

Abstract
This study examined the extent to which perceptions of partner suffering mediate the association between attachment insecurity (anxiety and avoidance) and personal distress among spouses of older adults with osteoarthritis. Fifty-three spouses watched two videos of targets (their partner and an opposite sex stranger) perform a pain-eliciting household task, and spouses were asked to rate their own distress and perceptions of the targets’ pain. Spouses also completed self-report measures of trait attachment. Results revealed that attachment anxiety was associated with greater personal distress in reaction to the partner’s suffering, and heightened perceptions of partner pain mediated this association. Avoidant attachment was associated with less distress in reaction to the partner’s suffering, but not with less perceived pain. The results of this study identify an important mechanism linking attachment insecurity and heightened distress responses when observing the suffering of a significant other.
Keywords: attachment, caregiving, emotion, older adults, osteoarthritis
In close relationships, there are times when people are faced with their partners’ suffering. Being in a relationship often involves witnessing a loved one get sick, receive bad news, or fail to accomplish important goals. In these circumstances, most people feel some amount of personal distress along with compassion and typically offer support to their partners. Others are more likely to feel overwhelmed by their own distress, impeding their ability to provide support to their partners.
Attachment theory provides a useful framework for identifying individuals who are at a greater risk for feeling personal distress in the face of their partners’ suffering because it identifies individual differences in peoples’ ability to regulate emotions and to maintain felt security (e.g. Bretherton, 1985; Kobak & Sceery, 1988). Past studies have shown that attachment insecurity is predictive of personal distress in response to partners’ vulnerability in experimental settings (Mikulincer, Gillath, Halevy, Avihou, Avidan, & Eshkoli, 2001; Westmaas & Silver, 2001) and in the context of caregiving (Braun, Mikulincer, Rydall, Walsh, & Rodin, 2007; Crispi, Schiaffino, & Berman, 1997; Daire, 2002; Markiewicz, Reis, & Gold, 1997). Studies consistently show that anxious attachment is associated with greater personal distress, consistent with theory that anxiously attached individuals are egoistically self-involved (Collins & Read, 1994; Mikulincer et al., 2001). However, findings for avoidant attachment are less clear. Some studies show that avoidant attachment is associated with increased distress (e.g., Braun et al., 2007), whereas others find no significant associations (e.g., Mikulincer et al., 2001). Both patterns are inconsistent with theory asserting that avoidant individuals report less distress (e.g., Fraley & Shaver, 1997). Inconsistency in findings may be due to differences in the degree to which the situation is threatening (Mikulincer & Florian, 2001). For example, Braun and colleagues’ (2007) study involved caregivers of cancer patients, a particularly threatening context in which there is knowledge of a loved one’s impending death and/or separation; Mikulincer and colleagues’ (2001) study, however, asked participants to remember a situation “in which they witnessed the plight of another person”, a less threatening context. Differences may also be due to the degree to which the context is chronically stressful.
In the present study we examine spouses of older adults with osteoarthritis (OA), a context in which spouses are faced with a partner’s pain and disability on a daily basis. Based on past research and theory, we hypothesize that people high in attachment anxiety will be more likely to feel personally distressed by their partner’s suffering than people low in attachment anxiety (hypothesis 1a), and people high in avoidant attachment will be less likely to feel personally distressed by their partners’ suffering than people low in avoidant attachment (hypothesis 1b). Because the present context is less threatening than the context examined in Braun and colleagues’ study but is more chronically stressful than the context examined in Mikulincer and colleagues’ study, our hypothesis regarding avoidant attachment is based on theory.
Another aim of the present study is to test a possible mechanism for the associations between attachment insecurity and distress reactions to partners’ suffering. We hypothesize that one reason attachment insecurity is differentially related to personal distress is due to perceptions of partners’ suffering. Research has shown that individuals high in attachment anxiety are hyper-vigilant to signs of vulnerability in others (Fraley, Niedenthal, Marks, Brumbaugh, & Vicary, 2006). According to attachment theory there are a number of possible reasons for this. One is that people high in attachment anxiety are sensitive to signs of threat in the environment that activate the attachment system (Bowlby, 1973). A partner’s vulnerability may be threatening because anxious individuals do not feel they can cope with negative emotions in general (Pietromonaco, Feldman Barrett, & Powers, 2006) or because the vulnerability signals that the partner is temporarily unavailable to provide care to the anxiously attached person. Another possible reason for anxiously attached individuals’ hyper-vigilance is that vulnerability offers an opportunity for increased intimacy, which is a primary motivating factor for anxious individuals (Shaver & Mikulincer, 2003). In contrast, research and theory suggest that avoidant individuals direct their attention away from cues in the environment that make attachment needs salient (Fraley & Shaver, 1997; Mikulincer & Shaver, 2003). As a result, they should be less likely to perceive their partners’ suffering. Thus, we hypothesize that people high in attachment anxiety will be more likely (hypothesis 2a) and people high in avoidant attachment will be less likely (hypothesis 2b) to perceive that their partners are suffering, and that perceptions of suffering will mediate the associations between attachment anxiety and distress (hypothesis 3a) and avoidant attachment and distress (hypothesis 3b).
Method
Participants
Fifty-three care recipients with OA and their caregiving spouses participated as part of a larger study (Monin, Schulz, Martire, Jennings, Lingler, & Greenberg, 2010). See Table 1 for characteristics of the sample. In order to be eligible to participate, care recipients had to be over 45 years old, have experienced pain of at least moderate intensity over the past month, had difficulty with at least one Instrumental Activity of Daily Living (IADL), and received assistance from the caregiver with at least one IADL. Participants had to meet a standard criterion (i.e., at least 7 out of 10 items answered correctly) for cognitive functioning as measured by the Short Portable Mental Status Questionnaire (Pfeiffer, 1975).1
Table 1.
Characteristics of the Sample
| Care Recipient | Caregiver | |||
|---|---|---|---|---|
| Characteristic | N | % | N | % |
| Gender | ||||
| Female | 26a | 50 | 26 | 49 |
| Male | 26 | 50 | 27 | 51 |
| Education | ||||
| < High school | 2 | 3.8 | 3 | 6 |
| High school | 12 | 23.1 | 11 | 21 |
| More than HS | 38 | 73.1 | 39 | 73 |
| Employment | ||||
| Employed | 12 | 23 | 15 | 38 |
| Homemaker | 6 | 11 | 4 | 7 |
| Retired | 32 | 60 | 32 | 60 |
| Unemployed | 2 | 4 | 2 | 4 |
| Race | ||||
| White | 44 | 83 | 44 | 83 |
| AA | 6 | 11 | 6 | 11 |
| Other | 2 | 4 | 3 | 6 |
| Incomeb | ||||
| < $20,000 | 7 | 14 | ||
| $20,000 – $39,999 | 16 | 32 | ||
| $40,000 – $59,999 | 8 | 16 | ||
| > $60,000 | 19 | 38 | ||
Note.
Twenty seven female care recipients participated in the study; however, one participant chose not to complete the questionnaires.
We include the caregiver’s report of the couple’s combined household income only. Three caregivers refused to report income.
Preparation of Stranger Stimuli
Prior to the study, two standardized videos were made of one older male and one older female “stranger” (that met the same requirements as the care recipients and were not known to caregivers in the study) expressing pain while performing a log carrying task. In the task, the “stranger” loaded two 5-lb artificial logs into a leather carrier, carried the logs across an 8 ft space, unloaded each log from the carrier, and repeated the process for 3 minutes. This task is similar to those used in previous research on participants with OA and their spouses to elicit pain expression (Martire et al., 2006; Romano et al., 1991). The “stranger” was instructed to freely express pain verbally and nonverbally as they experienced it. Caregivers later watched the video of the opposite sex “stranger” in one condition of the experimental session. These videos served as control stimuli in testing our hypotheses that attachment insecurity uniquely impacts caregivers’ personal distress in reaction to the perceived suffering of a spouse (an attachment figure).
Procedure: The Experimental Session
Videotaping the care recipient perform the pain-eliciting log task. Each couple came to the laboratory for a two hour session. After introductions and consent, the experimenter escorted the caregiver to a waiting room. Meanwhile the care recipient was videotaped while performing the pain-eliciting task (see details of the task in the previous section) in a separate area of the laboratory. The caregiver was not present during the care recipient’s performance of the task; however, care recipients were told during the introduction that their video would be shown to the caregiver.
Because it was not possible to exactly match the stranger and partner conditions in terms of the objective amount of pain expressed, we examined overall differences in pain expression between the stranger and partner videos using independent observers. Ten independent observers rated the pain expression of one of the stranger videos and one of 10 randomly selected care recipient videos on a scale from 0 (no pain) to 10 (pain as bad as could be). Raters were not aware of which videos were of strangers and which were of actual participants. According to the observers, more pain was expressed in the stranger videos (M=4.60, SD=2.01) than in the partner videos (M=2.45, SD=2.50; t(9)=3.04, p<.05; Cohen’s d=.95).
Exposure to care recipient’s and stranger’s pain. After the care recipient was videotaped, the caregiver watched the care recipient’s video as well as the video of the opposite sex stranger. The order in which caregivers watched the care recipient and stranger videos was counterbalanced.
Caregivers’ ratings of personal distress. Immediately after watching each of the videos, caregivers were asked to rate the extent to which they experienced a series of distressed feelings (4 items: disturbed, uneasy, distressed, and troubled) while watching the videos on a scale from 1 (not at all) to 7 (extremely; Eisenberg et al., 1989). These items were embedded in a list with other adjectives not relevant to the present study hypotheses. The ratings for each distress-related adjective were averaged to create a composite measure of personal distress (α=.90 for the stranger video and α=.96 for the care recipient video). See Table 2 for descriptive statistics for caregivers’ ratings of personal distress as well as for all other study variables. Caregivers’ distress in reaction to the spouses’ pain (M=2.69, SD=1.85) was significantly higher than caregivers’ distress in reaction to the strangers’ pain (M=2.10, SD=1.25; t(51)=2.62, p<.05; Cohen’s d= .37).
Table 2.
Descriptive Statistics for Caregiver Attachment Dimensions, Potential Covariates, and Outcomes
| Variable | M | SD | Range |
|---|---|---|---|
| CG attachment anxiety | 2.58 | 1.38 | 1–7 |
| CG attachment avoidance | 2.50 | 1.36 | 1–7 |
| CG marital satisfaction | 92.54 | 13.60 | 47–111 |
| CG IADL support | 7.35 | 4.45 | 0–16 |
| CG co-morbidity | 4.28 | 1.99 | 0–11 |
| CR co-morbidity | 5.71 | 2.85 | 1–13 |
| CG distress when watching spouse’s pain eliciting task | 2.10 | 1.25 | 1–7 |
| CG distress when watching stranger’s pain eliciting task | 2.69 | 1.85 | 1–6 |
| CG rating of spouse pain | 46.11 | 20.82 | .66–92.83 |
| CG rating of stranger pain | 44.36 | 27.07 | 3.97–76.21 |
| CR pain own rating | 33.47 | 21.24 | 1.74–70.30 |
Note. CG= caregiver; CR= care recipient
Caregivers’ and care recipients’ continuous ratings of the targets’ pain. While watching the videos of the partner and the opposite sex stranger perform the log carrying task, caregivers continuously rated how much pain they felt the target was experiencing on a visual analogue scale using a personal computer. Care recipients also watched their own video and rated their own pain. They moved the cursor on the scale by turning a rating dial. Each second, a computer program recorded the position of the cursor on the scale. The end points of the scale were labeled 0 (no pain) to 100 (pain as bad as it can be). Scores were calculated by averaging the position on the scale over the 180 seconds. Caregivers’ ratings of the spouses’ (M=44.36, SD=27.07) and strangers’ (M=46.11, SD=20.82) pain were not significantly different from each other (t(48)=.53, ns). Care recipients’ self reported pain (M=33.47, SD=21.24) was significantly lower than caregivers’ perceptions of care recipients’ pain (M=44.36, SD=27.07; t(49)=3.01, p<.01; Cohen’s d= .45).
Caregivers’ Attachment Style
While the care recipient performed the log carrying task, caregivers completed a modified 12-item version of the Experiences in Close Relationships Scale (ECR; Brennan, Clark & Shaver, 1998). The ECR assesses two dimensions of adult attachment: attachment-related avoidance (e.g. “I don’t feel comfortable opening up to others,” α=.89) and anxiety (e.g. “I worry about being alone,” α=.87). Participants responded to each item using a 7-point scale ranging from 1 (disagree strongly) to 7 (agree strongly), and means were calculated for each dimension. The correlation between anxiety and avoidance was r(52)=.67, p<.001. 2
Results
Preliminary Analyses
First we examined the extent to which caregivers’ attachment dimensions were associated with possible covariates. We found that age was inversely related to attachment anxiety and avoidant attachment (r(52)=−.32, p<.05 and r(52)=−.29, p<.05, respectively). There was also a significant main effect of task order predicting pain, such that watching the stranger first resulted in greater perceptions of pain across the two conditions (b=14.07, SE=6.03, t(50)=2.33, p<.05).3 Thus, in all regression models, we control for age and task order. Marital satisfaction, IADL support, co-morbidity, care recipients’ self reported pain, and task order × type were not significantly correlated with attachment style.
Distress
Because this was a repeated measures design and we had ratings of distress in two tasks, we generated a level 1 variable representing distress, a level 2 variable representing task type (partner vs. stranger), and we conducted multi-level analyses using PROC-MIXED in SAS. As shown in Model 1 of Table 3, there was a significant interaction between attachment anxiety and task type predicting distress, as predicted (hypothesis 1a). Follow-up analyses revealed that attachment anxiety was significantly associated with more distress in the partner task (B= .64, SE=.21, t(42)=2.98, p<.01), but not in the stranger task (B= .04, SE=.21, t(42)=.20, p=.84; see Figure 1). Also, consistent with hypothesis 1b, the interaction between avoidant attachment and task was significant, such that avoidance was associated with less distress in reaction to the partner task (B= −.14, SE=.24, t(42)=−.06, p=.56) but more distress in reaction to the stranger task (B= .29, SE=.24, t(42)=1.23, p=.23; see Figure 2).
Table 3.
Steps for Mediated Moderation in Multilevel Analyses: Caregivers’ Perceptions of Partner Pain Mediate the Association between Attachment Anxiety × Task Type and Personal Distress
| estimate | SE | df | t | |
|---|---|---|---|---|
| Model 1: Attachment dimensions × Task type → Personal distress | ||||
| Intercept | 1.26 | 1.47 | 44 | .86 |
| Age | .00 | .02 | 44 | .08 |
| Task type | .48 | .21 | 43 | 2.31* |
| Task order | −.28 | .42 | 44 | −.68 |
| Attachment anxiety | .05 | .21 | 43 | .22 |
| Avoidant attachment | .28 | .23 | 44 | 1.23 |
| Attachment anxiety × avoidant attachment | −.18 | .09 | 43 | −1.90 |
| Attachment anxiety × task type | .60 | .20 | 43 | 3.02** |
| Avoidant attachment × task type | −.43 | .21 | 43 | −2.09* |
| Model 2: Attachment dimensions × Task type → Perceived pain | ||||
| Intercept | 44.57 | 23.32 | 44 | 1.91 |
| Age | −.04 | .34 | 44 | −.11 |
| Task type | −2.32 | 2.69 | 43 | −.86 |
| Task order | 13.22 | 6.61 | 44 | 2.00 |
| Attachment anxiety | 1.12 | 3.22 | 43 | .35 |
| Avoidant attachment | 1.06 | 3.52 | 44 | .30 |
| Attachment anxiety × avoidant attachment | .54 | 1.50 | 43 | .36 |
| Attachment anxiety × task type | 5.34 | 2.61 | 43 | 2.04* |
| Avoidant attachment × task type | −1.98 | 2.71 | 43 | −.73 |
| Model 3: Perceived pain → Personal distress | ||||
| Intercept | −.20 | .29 | 47 | −.69 |
| Perceived pain | .04 | .01 | 47 | 6.51** |
| Model 4: Attachment dimensions × Task type (controlling for perceived pain) → Personal distress | ||||
| Intercept | 1.18 | 1.00 | 44 | 1.19 |
| Age | .00 | .01 | 44 | .22 |
| Task type | .58 | .19 | 42 | 2.99** |
| Task order | −.84 | .29 | 44 | −2.90** |
| Attachment anxiety | .00 | .16 | 42 | −.06 |
| Avoidant attachment | .25 | .17 | 44 | 1.44 |
| Attachment anxiety × avoidant attachment | −.20 | .06 | 42 | −3.18** |
| Attachment anxiety × task type | .38 | .19 | 42 | 2.01 |
| Avoidant attachment × task type | −.35 | .19 | 42 | −1.81 |
| Perceived pain | .04 | .01 | 42 | 7.64** |
Note.
p<.05,
p<.01
Figure 1.
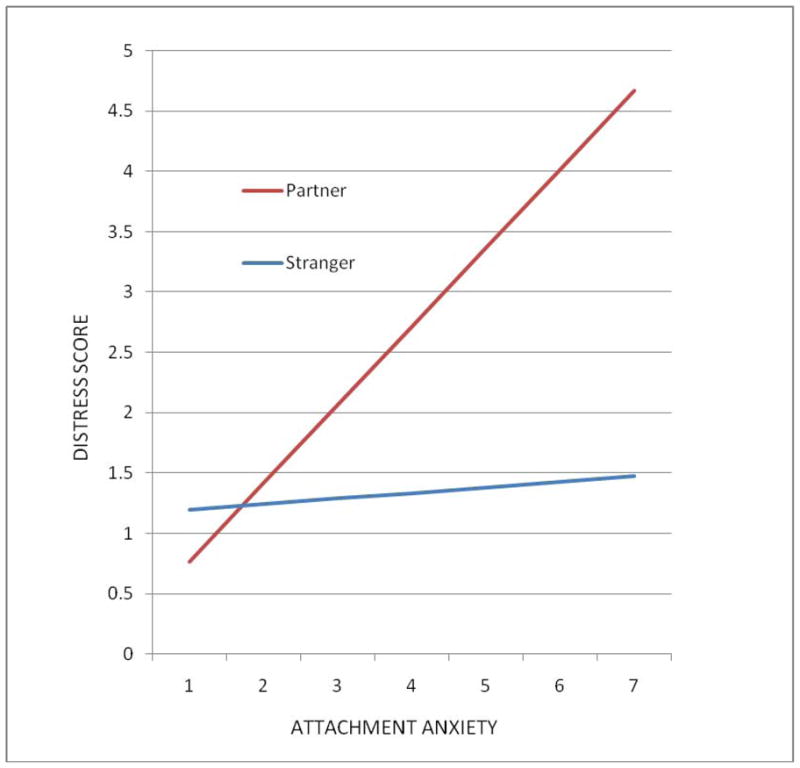
The association between attachment anxiety and distress in reaction to a partner vs. a stranger performing the pain eliciting task.
Figure 2.
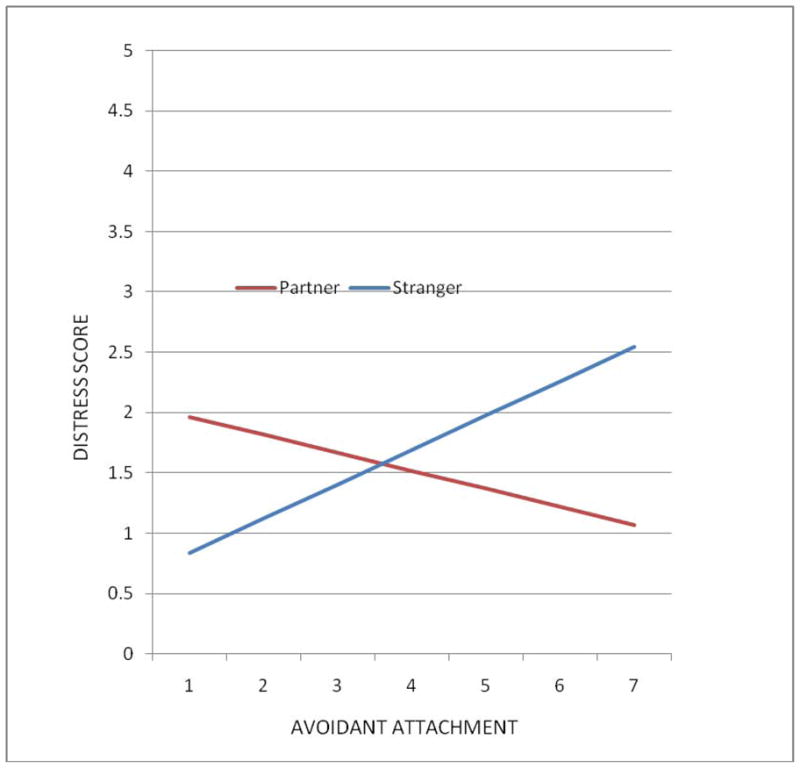
The association between avoidant attachment and distress in reaction to a partner vs. a stranger performing the pain eliciting task.
Perceived suffering
Also as hypothesized (2a), the interaction between attachment anxiety and task type predicting perceived pain was significant (see Model 2 in Table 3). Attachment anxiety was associated with greater perceptions of spouses’ pain (B=6.71, SE=3.32, t(42)=2.02, p<.05) but not strangers’ pain (B=1.00, SE=3.32, t(42)=0.29, p=.78). In contrast to our hypothesis (2b), the interaction between avoidant attachment and task type predicting perceived pain was not significant.
Mediation
To test hypothesis 3a we followed the steps for testing mediated moderation (Baron & Kenny, 1986; Muller, Judd, & Yzerbt, 2005). In addition to showing that the first two necessary conditions for mediation were met (hypotheses 1a and 2a; Models 1 and 2 in Table 3), we showed that (a) perceived pain was associated with distress (Model 3) and (b) including perceived pain as a predictor in the first model decreased the association between the attachment anxiety × task type interaction and distress (Model 4; Sobel test= 1.97, p<.05). Thus, as hypothesized, perceived pain was a significant mediator of the link between attachment anxiety and distress. Because the interaction between avoidant attachment and task type predicting distress was not significant, at least one of the conditions for mediated moderation were not satisfied for hypothesis 3b.
Discussion
The results of our study indicate that attachment anxiety is associated with more distress in reaction to a partner’s suffering. Specifically, caregivers’ attachment anxiety was associated with more distress when watching a partner, but not a stranger, perform a pain-eliciting task. Furthermore, heightened perceptions of partner pain accounted for increased distress. These results are consistent with past research and theory indicating that anxiously attached individuals are hyper-vigilant to signs of other’s suffering (Fraley et al., 2006), and are likely to respond with distress, which may interfere with their ability to provide appropriate support and to feel compassion (Collins & Read, 1994; Feeney & Collins, 2001; Mikulincer et al., 2001).
We also found that attachment avoidance was associated with less distress in reaction to the partner’s suffering, but more distress in response to the stranger’s pain. These findings support previous research on avoidant individuals’ tendency to mask their feelings of distress (Fraley & Shaver, 1997; Mikulincer & Florian, 2001), but only when the partner is an attachment figure. Our results also support the idea that when the context is less threatening (compared to facing death or separation from the partner), avoidant strategies may be effective (Mikulincer & Florian, 2001). Avoidant strategies may also be more influential when there is a chronic stressor.
A limitation of this study is that we had a small and homogeneous sample limiting our power to detect effects and generalize to other groups of people. Also our design only allowed for correlational analyses. Thus, we cannot make unequivocal conclusions about the directions of the effects. In addition to perceptions of suffering influencing distress, it may be that feeling more distress influences perceptions of partners’ suffering. However, this is unlikely considering the results of our mediation analyses.
In conclusion, the results of this study are important because they help identify who as at a greater risk for caregiving burden and the negative health consequences of caregiving. Few studies have focused on relationship-relevant personality factors that predict how caregivers and care recipients cope with the daily effects of suffering. Furthermore, the results of this study identify a mechanism through which attachment insecurity (particularly attachment anxiety) leads to personal distress—heightened perceptions of a partner’s suffering. Finally, and more broadly, this study shows that attachment theory is an important and underutilized tool in understanding relationship processes among older adult spouses.
Acknowledgments
This research was supported in part by grants from the National Institute on Aging, the Pittsburgh Mind Body Center, and the University of Pittsburgh.
We thank Edward P. Lemay, Jr. for his insight regarding statistical analyses.
Footnotes
Due to missing data, our final sample size for the multilevel analyses was 48 couples (Power = 92% for effect size of .5 at alpha = .05).
Caregivers also completed measures of potential covariates (marital satisfaction, IADL support, and co-morbidity).
The main effect of order on distress was not significant (b=−.22, SE=.39, t(51)=−.58, ns), and the interaction between task type and order was not significant for distress (b=.76, SE=0.44, t(46)=1.73, ns) or pain ratings (b=5.79, SE=5.65, t(46)=1.02, ns).
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Contributor Information
Joan K. Monin, University Center for Social and Urban Research, University of Pittsburgh
Richard Schulz, University Center for Social and Urban Research, University of Pittsburgh.
Brooke C. Feeney, Department of Psychology, Carnegie Mellon University
Thomas B. Cook, University Center for Social and Urban Research, University of Pittsburgh
References
- Baron RM, Kenny DA. The moderator-mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. Journal of Personality and Social Psychology. 1986;51(6):1173–1182. doi: 10.1037//0022-3514.51.6.1173. [DOI] [PubMed] [Google Scholar]
- Bradley MM, Lang PJ. Emotion and motivation. In: Cacioppo JT, Tassinary LG, Bertson GG, editors. Handbook of psychophysiology. 3. Cambridge: 2007. pp. 587–589. [Google Scholar]
- Braun M, Mikulincer M, Rydall A, Walsh A, Rodlin G. Hidden morbidity in cancer: Spouse caregivers. Journal of Clinical Oncology. 2007;25(30):4829–4834. doi: 10.1200/JCO.2006.10.0909. [DOI] [PubMed] [Google Scholar]
- Brennan KA, Clark CL, Shaver PR. Self-report measurement of adult attachment: An integrative overview. In: Simpson JA, Rholes WS, editors. Attachment theory and close relationships. New York: Guilford Press; 1998. pp. 46–76. [Google Scholar]
- Bretherton I. Attachment theory: Retrospect and prospect. Monographs of the Society for Research in Child Development. 1985;50(1 & 2):3–35. [PubMed] [Google Scholar]
- Collins NL, Read SJ. Adult attachment, working models, and relationship quality in dating couples. Journal of Personality and Social Psychology. 1990;58:644–663. doi: 10.1037//0022-3514.58.4.644. [DOI] [PubMed] [Google Scholar]
- Crispi EL, Schiaffino K, Berman WH. The contribution of attachment to burden in adult children of institutionalized patients with dementia. The Gerontologist. 1997;37:52–60. doi: 10.1093/geront/37.1.52. [DOI] [PubMed] [Google Scholar]
- Daire AP. The influence of parental bonding on emotional distress in care giving sons for a parent with dementia. The Gerontologist. 2002;42:766–771. doi: 10.1093/geront/42.6.766. [DOI] [PubMed] [Google Scholar]
- Eisenberg N, Fabes RA, Miller PA, Fultz J, Shell R, Mathy RM, Reno RR. Relation of sympathy and personal distress to prosocial behavior: A multimethod study. Journal of Personality and Social Psychology. 1989;57:55–66. doi: 10.1037//0022-3514.57.1.55. [DOI] [PubMed] [Google Scholar]
- Feeney BC, Collins NL. Predictors of caregiving in adult intimate relationships: An attachment theoretical perspective. Journal of Personality and Social Psychology. 2001;80:972–994. [PubMed] [Google Scholar]
- Fraley RC, Niedenthal PM, Marks M, Brumbaugh C, Vicary A. Adult attachment and the perception of emotional expressions: Probing the hyperactivating strategies underlying anxious attachment. Journal of Personality. 2006;74(4):1163–1190. doi: 10.1111/j.1467-6494.2006.00406.x. [DOI] [PubMed] [Google Scholar]
- Fraley RC, Shaver ER. Adult attachment and the suppression of unwanted thoughts. Journal of Personality and Social Psychology. 1997;73:1080–1091. doi: 10.1037//0022-3514.73.5.1080. [DOI] [PubMed] [Google Scholar]
- Katz JN, Chang LC, Sangha O, Fossel AH, Bates DW. Can comorbidity be measured by questionnaire rather than medical record review? Medical Care. 1996;34:73–84. doi: 10.1097/00005650-199601000-00006. [DOI] [PubMed] [Google Scholar]
- Levenson RW. Autonomic nervous system differences among emotions. Psychological Science. 1992;3:23–27. [Google Scholar]
- Locke H, Wallace K. Short marital-adjustment and prediction tests: Their reliability and validity. Marriage and Family Living. 1959;21:251–255. [Google Scholar]
- Martire LM, Keefe FJ, Schulz R, Ready R, Beach SR, Rudy TE, Starz TW. Older spouses’ perceptions of partners’ chronic arthritis pain: Implications for spousal responses, support provision, and caregiving experiences. Psychology and Aging. 2006;21:222–230. doi: 10.1037/0882-7974.21.2.222. [DOI] [PubMed] [Google Scholar]
- Mikulincer M, Florian V. Attachment style and affect regulation implications for coping with stress and mental health. In: Fletcher G, Clark M, editors. Blackwell Handbook of Social Psychology: Interpersonal Processes. Oxford, United Kingdom: Blackwell Publishers; 2001. pp. 537–557. [Google Scholar]
- Mikulincer M, Gillath O, Halevy V, Avihou N, Avidan S, Eshkoli N. Attachment theory and reactions to others’ needs: Evidence that activation of the sense of attachment security promotes empathic responses. Journal of Personality and Social Psychology. 2001;81(6):1205–1224. [PubMed] [Google Scholar]
- Muller D, Judd CM, Yzerbt VY. When moderation is mediated and mediation is moderated. Journal of Personality and Social Psychology. 2005;89(6):852–863. doi: 10.1037/0022-3514.89.6.852. [DOI] [PubMed] [Google Scholar]
- Romano JM, Turner JA, Friedman LS, Bulcroft RA, Jensen MP, Hops H. Observational assessment of chronic pain patient-spouse behavioral interaction. Behavior Therapy. 1991;22:549–568. [Google Scholar]