

We have previously shown the HLA matching effect on liver allografts, which suggested the importance of class I matching in liver transplantation. 1 In this study, using a new set of patients, we reviewed our earlier analysis to study whether or not the class I matching effect still remained.
MATERIALS AND METHODS
This study consisted of a total of 347 patients who received orthotopic liver transplantation (OLT) at the Presbyterian University Hospital and Pittsburgh Children Hospital from January 1, 1991 to December 31, 1991. All patients had first OLTs with a negative T-lymphocyte crossmatch. The only patients excluded from the study were those who received simultaneous pancreas, kidney, or small intestine transplants. Initial immunosuppressive drug therapy consisted of either cyclosporine (CyA) or FK 506 in combination with prednisone. Acute cellular rejection was treated with bolus methylprednisone and/or OKT3.
HLA typing was performed according to the standard NIH method2 using HLA typing trays obtained commercially (Gen Trak, Inc, Plymonth Meeting, PA, and One Lambda, Inc, Canogo Park, Calif).
Both patient death and allograft removal, regardless of reasons, were considered as graft failure. Graft survival rates were computed by the life table method and the generalized Wilcoxon test was used for statistics.
RESULTS
HLA-A and -B Loci
The 1-year graft survival rate of patients with 2 A locus mismatched grafts was lower than that with 0 or 1 A locus mismatched grafts (Fig 1).
Fig 1.
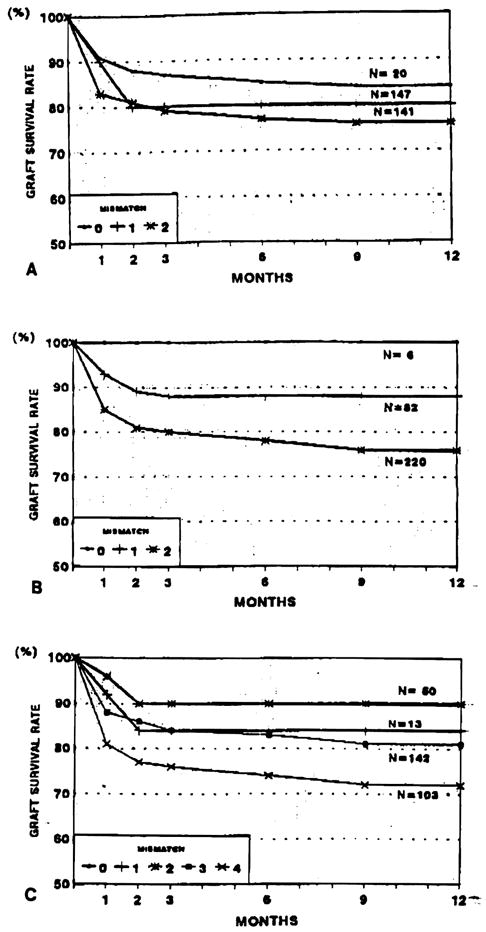
Graft survival by mismatched at HLA-A and/or -B locus: (A) HLA-A, (B) HLA-B, (C) HLA-A,B.
As to the HLA-B locus, the matching effect appears to be clear (Fig 1). That is, the best survival rate was observed in patients with 0 B mismatches and the worst was in patients with 2 B mismatched grafts. When class I antigens were combined, the matching effect on the transplanted liver allografts became clearer (Fig 1).
HLA-DR Locus
It was revealed that the 1-year graft survival rate of patients with 0 DR mismatched grafts was worse than those with 1 or 2 DR mismatched transplants. The 1-year graft survival rates of patients with 0, 1, and 2 DR mismatches were 65.6%, 84%, and 79%, respectively (Fig 2).
Fig 2.
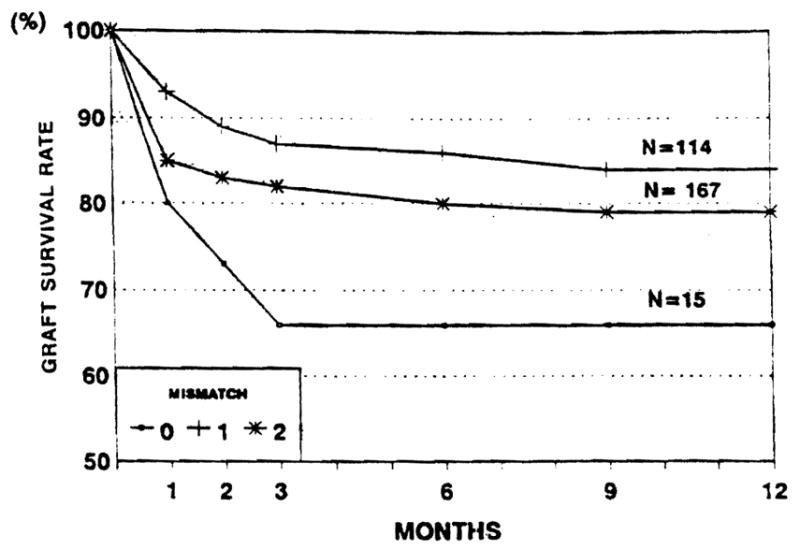
Graft survival by mismatched at HLA-DR locus.
The analysis of B, DR matching as well as 6-antigen matching (A, B, DR) did not provide any informative trends (data not shown).
DISCUSSION
This study shows clear evidence of an HLA-A and -B matching effect (class I matching effect) on liver allografts. The differences in the 6-month graft survival rates between the best and worst matched transplants were 6.6% for the A locus, 10.4% for the B locus, and 10.9% for the A, B loci.
The outcome of liver transplants has been improving during the last decade, with the introduction of CyA3 and the University of Wisconsin (UW) solution.4 In addition, improved posttransplant care and improved operative procedures reduced nonimmunologic early graft failures.5 These contributions probably helped to unveil the HLA matching effect in liver transplantation. In point of fact, the patients in this study had a 1-year survival rate of nearly 80%, which is significantly higher than those reported earlier.6
The DR matching effect seems to be stronger than AB matching in kidney transplants; however, we failed to obtain a DR matching effect in this study. Moreover, liver allografted patients with 0 DR mismatches had a lower graft survival rate than those with 1 or 2 DR mismatched transplants. There is a possibility that patients in our study with 0 DR mismatched transplants were not really 0 DR mismatched transplants as recently reported by Opelz et al.7 However, it should be noted that at our institution, the DR matching effect was clearly shown for kidney patients transplanted during the same period. Thus, there must be an additional reason(s) why DR matched liver graft survival rates were inferior.
References
- 1.Kobayashi M, Yagihashi A, Noguchi K, et al. HLA. New York: Oxford University Press; 1991. (in press) [Google Scholar]
- 2.Zachary AA, Teresi GA, editors. ASHI Laboratory Manual. American Society for Histocompatibility and Immunogenetics; 1990. [Google Scholar]
- 3.Calne RY, Rolles K, White DJG, et al. Lancet. 1979;ii:1033. [Google Scholar]
- 4.Todo S, Nery J, Yanaga K, et al. JAMA. 1989;261:711. [PMC free article] [PubMed] [Google Scholar]
- 5.Starzl TE, Todo S, Tzakis AG, et al. Transplant Proc. 1989;21:2197. [PMC free article] [PubMed] [Google Scholar]
- 6.Markus BH, Duquesnoy RJ, Gordon RD, et al. Transplantation. 1988;46:372. [PMC free article] [PubMed] [Google Scholar]
- 7.Opelz G, Mytilineos J, Scherer S, et al. Lancet. 1991;338:461. doi: 10.1016/0140-6736(91)90540-6. [DOI] [PubMed] [Google Scholar]