

Abstract
Exercise self-efficacy is a powerful predictor of physical activity behavior, which enhances health and well-being for older adults. Social relations have been proposed as influential precursors for exercise self-efficacy. In a longitudinal study of 160 older adults with osteoarthritis (76.9% women), the authors found that social support (but not social strain) significantly predicted exercise self-efficacy in a structural equation model examining cross-sectional data: χ2(178, N = 160) = 264.57, p < .01; RMSEA = .06; CFI = .92; TLI = .90. When data were examined longitudinally, however, social strain (but not social support) significantly predicted lower exercise self-efficacy 1 year later: χ2(233, N = 160) = 288.64, p < .01; RMSEA = .04; CFI = .96; TLI = .95. Results support the negativity effect, suggesting that social strain might be the more potent aspect of social relations and should be the target of interventions.
Keywords: social support, social strain, arthritis
According to the American College of Sports Medicine (ACSM, 2000), exercise or regular physical activity provide a number of health benefits including decreased mortality and morbidity; reduced risk for heart disease, obesity, diabetes, stroke, cancer, and osteoporosis; enhanced cognitive functioning; and increased feelings of psychological well-being. Exercise is particularly beneficial for older adults with osteoarthritis (OA), because it helps decrease pain, maintain joint function, and control weight (Bassey, 2000; Hughes et al., 2004).
Exercise is vital for the aging population. One of the most effective ways to promote exercise behavior is to enhance exercise self-efficacy, or perceived beliefs in control over one's ability to exercise (e.g., Bandura, 1997; Rimal, 2001). Previous research has demonstrated that increasing social support for exercise promotes increased exercise self-efficacy and enhances exercise behavior in turn (McAuley, Jerome, Marquez, Elavsky, & Blissmer, 2003). Previous literature has not examined social strain or the negative aspects of social relationships, however, for their influence on self-efficacy and exercise (Chogahara, O'Brien Cousins, & Wankel, 1998), even though social strain might have a more powerful influence on self-efficacy than social support (Rook, 2001). Therefore, in the current study we examined the relative influences of social support and social strain on exercise self-efficacy in a sample of older adults with OA to inform health and well-being interventions.
Benefits of Exercise for OA
Although exercise is beneficial for the general older adult population, it is particularly beneficial for older adults with OA, because it might both help prevent the development of OA and treat symptoms of OA once the disease has developed (Vuori, 2001). OA is a degenerative joint disease that affects 21 million Americans (Arthritis Foundation, 2007), and it is the most common disease among older adults (Felson & Zhang, 1998). It is characterized by a breakdown of the joint's cartilage, which causes bones to rub against each other, and can be painful and disabling (Arthritis Foundation). Participation in physical activity might indirectly prevent OA by helping prevent obesity, because exercise helps to control the excess weight that increases joint load (Vuori).
In addition to reducing the risk of OA, exercise can also be an effective treatment for OA symptoms. For example, exercise therapy such as stationary cycling has been shown to relieve pain and reduce disability from knee and hip OA (Vuori, 2001). Furthermore, Bassey (2000) reported that moderate exercise (e.g., walking, swimming, cycling) and strengthening the muscles supporting joints (e.g., quadriceps exercises for the knee joint) helps older adults with OA maintain joint function, control weight, and avoid excessive joint load, which helps control joint pain and minimize disability.
Exercise Promotion
Enhancing exercise self-efficacy is one of the most effective methods of increasing exercise participation because it instills a sense of self-confidence in personal abilities to become and remain physically active (Bandura, 1997; Jette et al., 1998; McAuley et al., 2003). In fact, in two longitudinal studies of data from over 1,000 adults in the Stanford Five-City Project, a cardiovascular disease-prevention field experiment in California, Rimal (2001) found that, in structural equation models (controlling for education, income, and age of participant), exercise self-efficacy was the strongest predictor of subsequent exercise behavior.
Increasing Exercise Self-Efficacy
Increasing exercise is a powerful tool for enhancing the health and well-being of older adults with OA, and bolstering exercise self-efficacy lays the foundation for increased exercise participation. Therefore, exercise interventions must address methods for increasing exercise self-efficacy. According to social cognitive theory (Bandura, 1997), the social environment provides the context for behavior and contributes significantly to feelings of self-efficacy. The impact of the social environment on self-efficacy beliefs depends, however, on the nature of the social environment: Social relations can be positive (social support), providing good models, teachers, and positive feedback, thus bolstering self-efficacy, and negative (social strain), providing poor models and negative feedback, thus undermining self-efficacy.
Social Support Versus Social Strain
Most of the research conducted on exercise has investigated the influence of social support on exercise behavior, ignoring the potential impact of social strain (Chogahara et al., 1998). Such studies have shown that perceiving social support for exercise (e.g., encouragement) predicts exercise self-efficacy (e.g., Brassington, Atienza, Perczek, DiLorenzo, & King, 2002; McAuley et al., 2003; Resnick, Orwig, Magaziner, & Wynne, 2002). The influence of social strain on exercise, however, has not yet been widely examined in the context of exercise promotion despite the fact that some researchers (e.g., Rook, 2001) argue that social strain has a more potent and long-lasting effect than social support on health and well-being.
Rook (1990) has termed this differential influence of social strain over social support the negativity effect, arguing that social strain is more powerful than social support because acts of social strain violate our expectations that friends and family are supposed to be supportive (Rook & Pietromonaco, 1987). Therefore, social strain for exercise might play a more influential role in exercise adoption and adherence than social support, especially over time, by undermining confidence in ability to exercise, thus squelching motivation to exercise. In fact, the few studies that have examined social strain for exercise behavior have reported that higher perceived social strain is associated with lower exercise participation (Chogahara, 1999; Hirvensalo, Heikkinen, Lintunen, & Rantanen, 2005).
General Versus Exercise-Specific Social Relations
In addition to the role of social strain, previous studies have also ignored the contribution of the broad social context to exercise self-efficacy and exercise participation and, instead, have limited their focus to the contributions of domain-specific social interactions. For example, as stated previously, researchers have examined the influence of social support for exercise on exercise self-efficacy and exercise behavior. General social support and general social strain have both demonstrated important influences on health and well-being but have not yet been included in exercise studies. For example, general social support has been shown to promote positive health behaviors (Cohen, 2004) and positively affect physical and psychological well-being (Berkman, Glass, Brissette, & Seeman, 2000; Heller & Rook, 2001; Seeman, 2000), as well as encourage exercise participation (Carron, Hausenblas, & Mack, 1996). Therefore, general social support might also have an impact on exercise self-efficacy. Furthermore, general social strain has been shown to negatively influence health and well-being (Antonucci, Akiyama, & Lansford, 1998; Rook, 1990). To our knowledge, the influence of general social strain on exercise self-efficacy or exercise behavior has not yet been investigated empirically but should be because of its potentially powerful effects on both outcomes.
Lachman and Weaver (1998) argue that demonstrating relationships between predictor variables and health and well-being outcomes using generalized measures would be even more compelling than showing such relationships with domain-specific measures because significant relationships using generalized measures would apply to multiple domains of functioning. Therefore, if general social interactions influence exercise to a similar extent as do exercise-specific social interactions, interventions can aim to influence general social relations instead of exercise-specific social relations. This could have the added benefit of enhancing health behaviors and health outcomes in addition to exercise, which could lead to more comprehensive health interventions. In other words, targeting general social relations might result in less expensive and more effective interventions.
The Current Study
Based on the arguments just presented, in the current investigation we were interested in the influences of general social support and general social strain on exercise self-efficacy both simultaneously and over time. Specifically, we hypothesized that higher social support and lower social strain would predict higher exercise self-efficacy in cross-sectional and longitudinal analyses for older adults with OA (see Figure 1).
Figure 1.
Conceptual model: Higher social support and lower social strain predict higher exercise self-efficacy.
Method
Participants
Participants were recruited for Time 1 data collection through newspaper ads, flyers, group newsletters, and presentations at local senior centers. One hundred sixty older adults age 58–94 years (M = 73.25, SD = 8.00) volunteered to participate at Time 1 (76.9% women). All participants resided in the Boston area, spoke fluent English, and experienced pain from self-reported OA in the knee or the hip joints on at least 3 days in the typical week. Most participants considered themselves White (85.6%), one third were married (31.9%), all were well educated, and their median annual income was $20,001–50,000 (see Table 1 for demographic characteristics). Participants were informed at Time 1 that we would ask for their participation at Time 2, although they were, of course, free to decline to participate at Time 2.
Table 1. Summary of Demographic Characteristics (N = 160).
| Trait | % |
|---|---|
| Ethnicity | |
| White | 85.6 |
| African American | 3.1 |
| Asian/Asian American | 2.5 |
| Hispanic/Latino(a) | 0.6 |
| Native American/American Indian | 3.1 |
| Education | |
| some high school education | 5.0 |
| high school diploma/GED | 16.3 |
| some college education | 22.5 |
| associate's degree | 6.3 |
| bachelor's degree | 11.9 |
| some graduate education | 8.1 |
| master's degree | 20.0 |
| doctoral degree | 5.6 |
| Marital status | |
| single | 10.0 |
| married | 31.9 |
| divorced/separated | 27.5 |
| widowed | 26.3 |
| Annual income | |
| less than $10,000 | 15.0 |
| $10,001–20,000 | 26.9 |
| $20,001–50,000 | 30.6 |
| $50,001–75,000 | 10.6 |
| $75,001 or more | 9.4 |
For Time 2 data collection, we attempted to contact all Time 1 participants 9–12 months after their first appointment and asked them to participate in another interview. Eighty-three percent of participants were retained for the second wave of data collection. Of the 25 participants lost to follow-up, 1 died, 2 were hospitalized or too sick to participate, 8 were not interested in participating the second time or generally declined future participation, and 14 were unreachable by phone or mail. There were no significant differences on any baseline variables between participants who were retained at Time 2 and those who were not.
Measures
Self-efficacy for exercise was assessed using three scales: one measure of self-efficacy for exercise, one measure of attitudes about exercise and health, and one measure of beliefs about control over exercise behavior. Each exercise-self-efficacy subscale was used as an indicator of the latent construct of exercise self-efficacy in structural equation models.
The Self-Efficacy for Exercise Scale (Jette et al., 1998) consists of nine items that measure participants' confidence that they will exercise under various circumstances. Responses are given on a 4-point scale (1 = very sure, 4 = not at all sure) with a fifth option of “I do not usually do this” (with a value of 0). Responses are summed, with possible scores ranging from 0 to 36. Scores for this sample also ranged from 0 to 36 (M = 23.94, SD = 8.21 at Time 1, M = 23.41, SD = 8.15 at Time 2). Jette et al. have reported high internal consistency for this scale (α = .88). The current sample revealed a high Cronbach's alpha at Time 1 (α = .93) and at Time 2 (α = .93).
The Attitudes about Exercise and Health Scale (Jette et al., 1998) consists of three items that evaluate the extent to which participants believe that exercising is desirable and beneficial to their health. Responses are measured on a 5-point scale (1 = strongly agree, 5 = strongly disagree) and summed, with possible scores ranging from 3 to 15. Scores for this sample ranged from 3 to 15 (M = 13.67, SD = 2.24) at Time 1 and from 7 to 15 (M = 13.80, SD = 1.89) at Time 2. Jette et al. have reported low internal consistency for this scale (α = .57). Reliability analyses with the current sample revealed an acceptable Cronbach's alpha at Time 1 (α = .73) but a relatively low Cronbach's alpha at Time 2 (α = .65).
The Beliefs about Control over Exercise Behavior Scale (Jette et al., 1998) consists of six items that evaluate participants' beliefs about the extent to which they can control their exercise behavior. Responses are given on a 5-point scale (1 = strongly agree, 5 = strongly disagree) and summed, with possible scores ranging from 6 to 30. Scores for this sample ranged from 6 to 30 (M = 25.06, SD = 4.36) at Time 1 and from 16 to 30 (M = 24.76, SD = 3.56) at Time 2. Jette et al. have reported low internal consistency for this scale (α = .59), but reliability analyses with the current sample revealed a high Cronbach's alpha at Time 1 (α = .84) and a reasonable alpha at Time 2 (α = .76).
Social support was measured with the Medical Outcomes Study—Social Support Survey (Sherbourne & Stewart, 1991), which measures assistance and companionship given to participants by people in their lives. The questions ask the respondent to rate the availability of specific domains of help on a 5-point scale (1 = none of the time, 5 = all of the time) including emotional/informational (α = .96), affection (α = .91), tangible (α = .92), and positive interaction support (α = .94). Each social-support subscale was used as an indicator of the latent construct of social support in structural equation models. Possible scores for the emotional/informational-support subscale ranged from 8 to 40 (M = 29.15, SD = 7.70 for the current sample). Possible scores for affection ranged between 3 and 15 (M = 11.08, SD = 3.23 for the current sample). Possible scores for tangible support ranged between 4 and 20 (M = 13.73, SD = 4.35 for the current sample). Possible scores for positive interaction ranged between 3 and 15 (M = 11.28, SD = 2.97 for the current sample). Sherbourne and Stewart have reported high convergent and divergent validity, as well as high internal consistency, for the subscales. Reliability analyses with the current sample also revealed high reliability for the tangible (α = .89), affection (α = .91), emotional/informational (α = .96), and positive-interaction (α = .93) subscales.
Social strain was measured with the Test of Negative Social Exchange (Ruehlman & Karoly, 1991), which measures unsupportive actions and negative interactions with people involved in the participant's life. The 18 questions are rated on a 4-point scale (1 = very seldom, 4 = more than once a week). Responses are divided into four subscales with acceptable reliability (Ruehlman & Karoly): hostility/impatience (α = .83), insensitivity (α = .82), interference (α = .75), and ridicule (α = .70). These four indicators of social strain were used as manifest indicators of the latent construct social strain in structural equation models. Scores on the hostility/impatience subscale range from 6 to 24 (M = 8.54, SD = 3.72 for the current sample). Scores on the insensitivity subscale range from 5 to 20 (M =7.35, SD = 2.78 for the current sample). Scores on the interference subscale range from 4 to 16 (M = 5.46, SD = 2.05 for the current sample). Scores on the ridicule sub-scale range from 3 to 12 (M = 3.53, SD = 1.22 for the current sample). Reliability analyses for the subscales in this sample revealed good Cronbach's alphas for all the subscales (α = .92 for hostility/impatience, α = .81 for insensitivity, α = .75 for interference, and α = .75 for ridicule).
Perceived OA severity was measured with four items asking participants to rate the severity of their OA symptoms on an 11-point scale (0 = none, 10 = severe). Items were “How much pain have you had in the past week?” “How much stiffness did you experience in the past week?” “How much difficulty did you have with physical activities you wanted to do over the past week because of your osteoarthritis symptoms?” and “Considering all the ways that osteoarthritis affects you, rate how you are doing on the following scale.” A composite severity score is computed by summing participants' responses to all items, with a higher score indicating more perceived OA severity. Possible scores range from 0 to 40. The range of scores for this sample was 0–40 (M = 18.50, SD = 7.86). Reliability in this sample was high (α = .83).
Physical disability was measured with a physical-disability measure from the Fitness and Arthritis in Seniors Trial (Ettinger et al., 1997). The measure consists of 23 items asking participants to rate the amount of difficulty, in the past month, they have had doing each of the listed daily activities because of their arthritis (e.g., “How difficult was it climb a flight of stairs?”). Participants rate each item on 5-point Likert-type scale (1 = not difficult, 5 = I was unable to do this activity). We added a sixth option (with a value of 0), “I do not usually do this activity for other reasons unrelated to my arthritis,” to distinguish participants who did not do an activity because of their physical condition from those for whom the activity was not applicable for some other reason (e.g., they did not have any stairs in their home). A composite disability score is computed by summing participants' responses to all items. Possible scores range from 0 to 115. One item from the scale (“How difficult was it to take care of a family member?”) was deleted from analyses because of a high frequency of selecting the “I do not usually do this activity” option (36.6%), thus changing the possible range of scores to 0–110. The range of scores for this sample was 22–79 (M =38.01, SD =11.31). Reliability for the original disability subscale of the Fitness and Arthritis in Seniors Trial is high (α = .79, Ettinger et al.), and reliability for the modified scale in the current sample was also high (α = .88).
Procedure
Participants were recruited through advertisements and presentations at local senior centers and senior housing. Older adults with OA who were interested in participating in the study phoned the investigators to schedule a time and location for the interview (e.g., on campus, at the participant's home, or a safe public location like a public library). After a full informed-consent process, including answering any questions from participants, the experimenter explained how to use the computer to complete the questionnaire and allowed the participant to practice with several sample questions to adjust to the computer format.
The survey was conducted on the Windows research software package Media-Lab (Empirisoft), which presented individual questionnaires in random order for the first half of the survey and fixed order for the second half. Thirty-one participants opted to fill out paper surveys for two reasons: either discomfort using a computer or because they participated in a small-group interview for which there were not enough computers for all participants.1 The order of individual questionnaires on the paper surveys was not randomized. The researcher remained available throughout the study to answer participants' questions. At the completion of the survey, participants were debriefed and given a $20 honorarium. Identical procedures were followed for Time 2 interviews.
Analysis Plan
To examine the relative contributions of social support and social strain to exercise self-efficacy, variables were examined in structural equation models using AMOS 6.0 software (Arbuckle, 2004). Because multiple indexes of fit are preferable when explaining how well data fit the structural equation models (Byrne, 1998), we reported the root mean square error of approximation (RMSEA), the comparative-fit index (CFI), and the Tucker-Lewis Index (TLI)/Non-Normed Fit Index (NNFI; Boomsma, 2000). The RMSEA is an index of fit that takes the error of approximation of the population into account. A value less than .05 reflects a good fit, a value less than .08 reflects a reasonable fit, and a value greater than .10 indicates a poor fit (Browne & Cudeck, 1993). The CFI reflects the degree to which an independent model matches the observed data, with values greater than .95 indicating an acceptable fit and values greater than or equal to .97 indicating a good fit (Schermelleh-Engel, Moosbrugger, & Müller, 2003). The TLI/NNFI is based on a comparison of a null model with the hypothesized model, with indexes greater than .95 indicating an acceptable fit and values greater than .97 indicating a good fit (Schermelleh-Engel et al.).
Results
Examining Normality
First, variables were examined for normality of distribution. The social-strain sub-scales (hostility/impatience, insensitivity, interference, and ridicule) were highly skewed such that nearly all participants reported low social strain. A log 10 transformation of the strain subscales yielded greater similarity to the normal curve, so these transformed strain subscales were used in all further analyses. All other variables in the analyses were normally distributed.
Next, bivariate correlation analyses were conducted between variables (see Tables 2–4). Based on patterns of correlation, in subsequent models we controlled for the following demographic variables: marital status, education, gender, income, duration of OA, severity of OA symptoms, pain, physical disability, and mode of survey administration (paper vs. computer).
Table 2. Bivariate Correlations Between All Variables (N = 160), Part 1 of 3.
| Variable | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 Age | — | −.12 | −.07 | −.07 | −.04 | −.02 | −.12 | .13 | .10 | .11 | .00 | −.00 |
| 2 Gender | — | −.05 | −.31** | −.06 | −.13 | .15 | .17* | .00 | .07 | −.18* | −.12 | |
| 3 Ethnicity | — | .14 | .05 | .12 | −.04 | −.00 | .02 | −.12 | −.03 | −.04 | ||
| 4 Marital status | — | .09 | .32** | −.01 | −.13 | −.08 | −.20* | .23** | .24** | |||
| 5 Education | — | .26** | .02 | −.25** | −.13 | −. 29** | .03 | −.05 | ||||
| 6 Income | — | .08 | −.13 | −.12 | −. 29** | .08 | .04 | |||||
| 7 OA duration | — | .13 | −.09 | .02 | .08 | .09 | ||||||
| 8 Physical disability | — | .59** | .22* | −.19* | −.13 | |||||||
| 9 OA severity | — | .16 | −.24** | −.15 | ||||||||
| 10 Survey mode | — | −.04 | .01 | |||||||||
| 11 Tangible support | — | .72** | ||||||||||
| 12 Affection | — |
Note. OA = osteoarthritis. Gender was dichotomized such that 0 = men, 1 = women; ethnicity was dichotomized such that 0 = White, 1 = other; marital status was dichotomized such that 0 = single/widowed/divorced/separated, 1 = married; education was dichotomized such that 0 = some college or less, 1 = associate's degree or higher; annual income was dichotomized such that 0 = $20,000 or less, 1 = $20,001 or more; duration of OA symptoms was dichotomized such that 0 = 2 years or less, 1 = more than 2 years; survey mode was dichotomized such that 0 = computer administration, 1 = paper-and-pencil administration.
p < .05.
p < .01.
Table 4. Bivariate Correlations Between All Variables (N = 160), Part 3 of 3.
| Variable | 13 | 14 | 15 | 16 | 17 | 18 | 19 | 20 | 21 | 22 | 23 | 24 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 13 positive interaction | — | .84** | .05 | −.22** | −.13 | −.26** | .20* | .19* | .19* | .16 | .18* | .21* |
| 14 Emotional/Informational support | — | −.05 | −.26** | −.17* | −.27** | .22** | .20* | .23** | .16 | .17 | .20* | |
| 15 Hostility/Impatience | — | .64** | .59** | .46** | −.08 | −.05 | −.05 | −.23** | −.24** | −.17 | ||
| 16 Insensitivity | — | .50** | .49** | −.13 | −.02 | −.10 | −.23** | −.23** | −.20* | |||
| 17 Interference | — | .52** | −.05 | −.05 | −.12 | −.12 | −.18* | −.13 | ||||
| 18 Ridicule | — | −.04 | −.08 | −.11 | −.13 | −.18* | −.11 | |||||
| 19 Exercise self-efficacy | — | .59** | .61** | .73** | .56** | .45** | ||||||
| 20 Attitudes about exercise | — | .73** | .41** | .52** | .40** | |||||||
| 21 Control over exercise | — | .46** | .43** | .56** | ||||||||
| 22 Time 2 exercise self-efficacy | — | .67** | .56** | |||||||||
| 23 Time 2 attitude about exercise | — | .54** | ||||||||||
| 24 Time 2 control over exercise | — |
Note. Gender was dichotomized such that 0 = men, 1 = women; ethnicity was dichotomized such that 0 = White, 1 = other; marital status was dichotomized such that 0 = single/widowed/divorced/separated, 1 = married; education was dichotomized such that 0 = some college or less, 1 = associate's degree or higher; annual income was dichotomized such that 0 = $20,000 or less, 1 = $20,001 or more; duration of osteoarthritis symptoms was dichotomized such that 0 = 2 years or less, 1 = more than 2 years; survey mode was dichotomized such that 0 = computer administration, 1 = paper-and-pencil administration.
p < .05.
p < .01.
Hypothesized Structural Equation Model: Cross-Sectional Analysis
We first examined the hypothesized cross-sectional model (see Figure 2) in which Time 1 social support and Time 1 social strain predicted Time 1 exercise self-efficacy. To control for the effects of chance when conducting multiple significance tests simultaneously, we adopted the false-discovery-rate method (Benjamini & Hochberg, 1995; Keselman, Cribbie, & Holland, 1999) for determining the statistical significance of a path coefficient. In accordance with others who have applied this method to structural equation modeling (Lackner, Jaccard, & Blanchard, 2004), a family of tests was defined as the path coefficients leading from the exogenous variables to a given endogenous variable. The hypothesized model yielded a moderate fit to the data: χ2(178, N = 160) = 264.57, p < .01; RMSEA = .06; CFI = .92; TLI = .90 (attempts to improve model fit did not result in significantly different fit statistics). In the cross-sectional model, 6.2% of the variance in Time 1 exercise self-efficacy was explained. Time 1 social support had a significant influence on Time 1 exercise self-efficacy (β = .23, p < .05), suggesting that higher social support is related to higher exercise self-efficacy. Contrary to predictions, however, social strain did not have a significant cross-sectional relationship with exercise self-efficacy (β = −.10, p = ns).
Figure 2.
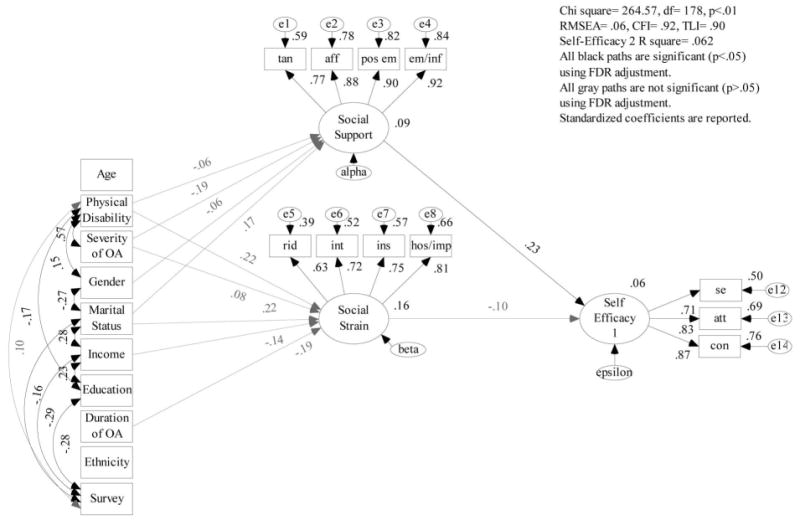
Cross-sectional structural equation model in which higher social support predicts higher exercise self-efficacy. Note. Gender was dichotomized such that 0 = men, 1 = women; ethnicity was dichotomized such that 0 = White, 1 = other; marital status was dichotomized such that 0 = single/widowed/divorced/separated, 1 = married; education was dichotomized such that 0 = some college or less, 1 = associate's degree or higher; annual income was dichotomized such that 0 = $20,000 or less, 1 = $20,001 or more; duration of osteoarthritis symptoms was dichotomized such that 0 = 2 years or less, 1 = more than 2 years; survey mode was dichotomized such that 0 = computer administration, 1 = paper-and-pencil administration.
We next examined the hypothesized longitudinal model (see Figure 3) in which Time 1 social support and Time 1 social strain predicted Time 2 exercise self-efficacy (controlling for Time 1 exercise self-efficacy). Using the false-discovery-rate method, the hypothesized model yielded an adequate fit to the data: χ2(233, N = 160) = 288.64, p < .01; RMSEA = .04; CFI = .96; TLI = .95 (attempts to improve model fit did not result in significantly different fit statistics). The longitudinal model explained 56.3% of the variance in Time 2 exercise self-efficacy. As predicted, social strain had a significant longitudinal influence on exercise self-efficacy (β = −.17, p < .05), suggesting that higher social strain predicts lower exercise self-efficacy a year later, while adjusting for the effect of baseline self-efficacy. Contrary to predictions, however, social support did not have a significant influence on exercise self-efficacy over time (β = .08, p = ns).
Figure 3.
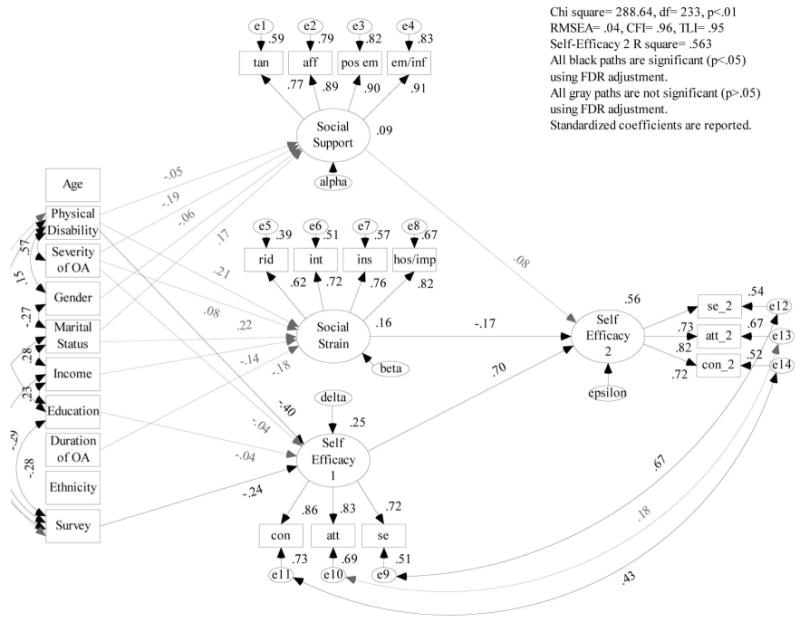
Longitudinal structural equation model in which lower social strain at Time 1 predicts higher exercise self-efficacy 1 year later. Note. Gender was dichotomized such that 0 = men, 1 = women; ethnicity was dichotomized such that 0 = White, 1 = other; marital status was dichotomized such that 0 = single/widowed/divorced/separated, 1 = married; education was dichotomized such that 0 = some college or less, 1 = associate's degree or higher; annual income was dichotomized such that 0 = $20,000 or less, 1 = $20,001 or more; duration of osteoarthritis symptoms was dichotomized such that 0 = 2 years or less, 1 = more than 2 years; survey mode was dichotomized such that 0 = computer administration, 1 = paper-and-pencil administration.
Discussion
The results of the current study suggest two important implications: first, that social strain has an important longitudinal influence on exercise self-efficacy, and second, that health and well-being interventions for older adults with OA could target general social relations.
Importance of Social Support and Social Strain
Consistent with hypotheses, higher baseline reports of social support were related to higher baseline reports of exercise self-efficacy. These results support the wealth of research touting the benefits of social support for health (Cohen, 2004), well-being (Berkman et al., 2000; Heller & Rook, 2001; Seeman, 2000; Walen & Lachman, 2000), and exercise participation (Carron et al., 1996). Most of this previous work, however, did not assess social support concurrently with social strain.
In our cross-sectional structural equation model, we found that baseline reports of social strain were not related to baseline reports of exercise self-efficacy. In the longitudinal model, however, higher reports of baseline social strain significantly predicted reports of lower exercise self-efficacy 1 year later. Baseline reports of social support were not related to reported exercise self-efficacy 1 year later in the longitudinal model.
Our results are consistent with recent work by Newsom, Nishishiba, Morgan, and Rook (2003), who reported that social strain was a more potent longitudinal predictor of psychological outcomes than social support was. Using comparable measures of support and strain, Newsom et al. found that when cross-sectional data were analyzed, data supported a “domain-specific model” in which social support predicted positive affect and social strain predicted negative affect. The current results are consistent with those of Newsom et al., as the positive predictor social support predicted the positive outcome of exercise self-efficacy, whereas the negative predictor social strain had no cross-sectional relationship with the positive outcome exercise self-efficacy.
When Newsom et al. (2003) analyzed longitudinal data (change over 6 weeks), however, they found support for a negativity effect (Rook, 1990), wherein social strain predicted longitudinal outcomes (both positive and negative affect) but social support did not significantly predict either outcome. The current results are consistent with those of Newsom et al., as the negative predictor social strain predicted the positive outcome of exercise self-efficacy, whereas the positive predictor social support had no longitudinal relationship with the positive outcome exercise self-efficacy. Furthermore, the current study extends the findings of Newsom et al. to demonstrate the negativity effect when change is examined over a longer period of time (1 year).
It is possible that social strain is the more powerful and long-lasting predictor of outcomes for older adults with OA, and the scientific community has been focusing interventions on the less powerful and less enduring aspect of social relationships. Previous studies examining social support's longitudinal relationship to health and well-being outcomes that did not control for social strain might have yielded different results had social strain been measured and included in analyses. Future studies should revisit the already investigated relationships of social support to outcomes, controlling for social strain, to confirm or disconfirm this suggestion to make interventions as powerful as possible.
Importance of General Intervention Targets
In addition to demonstrating the importance of social strain as a longitudinal influence on self-efficacy beliefs, the current study also demonstrates an efficacious possibility for intervention reform. Although exercise-specific social relations were not addressed in the current study, interventions that focus on decreasing exercise-specific social strain might be more powerful than interventions focusing on decreasing general social strain for the purpose of increasing exercise self-efficacy and exercise behavior. As already mentioned, however, Lachman and Weaver (1998) argue that the relationships of social and personal predictors with health and well-being using generalized measures would be even more compelling than with the use of domain-specific measures because they would apply to multiple domains of functioning. Previous studies have demonstrated that social strain influences health in several domains (Davis & Swan, 1999; Rook, 1984; Sherman, 2003). In the current study we demonstrated that social strain influences exercise self-efficacy over time. Therefore, if interventions for older adults with OA focus on reducing social strain in relationships they will not only be influencing future exercise self-efficacy, they might also promote other future health behaviors, as well as general well-being.
Limitations and Future Directions
There are some important limitations to the current study. First, participants were mostly White, educated, wealthy, and healthy. These sample characteristics limit the generalizability of our results. If possible, future investigations should examine more representative samples of older adults with OA. Second, all variables were measured with a survey. Therefore, shared method variance might have limited our ability to detect true relationships. This limitation was at least partially controlled through the use of structural equation modeling, however, which takes into account measurement error, allowing for more confident interpretation of the results. Furthermore, as stated previously, enhancing exercise self-efficacy is one of the most effective methods of increasing exercise participation (Bandura, 1997; Jette et al., 1998; McAuley et al., 2003; Rimal, 2001). The current study would have benefited, however, from the inclusion of an objective measure of physical activity behavior to determine whether exercise self-efficacy was an effective proxy for physical activity behavior with this sample. Finally, comparable measures of social support and social strain were not available for the current study. Without similar measures it is difficult to determine the relative influences of support and strain. Thus, future studies should examine these relationships using measures of support and strain with parallel content and equivalent reliability and validity to eliminate bias introduced by differences between questionnaires.
Conclusion
Health and well-being interventions for older adults with OA should focus on improving the quality of social relationships, specifically, decreasing social strain. Not only could this potential improvement positively influence exercise self-efficacy, and possibly exercise participation in turn, but the health and well-being of older adults with OA might also be improved via improved social relationships with others.
Table 3. Bivariate Correlations Between All Variables (N = 160), Part 2 of 3.
| Variable | 13 | 14 | 15 | 16 | 17 | 18 | 19 | 20 | 21 | 22 | 23 | 24 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 Age | −.02 | −.03 | −.03 | −.10 | −.03 | −.03 | −.09 | −.10 | −.07 | −.08 | −.07 | −.13 |
| 2 Gender | −.12 | −.07 | −.13 | .12 | −.09 | −.04 | −.03 | .00 | .01 | −.10 | .00 | −.09 |
| 3 Ethnicity | −.04 | −.11 | −.12 | .01 | .06 | −.08 | −.00 | −.06 | −.03 | .06 | −.07 | −.01 |
| 4 Marital status | .19* | .14 | .21** | .03 | .15 | −.08 | .05 | .04 | .02 | −.05 | .03 | −.17 |
| 5 Education | −.01 | −.03 | .07 | −.03 | .10 | −.08 | .03 | .17* | .12 | .05 | .04 | .07 |
| 6 Income | .04 | .03 | −.02 | −.08 | −.12 | −.25** | −.01 | .08 | .02 | −.00 | .04 | −.04 |
| 7 OA duration | .06 | .09 | −.20* | −.11 | −.10 | −.06 | −.02 | .02 | .05 | .02 | −.03 | .04 |
| 8 Physical disability | −.19* | −.18* | .14 | .21** | .13 | .22** | −.28** | −.38** | −.43** | −.30** | −.33** | −.31** |
| 9 OA severity | −.17* | −.27** | .16* | .15 | .20* | .16 | −.24** | −.25** | −.26** | −.22* | −.24** | −.20* |
| 10 Survey mode | .04 | −.05 | .04 | .08 | .00 | .11 | −.25** | −.26** | −.28** | −.19* | −.15 | −.12 |
| 11 Tangible support | .69** | .69** | .04 | −.25** | −.11 | −.16* | .24** | .16 | .15 | .24** | .26** | .18* |
| 12 Affection | .80** | .81** | .01 | −.27** | −.07 | −.23** | .19* | .12 | .07 | .17 | .14 | .13 |
Note. OA = osteoarthritis. Gender was dichotomized such that 0 = men, 1 = women; ethnicity was dichotomized such that 0 = White, 1 = other; marital status was dichotomized such that 0 = single/widowed/divorced/separated, 1 = married; education was dichotomized such that 0 = some college or less, 1 = associate's degree or higher; annual income was dichotomized such that 0 = $20,000 or less, 1 = $20,001 or more; duration of OA symptoms was dichotomized such that 0 = 2 years or less, 1 = more than 2 years; survey mode was dichotomized such that 0 = computer administration, 1 = paper-and-pencil administration.
p < .05.
p < .01.
Acknowledgments
This research was supported by NIH/NIA grant R03- AG 23322-01 to Dr. Sherman. A portion of this manuscript was presented at the 2006 annual meeting of the Gerontological Society of America, Dallas, TX. We thank Amanda R. Hemmesch, MA, Meghan Walsh, Angie Forgues, Elizabeth Jiang, Abby Reiss, Rio May del Rosario, and Adrienne Skrzypek for their assistance in data collection and data management. We also express appreciation for the contribution of our participants.
Footnotes
There were a few significant differences between responses from paper surveys and responses from computer surveys. Participants who completed paper surveys reported significantly lower exercise self-efficacy, t(35.32) = 2.63, p < .05; significantly lower attitudes about exercise, t(31.06) = 2.22, p < .05; significantly lower beliefs about control over exercise, t(31.87) = 2.45, p < .05; significantly higher physical disability scores, t(35.06) = −2.26, p = .05; significantly lower education, χ2(l) = 13.07, p < .01; and significantly lower income, χ2(l) = 12.75, p < .01, and were significantly less likely to be married, χ2(l) = 6.15, p < .05. Because of these differences, we controlled for survey mode of administration in all analyses.
References
- American College of Sports Medicine. ACSM's guidelines for exercise testing and prescription. Philadelphia: Lippincott Williams & Wilkins; 2000. [Google Scholar]
- Antonucci TC, Akiyama H, Lansford JE. The negative effects of close social relations among older adults. Family Relations. 1998;47:379–384. [Google Scholar]
- Arbuckle JL. Amos 6.0 user's guide. Chicago: SPSS; 2004. [Google Scholar]
- Arthritis Foundation. Osteoarthritis. 2007 Retrieved September 9, 2007, from www.arthritis.org/conditions/DiseaseCenter/oa.asp.
- Bandura A. Self-efficacy: The exercise of control. New York: W.H. Freeman; 1997. [Google Scholar]
- Bassey EJ. The benefits of exercise for the health of older people. Reviews in Clinical Gerontology. 2000;10:17–31. [Google Scholar]
- Benjamini Y, Hochberg Y. Controlling the false discovery rate: A practical and powerful approach to multiple testing. Journal of the Royal Statistical Society: Series B. 1995;57:289–300. [Google Scholar]
- Berkman LF, Glass T, Brissette I, Seeman TE. From social integration to health: Durkheim in the new millennium. Social Science and Medicine (1982) 2000;51:843–857. doi: 10.1016/s0277-9536(00)00065-4. [DOI] [PubMed] [Google Scholar]
- Boomsma A. Reporting analysis of covariance structures. Structural Equation Modeling. 2000;7:461–483. [Google Scholar]
- Brassington GS, Atienza AA, Perczek RE, DiLorenzo TM, King AC. Intervention-related cognitive versus social mediators of exercise adherence in the elderly. American Journal of Preventive Medicine. 2002;23:80–86. doi: 10.1016/s0749-3797(02)00477-4. [DOI] [PubMed] [Google Scholar]
- Browne MW, Cudeck R. Alternative ways of assessing model fit. In: Bollen KA, Long JS, editors. Testing structural equation models. Newbury Park, CA: Sage; 1993. pp. 136–162. [Google Scholar]
- Byrne BM. Structural equation modeling with LISREL, PRELIS, and SIMPLIS: Basic concepts, applications, and programming. Mahwah, NJ: Lawrence Erlbaum; 1998. [Google Scholar]
- Carron AV, Hausenblas HA, Mack D. Social influence and exercise: A meta-analysis. Journal of Sport & Exercise Psychology. 1996;18:1–16. [Google Scholar]
- Chogahara M. A multidimensional scale for assessing positive and negative social influences on physical activity in older adults. The Journals of Gerontology. Series B, Psychological Sciences and Social Sciences. 1999;54:S356–S367. doi: 10.1093/geronb/54b.6.s356. [DOI] [PubMed] [Google Scholar]
- Chogahara M, O'Brien Cousins S, Wankel LM. Social influences on physical activity in older adults: A review. Journal of Aging and Physical Activity. 1998;6:1–17. [Google Scholar]
- Cohen S. Social relationships and health. The American Psychologist. 2004;59:676–684. doi: 10.1037/0003-066X.59.8.676. [DOI] [PubMed] [Google Scholar]
- Davis MC, Swan PD. Association of negative and positive social ties with fibrinogen levels in young women. Health Psychology. 1999;18:131–139. doi: 10.1037//0278-6133.18.2.131. [DOI] [PubMed] [Google Scholar]
- Ettinger WH, Burns R, Messier SP, Applegate W, Rejeski WJ, Morgan T, et al. A randomized trial comparing aerobic exercise and resistance exercise with a health education program in older adults with knee osteoarthritis. The Fitness Arthritis and Seniors Trial (FAST) Journal of the American Medical Association. 1997;277:25–31. [PubMed] [Google Scholar]
- Felson DT, Zhang YQ. An update on the epidemiology of knee and hip osteoarthritis with a view to prevention. Arthritis and Rheumatism. 1998;41:1343–1355. doi: 10.1002/1529-0131(199808)41:8<1343::AID-ART3>3.0.CO;2-9. [DOI] [PubMed] [Google Scholar]
- Heller K, Rook KS. Distinguishing the theoretical functions of social ties: Implications for support interventions. In: Sarason BR, Duck S, editors. Personal relationships: Implications for clinical and community psychology. Chichester, England: John Wiley & Sons; 2001. pp. 119–139. [Google Scholar]
- Hirvensalo M, Heikkinen E, Lintunen T, Rantanen T. Recommendations for and warnings against physical activity given to older people by health care professionals. Preventive Medicine. 2005;41:342–347. doi: 10.1016/j.ypmed.2004.11.020. [DOI] [PubMed] [Google Scholar]
- Hughes SL, Seymour RB, Campbell R, Pollak N, Huber G, Sharma L. Impact of the Fit And Strong Intervention on older adults with osteoarthritis. The Gerontologist. 2004;44:217–228. doi: 10.1093/geront/44.2.217. [DOI] [PubMed] [Google Scholar]
- Jette AM, Rooks D, Lachman M, Lin TH, Levenson C, Heislein D, et al. Home-based resistance training: Predictors of participation and adherence. The Gerontologist. 1998;38:412–421. doi: 10.1093/geront/38.4.412. [DOI] [PubMed] [Google Scholar]
- Keselman HJ, Cribbie R, Holland B. The pairwise multiple comparison multiplicity problem: An alternative approach to familywise and comparisonwise Type I error control. Psychological Methods. 1999;4:58–69. [Google Scholar]
- Lachman ME, Weaver SL. The sense of control as a moderator of social class differences in health and well-being. Journal of Personality and Social Psychology. 1998;74:763–773. doi: 10.1037//0022-3514.74.3.763. [DOI] [PubMed] [Google Scholar]
- Lackner JM, Jaccard J, Blanchard EB. Testing the sequential model of pain processing in irritable bowel syndrome: A structural equation modeling analysis. European Journal of Pain (London, England) 2005;9:207–218. doi: 10.1016/j.ejpain.2004.06.002. [DOI] [PubMed] [Google Scholar]
- McAuley E, Jerome GJ, Marquez DX, Elavsky S, Blissmer B. Exercise self-efficacy in older adults: Social, affective, and behavioral influences. Annals of Behavioral Medicine. 2003;25:1–7. doi: 10.1207/S15324796ABM2501_01. [DOI] [PubMed] [Google Scholar]
- Newsom JT, Nishishiba M, Morgan DL, Rook KS. The relative importance of three domains of positive and negative social exchanges: A longitudinal model with comparable measures. Psychology and Aging. 2003;18:746–754. doi: 10.1037/0882-7974.18.4.746. [DOI] [PubMed] [Google Scholar]
- Resnick B, Orwig D, Magaziner J, Wynne C. The effect of social support on exercise behavior in older adults. Clinical Nursing Research. 2002;11:52–70. doi: 10.1177/105477380201100105. [DOI] [PubMed] [Google Scholar]
- Rimal RN. Longitudinal influences of knowledge and self-efficacy on exercise behavior: Tests of a mutual reinforcement model. Journal of Health Psychology. 2001;6:31–46. doi: 10.1177/135910530100600103. [DOI] [PubMed] [Google Scholar]
- Rook KS. The negative side of social interactions: Impact on psychological well-being. Journal of Personality and Social Psychology. 1984;46:1097–1108. doi: 10.1037//0022-3514.46.5.1097. [DOI] [PubMed] [Google Scholar]
- Rook KS. Stressful aspects of older adults' social relationships: Current theory and research. In: Stephens MAP, Crowther JH, Hobfall SE, Tennenbaum DL, editors. Stress and coping in later life. Washington, DC: Hemisphere; 1990. pp. 157–169. [Google Scholar]
- Rook KS. Emotional health and positive versus negative social exchanges: A daily diary analysis. Applied Developmental Science. 2001;5:86–97. [Google Scholar]
- Rook KS, Pietromonaco PR. Close relationships: Ties that heal or ties that bind? In: Jones WH, Perlman D, editors. Advances in personal relationships. Greenwich, CT: JAI Press; 1987. pp. 1–35. [Google Scholar]
- Ruehlman LS, Karoly P. With a little flak from my friends: Development and preliminary validation of the Test of Negative Social Exchange (TENSE). Psychological assessment. Journal of Consulting and Clinical Psychology. 1991;3:97–104. [Google Scholar]
- Schermelleh-Engel K, Moosbrugger H, Müller H. Evaluating the fit of structural equation models: Tests of significance and descriptive goodness-of-fit measures. Methods of Psychological Research. 2003;8:23–74. [Google Scholar]
- Seeman TE. Health promoting effects of friends and family on health outcomes in older adults. American Journal of Health Promotion. 2000;14:362–370. doi: 10.4278/0890-1171-14.6.362. [DOI] [PubMed] [Google Scholar]
- Sherbourne CD, Stewart AL. The MOS social support survey. Social Science & Medicine. 1991;32:705–714. doi: 10.1016/0277-9536(91)90150-b. [DOI] [PubMed] [Google Scholar]
- Sherman AM. Social relations and depressive symptoms in older adults with knee osteoarthritis. Social Science & Medicine. 2003;56:247–257. doi: 10.1016/s0277-9536(02)00023-0. [DOI] [PubMed] [Google Scholar]
- Vuori IM. Dose-response of physical activity and low back pain, osteoarthritis, and osteoporosis. Medicine and Science in Sports and Exercise. 2001;33:S551–S586. doi: 10.1097/00005768-200106001-00026. [DOI] [PubMed] [Google Scholar]
- Walen HR, Lachman ME. Social support and strain from partner, family, and friends: Costs and benefits for men and women in adulthood. Journal of Social and Personal Relationships. 2000;17:5–30. [Google Scholar]