is being introduced and identifying the factors that are likely to enhance or constrain the acceptability and utility of the intervention provides data that are essential to inform decisions likely to affect the long-term success of that program.10 The aim of this current study was to identify the factors that affect perceptions of the utility and usability of the screening interventions in the context of the house screening trial, and to assess the relative acceptability of the two types of screening to the participants involved.
Materials and Methods
Study area.
A detailed description of the study site and population has been published elsewhere.11 Briefly, the study area was located ~170 km from the mouth of the Gambia River and encompassed 70 km2 of the North Bank Division in The Gambia, an area of Sudan savannah vegetation. Typically, there is a single rainy season annually, lasting from June to October, followed by a long dry season. Malaria transmission is largely confined to the rainy season. Ten percent of houses in the intervention trial were located in Farafenni town (Universal Transverse Mercator [UTM] coordinates: 1500200N, 435500E) and 90% in 25 villages located within 15 km of the town. The study area population included 7,852 people dominated by three ethnic groups; Mandinka (28%), Wollof (38%), and Fula (27%), with roughly equal numbers of men (53%) and women (47%).
Study design.
The study was designed as a three-armed randomized controlled trial. Houses were allocated to one of three arms: full screening, screened ceilings, or no screening. The study took place over 2 years, with a different cohort of houses used in year 1 and 2. Screening was installed between March and May in both years. Mosquito collections were made from June to October, followed by clinical surveys in November.5
Collection of acceptability and durability data.
Data were collected through a combination of qualitative and quantitative methods. A series of focus group discussions were held with a selection of householders in each trial arm to gather information on general perceptions of the types of screening and to identify the key concerns and benefits of the screening as perceived by those taking part in the trial. These data were then used to design a questionnaire survey to assess the extent to which these perceptions were held by all of the householders involved in the trial. In addition to data on participants' perceptions, indoor air temperature and relative humidity (RH) was recorded in houses in each trial arm to assess thermal comfort. Damage to the netting and other structural elements of the screening were recorded to assess durability.
Focus group discussions.
Focus group discussions (FGDs) were conducted in October and November, ~5 months after the screening had been installed. The discussions were used largely to evaluate the community's ideas concerning the effectiveness of the program. During the discussions the following topics were debated: the impact of the screening on 1) the presence of mosquitoes and other insects, 2) living conditions inside the house, 3) bed net use, 4) closing of doors and windows, 5) the appearance of the house, 6) upkeep, and 7) cost of screening replacement. It was of particular interest to see what the participants identified as major problems with the screening, and to build their needs into any changes in the design of the screening for the second year, if appropriate.
Each FGD, where possible, included six same-sex participants, all sleeping in one type of screened house (either full screening or screened ceiling). This composition of the groups was designed to encourage each individual participant to speak more freely about the trial without fear of being judged by others thought to be superior, more expert, or more conservative. This was important for the female groups, especially those containing young women, as they are traditionally less forthcoming in their ideas and opinions in the presence of their husbands and the village elders.
Focus group discussions were conducted in the local language common to the location, i.e., Mandinka, Wollof, or Fula. The FGDs were conducted by a trained moderator (PB) who was fluent in all three languages and English. PB was guided by a supervising moderator (MJK/CJ/AK). The moderator introduced each topic for discussion, following closely pre-prepared topic guides (Supplementary files 1 and 2, available at www.ajtmh.org) specific to each trial arm, and helped the group to participate in a lively and natural discussion. The controlling moderator had the final say about the direction of the discussion by pointing out questions that were not well explored or missed. Seating arrangements were as suggested for translator-assisted focus groups.12 There were two recorders present at every meeting to record the responses and quotes from the group. These were noted in English, the written language of The Gambia.
Questionnaires.
The FGD summary sheet data were used to design a questionnaire to test how widely the beliefs, attitudes, and opinions held by FGD members were expressed by all study participants. Specifically, householders from all screened houses were asked if they had experienced any or all of seven benefits and seven problems that were expressed commonly in FGDs. Participants from both intervention groups were then asked to choose whether to keep the screening they had been allocated or to have it removed, with the option of having the other screening type installed. Occupants of control houses were also given the choice of having either screening type installed but did not answer questions concerning benefits or problems. The questionnaire was administered after the clinical survey, at the same time as the 6-month durability survey. Bed net use by children was recorded in a separate study subject questionnaire.
Durability surveys.
Sensitization meetings were held in all study villages once the screening had been installed, to inform the participants of guidelines that, if followed, would help prevent damage and so maximize the durability of the screening against mosquito house entry. Occupants of both types of screened houses were instructed to keep their windows and doors closed wherever possible and to be careful when carrying sharp objects near the netting. Those in full screened houses were also told to use the door handles or kickboards to open and close the screened doors, rather than pushing on the netting. The durability surveys, carried out at 6 and 12 months after the screening was installed, recorded data specific to each type of screening. For screened ceilings these were 1) the condition (intact, some damage, badly damaged) and the number of holes larger than 1, 2, and 10 cm diameter, in the netting; 2) the condition of the wooden battens that secured the netting to the wall; 3) the condition of the mortar that sealed gaps between the battens and the wall; 4) the presence of any gaps between the battens and the wall. For full screened houses these were 1) the condition (intact, some damage, badly damaged) and the number of holes larger than 1, 2, and 10 cm diameter, in the netting; 2) the condition of the wooden framework of doors and windows; 3) the condition of the mortar that held the doors and windows in place; 4) the condition (intact, damaged, or missing) of the elastic door pull, the door handles, and door push bars; 5) whether the doors were still tightly fitted within the frames; 6) whether the doors were propped open at the time of survey, and if yes, what time were they closed; 7) the condition (intact, some damage, badly damaged) of the mortar that filled the eave gap; 8) the number of holes greater than 1 cm diameter in the mortar that filled the eave gap.
Indoor climatic conditions.
Indoor climatic conditions were recorded, concurrent with mosquito collection, from a subset of 274 study houses: 64 controls, 102 with screened ceilings and 108 full screened houses between June and November each year. In six houses each night, two from each arm of the trial in the same village when possible, a single data logger (HOBO U12 Temp/RH/Light External Data Logger, Onset Computer Corp., Bourne, MA) was hung inside the house. The loggers were pre-set to turn on automatically at 7:00 pm and to record conditions every 30 minutes. Loggers were collected each morning at 7:00 am and the data downloaded to Onset HOBOware version 2.0 software.
During the period Oct 29–Nov 4, 2007 data loggers were set to record conditions every 30 minutes for 24 hours in a separate subset of 27 houses: 7 controls, 9 with screened ceilings and 11 full screened houses.
Time to bed.
Six stopwatches, left each night in the same houses as the data loggers, were used to record the time at which the study children occupying those houses went to bed. A fieldworker recorded the time that she/he started the stopwatch, and instructed a responsible adult (usually the mother) to stop the watch once all the children (6 months to 10 years of age) that slept in that house had gone to bed. The stopwatches were collected the following morning and the time elapsed was added to the starting time to give the “time to bed.”
Qualitative data analysis.
At the end of every focus group there was a debriefing session that examined the focus group session notes in conjunction with the topic guides. The notes of both recorders were compared, consensus was sought where they disagreed, and sections that were poorly recorded were removed. A single transcript was generated for each FGD and sections that corresponded with the specific study questions were coded accordingly. All coded responses from all FGD were then entered into summary result sheets to draw generalized views across the issues discussed.
Quantitative data analysis.
Indoor climate data generated by data loggers were summarized first as nightly maximum, minimum, and mean values, and then as average values of these outcomes for the total number of samples taken for each house. Data for each intervention arm were weighted by the number of recordings made for each house and stratified by roof type (metal sheet or grass thatch). A paired t test was used to compare the mean maximum temperatures recorded from houses whose occupants subsequently reported that the screening made the room too hot (“hot houses”) with the mean maximum temperature from all other houses of the same intervention type recorded on the same night.
The frequencies of full screening and ceiling house occupants experiencing the common benefits and problems were compared using contingency tables to generate Mantel Haenszel χ2, stratifying by study year. Within each intervention group, the same approach was used to compare the frequency of experiences between participants that kept their screening and those who changed to the other type of screening. Contingency tables were also used to compare bed net use between intervention groups and the control group, and to compare the damage to the screening between surveys and years. The presence of holes in the doors of full screened houses and in the ceilings were analyzed in the same manner, as total number of holes (> 1 cm + > 2 cm + > 10 cm) and for each hole size category separately. The number of holes was analyzed as continuous data and separately as ordinal data (0–2 holes v 3 + holes). For the doors, the holes in the front door only and the mean number of holes for all doors combined were considered in separate analyses. To assess whether damage to the screening reduced the efficacy against mosquito house entry, the durability data was regressed against the geometric mean number of An. gambiae sensu lato and the total number of mosquitoes caught inside each house, weighted by the number of mosquito surveys for each house within 1 month either side of each durability survey. Analyses were done with SPSS version 15.0 (SPSS Inc., Chicago, IL), EpiInfo version 6 (CDC, Atlanta, GA), and Stata version 10.1 (Stata Corp., College Station, TX). This study was registered as an International Standard Randomized Controlled Trial, no. ISRCTN51184253.
Ethical approval.
Ethical approval for this study was given by the Gambian Government and Medical Research Council Laboratories Joint Ethical Committee and the Ethics Advisory Committee of Durham University. Verbal and written consent was given by all participants before the start of the study. Focus group discussion participants were reassured of their anonymity before discussion started.
Results
Focus group discussions.
In total 10 FGDs were conducted in eight different villages, five with participants from full screened houses, four with those from screened ceiling houses, and one mixed group. Four of the groups contained men only and six women only.
Most participants in screened ceiling houses noticed mosquito numbers were “reduced” or “minimized” after the ceiling was installed. One group that did not experience this thought this was because mosquitoes entered largely through their doors. Participants in full screened houses agreed unanimously that there were less mosquitoes, and were more emphatic than those in screened ceiling houses, citing “definite reductions,” “big impact,” and one participant stating screening was “the most protective equipment he had used” against mosquitoes. Many participants from both types of screened house noticed that the screening also stopped other animals from entering their house, including bats, cockroaches, earwigs, geckos, mice, rats, snakes, and toads. Also common to both interventions was a perception that occupants slept better at night, especially when it was windy or raining heavily. This was attributed to less dust, dirt, and leaves falling on them while they slept, and the extra security and “peace of mind” that the screening provided, particularly the doors.
Bed net use was similarly affected by both types of screening. Several occupants gave their nets away to family members or simply stopped using them once their houses were screened because there were few mosquitoes, yet in other situations the abandonment of nets seemed to be determined more by increases in temperature or the end of the rains, than the screening or number of mosquitoes. There was a considerable range of door practice among participants. At night, those in screened ceiling houses largely had their doors closed for privacy and security, but some preferred at least one door open for ventilation. This was also the case for those in full screened houses before the screened doors were installed, but afterwards most people left their outer doors open and kept the inner screened doors closed. During the day it was rare that anybody had their doors closed because it reduced airflow and restricted access to children and others who regularly passed through the house. Several participants also considered closing doors to be an impolite gesture signifying a reluctance to welcome visitors.
Opinion was divided on how the screening affected the temperature inside the house. Those in screened ceiling houses who expressed a view largely said the house was hotter, although this was qualified by one group who declared it to be cooler in the morning and evening, but hotter during the day. Some in full screened houses felt it was less hot at night, though this was undoubtedly because they no longer closed their external corrugated metal sheet doors at night but only shut the screened doors. A few others pointed out that the screened doors increased the heat in the house during the day.
The appearance of the screening was generally appreciated; it made the house look “clean,” “bright,” and “beautiful,” though in a few cases the mortar looked untidy or was poorly finished, and did not match the color of the walls that had been painted. The white netting showed the dirt easily and the majority of participants expressed a preference for a darker color.
One major problem experienced with the full screening was that children and domestic animals damaged the doors, either making holes in the netting or breaking the push bars, handles, and hinges. In only one or two cases did the house-owners attempt repairs, patching holes or re-fixing fittings. For screened ceilings the difficulties were holes made by rats, termite damage to the battens, and a lack of access to the top of the net to clean away the debris that fell there from the roof. In fact, the netting becomes dirty, after ~1 to 3 months, was a complaint of both interventions, yet those who attempted to clean it with cloths or brushes were in the minority. Table 1 lists all the benefits and problems commonly experienced by both screening groups.
Table 1.
The most common benefits and problems associated with screened ceilings and full screening
| Benefits | Problems |
|---|---|
| Stops mosquitoes entering the house | Netting is hard to clean |
| Stops other insects entering the house | Screening makes the room too hot |
| Stops other animals entering the house | Masonry looks untidy |
| Beautifies the house | Rats have made holes in the netting |
| Improves privacy/security | Damage to screening by children |
| Stops dust and dirt entering the house | Damage to screening by domestic animals |
| Keeps the room cool | Nowhere to hang/store personal items |
The screening was valued highly by almost all the participants. Although they found it hard to estimate how much it would cost and did not know if the materials were available locally, most declared it would cost more than a bed net and would be too expensive for them to install it themselves. However, more of them thought that they could afford to maintain it, stating “we are ready to maintain the screening even without the Medical Research Council (MRC), if it would cost selling a goat to repair our screening, we would do it as we know they are very useful,” and many suggested alternative materials that could be used in repair work. It was believed by most that the present designs could last for 3 years or more in the case of ceilings, and 2 years for screened doors.
Questionnaires.
Data from the questionnaires largely supported the findings of the FGDs. Almost all (96%) householders from full screened houses noticed a reduction in the number of mosquitoes indoors. A decrease in mosquito numbers was also apparent to most occupants of screened ceiling houses (79%). However, of more importance to that group was that the screened ceiling stopped other insects from entering the house (86%). In general, all the benefits identified during FGDs were appreciated significantly more by the full screening group compared with the screened ceiling group, except the prevention of dirt and dust entering the house, which was appreciated equally by both groups (Table 2). Moreover, most of the problems were experienced by significantly more people in the ceiling group, particularly difficulties in cleaning the netting, which was the most common problem in the ceiling group. Two problems were unique to the full screening group: damage by children, the most important problem associated with full screening (57%) and damage by domestic animals (21%).
Table 2.
Number (%) of occupants with experience of the most common benefits and problems associated with house screening*
| Full screening N = 176 (%) | Ceiling N = 163 (%) | M–H χ2 | P | |
|---|---|---|---|---|
| Benefits | ||||
| Stops mosquitoes | 169 (96) | 128 (79) | 24.0 | < 0.001 |
| Stops other insects | 173 (98) | 140 (86) | 16.7 | |
| Stops other animals | 176 (100) | 88 (54) | 107.8 | < 0.001 |
| Beautifies | 176 (100) | 153 (94) | 27.2 | < 0.001 |
| Improves privacy | 176 (100) | 118 (72) | 53.4 | < 0.001 |
| Stops dust and dirt | 175 (99) | 160 (98) | 0.3 | n.s. |
| Keeps room cool | 160 (91) | 130 (80) | 7.9 | 0.005 |
| Others | 5 (3) | 1 (1) | – | – |
| Problems | ||||
| Netting is hard to clean | 87 (49) | 103 (63) | 5.9 | 0.02 |
| Screening makes room too hot | 15 (9) | 28 (17) | 4.9 | 0.03 |
| Masonry looks untidy | 23 (13) | 65 (40) | 30.1 | < 0.001 |
| Rats have made holes | 18 (10) | 96 (59) | 89.1 | < 0.001 |
| Damage by children | 101 (57) | 0 (0) | 134.8 | < 0.001 |
| Damage by domestic animals | 37 (21) | 0 (0) | 36.2 | < 0.001 |
| Nowhere to hang/store personal items | 2 (1) | 103 (63) | 148.7 | < 0.001 |
| Others | 7 (4) | 3 (2) | – | – |
n.s. = not significant.
When offered a choice of screening, most participants chose full screening regardless of whether they initially received screened ceilings, full screening, or no screening (Table 3). Participants who initially received ceilings and chose to keep them were more likely to have appreciated that the ceiling improved the appearance of the house (beautification) compared with those who changed to full screening (97% versus 90%, M–H χ2 = 8.1, P = 0.004), whereas those who changed to full screening were more likely to have complained that the ceiling reduced the space available to hang personal items (71% versus 54%, M–H χ2 = 5.3, P = 0.02). Participants who initially received full screening and chose to change to screened ceilings were more likely to have complained that the screening made the room too hot, compared with those who chose not to change (36% versus 7%, M–H χ2 = 11.6, P = 0.008). There were no other significant differences in experiences of the common benefits and problems between these sub-groups for either intervention.
Table 3.
Screening type preferences of study participants at the end of the trial
| Original treatment↓ | Treatment chosen at end of study | ||
|---|---|---|---|
| No intervention | Screened ceiling | Full screening | |
| No intervention (N = 96) | 1% | 17% | 82% |
| Screened ceiling (N = 179) | 2% | 46% | 52% |
| Full screening (N = 182) | 1% | 5% | 94% |
Durability.
The extent of damage to full screened houses was highly varied. Screened windows suffered little or no damage; even after 12 months 80% (36/45) of windows were still intact, i.e., no holes larger than 1 cm diameter in the netting. The mortar blocking the eaves was similarly durable, remaining intact after 12 months in 88% (147/167) of houses. The screened doors suffered greater damage than the windows or eave filling, but there was a big difference between the 2 years (Figure 1). In year 2 there were more than twice as many intact doors after 6 months than year 1 (122/211 versus 56/215, M–H χ2 = 18.3, P < 0.001) and still nearly twice as many after 12 months (68/186 versus 37/179, M–H χ2 = 6.2, P = 0.01). Although the majority of doors had suffered some damage after 12 months, the average total number of holes was only four (interquartile range [IQR] 1, 8) of any size in year 1 and 2 (0, 5) in year 2. Holes in the netting are easier to repair than damage to the door frame; importantly, 84% (166/198) of front doors in year 1 and 94% (181/192) in year 2 still closed tightly in the frame after 12 months, with no gaps large enough for mosquitoes to pass through. Although 49% (90/185) of front doors were found propped open using wooden blocks or bricks, at the time of the questionnaire survey visits (~14:00–16:00), in 81% (73/90) of these cases the doors were then closed before 20:00 h, according to the residents. Forty-eight percent (79/165) of the elastic door pulls had been removed or badly damaged by 12 months (both years).
Figure 1.
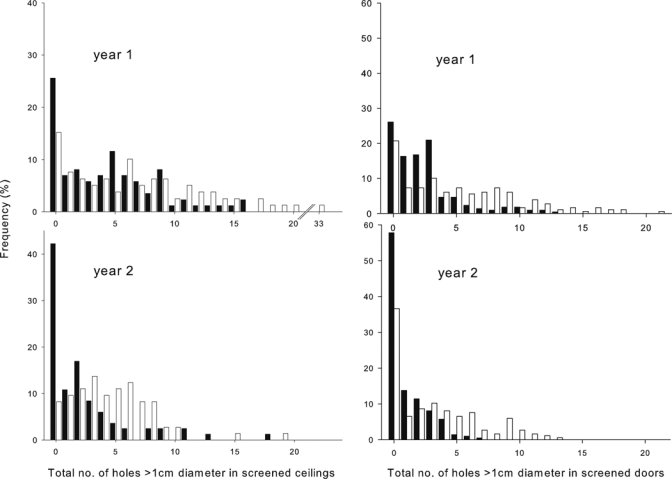
Comparison of total holes in netting at 6 (black bars) and 12 (white) months after installation.
In screened ceiling houses the main type of damage was also holes in the netting, with very little damage to the battens or masonry. Unlike the full screening, there were no differences between the 2 years in the number of intact ceilings at 6 months (22/86 versus 37/83, M–H χ2 = 3.2, P = 0.07) or 12 months (16/82 versus 7/74, M–H χ2 = 2.3, P = 0.13). Although nearly all ceilings had suffered some damage by 12 months, the average total number of holes of any size was again low: 6 (IQR 2, 11) in year 1 and 4 (2, 7) in year 2. Figure 1 shows the frequency of the number of holes in screened doors and screened ceilings after 6 and 12 months, for both years.
There were no statistically significant relationships between any of the measures of durability and the number of mosquitoes caught indoors for either intervention.
Indoor climatic conditions.
At night, full screened houses were approximately 0.5°C hotter and drier by 1% RH than unscreened control houses, and 0.25°C hotter than houses with screened ceilings. These differences, though small, were statistically significant (Table 4).
Table 4.
Comparison of indoor climatic conditions between trial arms*
| Mean value | Difference (95% CI) | t | P | |
|---|---|---|---|---|
| Temperature | ||||
| Control | 28.43°C | |||
| Screened ceiling | 28.68°C | vs. Control 0.25 (0.06, 0.45) | 2.7 | 0.01 |
| Full screening | 28.94°C | vs. Control 0.51 (0.35, 0.67) | 6.6 | < 0.001 |
| vs. Ceiling 0.26 (0.01, 0.52) | 2.1 | 0.05 | ||
| Relative humidity (RH) | ||||
| Control | 76.9% | |||
| Screened ceiling | 76.3% | vs. Control −0.6 (−1.5, 0.3) | −1.4 | n.s. |
| Full screening | 75.7% | vs. Control −1.2 (−2.2, −0.2) | −2.5 | 0.02 |
| vs. Ceiling −0.6 (−1.7, 0.5) | −1.2 | n.s. |
n.s. = not significant.
The 24 h experiment showed the screened ceiling houses were 0.34°C hotter (t = 2.5, P = 0.01) and the full screened houses 0.39°C (t = 4.5, P < 0.001) hotter than the control houses during the daytime hours (7:00 am–6:30 pm), but not different from each other. The results of the night-time hours replicated the main data set: full screened houses were 0.43°C hotter, and screened ceilings 0.24°C hotter than control houses (Figure 2).
Figure 2.
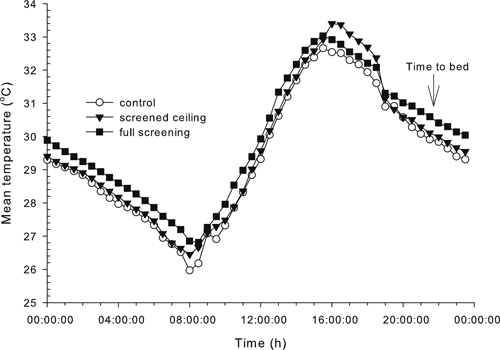
Variation in mean indoor temperatures recorded every 30 minutes from unscreened, full screened, and screened ceiling houses.
There were 54 nights of indoor climate data for houses whose occupants subsequently reported that the full screening made the room too hot (the full screening “hot houses”), and 68 nights for ceiling “hot houses.” On these nights maximum temperatures were on average 0.45°C higher in the full screening “hot houses” compared with the other full screened houses recorded on the same night (“hot house” mean maximum temperature = 31.49°C, 30.92–32.06; other full screened houses = 31.04°C, 30.56–31.53, t53 = 3.5, P < 0.001). However, there was no difference between the mean maximum temperature experienced in the ceiling “hot houses” and other ceiling houses on the same night (30.35°C versus 30.44°C, t68 = −0.9, p = not significant [n.s.]).
Time to bed.
There was no detectable influence of the installation of screening on the time at which children in the house went to bed. The average times were so remarkably similar (control = 9:50 pm [95% confidence intervals 9:34, 10:06], full screening = 9:47 pm [9:34, 10:00], screened ceiling = 9:49 pm [21:36, 22:02]) that the data were not analyzed further.
Bed net use.
At the end of the transmission season there were fewer children using any kind of bed net in the two intervention groups compared with the control group (Table 5). These differences are reflected strongly in the data for untreated nets, suggesting a reduction in the use of untreated nets accounts for the overall difference in net coverage between control and intervention groups. There were no differences in bed net coverage between the two intervention groups.
Table 5.
Variation in bed net coverage of study children between trial arm*
| Net type | Intervention | N | % | Comparison | N | % | M–H χ2 | P |
|---|---|---|---|---|---|---|---|---|
| ITN | Ceiling | 70 | 26 | vs. Control | 57 | 35 | 4.4 | 0.04 |
| Full screening | 98 | 31 | vs. Control | 57 | 35 | 0.7 | n.s. | |
| vs. Ceiling | 70 | 26 | 2.6 | n.s. | ||||
| Untreated net | Ceiling | 59 | 22 | vs. Control | 50 | 31 | 10.8 | 0.001 |
| Full screening | 64 | 23 | vs. Control | 50 | 31 | 9.6 | 0.002 | |
| vs. Ceiling | 59 | 22 | 0.07 | n.s. | ||||
| Any net | Ceiling | 129 | 47 | vs. Control | 107 | 66 | 15.0 | < 0.001 |
| Full screening | 163 | 52 | vs. Control | 107 | 66 | 8.4 | 0.004 | |
| vs. Ceiling | 129 | 47 | 1.6 | n.s. |
ITN = insecticide-treated net; n.s. = not significant.
Discussion
In an earlier study we showed that full screening (adjusted odds ratio 0.53) and screened ceilings (0.51) protected children against anemia by a similar degree.6 However, data from this study show that full screening was the more acceptable and appreciated option. Occupants of full screened houses were more likely to assert that they experienced the benefits of screening compared with those in screened ceiling houses; primarily a reduction in mosquitoes and other animals inside the house, and an increase in privacy. They also experienced fewer of the problems common to both interventions.
Because there was no significant difference between the two interventions in the number of mosquitoes caught inside the houses,6 it is interesting that the perceived level of protection given by ceilings was less than the full screening. Ceilings may raise awareness of mosquitoes in the house because those that enter the room become more visible when resting on the white netting ceiling. By using darker colored material this trend may be reversed. Darker material will also make dirt less apparent and so prolong the period before householders perceive the need to clean the netting, as has been reported for bed nets.10,13
Bed net use was lower in both intervention groups compared with the control group, but it is not uncommon for a trial intervention to have this effect on pre-existing mosquito control measures. For example, participants of a permethrin-treated bed net trial in Western Kenya reduced their use of mosquito coils and insect spray compared with the control group.14 The largest differences were in untreated net coverage, suggesting net users may stop using an untreated net if their house is screened, but would carry on using an insecticide-treated net (ITN).
The intention of comparing house screening with bed nets is not to suggest that one should be a substitute for the other, but to draw attention to situations in which screening may be the more favorable option. Although nationwide ITN coverage in The Gambia has been reported to be as high as 60–85%,15,16 surveys are typically concerned with net ownership, not use. We report much lower rates in this study (30% ITN usage and 53% for any net). Where there are too few bed nets to cover all individuals in a household, inequities in coverage associated with gender or status within the family may occur. In such circumstances it could be argued that house screening can overcome these inequities, because, as one participant put it, “screened [ceilings] are a bed net for the whole house.” Some people do not use bed nets as they find them uncomfortable, and sleeping under them too hot and stuffy.14 Furthermore, getting in and out of bed during the night can result in nets being used inefficiently,17 and nets are often not used year round.10,18 These problems do not apply to house screening, although to truly compare bed nets and screening it would be necessary to examine how comfortable it is sleeping under a bed net in a full screened house, compared with a bed net alone or screening alone. Nevertheless, there was little negative feedback about the screening in terms of thermal comfort, ventilation, or air movement. While mean temperatures were significantly higher inside intervention houses compared with control houses, these differences (< 0.5°C) were not reported as a problem by most occupants. Full screening group participants who complained about the heat occupied houses which were, in fact, significantly hotter than other full screened houses. In these houses it seems plausible that the installation of screening raised the temperature more than 0.5°C, though we cannot make this comparison as indoor climate data was not recorded from houses before the screening was installed. This pattern was not replicated in the ceiling group, suggesting temperature differences were too slight in screened ceiling houses to be detected by users. This appears to be reflected in the preference data—in the ceiling group the numbers recognizing room temperature as a benefit or a problem (either “makes room too hot” or “keeps room cool”), was not significantly different between those who kept the ceilings and those who changed to full screening. In fact, in houses with sheet metal roofs the ceiling may have an insulating effect, reducing the amount of heat released by the roof into the room. This phenomenon was observed in houses that received papyrus reed mat ceilings in another intervention trial.19 These ceilings reduced evaporation by 2% to 5%, and made the houses cooler (−1.3°C) during the day and warmer (+0.8°C) during the night. Temperatures in our study houses with screened netting ceilings were less markedly different from control houses during the day or night, suggesting that the increased air flow through the mesh may help to maintain a more constant internal environment.
Advantageously, both bed nets and house screening are often appreciated in communities for reasons unrelated to mosquitoes or disease control. These benefits are similar, but generally less prevalent for bed nets compared with those recorded for house screening in this and other studies.19,20 For bed nets they include avoiding roof debris (9.4% of respondents), providing warmth at night (4.9%), privacy (1.5%), and decoration.14,21 Preventing dust, plus “fashion” (interpretable as “beautifies”) were two of the top five reasons given in Dar es Salaam for installing house screening,20 while in Western Kenya focus group discussions indicated that papyrus ceilings were cheap and considered to beautify houses.19
The full screened houses of the second year suffered less damage on average at 6 and 12 months than the first year group. This is probably the result of several factors: 1) separate community meetings were held, in year 2 but not year 1, to discuss screening damage and durability specifically. At these meetings leaflets were distributed describing how to take care of the screening (supplementary file 3); 2) the carpentry team had gained experience of installing the screening (the same team was maintained for both years); 3) improvements to the door design were made—push plates replaced handles that were easily broken, and push bars were added at child eye level (~60 cm from the ground) to prevent children from pushing directly on the netting to open the door; 4) one mason was responsible for the majority of the masonry work for second year study houses, whereas in the first year a separate mason from each village had been used. In contrast, there were no differences in damage to screened ceilings between the 2 years because nothing was done to control rats, the likely cause of the most damage in those houses.
Few FGD participants recalled being told to keep their doors and windows closed. This indicates that this message was delivered poorly, or that people did not like to close the doors, for personal reasons or reasons relating to thermal comfort (or both). In many houses it was observed that the elastic door pulls that were supposed to keep the door closed were still intact but had been detached from the door frames soon after the screening was installed (these were scored as “removed”). It was clear that most people only wanted to close their doors when someone was sleeping inside the house, regardless of the time of day. Full screening was efficacious despite so many doors being propped open during the day, although probably the screening could be even better if people could be persuaded to keep the doors closed at all times. However, because closing doors is considered discourteous to other community members and unwelcoming to visitors, convincing people to do this poses a challenge. The socially unacceptable practice of closing doors appears to have a stronger influence than the incentive of reducing mosquito house entry: several participants said that having their doors open in the day allows mosquitoes to enter the house and that as a result they still had to use their bed nets at night. The technology for screening doors is still in its infancy; other changes that would increase the longevity of the screened doors might include backing the fiberglass netting with a larger mesh metal wire panel, using more robust materials for the frames, and improving access to fenced-off back yards thus preventing domestic animals from passing directly through the house.
Because there were no obvious relationships between damage at 6 or 12 months and Anopheles mosquito numbers caught indoors has several explanations that would merit further study. First, in full screened houses it may be that the doors are not an important point of house entry, as has been suggested elsewhere.22 Second, the presence of holes in the screening will not be relevant to house entry if doors are open at night—we have only anecdotal evidence that they remain closed throughout the night. Neither of these explanations account for the lack of a relationship between damage and mosquitoes in screened ceiling houses. A third explanation, perhaps most plausible, is that insufficient damage has occurred to the screening after 12 months to reduce the efficacy of screening against mosquitoes. It is estimated by the researchers and the participants themselves that the screening could endure for 2 to 3 years. Some houses collapse or are deliberately knocked down each year (5% in this study), usually because of damage caused by flooding, and thatched roofs are replaced every 2–3 years. As a result we anticipate that with small improvements to the design, screening installed in a newly-constructed house would endure for the lifetime of that house in most cases.
Perhaps the most important issue raised by this research is that of user-ownership of health technologies. It has been suggested that technologies developed outside of Africa with little input from local partners missed an opportunity to engage decision makers in malarial regions to take responsibility for their own malaria management and control.23 House screening should encourage the active involvement of local craftsmen and end-users. All the materials could be secured locally, even in rural locations, whereas construction and installation can be done by carpenters, tailors, and masons who are members of the local community. The house occupants had almost complete control of their interaction with the intervention: how, and to what extent, they adapted their domestic environment, e.g., cleaning, redecorating, propping doors open, etc., was up to them. Because this is not just an issue of adherence to a treatment regimen or a matter of distribution, but of domestic praxis, the maintenance of screening is embedded in social relationships. As a consequence, we believe that house screening can be considered “culturally compelling”24 and as such may be more accepted, appreciated, and maintained than other types of intervention.
Supplementary Material
Acknowledgments
We thank the participants, the local communities, and their leaders for giving us their time to discuss their perspectives on our research. We thank all staff members of STOPMAL for their dedication to this project. We are also grateful to all the organizations that have supported this research: the Vestergaard-Frandsen group; Medical Council Laboratories in The Gambia; the joint Gambian Government/MRC Ethics Committee; Durham University and the London School of Hygiene and Tropical Medicine.
Note: Supplemental files are available at www.ajtmh.org.
Footnotes
Financial support: This study was funded by Medical Research Council, UK.
Authors' addresses: Matthew J. Kirby, Caroline O. H. Jones, and Steve W. Lindsay, Disease Control and Vector Biology Unit, Department of Infectious and Tropical Diseases, London School of Hygiene and Tropical Medicine, London, United Kingdom, E-mails: mattkirby.tanga@gmail.com, caroline.jones@lshtm.ac.uk, and steve.lindsay@lshtm.ac.uk. Pateh Bah, Basse Field Station, Medical Research Council (UK) The Gambia, Banjul, The Gambia, E-mail: pateh_bah1962@yahoo.com. Ann H. Kelly, Health Policy Unit, Faculty of Public Health and Policy, London School of Hygiene and Tropical Medicine, London, United Kingdom, E-mail: ann.kelly@lshtm.ac.uk. Momodou Jasseh, Medical Research Council (UK) The Gambia, Banjul, The Gambia, E-mail: mjasseh@mrc.gm.
References
- 1.Hanafin JB. Further results in mosquito proofing barracks. J R Army Med Corps. 1928;51:127–130. [Google Scholar]
- 2.Watson RB. In: Malariology: A Comprehensive Survey of all Aspects of this Group of Diseases from a Global Standpoint. Boyd MF, editor. Philadelphia, PA: W.B. Saunders; 1949. pp. 1184–1202. (Location and mosquito-proofing of dwellings). [Google Scholar]
- 3.Orenstein AJ. Screening as an antimalaria measure. A contribution to the study of the value of screened dwellings in malaria regions. Proc Canal Zone Med Assoc. 1912;5:12–18. [Google Scholar]
- 4.Lindsay SW, Emerson PM, Charlwood JD. Reducing malaria by mosquito-proofing houses. Trends Parasitol. 2002;18:510–514. doi: 10.1016/s1471-4922(02)02382-6. [DOI] [PubMed] [Google Scholar]
- 5.Kirby MJ, Milligan PJ, Conway D, Lindsay SW. Study protocol for a three-armed randomized controlled trial to assess whether house screening can reduce exposure to malaria vectors and reduce malaria transmission in The Gambia. Trials. 2008;9:33. doi: 10.1186/1745-6215-9-33. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Kirby MJ, Ameh D, Bottomley C, Green C, Jawara M, Milligan PJ, Snell PC, Conway DJ, Lindsay SW. Effect of two different house screening interventions on exposure to malaria vectors and on anaemia in children in The Gambia: a randomized controlled trial. Lancet. 2009;374:998–1009. doi: 10.1016/S0140-6736(09)60871-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Brabin BJ, Premji Z, Verhoeff F. An analysis of anemia and child mortality. J Nutr. 2001;131:636S–648S. doi: 10.1093/jn/131.2.636S. [DOI] [PubMed] [Google Scholar]
- 8.Snow RW, Azevedo IB, Lowe BS, Kabiru EW, Neville CG, Mwankusye S, Kassiga G, Marsh K, Teuscher T. Severe childhood malaria in two areas of different falciparum transmission in East Africa. Acta Trop. 1994;57:289–300. doi: 10.1016/0001-706x(94)90074-4. [DOI] [PubMed] [Google Scholar]
- 9.Jones C, Williams H. Social science in malaria control. Trends Parasitol. 2002;18:195–196. doi: 10.1016/s1471-4922(02)02272-9. [DOI] [PubMed] [Google Scholar]
- 10.Binka FN, Adongo PB. Acceptability and use of insecticide impregnated bednets in northern Ghana. Trop Med Int Health. 1997;2:499–507. [PubMed] [Google Scholar]
- 11.Kirby MJ, Green C, Milligan P, Sismanidis C, Jasseh M, Conway DJ, Lindsay SW. Risk factors for house-entry by malaria vectors in a rural town and satellite villages in The Gambia. Malar J. 2008;7:2. doi: 10.1186/1475-2875-7-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Dawson S, Gunsalam J, Khan N, McNee A. The application of qualitative research methods in the study of health seeking behaviour in relation to childhood acute respiratory infections, Bohol, The Philippines. Brisbane: Tropical Health Program, University of Queensland; 1991. pp. 1–67. [Google Scholar]
- 13.Gyapong M, Gyapong JO, Amankwa J, Asedam J, Sory E. Introducing insecticide-impregnated bednets in an area of low bednet usage: an exploratory study in the north-east Ghana. Trop Med Int Health. 1996;1:328–333. doi: 10.1046/j.1365-3156.1996.d01-41.x. [DOI] [PubMed] [Google Scholar]
- 14.Alaii JA, Van den Borne HW, Kachur SP, Mwenesi H, Vulule JM, Hawley WA, Meltzer MI, Nahlen BL, Phillips-Howard PA. Perceptions of bed nets and malaria prevention before and after a randomized controlled trial of permethrin-treated bed nets in western Kenya. Am J Trop Med Hyg. 2003;68:142–148. [PubMed] [Google Scholar]
- 15.D'Alessandro U, Aikins MK, Langerock P, Bennet S, Greenwood BM. Nationwide survey of bednet use in rural Gambia. Bull World Health Organ. 1994;72:391–394. [PMC free article] [PubMed] [Google Scholar]
- 16.Aikins MK, Fox-Rushby J, D'Alessandro U, Langerock P, Cham K, New L, Bennet S, Greenwood BM, Mills A. The Gambian national impregnated bednet programme: costs, consequences and net cost-effectiveness. Soc Sci Med. 1998;46:181–191. doi: 10.1016/s0277-9536(97)00145-7. [DOI] [PubMed] [Google Scholar]
- 17.Reilley B, Abeyasinghe R, Pakianathar MV. Barriers to prompt and effective treatment of malaria in northern Sri Lanka. Trop Med Int Health. 2002;7:744–749. doi: 10.1046/j.1365-3156.2002.00919.x. [DOI] [PubMed] [Google Scholar]
- 18.Okrah J, Traoré C, Palé A, Sommerfield J, Müller O. Community factors associated with malaria prevention by mosquito nets: an exploratory study in rural Burkina Faso. Trop Med Int Health. 2002;7:240–248. doi: 10.1046/j.1365-3156.2002.00856.x. [DOI] [PubMed] [Google Scholar]
- 19.Atieli H, Menya D, Githeko A, Scott T. House design modifications reduce indoor resting malaria vector densities in rice irrigation scheme area in western Kenya. Malar J. 2009;8:108. doi: 10.1186/1475-2875-8-108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Ogoma SB, Kannady K, Sikulu M, Chaki PP, Govella NJ, Mukabana WR, Killeen GF. Window screening, ceilings and closed eaves as sustainable ways to control malaria in Dar es Salaam, Tanzania. Malar J. 2009;8:221. doi: 10.1186/1475-2875-8-221. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.MacCormack CP, Snow RW. Gambian cultural preferences in the use of insecticide-impregnated bednets. J Trop Med Hyg. 1986;89:295–302. [PubMed] [Google Scholar]
- 22.Njie M, Dilger E, Lindsay SW, Kirby MJ. Importance of eaves to house-entry by anopheline, but not culicine, mosquitoes. J Med Entomol. 2009;46:505–510. doi: 10.1603/033.046.0314. [DOI] [PubMed] [Google Scholar]
- 23.Mshinda H, Killeen GF, Mukabana WR, Mathenge EM, Mboera LE, Knols BG. Development of genetically modified mosquitoes in Africa. Lancet Infect Dis. 2004;4:264–265. doi: 10.1016/S1473-3099(04)01000-X. [DOI] [PubMed] [Google Scholar]
- 24.Panter-Brick C, Clarke SE, Lomas H, Pinder M, Lindsay SW. Culturally compelling strategies for behaviour change: a social ecology model and case study in malaria prevention. Soc Sci Med. 2006;62:2810–2825. doi: 10.1016/j.socscimed.2005.10.009. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.