

Abstract
Two longitudinal studies examined the associations between interpersonal goals (i.e., self-image and compassionate goals) and anxiety and dysphoria (i.e., distress). In Study 1, 199 college freshmen (122 females, 77 males) completed 12 surveys over 12 weeks. Compassionate goals predicted decreased distress and self-image goals predicted increased distress from pretest to posttest when distress was assessed as anxiety, dysphoria, or a composite, and when the goals were worded as approach goals, avoidance goals or a composite. In Study 2, 115 first-semester roommate pairs (86 female and 29 male pairs) completed 12 surveys over 12 weeks. Compassionate and self-image goals predicted distress in same-week, lagged-week, and pretest-to-posttest analyses; effects of compassionate goals remained significant when we controlled for several known risk factors. Having clear goals consistently explained the association between compassionate goals but not self-image goals and distress. Results supported a path model in which compassionate goals predict increased support given to roommates, which predicts decreased distress. Results also supported a reciprocal association; chronic distress predicted decreased compassionate and increased self-image goals from pretest to posttest, and weekly distress predicted decreased compassionate goals the subsequent week. The results suggest that compassionate goals contribute to decreased distress because they provide meaning and increase support given to others. Distress, in turn, predicts change in goals, creating the potential for upward and downward spirals of goals and distress.
Keywords: anxiety, depression, goals, social support, compassion, self-image
Goals can make people happy or miserable. Goals give meaning and personal significance to events, and shape emotional responses to them (e.g., Frijda, 1988). Research from a variety of theoretical perspectives demonstrates that goals can influence emotional distress, including anxiety and dysphoria. Yet, the reverse may also be true; emotional distress may shape people’s goals. The possibility of reciprocal associations between goals and distress could contribute to upward and downward spirals of distress over time, and help explain the episodic nature of emotional distress. The present studies examine the influence of two interpersonal goals—compassionate and self-image goals--and distress over time and investigate why compassionate and self-image goals predict change in distress, exploring qualities of the goals themselves, and consequences of the goals for social support. They also examine whether chronic distress predicts change in interpersonal goals.
Goals and Well-Being
Empirical research supports the idea that goals can exacerbate or alleviate distress. Simply having clear goals or a sense of purpose strongly correlates with well-being in daily life (e.g., King, Hicks, Krull, & Del Gaiso, 2006). Progress toward goals elicits positive affect, whereas setbacks elicit negative affect (e.g., Carver, Lawrence, & Scheier, 1996; Carver & Scheier, 1990; Emmons, Kaiser, Martin, & Tesser, 1996; King, Richards, & Stemmerich, 1998). The direction of goals--whether people seek to approach or avoid an end state—and the regulatory focus people have while pursing goals—promotion or prevention--influence the type of positive or negative affect people experience when they make progress or experience setbacks toward their goals (e.g., Carver, 2003, 2004; Higgins, 1998; Higgins, Shah, & Friedman, 1997; Strauman, 2002). For approach or promotion-focused goals, progress elicits joy or elation, whereas setbacks elicit dejection or sadness. For avoidance or prevention-focused goals, progress elicits relief whereas setbacks elicit anxiety or fear.
Other researchers propose that the content of goals influences well-being. For example, self-determination theory posits that controlled motivation, such as seeking to obtain rewards and avoid punishments or avoid shame and guilt and obtain self-esteem boosts, creates goal-related pressure and undermines well-being, whereas autonomous motivation, such as pursuing personally important or intrinsically interesting goals, fosters well-being (for a review, see Deci & Ryan, 2000). Based on Dweck and Leggett’s distinction between learning and performance goals, Dykman (1998) proposed a distinction between validation-seeking, the motivation to establish or prove one’s basic worth, and growth-seeking, the motivation to improve or grow as a person. Validation seeking predicts increases and growth seeking predicts decreases in anxiety and dysphoria (Dykman, 1998). Kasser and Ryan (1993; 1996) proposed a distinction between intrinsic and extrinsic aspirations. They proposed that extrinsic goals such as money, fame, and popularity undermine well-being because they interfere with satisfaction of one’s own fundamental human needs for autonomy, relatedness, and competence, whereas intrinsic goals such as community, growth, and health foster well-being because they facilitate satisfaction of one’s own fundamental human needs (for a review, see Deci & Ryan, 2000).
Interpersonal Goals
We propose that another aspect of goals may contribute to or alleviate distress—their interpersonal quality. Interpersonal goals seek to “attain, maintain, or avoid a specific end state for the partner or the relationship” (Fitzsimons & Bargh, 2003 p. 150). We focus on two interpersonal goals that seem to reflect a core feature of human social life and psychological experience: the role of other people vis a vis the self. When people have a narrowly self-interested egosystem perspective, they prioritize their own needs and desires even at the expense of others. Other people are important if they could potentially satisfy or thwart one’s own needs and desires. In this perspective people have what Crocker and Canevello (2008) called self-image goals; they want others to view them in desired ways so others will help rather than hinder satisfaction of the needs and desires of the self (Crocker, 2008; Crocker, Olivier, & Nuer, 2009).
In contrast, when people have a broader ecosystem perspective, they give equal priority to the needs of others. Other people are important because, as in biological ecosystems, the well-being of one person indirectly influences the well-being of all. People with an ecosystem perspective have what Crocker and Canevello (2008) called compassionate goals; they want to be constructive and supportive, and not harm others because they care about others’ well-being (Canevello & Crocker, in press; Crocker, 2008; Crocker, et al., 2009). In theory, people can have an egosystem or an ecosystem perspective, and self-image or compassionate goals, for virtually any activity, from accumulating wealth to philanthropy, depending on whether they prioritize satisfaction of their own needs and desires over others’ or genuinely care about and want to support others’ well-being.
Research on compassionate and self-image goals shows that both can fluctuate from day to day or week to week and can change over time (Canevello & Crocker, in press; Crocker & Canevello, 2008). Research also supports the idea that when people have compassionate goals they have an ecosystem perspective on the relation between self and others, whereas when they have self-image goals they have an egosystem perspective (Crocker & Canevello, 2008). When people have compassionate goals they believe that people should take care of each other, and have a nonzero-sum view of success (i.e., one person’s success need not detract from others’ success). College students with compassionate goals report giving more support to their roommates; their roommates also report receiving more support from them (Crocker & Canevello, 2008). People with self-image goals believe that people should take care of themselves even at the expense of others, and view desired outcomes of the self and others as zero-sum, so one person’s success detracts from others’ (Crocker & Canevello, 2008). College students’ with self-image goals give less support to their roommates; self-image goals also undermine the effects of compassionate goals on roommates’ perceptions of support received. Furthermore, because people tend to reciprocate support, students with compassionate goals not only give more support; they also receive more support from their roommates (Crocker & Canevello, 2008).
Qualities of Interpersonal Goals and Change in Distress
Compassionate and self-image goals might predict change in distress for a variety of reasons: goal direction (approach vs. avoidance), goal clarity, goal progress and setbacks, or goal-related pressure. Self-image goals might be more avoidance or prevention focused (e.g, “Never let them see you sweat”), whereas compassionate goals might be more approach or promotion focused (e.g., “Do the right thing”). Although measures of compassionate and self-image goals were developed to include both approach and avoidance items (e.g., Crocker & Canevello, 2008), it is possible that the avoidance items account for the effects of self-image goals and the approach items account for effects of compassionate goals (e.g., Carver, 2003, 2004; Higgins, 1998; Higgins, et al., 1997; Strauman, 2002). Alternatively, compassionate and self-image goals might have similar effects regardless of whether they are approach-oriented or avoidance-oriented, if the benefits of trying to be supportive accrue even when that means avoiding harm to others (as in the dictum, “Do no harm”), and the costs of trying to get others to see the self in a desired light accrue even when that means approaching, rather than avoiding (as in “Dress to impress”). That is, the benefits of compassionate goals and costs of self-image goals for distress may outweigh the effects of framing goals in approach vs. avoidance or promotion vs. prevention terms.
Goal clarity might also contribute to associations of compassionate and self-image goals with distress. When people have compassionate goals they report that their most important academic and friendship goals make them feel clear, engaged, and peaceful, whereas when people have self-image goals they report that their most important academic and friendship goals make them feel confused, ambivalent/conflicted, and distracted (Crocker & Canevello, 2008). These feelings suggest that compassionate goals provide a clear sense of purpose, whereas self-image goals do not. In light of research demonstrating an association between having clear goals and well-being (King, et al., 2006), goal clarity might account for effects of compassionate and self-image goals on distress.
In addition, it might be easier to make progress toward compassionate goals than toward self-image goals, because supporting others does not depend on others’ response, whereas getting others to view the self in a positive light does. In light of research showing that goal progress elicits positive affect whereas goal setbacks elicit negative affect, progress and setbacks might account for effects of compassionate and self-image goals on distress (e.g., Carver, et al., 1996; Carver & Scheier, 1990; Emmons, et al., 1996; King, et al., 1998)
Finally, compassionate goals might be more autonomous, and self-image goals more controlled, accounting for their associations with distress. Controlled self-regulation (e.g., doing things because one has to or should do them) creates feelings of pressure, whereas autonomous self-regulation (e.g., doing things because one enjoys them or values them) does not (Deci & Ryan, 1987; Deci & Ryan, 2000; Ryan, 1982). Thus, goal-related pressure might account for effects of compassionate and self-image goals on distress.
Interpersonal Goals, Giving and Receiving Support, and Change in Distress
In addition to these goal qualities, we propose that interpersonal goals predict change in distress through their effects on relationship experiences. When people have compassionate goals they both give and receive more support; when people have self-image goals, they give and receive less support (Crocker & Canevello, 2008). These relationship consequences of interpersonal goals have implications for well-being and emotional distress. People with poor social relationships may experience several types of psychological distress, including dysphoria and anxiety (Alden & Taylor, 2004; Coyne, 1976; Davila & Beck, 2002; Joiner & Coyne, 1999; Joiner & Metalsky, 2001; Newman & Erickson, 2008).
Although interpersonal goals predict both giving and receiving support, we propose that compassionate goals reduce distress through their effects on giving support, independent of their effects on receiving support. The social support literature focuses almost exclusively on the support people receive or perceive is available to them. Yet, giving and receiving support are often confounded, because people who receive support tend to reciprocate. Research suggests that giving has benefits that may actually outweigh the benefits of receiving. For example, three studies, including a nationally representative survey, a longitudinal study of people who received financial windfalls, and an experiment, found that people who spend money on others are happier than people who spend money on themselves (Dunn, Aknin, & Norton, 2008).
Closer to the issue of support, a cross-sectional study found that people who report providing autonomy support to close friends (i.e., acknowledging the other’s perspective, providing choice, encouraging self-initiation, or being responsive) also report receiving autonomy support in return. Both giving and receiving autonomy support correlate with the giver’s well-being, but when entered together in analyses, giving, rather than receiving, autonomy support more strongly related to the giver’s well-being (Deci, La Guardia, Moller, Scheiner, & Ryan, 2006).
Longitudinal research also suggests that giving support has benefits for well-being independent of receiving support. Providing emotional support to a spouse uniquely predicted reduced risk of mortality for the helper over five years, independent of support received (S. L. Brown, Nesse, Vinokur, & Smith, 2003). Among bereaved participants who experienced high loss-related grief, helping behavior predicted an accelerated decline in depressive symptoms for the helper 6 to 18 months following loss, independent of support received (S. L. Brown, Brown, House, & Smith, 2008).
Based on these considerations, we hypothesize that compassionate goals predict increases in giving and receiving support, whereas self-image goals predict decreased giving and receiving support. Increases in giving support, in turn, may predict decreased distress, even controlling for support received.
Distress Predicts Goals
Most research on the association between goals and distress includes goals as the predictor and distress as the outcome. Yet, this association may go in both directions, at least for interpersonal goals, creating the possibility of upward or downward spirals of goals and distress. Although the possibility that distress predicts change in goals has received far less attention than the idea that goals contribute to distress, such an association seems plausible on theoretical grounds. Evolutionary explanations for anxiety and dysphoria suggest that negative mood may signal difficulties with current goals, and foster shifts to more attainable, self-protective, or less risky goals (Keller & Nesse, 2006; Nesse, 1991; Nesse & Ellsworth, 2009; Wrosch & Miller, 2009). Related to this view, anxiety or dysphoria may signal that self-regulatory resources are depleted (Baumeister & Vohs, 2007), or that one’s needs or desires are not currently being met or not likely to be met collaboratively with others as an ecosystem perspective suggests. Consequently, emotional distress may prompt a shift to an egosystem perspective, away from compassionate goals that prioritize others’ well-being, and toward self-image goals that prioritize getting others to meet one’s needs and desires through construction of desired self-images. Thus, we expect distress to predict decreased compassionate goals and increased self-image goals.
Overview
In sum, we hypothesize that compassionate goals predict reduced distress because when people have compassionate goals, the support they give and receive increases; giving support, in particular, should reduce distress. We also hypothesize that distress predicts decreased compassionate goals and increased self-image goals. In Study 1, we examined whether students’ chronic self-image and compassionate goals averaged across 10 weekly reports predict change in their symptoms of anxiety and dysphoria over the first semester of college. We also examined whether these effects depend on whether the goals are framed in approach or avoidance terms, building on previous evidence that failure at approach or promotion goals predicts dejection, whereas failure at avoidance goals predicts anxiety. In Study 2, we examined whether students’ compassionate and self-image goals for their roommate relationship predict change in anxiety and dysphoria from week to week as well as over a semester. We tested path models in which compassionate goals predict increased social support given to and received from roommates, which in turn predict change in distress. Study 2 also included other variables previously demonstrated to predict increased or decreased distress that might account for the effects of interpersonal goals, and attempted to identify the specific characteristic(s) of compassionate and self-image goals that account for their association with distress. Specifically, we examined whether having clear goals, making progress toward goals, setbacks toward goals, or feeling goal-related pressure could explain the effects of compassionate and self-image goals. We also tested whether distress predicts change in goals.
STUDY 1
Study 1 used the Goals and Adjustment to College Study data (Crocker & Canevello, 2008, Study 1) to test the hypothesis that students’ chronic compassionate and self-image goals predict changes in their own anxiety, dysphoria, and a distress composite. It also examined whether avoidance and approach versions of compassionate and self-image goals differentially predicted change in anxiety and dysphoria.
Method
Participants
First-semester college students were recruited within the first three weeks of the fall semester: 122 (61.3%) females and 77 (38.7%) males, with a mean age of 18.08 years. Of the original sample of 199, 194 (97.5%) completed all 12 surveys. For more information about the participants and procedures see Crocker and Canevello (2008, Study 1).
Procedure
Participants completed the pretest survey in person, and received instructions for completing the remaining 11 surveys online. After completing all surveys, participants were debriefed and paid for their participation.
Pretest and Posttest Measures
At pretest and posttest, participants completed measures of distress (i.e., anxiety and dysphoria). At pretest, they completed measures of socially desirable responding and demographics.
We assessed anxiety with the Speilberger Trait Anxiety Scale (Spielberger, Vagg, Barker, Donham, & Westberry, 1980), which had good internal consistency at pretest (α = .89) and posttest (α = .91). Dysphoria was measured with the Center for Epidemiological Studies Depression Inventory (CES-D; Radloff, 1997), which had high internal consistency (αpretest =.88; αposttest =.91). The two measures were highly correlated at pretest, r = .70 and posttest, r = .83. Consequently, we standardized scores on each measure and averaged the z-scores to create an index of distress.
Social desirability was assessed with the Marlowe-Crowne Social Desirability scale (Crowne & Marlowe, 1964), which assesses socially desirable responding in a 33-item forced-choice scale. The scale had adequate internal consistency (α = .77).
Weekly Measures
We assessed compassionate and self-image goals in each weekly survey with the measures developed by Crocker and Canevello (2008, Study 1). The compassionate goals scale included seven items: four worded as approach goals (e.g., “be constructive in your comments to others,”) and three worded as avoidance goals (e.g., “avoid doing anything that would be harmful to others”). The self-image goals scale included six items, two worded as approach goals (e.g., "get others to recognize or acknowledge your positive qualities,") and four worded as avoidance goals (e.g., "avoid showing your weaknesses”). Both scales had high internal consistency each week of the study (self-image goals: .77 < α < .89, Mα = .83; compassionate goals: .83 < α < .93, Mα = .90).
Results and Discussion
Table 1 presents the means and standard deviations for all variables by gender. Table 2 presents correlations among pretest, posttest, and chronic (averaged across the weekly reports) variables, and test-retest reliabilities for variables measured at both pretest and posttest. Because the goals were positively correlated, we entered them simultaneously into the regression equations. Neither gender nor social desirability predicted change in anxiety, dysphoria, or distress (all βs ≤ .10, all ps ≥ .147), so we trimmed these variables from regression analyses.1
Table 1.
Study 1 Means and Standard Deviations for Pretest, Posttest, and Averaged Weekly Variables for All Participants, and by Gender.
| M (SD) | Males | Females | p | |
|---|---|---|---|---|
| 1. Pretest Anxiety | 2.00 (.52) | 1.92 (.46) | 2.04 (.56) | .09 |
| 2. Posttest Anxiety | 2.11 (.55) | 2.08 (.51) | 2.12 (.57) | .56 |
| 3. Pretest Dysphoria | 15.29 (9.56) | 13.17 (7.82) | 16.63 (10.32) | .012 |
| 4. Posttest Dysphoria | 14.76 (9.60) | 14.18 (9.25) | 15.14 (9.83) | .497 |
| 5. Pretest Distress | 0 (.92) | −.19 (.79) | .12 (.98) | .02 |
| 6. Posttest Distress | 0 (.96) | −.06 (.89) | .04 (1.00) | .51 |
| 7. Chronic Self-image Goals | 3.00 (.63) | 2.93 (.62) | 3.05 (.63) | .21 |
| 8. Avoid Self-image Goals | 3.01 (.65) | 2.92 (.64) | 3.06 (.66) | .16 |
| 9. Approach Self-image Goals | 2.99 (.68) | 2.95 (.68) | 3.01 (.66) | .51 |
| 10. Chronic Compassionate Goals | 3.31 (.67) | 3.14 (.71) | 3.42 (.62) | .005 |
| 11. Avoid Compassionate Goals | 3.26 (.69) | 3.12 (.73) | 3.34 (.66) | .03 |
| 12. Approach Compassionate Goals | 3.35 (.68) | 3.16 (.72) | 3.45 (.64) | .001 |
| 13. Social Desirability | .45 (.16) | .45 (.18) | .46 (.15) | .63 |
Note: N = 199 at pretest (77 males, 122 females); N = 194 at posttest (75 males, 119 females).
Table 2.
Zero-Order Correlations among Chronic Compassionate and Self-image Goals, Social Desirability, and Distress at Pretest (Below Diagonal) and Posttest (Above Diagonal) and Test-Retest Reliabilities (on Diagonal) in Study 1.
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
|---|---|---|---|---|---|---|---|---|---|
| Anxiety | Dysphoria | Distress | Self-image goals | Avoidance self-image goals | Approach self-image goals | Compassionate goals | Avoidance compassionate goals | Approach compassionate goals | Social desirability |
| 1 .68*** | .83*** | .96*** | .15* | .18* | .05 | −.19** | −.15* | −.20** | −.24** |
| 2 .70*** | .57*** | .96*** | .13 | .15* | .07 | −.14* | −.13 | −.14* | −.14 |
| 3 .91*** | .92*** | .66*** | .15* | .17* | .07 | −.17* | −.15* | −.18* | −.20** |
| 4 .18** | .16* | .19** | -- | ||||||
| 5 .22** | .20** | .23*** | .98*** | -- | |||||
| 6 .07 | .04 | .06 | .89*** | .79*** | -- | ||||
| 7 −.04 | −.01 | −.030 | .536*** | .494*** | .558*** | -- | |||
| 8 −.02 | .02 | .001 | .529*** | .499*** | .522*** | .960*** | -- | ||
| 9 −.05 | −.05 | −.053 | .512*** | .463*** | .555*** | .977*** | .879*** | -- | |
| 10 −.30*** | −.24** | −.292*** | −.145* | −.152* | −.103 | .296*** | .314*** | .267** | -- |
Note: N = 199 at pretest, N = 194 at posttest;
p ≤ .001,
p ≤ .01,
p ≤ .05.
Social desirability was measured only at pretest; self-image and compassionate goals were assessed in 10 weekly reports, and averaged.
Table 3 presents standardized regression coefficients, ts, and ps for the effects of compassionate and self-image goals on residual change in anxiety, dysphoria, and the distress composite from pretest to posttest. Compassionate goals predicted decreased anxiety, dysphoria, and distress from pretest to posttest. Self-image goals predicted increased anxiety, dysphoria, and distress from pretest to posttest. We grand mean centered the goals to reduce multicollinearity, and entered the main effects and interaction term in the equation, testing the significance of the change in R2 when the interaction was entered as a predictor. When entered in the second block, the interaction between self-image and compassionate goals was not significant in any of the analyses (i.e., the change in R2 was not significant, all Δ R2 < .006, ns).
Table 3.
Standardized Regression Coefficients, ts, and ps for the Associations of (1) Compassionate and Self-image Goals, (2) Avoidance Compassionate and Self-image Goals, and (3) Approach Compassionate and Self-image goals with Residual Change in Distress from Pretest to Posttest in Study 1
| Anxiety | Dysphoria | Distress | |||||||
|---|---|---|---|---|---|---|---|---|---|
| β | t | p | β | t | p | β | t | p | |
| Composite Goals | |||||||||
| Compassionate Goals | −.27 | −4.40 | .000 | −.24 | −3.25 | .001 | −.25 | −3.98 | .000 |
| Self-image Goals | .18 | 2.93 | .004 | .18 | 2.39 | .018 | .17 | 2.58 | .011 |
| Avoidance Goals | |||||||||
| Compassionate Goals | −.26 | −4.36 | .000 | −.20 | −2.80 | .006 | −.22 | −3.61 | .000 |
| Self-image Goals | .17 | 2.78 | .006 | .14 | 1.98 | .049 | .14 | 2.18 | .031 |
| Approach Goals | |||||||||
| Compassionate Goals | −.26 | −4.18 | .000 | −.21 | −2.92 | .004 | −.24 | −3.74 | .000 |
| Self-image Goals | .15 | 2.44 | .016 | .16 | 2.16 | .032 | .15 | 2.37 | .019 |
We next tested whether the effects of compassionate and self-image goals on residual change in anxiety, dysphoria, and distress depended on whether the goals were expressed as approach or avoidance goals by creating two measures of each goal, one composed of approach items, and one composed of avoidance items. We entered the two approach goals in one set of analyses, and then entered the two avoidance goals in another set of analyses. As Table 3 indicates, both avoidance-oriented and approach-oriented compassionate goals predicted decreased anxiety, dysphoria, and the distress composite from pretest to posttest, whereas both avoidance-oriented and approach-oriented self-image goals predicted increased anxiety, dysphoria, and distress.
In sum, Study 1 shows that students’ chronic self-image and compassionate goals predict change in their levels of distress in the first semester of college. Compassionate goals predicted decreased distress over the semester, and self-image goals predicted increased distress, regardless of whether the outcome was anxiety, dysphoria, or a composite of anxiety and dysphoria. Furthermore, compassionate goals predicted decreased distress, and self-image goals predicted increased distress, regardless of whether the goals were worded as approach goals, avoidance goals or a composite of the two. Therefore, the associations between compassionate goals and self-image goals and change in distress cannot be explained by the distinction between approach and avoidance goals or promotion and prevention focus. People can have promotion-or prevention-focused compassionate goals for friendships; both predict decreased dysphoria and anxiety over the first semester of college. People can also have promotion- or prevention-focused self-image goals; both predict increased dysphoria and anxiety. The distinction between compassionate and self-image goals appears to be prepotent in this context. Consequently, for brevity, in Study 2 we examined the effects of composite goals on change in distress.
We did not include a measure of compassionate and self-image goals at pretest or posttest in Study 1, nor did we assessed anxiety and dysphoria weekly, preventing us from testing whether distress predicts change in goals. Accordingly, we address this issue in Study 2.
STUDY 2
Overview
Study 2 used the Goals and Roommate Mental Health Study data (see also Canevello & Crocker, under review) to test whether students’ compassionate and self-image goals for their roommate relationship predict change in distress and whether distress predicts change in goals. In Study 2 we included both members of roommate dyads. We examined the roles of giving support to roommates and receiving support from roommates in distress, and tested path models in which compassionate goals predict increased social support given to and received from roommates, which in turn predict change in distress.
In Study 2, we measured compassionate and self-image goals, distress, and support given to and received from roommates at pretest, posttest, and each week for 10 weeks, so we could examined the cumulative effects of chronic goals on change in distress over a semester, within-person associations between goals and distress on the same week, and lagged-week effects of goals one week on change in distress the following week. Finding that chronic goals predict change in distress from pretest to posttest or that goals one week predict change in distress the subsequent week would provide further evidence consistent with a causal effect of goals on distress. We also examined the plausibility of a causal association between distress and goals, testing whether chronic distress predicts change in goals from pretest to posttest, and whether distress one week predicts change in goals from that week to the next. Significant within-person same-week associations would show that within-person fluctuations in goals from week to week are associated with distress on those weeks.
Previous research has demonstrated that compassionate and self-image goals are empirically distinct from constructs such as responsiveness, relationship quality, disclosure, attachment styles, narcissism, and Big Five factors of personality (Canevello & Crocker, in press; Crocker & Canevello, 2008). Study 2 extended the results of Study 1 by including other variables previously demonstrated to predict increased or decreased distress that might account for the effects of interpersonal goals. At pretest, we included measures of individual differences in risk factors for distress that might be associated with both chronic interpersonal goals and change in distress over a semester, creating spurious associations between chronic goals and change in distress. Researchers have identified many cognitive and motivational variables that predict distress. We examined whether chronic interpersonal goals explain change in distress when we controlled for pretest differences in dysfunctional attitudes, validation-seeking, and growth-seeking. Dysfunctional attitudes are all-or-nothing or perfectionistic beliefs about the implications of achievement and others’ approval for self-worth (Weissman & Beck, 1978); they are associated with both anxiety and dysphoria (G. P. Brown, Hammen, Craske, & Wickens, 1995). Validation-seeking predicts increases in anxiety and dysphoria, whereas growth-seeking predicts decreases (Dykman, 1998).
We also included measures of risk factors more likely to change from week to week in the weekly surveys, including rumination, reflection, and reassurance-seeking. Rumination involves repeated, passive, self-focused thoughts about distress and its possible causes and consequences; rumination exacerbates anxiety and dysphoria, whereas reflection, a style of self-referential thought that involves intellectual curiosity about the self, does not consistently do so (see Nolen-Hoeksema, Wisco, & Lyubomirsky, 2008, for a review). Reassurance-seeking refers to the tendency to ask other people for affirmation of one’s worth; it predicts increases in both dysphoria and anxiety (Joiner, Katz, & Lew, 1999; Joiner & Metalsky, 2001). By including these measures in the weekly surveys we can examine whether these risk factors account for the effects of goals on distress in analyses of change from pretest to posttest, same-week associations, and lagged week associations.
Finally, in Study 2 we also attempted to identify the specific characteristic(s) of compassionate and self-image goals that account for their association with distress. We examined whether having clear goals, making progress toward goals, setbacks toward goals, or feeling goal-related pressure could explain the effects of compassionate and self-image goals. In the weekly surveys we included single-item assessments of the qualities of students’ goals, including having a clear goal, goal progress, goal setbacks, and goal-related feelings of pressure.
Method
Participants
One hundred fifteen same-sex first-semester freshman roommate dyads who did not know each other prior to college volunteered for a study of goals and roommate relationships during the fall semester. Via advertisements in the campus newspaper and flyers, we offered each roommate $60 for completing 12 surveys over 12 weeks ($10 for each the pretest and posttest and $4 for each weekly survey) plus a $40 bonus for completing all 12 surveys. One hundred nine pairs (95%) completed the pretest, posttest, and at least 8 weekly surveys. Although 6 pairs completed fewer parts of the study, we retained all data for analyses where possible. Eighty-six pairs (75%) were female. Participants ranged in age from 18 to 21 years (M = 18.1 years, SD = .36).
Procedure
In groups of 1 to 8, roommate pairs attended a 1.5 hr session to learn about the study, give their informed consent, complete the pretest survey, and receive instructions for completing the remaining 11 surveys online. The weekly surveys took about 30 min to complete and roommates were required to complete weekly surveys within 48 hours of each other. To retain as many participants as possible in the study, participants had up to 11 weeks to complete the 10 weekly surveys. Once roommates had completed 10 weekly surveys, they completed the posttest survey and were paid for their participation.
Measures
At pretest, posttest, and in each weekly survey, participants completed measures of anxiety and dysphoria, compassionate and self-image goals, and support given to and received from roommates. At pretest, participants completed measures of dysfunctional attitudes, validation-seeking, and growth-seeking. In each weekly survey, participants completed measures of rumination, reflection, reassurance seeking, having clear goals, goal progress, goal setbacks, and goal-related feelings of pressure. The pretest survey also included demographic questions (gender, race/ethnicity, age, parental income).
Distress
As in Study 1, we assessed both anxiety and dysphoria. Anxiety was assessed with the Speilberger State Anxiety Scale (Spielberger, et al., 1980). At pretest and posttest, participants rated their anxiety in general on a scale ranging from 1 (never) to 5 (always); in the weekly surveys, they rated their anxiety over the past week on the same scale. Anxiety had high internal consistency at pretest (α =.91), posttest (α =.94), and in each of the weekly surveys (.94 ≤ α ≤ .95, Mα = .94). Dysphoria was assessed with the CES-D as in Study 1. The CES-D had high internal consistency at pretest (α =.86), posttest (α =.89) and each of the weekly surveys (.90 ≤ α ≤ .92, Mα = .91). Anxiety and dysphoria were highly correlated at pretest (r = .63) and posttest (r = .64). Separate analyses for each outcome yielded similar results, so for brevity, we created a composite distress index and conducted analyses on this index.
Self-image and compassionate goals for roommate relationships were measured with a modified version of the measure of self-image and compassionate goals used by Crocker and Canevello (2008, Study 2). Pretest and posttest items began with the phrase, “In my relationship with my roommate, I want/try to." Weekly items began with “This week, in my relationship with my roommate, I wanted/tried to.” All items were rated on a scale ranging from 1 (not at all) to 5 (extremely). Eight items assessed compassionate goals: (e.g., "have compassion for my roommate’s mistakes and weaknesses;" "avoid being selfish or self-centered"). Six items assessed self-image goals (e.g., "convince my roommate that I am right," "avoid showing my weaknesses"). As in Study 1, approach and avoidance compassionate goals were highly correlated (r = .89), as were approach and avoidance self-image goals (r = .70). Consequently, we created composite measures of compassionate goals and self-image goals by averaging across the approach and avoidance items for each scale. Both scales were internally consistent at pretest (self-image α = .79; compassionate α = .75), posttest (self-image α = .87; compassionate α = .94), and in each weekly survey (self-image goals: .83 ≤ α ≤ .91, Mα = .88; compassionate goals: .85 ≤ α ≤ .94, Mα = .91).
Social support given to and received from roommates was measured with a modified version of the Multidimensional Survey of Perceived Social Support (Zimet, Powell, & Farley, 1990). Participants rated their agreement on a scale ranging from 1 (strongly disagree) to 5 (strongly agree) with four items assessing social support received from their roommates. At pretest and posttest the items were worded generally (“My roommate really tries to help me,” “I can count on my roommate if things go wrong,” “I can share my joys and sorrows with my roommate,” and “I can talk about my problems with my roommate”). In the weekly surveys supportiveness was rated over the past week (e.g., “This week, I felt that my roommate really tried to help me”). Parallel items assessed how much support participants gave to their roommates. The measure of support received had high internal consistency at pretest (α = .93), posttest (α = .96), and in each weekly survey (.86 ≤ α ≤ .96, Mα = .94). The measure of support given also had high internal consistency at pretest (α = .92), posttest (α = .95), and in each weekly survey (.93 ≤ α ≤ .97, Mα = .96).
Pretest Covariates
The Dysfunctional Attitudes Scale (DAS), included in the pretest survey, assesses cognitive vulnerability to dysphoria (Weissman & Beck, 1978), specifically perfectionistic beliefs about achievement (e.g., “If I fail partly, it is as bad as being a complete failure,”) and others’ approval (e.g, “I cannot be happy unless most people I know admire me.”) (G. P. Brown, et al., 1995). The DAS had high internal consistency (α = .89) in the present study.
We assessed validation-seeking and growth-seeking using an abbreviated 10-item version of the Goal Orientation Inventory (Dykman, 1998) at pretest. These abbreviated subscales had good internal consistency in the present study for validation seeking (α = .82) and growth seeking (α = .83).
Weekly Covariates
Rumination and reflection were assessed in the weekly questionnaires with the Rumination-Reflection Questionnaire (Trapnell & Campbell, 1999), which includes a rumination scale assessing recurrent thinking about the self prompted by threats, losses, or injustices to the self (e.g., “I tended to “ruminate” or dwell over things that happen to me for a really long time afterward”), and a reflection scale assessing self-attentive thinking motivated by intrinsic interest in abstract or philosophical thinking (e.g., “I love exploring my “inner” self). Participants rated their agreement with each item in general (at pretest and posttest) or in the past week on a scale ranging from 1 (strongly disagree) to 5 (strongly agree). Rumination correlates with both dysphoria and anxiety; reflection does not (Trapnell & Campbell, 1999). Internal consistency was high in the present study for rumination (.90 ≤ α ≤ .90, Mα = .93) and reflection (.89 ≤ α ≤ .93, Mα = .91).
Reassurance-seeking was assessed in the weekly surveys with the 4-item Reassurance-Seeking Scale (Joiner & Metalsky, 2001), which predicts increases in both dysphoria and anxiety (Joiner, et al., 1999; Joiner & Metalsky, 2001). Participants rated how often they sought reassurance from their roommate in the past week (e.g., “Over the past week did you find yourself often asking your roommate how he/she truly feels about you?”) on scales ranging from 1 (never) to 5 (always). Internal consistency was high in the present study (.82 ≤ α ≤ .95, Mα = .92).
Goal characteristics
Four single-item measures assessed characteristics of goals that might account for the effects of compassionate and self-image goals on distress: having clear goals (“In the past week, I had very clear goals and aims in life.”), goal progress and setbacks (“How much progress did you make in the past week toward achieving your relationship goals with your roommate?” and “How much did you experience setbacks in the past week toward achieving your goals for your relationship with your roommate?”), and goal-related pressure (“To what extent does your main goal for your relationship with your roommate make you feel pressured?”).
Results
Overview of analyses
Analyses addressed the following questions: (1) Do compassionate and self-image goals predict change in distress (replicating Study 1)? (2) Do known risk factors for distress account for those associations? (3) Do other characteristics of goals including having clear goals and aims, progress and setbacks toward goals, or goal-related pressure account for associations between goals and distress? (4) Do goals predict distress through social support received from or given to roommates? and (5) Does distress predict change in goals? We addressed these questions by examining the effect of chronic goals (averaged across the weekly reports) on change in distress over the semester, and the lagged effect of goals one week on change in distress the next week.2
General analytic strategy
In these data, individuals were nested within dyads and dyads were crossed with weeks (Kashy, Donnellan, Burt, & McGue, 2008). Thus, we controlled for the non independence of individuals within dyads in all analyses using the MIXED command in SPSS (Campbell & Kashy, 2002; Campbell, Simpson, Boldry, & Kashy, 2005; Kenny, Kashy, & Cook, 2006), and because individuals within dyads were indistinguishable, we specified compound symmetry so that intercept variances between dyad members were equal. Coefficients for weekly and lagged-week analyses were derived from random-coefficients models using restricted maximum-likelihood estimation, and models included fixed and random effects for the intercept and each predictor (all weekly and lagged-week predictors were level-1 variables). Coefficients for testing change from pretest to posttest were derived from fixed-effects models using restricted maximum-likelihood estimation. We used a residual change strategy to test changes from week to week and pretest to posttest, regressing the Time N + 1 dependent variable on relevant Time N predictors, controlling for the Time N dependent variable. When change in a variable was a predictor, we entered the Time N and Time N + 1 predictors into the model and interpreted the Time N + 1 variable. In same-week analyses we person-centered all predictors to test the effect of fluctuations around each individual’s own average score. We grand mean centered predictors in lagged-week and pretest and posttest analyses to examine how levels of the predictors relative to the sample mean predicted residual change in outcomes the following week, or at posttest. We person-centered predictors in same-week analyses to examine how levels of a person’s predictors relative to their own mean level predicted that week’s outcomes.3
Path models were tested sequentially, with a separate regression equation for each path. For each path, we regressed the criterion on the predictor(s), controlling for all variables preceding that path in the model. Lagged analyses were conducted on all 10 weeks. For simplicity, we refer to Week N as “Week 1” and Week N+1 as “Week 2.” Partial correlations were calculated using the method described by Rosenthal and Rosnow (1991).
Table 4 shows the means and standard deviations overall and by gender for all primary pretest, posttest, and averaged weekly variables. Table 5 shows the within-person intraclass correlations, which adjust for the degree of non independence between dyad members (Griffin and Gonzalez, 1995). Because compassionate and self-image goals were significantly correlated, we regressed all outcome variables on compassionate and self-image goals simultaneously when applicable. Roommate’s goals did not predict students’ distress, support given or received, or other covariates in any analyses (all ps > .10). Although both gender and social desirability correlated with compassionate goals, neither gender nor social desirability predicted change in distress, or social support given or received in any analyses. Accordingly, we trimmed these variables from the regression analyses predicting change in outcomes.
Table 4.
Study 2 Means and Standard Deviations for Pretest, Posttest, and Averaged Weekly Variables for All Participants, and by Gender.
| M (SD) | Males | Females | p | |
|---|---|---|---|---|
| 1. Pretest Distress | .00 (.90) | .01 (.91) | −.00 (.91) | .908 |
| 2. Pretest Self-image Goals | 2.54 (.69) | 2.87 (.68) | 2.42 (.65) | .001 |
| 3. Pretest Compassionate Goals | 4.11 (.47) | 3.91 (.42) | 4.17 (.46) | .001 |
| 4. Pretest Support Given | 4.23 (.72) | 3.97 (.46) | 4.17 (.46) | .001 |
| 5. Pretest Support Received | 4.02 (.86) | 3.71 (.82) | 4.12 (.85) | .001 |
| 6. Pretest Dysfunctional Attitudes | 2.43 (.42) | 2.52 (.41) | 2.40 (.41) | .839 |
| 7. Pretest Validation Seeking | 3.05 (.81) | 3.22 (.71) | 2.99 (.84) | .141 |
| 8. Pretest Growth Seeking | 3.47 (.72) | 3.35 (.72) | 3.55 (.71) | .988 |
| 9. Posttest Distress | .00 (.91) | .05 (.94) | −.02 (.90) | .654 |
| 10. Posttest Self-image Goals | 2.35 (.76) | 2.47 (.73) | 2.31 (.78) | .200 |
| 11. Posttest Compassionate Goals | 3.92 (.81) | 3.74 (.78) | 3.95 (.82) | .108 |
| 12. Posttest Support Given | 4.11 (.83) | 3.94 (.83) | 4.17 (.83) | .093 |
| 13. Posttest Support Received | 3.97 (1.00) | 3.83 (.93) | 4.01 (1.02) | .261 |
| 14. Chronic Distress | .00 (.95) | .01 (.96) | −.01 (.95) | .898 |
| 15. Chronic Self-image Goals | 2.38 (.67) | 2.55 (.62) | 2.31 (.68) | .019 |
| 16. Chronic Compassionate Goals | 3.75 (.87) | 3.66 (.57) | 3.98 (.60) | .001 |
| 17. Chronic Rumination | 1.77 (.60) | 1.63 (.56) | 1.81 (.60) | .421 |
| 18. Chronic Reflection | 2.05 (.74) | 1.83 (.61) | 2.12 (.76) | .056 |
| 19. Chronic Reassurance Seeking | 1.11 (.26) | 1.10 (.24) | 1.11 (.25) | .527 |
| 20. Chronic Have Clear Goals | 3.51 (.86) | 3.57 (.88) | 3.45 (.86) | .394 |
| 21. Chronic Goal Progress | 3.50 (.68) | 3.35 (.67) | 3.54 (.68) | .776 |
| 22. Chronic Goal Setbacks | 1.79 (.60) | 1.71 (.52) | 1.83 (.62) | .062 |
| 23. Chronic Goal-Related Pressure | 1.59 (.60) | 1.67 (.66) | 1.57 (.58) | .263 |
Note: N = 230 (172 females, 58 males) at pretest and for chronic variables; N = 218 (166 females, 52 males) at posttest .
Table 5.
Intrapersonal Correlations for All Primary Variables in Study 2 at Pretest (Below Diagonal) and Posttest (Above Diagonal) and Test-Retest Reliabilities (on Diagonal).
| 1. | 2. | 3. | 4. | 5. | 6. | 7. | 8. |
|---|---|---|---|---|---|---|---|
| Distress | Self-image Goals | Compassionate Goals | Support Given | Support Received | Chronic Distress | Chronic Self-image | Chronic Compassionate |
| 1. .640 | .337 | −.316 | −.389 | −.343 | .830 | .326 | −.255 |
| 2. .268 | .535 | −.139 | −.218 | −.240 | .342 | .881 | −.235 |
| 3. −.227 | −.225 | .484 | .770 | .618 | −.287 | −.217 | .680 |
| 4. −.206 | −.277 | .446 | .386 | .744 | −.315 | −.250 | .453 |
| 5. −.270 | −.258 | .479 | .523 | .385 | −.337 | −.213 | .465 |
| 6. .766 | .241 | −.120 | −.179 | −.186 | -- | .371 | −.298 |
| 7. .330 | .670 | −.148 | −.197 | −.158 | .371 | -- | −.236 |
| 8. −.225 | −.235 | .680 | .453 | .465 | −.298 | −.236 | -- |
Note. N = 230 at pretest and for chronic variables; N = 218 at posttest. Chronic variables were calculated by averaging across the 10 weekly reports. Distress was standardized. All other variables were measured on scales ranging from 1 (strongly disagree/never/not at all) to 5 (strongly agree/always/extremely). p < .05 when |.14| ≤ r ≤ |.17|; p < .01 when |.18| ≤ r ≤ |.20|; p < .001 when r > |.21|.
Goals Predicting Change in Distress from Pretest to Posttest
As in Study 1, we hypothesized that chronic goals (averaged across the 10 weekly reports) predict residual change in distress.
Compassionate goals predict decreased distress
As Table 6 shows, chronic compassionate goals predicted decreased distress from pretest to posttest, replicating Study 1. Chronic compassionate goals significantly predicted decreased distress when we controlled for pretest dysfunctional attitudes, validation-seeking, or growth-seeking, indicating that pre-existing levels of these risk factors did not account for associations between chronic goals and change in distress. Compassionate goals predicted decreased distress when we controlled for chronic rumination, reflection, or reassurance-seeking measured in the weekly surveys, indicating that contemporaneous levels of these risk factors did not account for the association between chronic goals and distress; rumination and reflection significantly and reassurance-seeking marginally predicted increased distress independent of chronic compassionate and self-image goals (see Table 6).
Table 6.
Partial Correlations and ps for the Associations between Chronic Compassionate and Self-image Goals and Residual Change in Distress from Pretest to Posttest Controlling for Covariates Assessed in Study 2.
| Covariate | Compassionate Goals | Self-image Goals | Covariate | |||
|---|---|---|---|---|---|---|
| pr | p | pr | p | pr | p | |
| None | −.20 | .004 | .13 | .054 | ||
| Pretest Covariates | ||||||
| Dysfunctional Attitudes | −.20 | .004 | .11 | .098 | .03 | .682 |
| Growth Seeking | −.19 | .004 | .13 | .052 | −.09 | .212 |
| Validation Seeking | −.20 | .003 | .11 | .106 | .07 | .342 |
| Chronic Weekly Covariates | ||||||
| Rumination | −.21 | .003 | .11 | .099 | .23 | .001 |
| Reflection | −.22 | .001 | .12 | .070 | .17 | .013 |
| Reassurance Seeking | −.18 | .010 | .11 | .096 | .11 | .098 |
| Have Clear Goals | −.13 | .055 | .18 | .011 | −.18 | .008 |
| Goal Progress | −.16 | .021 | .12 | .079 | −.12 | .080 |
| Goal Setbacks | −.20 | .004 | .11 | .113 | .13 | .062 |
| Pressured | −.20 | .005 | .06 | .350 | .22 | .001 |
Note. N = 218 at posttest. Goals were entered simultaneously. Each covariate was entered in a separate regression equation.
Of the four goal characteristics assessed in the weekly surveys (have a clear goal, progress, setbacks, and pressure), only when we included having clear goals as a covariate did the effect of compassionate goals drop to marginal significance, although all of the goal characteristics significantly or marginally predicted change in distress in the expected direction, independent of compassionate and self-image goals. Thus, with the exception of having clear goals, none of the risk factors or goal characteristics accounted for the effect of chronic compassionate goals on change in distress.
Self-image goals marginally predict increased distress
Self-image goals marginally predicted increased distress even when we controlled for dysfunctional attitudes, growth-seeking, or validation-seeking assessed at pretest, and when we controlled for chronic weekly rumination, reflection, or reassurance-seeking (see Table 6). Self-image goals significantly predicted increased distress when we controlled for goal clarity, and did not predict change in distress when we controlled for goal-related pressure, indicating that feeling pressured may account for the marginally significant effect of self-image goals on change in distress.
Goals predict change in support given and received
Compassionate goals predicted increases in both support given (pr = .59, p < .001) and support received (pr = .42, p < .001) from pretest to posttest; self-image goals predicted decreases in support given (pr = −.16, p = .027), but not support received (pr = −.11, p = .13).
We tested a path model in which the effect of chronic compassionate and self-image goals on residual change in distress goes through change in support given and received. We controlled for reciprocity of support by including change in support given as a predictor of change in support received, and vice versa. As Figure 1 shows, chronic compassionate goals predicted increased support given to roommates, controlling for change in support received, but did not predict increased support received, controlling for change in support given. Controlling for chronic compassionate and self-image goals, residual change in support given predicted decreased distress, and the effect of compassionate goals on change in distress was reduced to nonsignificance. Chronic self-image goals did not predict residual change in either support given or support received. Furthermore, residual change in support received did not predict change in distress, controlling for change in support given. These results indicate that giving rather than receiving support accounts for the effect of compassionate goals on reduced distress.
Figure 1.
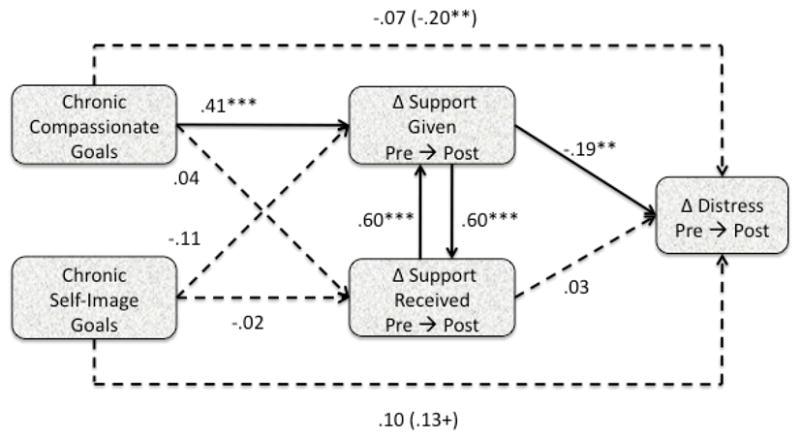
Partial Correlations for Path Model of Effects of Chronic Compassionate and Self-image Goals (Averaged across Weekly Reports) on Residual Change in Distress through Residual Change in Support Given and Received from Pretest to Posttest in Study 2.
Both chronically having clear goals and change in support given accounted for the effect of compassionate goals on change in distress when entered in separate regression equations. To examine whether they accounted for the same part of change in distress, we entered them together with chronic compassionate and self-image goals and residual change in support received as predictors of change in distress from pretest to posttest. Change in support given (pr = −.21, p = .002) and chronically having clear goals (pr = −.20, p = .003) predicted change in distress when entered together; neither change in support received (pr = .04, p = .603) nor compassionate goals (pr = .01, p = .892) predicted change in distress, but self-image goals did (pr = .15, p = .026). Thus, having clear goals and change in support given account for unique variance in change in distress.
Goals Predict Same Week Distress
Fluctuations in students’ compassionate and self-image goals relative to their own averages predicted their distress the same week, supporting the idea that distress varies as students’ compassionate and self-image goals vary (see Table 7). The same-week association between compassionate goals and distress remained significant when we controlled for same-week rumination, reflection, reassurance seeking, goal progress, goal setbacks, or goal-related pressure. Only controlling for having clear goals reduced the effect of compassionate goals to marginal significance. The effect of self-image goals remained significant in all analyses that included same-week covariates. Rumination and reflection positively and having a clear goal negatively related to same-week distress with compassionate and self-image goals controlled, indicating that they relate to that part of distress that is unrelated to compassionate and self-image goals.
Table 7.
Partial Correlations and ps for Analyses with Person-Centered Goals and Covariates One Week as Predictors of Distress the Same Week.
| Covariate | Compassionate Goals | Self-image Goals | Covariate | |||
|---|---|---|---|---|---|---|
| pr | p | pr | p | pr | p | |
| None | −.14 | .001 | .09 | .037 | ||
| Rumination | −.18 | .001 | .10 | .036 | .51 | .001 |
| Reflection | −.19 | .001 | .10 | .052 | .51 | .001 |
| Reassurance Seeking | −.12 | .002 | .08 | .04 | .06 | .125 |
| Have Clear Goals | −.06 | .080 | .09 | .013 | −.19 | .001 |
| Goal Progress | −.10 | .004 | .07 | .037 | −.05 | .342 |
| Goal Setbacks | −.10 | .003 | .08 | .018 | .06 | .246 |
| Pressured | −.11 | .003 | .08 | .033 | .06 | .200 |
Compassionate goals positively related to both support given (pr = .34, p < .001) and support received (pr = .32, p < .001) the same week. Self-image goals negatively related to support given (pr = −.09, p = .031) and received (pr = −.10, p = .019). When we entered support given and received together with compassionate and self-image goals as predictors of same-week distress, compassionate goals still related to decreased distress, pr = −.07, p = .018, and self-image goals marginally related to increased distress, pr = .06, p = .071, but neither support given, pr = −.05, p = .166, nor support received, pr = −.02, p = .58, related to distress that week. Thus, neither support given nor support received accounted for the same-week association between goals and distress. We did not test a path model because same-week associations do not address the plausibility of causal pathways over time.
Weekly Goals Predict Change in Distress the Following Week
Lagged-week analyses examined whether goals one week predict change in distress the following week. Examination of the temporal sequence of effects across weeks does not demonstrate causality but can shed light on the plausibility or implausibility of causal pathways (Kenny, 1975; Rogosa, 1980; West, Biesanz, & Pitts, 2000). We grand mean centered predictors, so regression coefficients represent the effects of students’ Week 1 goals relative to the sample mean on change in the outcome from Week 1 to Week 2.
As Table 8 shows, Week 1 compassionate goals marginally predicted decreased Week 2 distress and Week 1 self-image goals predicted increased Week 2 distress, consistent with causal paths from self-image goals one week to increased distress and from compassionate goals one week to decreased distress the following week. These effects remained when we controlled for Week 1 risk factors (rumination, reflection, or reassurance-seeking), and Week 1 goal progress, goal setbacks, or goal-related pressure. The effect of compassionate goals was reduced from pr = −.13 to pr = −.08 when we controlled for having a clear goal on Week 1, and Week 1 having a clear goal marginally predicted change in distress the next week.
Table 8.
Partial Correlations and ps for Analyses with Distress, Goals, and Covariates One Week as Predictors of Distress the Following Week.
| Covariate | Compassionate Goals | Self-image Goals | Covariate | |||
|---|---|---|---|---|---|---|
| pr | p | pr | p | pr | p | |
| None | −.13 | .066 | .17 | .019 | ||
| Rumination | −.13 | .053 | .17 | .012 | .04 | .515 |
| Reflection | −.13 | .047 | .17 | .011 | .00 | .951 |
| Reassurance Seeking | −.11 | .092 | .15 | .025 | .08 | .183 |
| Have Clear Goals | −.08 | .165 | .18 | .004 | −.12 | .089 |
| Goal Progress | −.10 | .068 | .13 | .022 | −.04 | .593 |
| Goal Setbacks | −.11 | .074 | .14 | .009 | .01 | .918 |
| Pressured | −.12 | .055 | .14 | .029 | .07 | .296 |
Week 1 compassionate goals predicted increased Week 2 support given and received. Self-image goals predicted decreases in support given but not support received. We tested the path from Week 1 compassionate and self-image goals to Week 2 distress through change in support given and received from Week 1 to Week 2 (see Figure 2). As in pretest-posttest analyses, we controlled for reciprocity of support by including paths from change in support given to change in support received, and vice versa. The full model did not converge, so we set week one support given and received as fixed; the model then converged.
Figure 2.
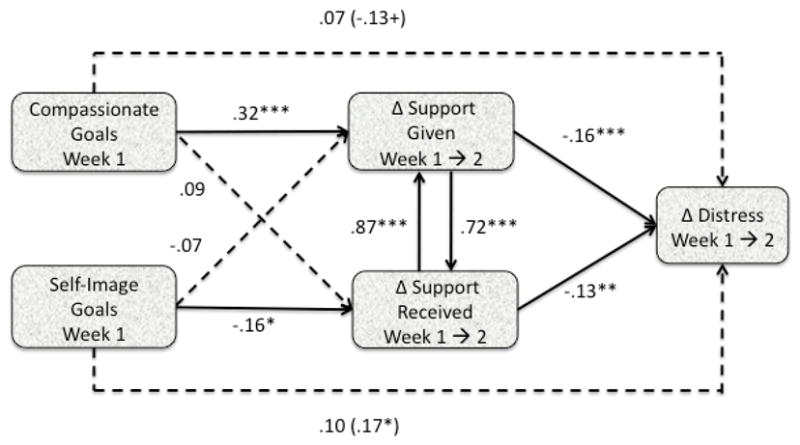
Partial Correlations for Path Model of Effects of Compassionate and Self-image Goals One Week on Residual Change in Distress the Subsequent Week through Residual Change in Support Given and Received in Study 2.
Controlling for change in support received, Week 1 compassionate goals predicted increased support given on Week 2; self-image goals did not. Controlling for change in support given, Week 1 compassionate goals did not predict increased support received on Week 2; self-image goals predicted decreased support received. Controlling for both goals, increased support given and received predicted decreased distress. Thus, the lagged week analyses suggest a path from compassionate goals through increased support given and from self-image goals through decreased support received to change in distress the following week.
Because both Week 1 goal clarity and increased support given and received from Week 1 to Week 2 predicted decreased Week 2 distress (controlling for Week 1 distress), we entered them together as predictors to test whether they account for unique variance in change in distress. Change in support given (pr = −.14, p = .005), and change in support received (pr = −.12, p = .002), predicted change in distress; having a clear goal on Week 1 still marginally predicted decreased distress (pr = −.11, p = .062). Thus, having clear goals on Week 1 marginally predicted that part of decreased Week 2 distress that was unrelated to Week 1 compassionate and self-image goals or change in support given and received from Week 1 to Week 2.
Distress Predicts Change in Goals
We hypothesized that when people feel distressed, they have decreased compassionate and increased self-image goals. We tested this effect in pretest-posttest and lagged week analyses, using the same analytic approach described previously.
Chronic distress (averaged across the 10 weekly reports) predicted decreased compassionate goals (pr = −.26, p < .001) and increased self-image goals (pr = .27, p < .001) from pretest to posttest. In lagged week analyses, weekly distress predicted decreased compassionate goals the following week, pr = −.20, p = .015, but not change in self-image goals, pr = .12, p = .11.
Discussion
Study 2 addressed five questions: (1) Do compassionate and self-image goals predict change in distress, replicating Study 1? (2) Do known risk factors for distress account for those associations? (3) Do other characteristics of goals including having clear goals and aims, progress and setbacks toward goals, or goal-related pressure account for associations between goals and distress? (4) Do goals predict distress through social support received from or given to roommates? and (5) Does distress predict change in goals? We examined these issues across three time frames: change from pretest to posttest, associations the same week, and lagged week associations.
Do compassionate and self-image goals predict change in distress?
The results of Study 2 support our hypothesis that compassionate and self-image goals predict change in distress, consistent with Study 1. Chronic compassionate goals predicted decreased distress from pretest to posttest, within the same week, and on the subsequent week, although the lagged week effect was only marginally significant. Self-image goals predicted increased distress from pretest to posttest (although this effect was only marginally significant), within the same week, and on the subsequent week.
The findings indicate that compassionate and self-image goals relate to distress when assessed as chronic goals, as departures from participants’ average levels of the goals (same-week analyses), or as predictors of distress the next week, controlling for current week distress. These three types of analyses each provide unique information about the association between interpersonal goals and distress. The pretest to posttest analyses indicate that chronic compassionate and self-image goals predict change in distress, consistent with a causal effect of individual differences in goals on change in distress over 12 weeks. The lagged week analyses indicate that the goals people have one week, due either to individual differences in chronic goals or fluctuations in goals from week to week, predict change in distress the following week, consistent with a causal effect of weekly goals on distress over a much shorter time frame. The same-week analyses show that within-person fluctuations in weekly goals around people’s own typical levels predict how distressed they are that week, ruling out the possibility that the associations of goals with distress are solely due to stable characteristics of participants, such as gender, social desirability, or stable personality traits, because we removed individual differences in chronic goals through person-centering. These analyses suggest that interventions to alter people’s goals might change their levels of distress currently, one week later, or and 12 weeks later.
Do known risk factors for distress account for associations between goals and distress?
None of the known risk factors assessed at pretest or in the weekly measures explained the associations between compassionate and self-image goals and distress in the pretest to posttest, same-week, or lagged week analyses. However, chronic rumination and reflection predicted increased distress from pretest to posttest, and weekly rumination and reflection predicted same week distress, with goals controlled. These results indicate that compassionate and self-image goals predict variance in distress that is unrelated to the variance explained by the risk factors assessed in Study 2. Thus, compassionate and self-image goals may constitute unique protective and vulnerability factors, respectively, not captured by other constructs. None of the risk factors assessed weekly predicted distress the subsequent week, independent of the effect of goals, suggesting that they may be a consequence, rather than a cause, of short-term change in distress.
Of course, research has identified many other risk factors for anxiety and dysphoria not included in Study 2. Subsequent research should test whether other known risk factors account for the effects of compassionate and self-image goals. Furthermore, dysfunctional attitudes, validation-seeking, and growth-seeking were not assessed in the weekly surveys. Analyses controlling for these variables indicate that pre-existing levels of these variables do not create spurious associations between chronic self-image and compassionate goals on change in distress. However, because we assessed them only at pretest, we cannot test whether chronic levels of these variables averaged across weekly reports would account for the effect of goals, or whether fluctuations in these variables from week to week would account for the same-week or lagged-week effects of goals. We assessed dysfunctional attitudes, growth-seeking, and validation-seeking at pretest for both practical and theoretical reasons. Practically, measures of these variables were too lengthy to include in the weekly surveys. Theoretically, these constructs are conceived as individual differences that create or reduce risk of developing anxiety or dysphoria. We did not expect them to fluctuate meaningfully from week to week. Future research could examine whether these variables do fluctuate meaningfully over time and predict change in distress.
Do other characteristics of goals account for associations between goals and distress?
We included several single-item measures of goal characteristics, in an effort to identify what features of compassionate and self-image goals account for their associations with change in distress. Despite the fact that single item measures are less than ideal, because their internal consistency cannot be assessed, several of these items were associated with change in distress, suggesting that they were valid, if imperfect measures. Neither goal progress nor goals setbacks accounted for the effects of compassionate or self-image goals on distress in any time frame, indicating that compassionate goals do not reduce distress simply because they are easy to achieve, and self-image goals do not increase distress because they are difficult to achieve.
Chronic goal clarity significantly predicted decreased distress in pretest-posttest and same-week analyses, and marginally in lagged-week analyses, providing further support for the importance of meaning and purpose to well-being (Emmons, 1991; King, et al., 2006; King & Napa, 1998). King and her colleagues reported that meaning did not predict positive affect two years later; consequently, they focused attention on whether positive affect increases meaning in life (King, et al., 2006). Because they involved different time intervals, the findings of Study 2 do not contradict King’s findings. Rather, results indicate that having clear goals and aims, a key component of meaning, does predict decreased anxiety and dysphoria one week and 10 weeks later, consistent with a causal effect of meaning on reduced negative affect. Controlling for goal clarity reduced the effect of compassionate goals in every analysis, suggesting that compassionate goals may reduce distress because they give clarity to goals in daily life. Whereas "having clear goals" pertained to life in general, the other goal characteristics more narrowly focused on the participants’ relationship with their roommates. It is striking, then, that general goal clarity accounted for the effects of compassionate goals for roommate relationships better than items more directly related to roommate relationship goals.
According to self-determination theory, goal-related pressure is a key aspect of controlled self-regulation (Deci & Ryan, 1987; Deci & Ryan, 2000; Ryan, 1982). Consistent with self-determination theory, chronic goal-related pressure significantly predicted increased distress from pretest to posttest, and explained the effects of self-image goals in pretest-posttest analyses, suggesting that chronic self-image goals predict decreased distress because they represent controlled, rather than autonomous, self-regulation. However, pressure did not predict distress in the same-week or lagged-week analyses, indicating that goal-related pressure cannot account for the immediate or short-term associations between self-image goals and distress. Perhaps pressure accumulates over time in people who have chronic self-image goals, leading to relatively long-term change in distress. Lower feelings of pressure did not account for the effects of compassionate goals on reduced distress in any analyses. If goal-related pressure indicates controlled self-regulation, as self-determination theory argues, then compassionate goals do not predict reduced distress because they are less controlled. However, other measures of autonomous and controlled motivation should be included in future research to further explore this possibility.
Goal clarity accounted for effects of compassionate but not self-image goals on distress, and goal-related pressure accounted for effects of self-image but not compassionate goals (in pretest-posttest analyses), providing further evidence that compassionate and self-image goals do not represent opposite ends of a single continuum of interpersonal goals. Compassionate and self-image goals apparently related to distress through distinct psychological processes.
Do goals predict distress through social support received from or given to roommates?
We hypothesized that compassionate and self-image goals predict change in the support people give to and receive from others, and change in support given, in particular, predicts change in distress. Compassionate goals consistently related to increased support given to and received from roommates in pretest-posttest, same-week, and lagged week analyses. Consistent with accumulating evidence that giving support benefits psychological well-being (e.g., S. L. Brown, et al., 2008; Deci, et al., 2006), increased support given predicted reduced distress from pretest to posttest and in from one week to the next, even with compassionate and self-image goals and support received controlled, consistent with a path from compassionate goals to reduced distress through change in support given. In same-week analyses, support given was not associated with distress when compassionate and self-image goals and support received were controlled, suggesting that change in support, not simply current levels of support, accounts for the association between compassionate goals and change in distress.
Compassionate goals predicted change in support received from pretest-to-posttest, in the same week, and on lagged weeks, but this effect became nonsignificant when we controlled for support given, suggesting that people with compassionate goals receive more support because they give more support, which is reciprocated. Apparently, people with compassionate goals do not give more support simply because they receive more support, which they then reciprocate. Compassionate goals appear to promote giving support, which reduces distress; receiving support is a side effect of compassionate goals. Change in support received did not predict change in distress from pretest to posttest but did predict change in distress from one week to the next with change in support given controlled, suggesting that receiving support reduces distress over a week, independent of support given, but not over a semester.
Because both having clear goals and change in support given predicted reduced distress in separate analyses, we entered them together as predictors of change in distress, along with goals and change in support received, to see if one of these variables could account for the effects of the other. When predicting change in distress from pretest to posttest, both chronically having clear goals and increased support given predicted reduced distress, suggesting that they explain different parts of the variance in change in distress. In the lagged-week analyses, Week 1 goal clarity marginally predicted change in distress from Week 1 to Week 2, even with change in support given and received controlled, despite the fact that change in support was measured at the same time as change in distress, and goal clarity was measured only on Week 1. Change in support given and received still significantly predicted change in distress. Taken together, these findings suggest that compassionate goals predict reduced distress both because they are associated with goal clarity, and because they lead to increased support given to others.
Does distress predict change in goals?
As hypothesized, distress predicted decreased compassionate goals from pretest to posttest, in the same week, and on the following week; distress predicted increased self-image goals from pretest to posttest and in the same week, but not on the following week. These results are consistent with reciprocal causal associations between compassionate goals and decreased distress, and self-image goals and increased distress (although less consistently), and raise the possibility of virtuous or vicious cycles of goals and distress.
GENERAL DISCUSSION
A growing body of research suggests that both the content and the quality of people’s goals can increase or decrease their distress (e.g., Carver, 2003, 2004; Carver, et al., 1996; Carver & Scheier, 1990; Deci & Ryan, 2000; Dykman, 1998; Emmons, et al., 1996; Higgins, 1998; Higgins, et al., 1997; Kasser & Ryan, 1993; 1996; King, et al., 2006; King, et al., 1998; Strauman, 2002). One aspect of goals not explicitly addressed in other formulations concerns whether people have an egosystem or an ecosystem view of others in relation to the self as they pursue activities in daily life, and what they try to do, interpersonally, as a result. While doing almost any activity or pursuing any goal or aspiration, people may try to get others to satisfy, or not block, their needs and desires by getting others to see them in desired ways, or they may try to be constructive and supportive of others’ needs and desires, or at least not harm others. The present studies show that these interpersonal goals predict change in psychological distress, specifically anxiety and dysphoria.
The Benefits of Compassionate Goals and Giving Support
Compassionate goals predict reduced distress in part because they are associated with having clear goals and aims, and in part because they predict increased giving and receiving of support, which in turn predict reduced distress. Increases in giving support predicted reduced distress even more than increases in receiving support. Our previous research showed that compassionate goals predict increased support over 12 weeks, whereas self-image goals undermine this effect (Crocker & Canevello, 2008). The present studies extend this prior research in several ways. In new data, we measured support given and received weekly as well as in pretest and posttest questionnaires, and pitted support given against support received as predictors of change in distress from pretest to posttest, same-week, and lagged week analyses. As expected, controlling for support received, compassionate goals predicted increased support given to others, which predicted reduced distress over one week and over the first semester of college.
These results reinforce previous research demonstrating the benefits of giving support (e.g., S. L. Brown, et al., 2008; Deci, et al., 2006), and have potentially important implications for the support literature, which emphasizes the support people receive as a predictor of well-being. The idea that giving support improves well-being more effectively than receiving support, and increases support received as a side effect, suggests that support interventions might focus on developing goals to give rather than receive support. Of course, the present studies involve healthy college students; giving support might not be as beneficial for everyone. Yet, Brown and her colleagues showed that caregiving attenuates dysphoria in older couples, and even predicts decreased mortality, indicating that giving support might benefit many people (S. L. Brown, et al., 2008; S. L. Brown, et al., 2003).
Compassionate Goals and Intrinsic Aspirations
The finding that compassionate goals predict increased support given and received fits Kasser and Ryan’s (1996) conception of intrinsic aspirations, which presumably lead to satisfaction of fundamental needs such as the need for relatedness. Our conception of compassionate goals differs from their conception of intrinsic goals, however, in that compassionate goals focus explicitly on the well-being of others. Intrinsic aspirations focus more on the well-being and desires of the self, as indicated by intrinsic goals items such as “There will always be someone around to take care of me;” “I will feel that there are people who really love me;” and “I will find satisfying religious and/or spiritual activities.”
Empirically, intrinsic aspirations and compassionate goals both predict increased well-being over time (e.g., Kasser & Ryan, 1996). In theory, however, intrinsic aspirations predict satisfaction of one’s own organismic needs, such as increased support received from others, which in turn predicts well-being; in contrast, compassionate goals predicted decreased distress through support given, not support received. Thus, although the present studies were not designed to pit compassionate and self-image goals directly against the intrinsic/extrinsic aspirations distinction, the finding that compassionate goals reduce distress through support given rather than support received does not seem to fit the conception of intrinsic goals. These two frameworks could be reconciled if people have a fundamental need to give support, independent of receiving support; increasing evidence that giving support has benefits for health, happiness, and well-being is consistent with this possibility. Future research should address this issue empirically by including compassionate and self-image goals and a measure of intrinsic aspirations as predictors of distress.
Distress Predicts Change in Goals
We predicted that distress and interpersonal goals are mutually reinforcing. As expected, when people feel distressed, their compassionate goals decline and their self-image goals increase over every time frame we examined, consistent with the idea that distress signals problems with one’s current goals: that they are unattainable, depleting, or too risky, or otherwise problematic. This shift in goals may not be adaptive, however; self-image goals predict increased distress, and compassionate goals predict both increased support and decreased distress, suggesting that people who are anxious and dysphoric are caught in a downward spiral in which distress fosters goals that lead to more distress. The shift toward more self-image and less compassionate goals could be adaptive in the short term while having costs in the long term, if they shift attention to getting one’s own needs met immediately, rather than on building supportive relationships that meet one’s needs over time.
Caveats
The present studies are consistent with the hypotheses that interpersonal goals increase or decrease distress, and that distress alters people’s interpersonal goals. However, only studies that manipulate people’s goals or distress can definitively establish causal relationships between goals and distress. Research that manipulates goals would be particularly valuable because it also might inform interventions.
Participants in the present studies were first-semester college students; we do not know whether these findings would generalize to other samples. Accumulating evidence that giving support predicts increased well-being in very different samples (S. L. Brown, et al., 2008; Deci, et al., 2006), however, suggests that compassionate goals might predict reduced distress in many people.
Conclusions
Almost any activity can be done with compassionate or self-image interpersonal goals. Previous research suggests that these goals reflect different views regarding the fundamental association between the self and other people; with an egosystem perspective, other people may be important for satisfaction of one’s own needs and desires; with an ecosystem perspective they may be important because their well-being matters to the well-being of the larger human ecosystem. Consistent with other goals frameworks, the present studies suggest that the interpersonal goals people adopt affect the distress they experience. They also suggest that distress, in turn, shapes interpersonal goals. Self-image goals seem to work like quicksand; the more people try to get others to see the self in desired ways, the more miserable they feel, and the more miserable they feel, the more they try to get others to see the self in desired ways; this cycle undermines, rather than builds, support. Compassionate goals, in contrast, seem to create a virtuous cycle; they provide clarity of goals and increase support, which reduces distress, which in turn fosters more compassionate goals, suggesting that people might be able to decrease their own distress by adopting more compassionate goals.
Acknowledgments
The project described was supported by Grant Number R01MH058869 from the National Institute of Mental Health. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institute of Mental Health or the National Institutes of Health.
We are grateful to Rebecca Caulfield, Timothy Cavnar, Andrew Crocker, Paul Denning, Sarah Franz, Lilita Matison, and Dominik Mischkowski for their assistance with data collection and entry.
Footnotes
We tested the moderating effect of gender by grand mean centering the goals and enteringthe interaction with gender into hierarchical regression equations predicting residual change in distressfrom pretest to posttest. In two separate analyses, the Gender X Self-image Goals interaction (ΔR2 = .02, p = .01, rpartial = −.18) and the Gender X Compassionate Goals interaction (ΔR2 = .02, p = .009, rpartial = −.14) significantly increased the variance explained. To examine the nature of these interactions, we computed the simple slopes for males and females (Aiken & West, 1991). Although the effects of both goals were in the same direction for both genders, self-image goals predicted increased distress for males (β = .39, p < .001) but not females (β = .10, ns), whereas compassionate goals predicted decreased distress for females (β = −.45, p < .001) but only marginally predicted decreased distress for males (β = −.16, p = .08).
Gender did not moderate the effects of compassionate or self-image goals on residual change in distressfrom pretest to posttest in Study 2. There were no Gender X Self-image Goals or Gender X Compassionate Goals interactions for change in anxiety, dysphoria, or distress(all R2 < .01, ns, rpartial < .01).
Although several authors provide guidelines for centering in multilevel analyses (e.g., Kreft & de Leeuw, 1998; Raudenbush & Bryk, 2002), they also discourage “thoughtless application” of these guidelines (Enders & Tofighi, 2007, p. 136)and, instead, encourage centering strategies based on specific substantive research questions. Although lagged analyses are performed on weekly data, person-centering in these analyses does not test our hypothesis. Lagged analyses examine whether change in the outcome from oneweek to the next is related to levels of the goal (or other predictor), regardless of the source individual differences or weekly fluctuations around those individual differences. We hypothesize that students’ goals one week predict their distressthe following week, controlling for that week’s distress. Person centering predictors tests whether fluctuations in students’goals from students’own average goals predict outcomes. Consequently, person-centering predictors in lagged analyses tests whether within-person departures from students’ average goals one week predict students’ distressthe following week, controlling for within-person departures from students’ average distressthat week. This does not test our lagged hypothesis. Thus, centering on the grand mean for that week is justified and appropriate in these analyses(e.g., Enders & Tofighi, 2007).
Publisher's Disclaimer: The following manuscript is the final accepted manuscript. It has not been subjected to the final copyediting, fact-checking, and proofreading required for formal publication. It is not the definitive, publisher-authenticated version. The American Psychological Association and its Council of Editors disclaim any responsibility or liabilities for errors or omissions of this manuscript version, any version derived from this manuscript by NIH, or other third parties. The published version is available at www.apa.org/pubs/journals/psp
Contributor Information
Jennifer Crocker, University of Michigan.
Amy Canevello, University of Michigan.
Juliana G. Breines, University of California at Berkeley
Heather Flynn, University of Michigan.
References
- Aiken LS, West SG. Multiple regression: Testing and interpreting interactions. Newbury Park, CA: Sage; 1991. [Google Scholar]
- Alden LE, Taylor CT. Interpersonal processes in social phobia. Clinical Psychology Review. 2004;24:857–882. doi: 10.1016/j.cpr.2004.07.006. [DOI] [PubMed] [Google Scholar]
- Baumeister RF, Vohs KD. Self-regulation, ego depletion, and motivation. Social and Personality Psychology Compass. 2007;1:115–128. [Google Scholar]
- Brown GP, Hammen CL, Craske MG, Wickens TD. Dimensions of dysfuncitonal atittudes as vulnerabilities to depressive symptoms. Journal of Abnormal Psychology. 1995;104:431–435. doi: 10.1037//0021-843x.104.3.431. [DOI] [PubMed] [Google Scholar]
- Brown SL, Brown RM, House JS, Smith DM. Coping with spousal loss: Potential buffering effects of self-reported helping behavior. Personality and Social Psychology Bulletin. 2008;34:849–861. doi: 10.1177/0146167208314972. [DOI] [PubMed] [Google Scholar]
- Brown SL, Nesse RM, Vinokur AD, Smith DM. Providing social support may be better than receiving it: Results from a prospective study. Psychological Science. 2003;14:320–327. doi: 10.1111/1467-9280.14461. [DOI] [PubMed] [Google Scholar]
- Campbell L, Kashy DA. Estimating actor, partner, and interaction effects for dyadic data using PROC MIXED and HLM: A user-friendly guide. Personal Relationships. 2002;9:327–342. [Google Scholar]
- Campbell L, Simpson JA, Boldry J, Kashy DA. Perceptions of conflict and support in romantic relationships: The role of attachment anxiety. Journal of Personality and Social Psychology. 2005;88:510–531. doi: 10.1037/0022-3514.88.3.510. [DOI] [PubMed] [Google Scholar]
- Canevello A, Crocker J. Creating good relationships: Responsiveness, relationship quality, and interpersonal goals. Journal of Personality and Social Psychology. doi: 10.1037/a0018186. in press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carver CS. Pleasure as a sign you can attend to something else: Placing positive feelings within a general model of affect. Cognition & Emotion. 2003;17:241–261. doi: 10.1080/02699930302294. [DOI] [PubMed] [Google Scholar]
- Carver CS. Negative affects arising from the behavioral approach system. Emotion. 2004;4:3–22. doi: 10.1037/1528-3542.4.1.3. [DOI] [PubMed] [Google Scholar]
- Carver CS, Lawrence JW, Scheier MF. A control-process perspective on the origins of affect. In: Martin LL, Tesser A, editors. Striving and feeling: Interactions among goals, affect, and self-regulation. Hillsdale, NJ: Erlbaum; 1996. [Google Scholar]
- Carver CS, Scheier MF. Origins and functions of positive and negative affect: A control-process view. Psychological Review. 1990;97:19–35. [Google Scholar]
- Coyne JC. Toward an interactional description of depression. Psychiatry: Journal for the Study of Interpersonal Processes. 1976;39:28–40. doi: 10.1080/00332747.1976.11023874. [DOI] [PubMed] [Google Scholar]
- Crocker J. From egosystem to ecosystem: Implications for learning, relationships, and well-being. In: Wayment HA, Brauer JJ, editors. Transcending self-interest: Psychological explorations of the quiet ego. Washington, DC: APA; 2008. pp. 63–72. [Google Scholar]
- Crocker J, Canevello A. Creating and undermining social support in communal relationships: The role of compassionate and self-image goals. Journal of Personality and Social Psychology. 2008;95:555–575. doi: 10.1037/0022-3514.95.3.555. [DOI] [PubMed] [Google Scholar]
- Crocker J, Olivier MA, Nuer N. Self-image goals and compassionate goals: Costs and benefits. Self and Identity. 2009;8:251–269. doi: 10.1080/15298860802505160. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Crowne D, Marlowe D. The approval motive: Studies in evaluative dependence. New York: Wiley; 1964. [Google Scholar]
- Davila J, Beck JG. Is social anxiety associated with impairment in close relationships? A preliminary investigation. Behavior Therapy. 2002;33:427–446. [Google Scholar]
- Deci EL, La Guardia JG, Moller AC, Scheiner MJ, Ryan RM. On the benefits of giving as well as receiving autonomy support: Mutuality in close friendships. Personality and Social Psychology Bulletin. 2006;32:313–327. doi: 10.1177/0146167205282148. [DOI] [PubMed] [Google Scholar]
- Deci EL, Ryan RM. The support of autonomy and the control of behavior. Journal of Personality and Social Psychology. 1987;53:1024–1037. doi: 10.1037//0022-3514.53.6.1024. [DOI] [PubMed] [Google Scholar]
- Deci EL, Ryan RM. The “what” and “why” of goal pursuits: Human needs and the self-determination of behavior. Psychological Inquiry. 2000;11:227–268. [Google Scholar]
- Dunn EW, Aknin LB, Norton MI. Spending money on others promotes happiness. Science. 2008;319:1687–1688. doi: 10.1126/science.1150952. [DOI] [PubMed] [Google Scholar]
- Dykman BM. Integrating cognitive and motivational factors in depression: Initial tests of a goal orientation approach. Journal of Personality and Social Psychology. 1998;74:139–158. doi: 10.1037//0022-3514.74.1.139. [DOI] [PubMed] [Google Scholar]
- Emmons RA. Personal strivings, daily life events, and psychological and physical well-being. Journal of Personality. 1991;59:453–472. doi: 10.1111/j.1467-6494.1991.tb00256.x. [DOI] [PubMed] [Google Scholar]
- Emmons RA, Kaiser HA, Martin LL, Tesser A. Striving and feeling: Interactions among goals, affect, and self-regulation. Hillsdale, NJ England: Lawrence Erlbaum Associates, Inc; 1996. Goal orientation and emotional well-being: Linking goals and affect through the self; pp. 79–98. [Google Scholar]
- Fitzsimons GiM, Bargh JA. Thinking of you: Nonconscious pursuit of interpersonal goals associated with relationship partners. Journal of Personality and Social Psychology. 2003;84:148–163. [PMC free article] [PubMed] [Google Scholar]
- Frijda NH. The laws of emotion. American Psychologist. 1988;43:349–358. doi: 10.1037//0003-066x.43.5.349. [DOI] [PubMed] [Google Scholar]
- Higgins ET. Promotion and prevention: Regulatory focus as a motivational principle. In: Zanna MP, editor. Advances in experimental social psychology. Vol. 30. New York: Academic Press; 1998. pp. 1–46. [Google Scholar]
- Higgins ET, Shah J, Friedman R. Emotional responses to goal attainment: Strength of regulatory focus as a moderator. Journal of Personality and Social Psychology. 1997;72:515–525. doi: 10.1037//0022-3514.72.3.515. [DOI] [PubMed] [Google Scholar]
- Joiner TE, Jr, Coyne JC. The interactional nature of depression: Advances in interpersonal approaches. Washington, DC, US: American Psychological Association; 1999. [Google Scholar]
- Joiner TE, Jr, Katz J, Lew A. Harbingers of depressotypic reassurance seeking: Negative life events, increased anxiety, and decreased self-esteem. Personality and Social Psychology Bulletin. 1999;25:630–637. [Google Scholar]
- Joiner TE, Jr, Metalsky GI. Excessive reassurance seeking: Delineating a risk factor involved in the development of depressive symptoms. Psychological Science. 2001;12:371–378. doi: 10.1111/1467-9280.00369. [DOI] [PubMed] [Google Scholar]
- Kashy DA, Donnellan MB, Burt SA, McGue M. Growth curve models for indistinguishable dyads using multilevel modeling and structural equation modeling: The case of adolescent twins’ conflict with their mothers. Developmental Psychology. 2008;44:316–329. doi: 10.1037/0012-1649.44.2.316. [DOI] [PubMed] [Google Scholar]
- Kasser T, Ryan RM. A dark side of the American dream: Correlates of finanical success as a central life aspiration. Journal of Personality and Social Psychology. 1993;65:410–422. doi: 10.1037//0022-3514.65.2.410. [DOI] [PubMed] [Google Scholar]
- Kasser T, Ryan RM. Further examining the American dream: Differential correlates of intrinsic and extrinsic goals. Personality and Social Psychology Bulletin. 1996;22:280–287. [Google Scholar]
- Keller MC, Nesse RM. The evolutionary significance of depressive symptoms: Different adverse situations lead to different depressive symptom patterns. Journal of Personality and Social Psychology. 2006;91:316–330. doi: 10.1037/0022-3514.91.2.316. [DOI] [PubMed] [Google Scholar]
- Kenny DA. Cross-lagged panel correlation: A test for spuriousness. Psychological Bulletin. 1975;82:887–903. [Google Scholar]
- Kenny DA, Kashy DA, Cook WL. Dyadic data analysis. Guilford Press; 2006. [Google Scholar]
- King LA, Hicks JA, Krull JL, Del Gaiso AK. Positive affect and the experience of meaning in life. Journal of Personality and Social Psychology. 2006;90:179–196. doi: 10.1037/0022-3514.90.1.179. [DOI] [PubMed] [Google Scholar]
- King LA, Napa CK. What makes a life good? Journal of Personality & Social Psychology. 1998;75:156–165. doi: 10.1037//0022-3514.75.1.156. [DOI] [PubMed] [Google Scholar]
- King LA, Richards J, Stemmerich ED. Daily goals, life goals, and worst fears: Means, ends, and subjective well-being. Journal of Personality. 1998;66:713–744. doi: 10.1111/1467-6494.00030. [DOI] [PubMed] [Google Scholar]
- Nesse RM. What good is feeling bad? The evolutionary benefits of psychic pain. The Sciences. 1991;31:30–37. [Google Scholar]
- Nesse RM, Ellsworth PC. Evolution, emotions, and emotional disorders. American Psychologist. 2009;64:129–139. doi: 10.1037/a0013503. [DOI] [PubMed] [Google Scholar]
- Newman MG, Erickson T. Gneralized anxiety disorder. Pennsylvania State University; 2008. [Google Scholar]
- Nolen-Hoeksema S, Wisco BE, Lyubomirsky S. Rethinking rumination. Perspectives on psychological science. 2008;3:400–424. doi: 10.1111/j.1745-6924.2008.00088.x. [DOI] [PubMed] [Google Scholar]
- Rogosa D. A critique of cross-lagged correlation. Psychological Bulletin. 1980;88:245–258. [Google Scholar]
- Rosenthal R, Rosnow R. Essentials of behavioral research: Methods and data analysis. 2. New York: McGraw Hill; 1991. [Google Scholar]
- Ryan RM. Control and information in the interpersonal sphere: An extension of cognitive evaluation theory. Journal of Personality and Social Psychology. 1982;43:450–461. [Google Scholar]
- Spielberger CD, Vagg PR, Barker LR, Donham GW, Westberry LG, editors. The factor structure of the state-trait anxiety inventory. Vol. 7. Washington, D.C: Hemisphere; 1980. [Google Scholar]
- Strauman TJ. Self-regulation and depression. Self and Identity. 2002;1:151–157. [Google Scholar]
- Trapnell PD, Campbell JD. Private self-consciousness and the five-factor model of personality: Distinguishing rumination from reflection. Journal of Personality and Social Psychology. 1999;76:284–384. doi: 10.1037//0022-3514.76.2.284. [DOI] [PubMed] [Google Scholar]
- Weissman AN, Beck AT. Development and validation of the Dysfunctional Attitude Scale: A preliminary investigation; Paper presented at the annual meeting of the American Psychological Association; Toronto, Canada. 1978. [Google Scholar]
- West SG, Biesanz JC, Pitts SC, editors. Causal inference and generalization in field settings: Experimental and quasi-experimental designs. Cambridge: Cambridge University Press; 2000. [Google Scholar]
- Wrosch C, Miller GE. Depressive symptoms can be useful: Self-regulatory and emotional benefits of dysphoric mood in adolescence. Journal of Personality and Social Psychology. 2009;96:1181–1190. doi: 10.1037/a0015172. [DOI] [PubMed] [Google Scholar]
- Zimet GD, Powell SS, Farley GK. Psychometric characteristics of the Multidimensional Scale of Perceived Social Support. Journal of Personality Assessment. 1990;55:610–617. doi: 10.1080/00223891.1990.9674095. [DOI] [PubMed] [Google Scholar]