

Abstract
Background
Physical activity is an essential ingredient in the recipe for successful aging, yet physical activity engagement declines with advancing age.
Methods
In a national sample of 3848 participants aged 32 to 84 (55% women), we examined potential psychosocial moderators of the relationship between age and physical activity.
Results
In a cross-sectional hierarchical multiple regression analysis [Adj. R2 = .14, F(10, 3546) = 57.10, P < .001] we found that participants reporting higher education (β = .08), higher social support (β = .05), higher social strain (β = .12), and a higher sense of control (β = .09) were significantly more physically active. Furthermore, 2 significant interactions showed that higher education and higher social strain were associated with higher physical activity in older adulthood, suggesting that social strain and education may protect against age-related declines in physical activity.
Conclusions
Social strain may positively influence adaptive health promoting behaviors. Potential pathways are considered.
Keywords: aging, social support, social strain, control beliefs, education
Physical activity is an essential ingredient in the recipe for successful aging. Despite the health benefits of physical activity,1 most older adults are not active enough to enjoy these benefits.2 Therefore, it is important to identify psychosocial factors that attenuate the relationship between age and physical activity to identify potential avenues for intervention.
Physical Activity
The Centers for Disease Control and Prevention recommend that adults accumulate at least 30 minutes of moderate aerobic activity on most days of the week or 20 minutes of vigorous aerobic activity 3 days per week, in addition to 2 days of strength training per week.3 Despite these recommendations, at least 50% of American adults did not engage in the recommended levels of physical activity in 2005, and 14% were completely inactive.3 Moreover, more than 24% of American older adults (age 65 and older) were completely inactive, suggesting that physical inactivity increases with age. Thus, it is important to identify factors with the potential to reduce the negative association between age and physical activity to promote health and independence through the life course, especially into the later stages.
Age
Given the physical, emotional, and cognitive benefits of physical activity for adults of all ages,1 it is a concern that so many Americans remain sedentary. Sedentary lifestyle among older adults is of particular concern because sedentary lifestyle is particularly risky for older adults, who are more likely to suffer from chronic illnesses that respond well to physical activity, such as osteoarthritis.1 Despite its benefits, engaging in physical activity is difficult for many adults. For example, many adults report that lack of time, monetary resources, and social support prevents them from engaging in physical activity.4 Among older adults, health problems,5 lack of exercise partners,6 unsafe neighborhoods, inclement weather, lack of transportation, and lack of monetary resources7 are frequently cited as barriers to engaging in regular physical activity. Furthermore, some older adults fear that exercise will cause injury.8 Finally, older adults often assume that physical decline is a natural and inevitable part of the aging process, and therefore have a low sense of control over the physical declines associated with advancing age.9,10
Sense of Control
Lachman et al11 define the sense of control as “beliefs or expectations about the extent to which one's actions can bring about desired outcomes” (p. 254). Maintaining a sense of control in older adulthood is beneficial for both physical and psychological health12 (eg, fewer acute and chronic illnesses, better physical functioning status, lower depressive symptoms, higher life satisfaction). However, older adults experience declines in beliefs in personal control over health and physical functioning with age,9,10,12 manifested as higher perceptions of constraints on the ability to exert personal control.9
Because a lack of belief in control is associated with low motivation for action,13 a low sense of control may be associated with fewer health-promoting behaviors.14 In the context of physical activity, older adults may experience low self-confidence in their ability to engage in exercise, thus avoiding physical activity, and in turn allowing for further physical deterioration.11
Many researchers have found that exercise-specific control, often identified as exercise self-efficacy, is a strong predictor of exercise behavior. In fact, a number of studies examining variables from the contemporary theoretical frameworks describing exercise adoption and maintenance (eg, Social Cognitive Theory,15 Theory of Planned Behavior,16 Transtheoretical Model17) have revealed self-efficacy/perceived behavioral control as the strongest predictor of continued exercise behavior.18
Despite the well-documented association of domain-specific control beliefs and behavior within that domain, little is known about the relationship of more general control beliefs and specific behaviors. Evaluating the impact of these general control beliefs is vital because, as Lachman and Weaver19 argue, the influence of the general sense of control would be even more compelling than the use of domain-specific control because the effects of a general sense of control should apply to multiple domains of functioning. Results examining more generalized control beliefs could impact the focus of interventions, making them broader and less costly, yet more effective at promoting the health and health behaviors of older adults.
Education
One variable that may influence both control beliefs and physical activity is education. In a large national sample of adults, Lachman and Weaver19 found that respondents reporting higher education also reported more mastery and fewer constraints on their perceived control. Furthermore, other studies of large national samples have demonstrated that higher education is associated with greater physical activity.20,21 However, the older cohort tends to be less educated than the younger cohorts.22 Therefore, education may play a more important role in the physical activity of older adults than it does for younger adults.
Social Relations
In addition to education and beliefs about control, social factors such as the quality of social relationships can also impact health and health behaviors.23 Depending on the nature of the social relationship, social influences can promote or undermine behavior change. Social relations can be positive (social support), providing emotional and instrumental assistance, or negative (social strain), providing criticism and hostility.24
Just as the sense of control changes with advancing age, so do social relationships. However, the social environment tends to improve: In a national study of married or cohabiting adults, Walen and Lachman25 found that older adults reported more social support and less social strain from their families than did younger or middle-aged adults. Increases in social support are important for older adults, as social support has been shown to positively affect physical and psychological well-being,25–27 and promote positive health behaviors,23 including exercise.28
Similar to studies of control beliefs on physical activity, most of the research conducted on exercise has investigated the influences of domain-relevant social support (eg, support specifically for exercise behavior), as opposed to general social support. These studies have shown that perceiving social support for exercise predicts exercise self-efficacy.29,30 As described above, general social support has been shown to promote positive health behaviors23 and positively affect physical and psychological well-being,25–27 as well as encourage exercise behavior.28 Thus, general social support is an intervention avenue worthy of exploration.
Social strain, either general or exercise-specific, has not been widely examined in the context of exercise, but may also play an important role in exercise adoption and adherence. Generally, social strain has been shown to negatively affect health and well-being.31–33 More specifically, social strain may predict less confidence in ability to exercise, thus squelching motivation to exercise by making the person feel badly about him or herself. Consistent with this example, Cotter and Sherman34 found that older adults with osteoarthritis who reported more general social strain reported lower exercise self-efficacy 1 year later, suggesting that social strain undermines confidence in exercise abilities.
Alternatively, social strain may serve as a motivator for exercise. For example, Krause, Goldenhar, Liang, Jay and Maeda35 reported that negative social interaction was associated with more frequent exercise among Japanese older adults. The authors argue that informal social sanctions can promote positive health behaviors, an interpretation consistent with the social control literature.36 Social control “refers to interactions that involve influence and regulation”37 (p. 267) either indirectly, through a sense of obligation, or directly, though persuasion. Hughes and Gove38 argue that social control results in better health practices, but also more psychological distress (eg, hostility/anger and sadness/guilt37). As the association between social strain and physical activity has not been investigated in Western samples, the relationship of social strain (either general of exercise-specific) to physical activity requires further investigation.
The Current Study
Previous research has informed our understanding of the benefits of regular physical activity for successful aging. However, we have a limited understanding of the potential moderators of the age-activity relationship. Identifying these moderators may provide insight for interventions, especially when targeted at older adults. Furthermore, social relationships and control beliefs have long been described as important aspects of successful aging and positive health behavior promotion, but the effects of general social relations and control beliefs have not been examined in the context of observational or intervention studies on exercise. Evaluating the impact of these general constructs is vital because they may apply to multiple domains of functioning. Finally, the effects of social strain in the context of exercise behavior are largely unstudied. Thus, the current study examines the relationships of general social support, social strain, and control beliefs to physical activity across the lifespan.
Hypotheses
Consistent with previous research, we predicted that younger age, male gender, higher education,20,21 higher general social support,23 and a higher sense of control11 would be associated with more frequent physical activity. Based on social strain's associations with health and well-being,33 we also predicted that lower general social strain would be associated with more frequent physical activity. Furthermore, we examined the possible moderating effects of gender, race, self-rated health, education, control beliefs, and social relations on age-related differences in physical activity participation to distinguish points of intervention that would help adults to become more active or maintain activity levels across the lifespan.
Method
Data for the current study are from the second wave of the study of Midlife Development in the United States (MIDUS), a national longitudinal investigation of the role of behavioral, psychological, and social factors in age-related differences in physical and mental health.
Participants
Participants were 3848 English-speaking adults ages 32 to 84 (mean = 55.77 years, SD = 12.23), who volunteered to participate in a telephone survey and a self-administered paper-and-pencil questionnaire. Fifty-five percent of participants were women and annual household income ranged from $0 to $300,000 (mean = $78,780.11, SD = $55,073.27). Race was dichotomized such that Caucasians consisted of 1 group (94%) and all other races were combined to create the non-Caucasian group (6%). Education (measured with 12 categories) was also dichotomized such that participants with a high school diploma or lower education consisted of the low-education group (32%), and participants with some college education and higher consisted of the high education group (68%). Seventy-five percent of participants were currently married and/or cohabitating with their partner, while 25% were single, separated, divorced, or widowed and not living with their partner. See Table 1 for a complete description of participant characteristics.
Table 1. Summary of Participant Characteristics (N = 3848).
| Variable | N | % | Variable | N | % |
|---|---|---|---|---|---|
| Gender | Education | ||||
| Male | 1739 | 45.2 | No school/some grade school | 11 | .3 |
| Female | 2109 | 54.8 | 8th grade/junior high school | 47 | 1.2 |
| Race | Some high school | 164 | 4.3 | ||
| White | 3462 | 93.7 | GED | 50 | 1.3 |
| Black | 137 | 3.7 | High school graduation | 975 | 25.4 |
| Native American | 14 | .4 | 1–2 years of college | 656 | 17.1 |
| Asian or Pacific Islander | 22 | .6 | 3 or more years of college | 150 | 3.9 |
| Other | 37 | 1.0 | Associate's degree | 300 | 7.8 |
| Multiracial | 21 | .6 | Bachelor's degree | 761 | 19.8 |
| Marital Status | Some graduate school | 124 | 3.2 | ||
| Married | 2735 | 71.2 | Master's degree | 412 | 10.7 |
| Separated | 53 | 1.4 | Professional degree | 193 | 5.0 |
| Divorced | 482 | 12.5 | Cohabitation with partner | ||
| Widowed | 276 | 7.2 | Living with partner | 140 | 12.6 |
| Never married | 296 | 7.7 | Not living with partner | 969 | 87.4 |
| Variable | N | Range | Mean | SD | |
| Age | 3848 | 32–84 | 55.77 | 12.23 | |
| Income | 3846 | 0–300,000 | 78,780.11 | 55,073.27 | |
| Self-rated physical health | 3847 | 1–5 | 3.57 | 1.00 | |
Measures
Because healthier individuals tend to be more active,39 we controlled for current self-rated health. Self-rated health was measured with 1 item asking participants to rate, on a 5-point scale, “In general, would you say your physical health is excellent (5), very good (4), good (3), fair (2), or poor (1)?” Responses ranged from 1 to 5 (mean = 3.57, SD = 1.00). This single item subjective measure of health has been shown to correspond well to multiple item measures and more objective measures of health.39
Social relations
Were measured as social support (eg, How much does your partner appreciate you?) and social strain (eg, How often does your partner criticize you?) from 3 different sources: the spouse/partner, family, and friends.25 Walen and Lachman reported high reliability for each subscale (α range from .79 to .91).25 Responses to items were averaged, with higher scores reflecting more of the social relation characteristic (possible scores ranged from 1 to 4). Social support scores ranged from 1.25 to 4 (mean = 3.45, SD = .46, α = .84), and social strain scores ranged from 1 to 3.92 (mean = 1.98, SD = .45, α = .84).
Control belief
Were measured with the Mastery and Perceived Constraints scales.40 Prenda and Lachman41 report high reliability for this scale (α = .85). Responses to items were averaged, with higher scores reflecting a higher sense of control (constraints items were reverse-coded). Possible scores ranged from 1 to 7, and scores for the present sample ranged from 1.08 to 7 (mean = 5.53, SD = 1.00, α = .88).
Physical activity
Was measured with 12 items assessing the participant's frequency of vigorous and moderate physical activity in home, work, and leisure settings during both the summer and winter months (see Appendix for complete measure). Leisure-time physical activity was the domain in which participants were most active: 65.0% of participants reported being most active during their leisure time, 24.5% of participants reported being most active at home, and 10.5% of participants reported being most active at work.
As this was a new measure of physical activity, we first examined whether our estimates of physical activity were similar to reports from the Centers for Disease Control and Prevention (CDC; 3). To do this we classified adults who reported moderate and/or vigorous physical activity never, less than once a month, or once a month as “inactive” (29.8%). People who reported physical activity several times a week (thus meeting the CDC's recommendations) were classified as “regularly active” (19.4%), and participants who reported physical activity somewhere in between (once a week, several times a month) were classified as “not regularly active” (50.8%). Our estimates of physical inactivity are slightly higher than reports from the CDC (3), but our measure was less sensitive than the CDC's. For example, we only asked participants to report their activity for the summer and winter months, when they likely reported less activity than they would have reported for the spring and fall months. Therefore, the estimates of physical activity derived from this measure are conservative.
To create a continuous measure of physical activity that would be more amenable to multivariate-statistical analyses than are useful for categorical data, we created an overall physical activity score for both moderate and vigorous activity, and these were combined to create an overall activity score. The respondent's highest moderate physical activity score from either the work, home, or leisure category in the summer months was averaged with the respondent's highest moderate physical activity score from either the work, home, or leisure category in the winter months to create the participants' moderate physical activity score. In this manner, if the participant performed regular moderate activity in the home but not at work or during leisure time, the respondent was still classified as regularly moderately active. An identical procedure was followed to create vigorous physical activity scores. The highest score of these (either moderate or vigorous) was used as the measure of frequency of physical activity. (Moderate and vigorous activity were highly correlated with each other, r = .77, α = .92 for all 12 items). Calculating the physical activity score in this manner yields the best approximation possible to data from the CDC,3 which recommends that adults accumulate at least 30 minutes of moderate aerobic activity on most days of the week or 20 minutes of vigorous aerobic activity 3 days per week. On a six-point scale (0 = never, 5 = several times a week) leisure-time remained the domain in which participants were most frequently active (mean = 2.61, SD = 1.69), followed by home (mean = 2.43, SD = 1.52), followed by job (mean = 1.26, SD = 1.67). Scores for physical activity frequency ranged from 0 to 5 (mean = 3.57, SD = 1.63).
Procedure
Participants were recruited in 1994 and 1995 by Survey Sampling, Inc. using a random digit dialing procedure, which sampled working telephone banks in the coterminous United States (N = 7100).42 Participants were contacted again in 2004 and 2005, when they were 32 to 84 years old, and asked to participate in the second wave of data collection (N = 4967, 69.8% of the Time 1 sample). Comprehensive information regarding physical activity behavior was collected at this time, thus only data from participants who answered these questions in the second wave of data collection were examined in the current study (N = 3848). As is typical of longitudinal survey data, women and participants with higher education and income and better self-rated health were more likely to remain in the study (results available upon request from the first author). Participants were treated in accordance with the ethical standards outlined by the American Psychological Association, through approval by the University Internal Review Board.
Analysis Plan
First, analyses were conducted on all variables to determine normality of the distribution and reliability of measures. Second, zero-order correlations between all variables were calculated (see Table 2). Next, the direct and moderated relationships with physical activity were examined in a Hierarchical Multiple Regression (HMR) analysis, in which the demographic variables age, gender, race, education, and self-rated health were centered and entered into the model in the first step. Psychosocial variables social support, social strain, and control beliefs were centered and entered into the model in the second step, followed by the interaction terms, which were each entered on the final step. All possible two-way interactions with age were examined to determine if factors that are associated with exercise vary by age, which could be used to inform and tailor interventions (age × gender, age × race, age × self-rated health, age × education, age × support, age × strain, age × control beliefs), but only the significant interactions are reported.
Table 2. Correlations Between all Variables (N = 3848).
| Variable | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Gender | — | .05** | −.00 | −.03 | −.07*** | .09*** | .06*** | −.08*** | −.10*** |
| 2 | Race | — | −.06*** | −.04* | -.00 | −.05** | .06*** | −.03 | −.07*** | |
| 3 | Health | — | −.17*** | .23*** | .14*** | −.09*** | .31*** | .20*** | ||
| 4 | Age | — | −.14*** | .09*** | −.23*** | −.06*** | −.27*** | |||
| 5 | Education | — | .05** | .03 | .15*** | .17*** | ||||
| 6 | Support | — | −.37*** | .39*** | .04* | |||||
| 7 | Strain | — | −.29*** | .11*** | ||||||
| 8 | Control | — | .15*** | |||||||
| 9 | Activity | — |
Note.
P ≤ .05,
P ≤ .01,
P ≤ .001.
Gender was dichotomized such that 0 = male and 1 = female; race was dichotomized such that 0 = Caucasian and 1 = other racial background; and education was dichotomized such that 0 = high school graduation or less and 1 = some college or more.
Results
Predictor variables explained 13.6% of the variance in physical activity in the HMR analysis, F(10, 3546) = 57.10, P < .001. Consistent with predictions, younger age (ΔR2 = .04, β = −.22, P < .001, Cohen's f = .05), male gender (ΔR2 = .008, β = −.09, P < .001, Cohen's f = .009), Caucasian race (ΔR2 = .005, β = −.07, P = .001, Cohen's f = .005), higher education (ΔR2 = .006, β = .08, P < .001, Cohen's f = .007), and better self-rated health (ΔR2 = .011, β = .11, P < .001, Cohen's f = .013) were significantly related to more frequent physical activity and explained 11.9% of the variance. Higher social support (ΔR2 = .002, β = .05, P = .006, Cohen's f = .002) and a higher sense of control (ΔR2 = .006, β = .09, P < .001, Cohen's f = .007) were also significantly related to higher physical activity (see Table 3 for complete results). Contrary to predictions, higher (not lower) social strain was significantly related to higher physical activity (ΔR2 = .011, β = .12, P < .001, Cohen's f = .013). The psychosocial variables explained an additional 1.6% of the variance in physical activity.
Table 3. Hierarchical Multiple Regression Analysis Predicting Physical Activity.
| Variable | Step 1 | Step 2 | Step 3 | ||||||
|---|---|---|---|---|---|---|---|---|---|
| B | SE | β | B | SE | β | B | SE | β | |
| Age | −.03 | .00 | −.24*** | −.03 | .00 | −.21*** | −.03 | .00 | −.22*** |
| Gender | −.30 | .05 | −.09*** | −.31 | .05 | −.10*** | −.30 | .05 | −.09*** |
| Race | −.45 | .11 | −.07*** | −.46 | .11 | −.07*** | −.46 | .11 | −.07*** |
| Education | .33 | .06 | .10*** | .29 | .06 | .08*** | .28 | .06 | .08*** |
| Self Rated Health | .22 | .03 | .13*** | .19 | .03 | .11*** | .19 | .03 | .11*** |
| Support | .17 | .06 | .05** | .17 | .06 | .05** | |||
| Strain | .43 | .07 | .12*** | .43 | .06 | .12*** | |||
| Control | .15 | .03 | .09*** | .14 | .03 | .09*** | |||
| Age × Education | .01 | .00 | .04* | ||||||
| Age × Strain | .01 | .01 | .05** | ||||||
| ΔR2 = .119, | ΔR2 = .016, | ΔR2 = .003, | |||||||
| Adj. R2 = .118, | Adj. R2 = .133, | Adj. R2 = .136, | |||||||
| ΔF (5, 3551) = 69.19 | ΔF (3, 3548) = 21.92 | ΔF (2, 3546) = 6.94 | |||||||
Note.
P < .05,
P < .01,
P < .001.
Gender was dichotomized such that 0 = male and 1 = female; race was dichotomized such that 0 = Caucasian and 1 = other racial background; and education was dichotomized such that 0 = high school graduation or less and 1 = some college or more.
In addition to direct relationships with physical activity, the interaction terms of age and education (ΔR2 = .001, β = .04, P = .03, Cohen's f = .001) and age and social strain (ΔR2 = .002, β = .05, P = .003, Cohen's f = .002) were significantly related to physical activity, and explained an additional .3% of the variance. As shown in Figure 1a, there are main effects for age and education, such that younger age and higher education are related to more frequent physical activity. However, education moderates the relationship of age and physical activity, such that having some college education is associated with higher physical activity frequency among older adults than having less education. Similarly, as shown in Figure 1b, social strain moderates the relationship of age to physical activity, such that having more social strain is related to more frequent physical activity among older adults than having less social strain. These results suggest that higher education and higher social strain may be protective against age-related declines in physical activity. (A post hoc three-way interaction between age, education, and social strain was examined, but did not significantly predict physical activity).
Figure 1.
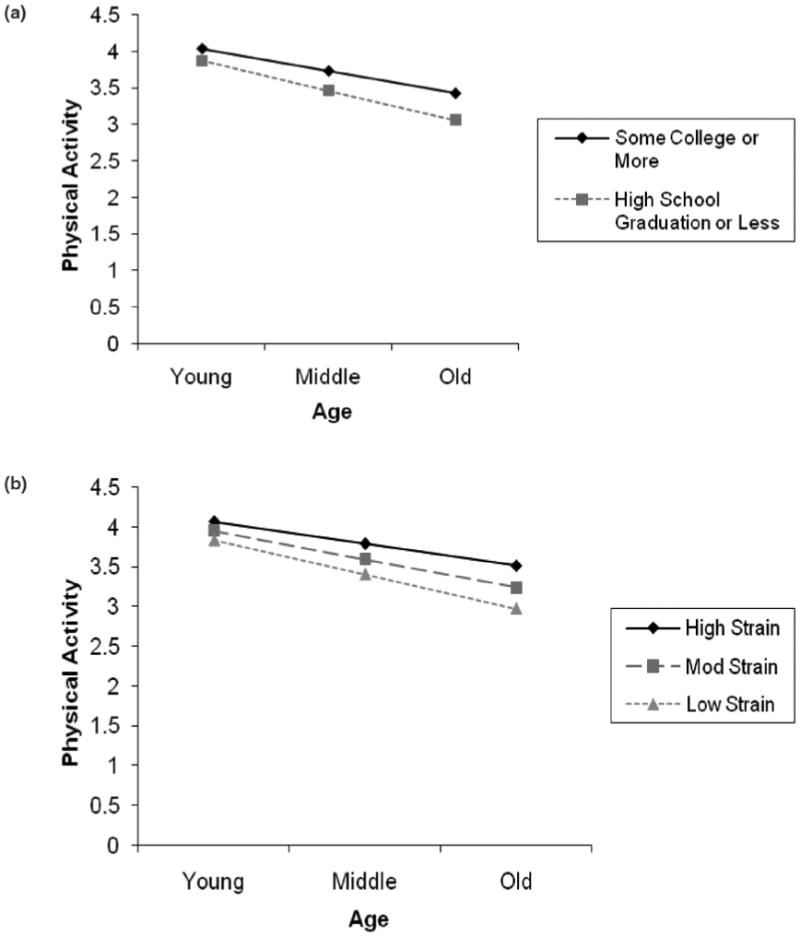
(a) The Interaction of Age and Education on Physical Activity (0–5 scale). (b) The Interaction of Age and Social Strain on Physical Activity (0–5 scale).
Discussion
Consistent with previous studies examining physical activity,3,20,21 the present investigation confirmed that older age, female gender, racial minority status, lower education, and worse self-rated health are related to less frequent physical activity. The current study also expands on previous literature to demonstrate that a higher sense of control, more social support, and more social strain are related to more physical activity. Finally, the present investigation reveals that the relationship of age and physical activity is moderated by education and social strain, such that having higher education and having higher social strain may protect against age-related declines in physical activity participation.
Age
Consistent with reports from the CDC,3 results from the current study show a negative relationship between physical activity and age. Physical activity may show age-related decline because older adults are more likely to suffer from physical limitations that keep them from engaging in physical activity.4 Consistent with this suggestion, the current study revealed that older adults tend to report worse self-rated health than younger respondents. However, because this is a cross-sectional study, the results could also be explained by a cohort effect, whereby older cohorts are less likely to exercise than younger cohorts.
Control Beliefs
Further still, many older adults do not believe they are capable of engaging in physical activity,7,9,10 or may be discouraged from exercise due to fear that physical activity will cause injury.8 In fact, in the current study we found that older adults reported less control than did younger adults. Supporting predictions, our results also revealed that a higher sense of control was related to more physical activity over time. This is consistent with studies that have examined domain-specific control beliefs, or self-efficacy.15,29 This is the first study, however, to demonstrate a relationship between general control beliefs and physical activity behavior. While the effect size in the current study was smaller than those usually detected in studies using domain-specific measures,29 the present results suggest that a general sense of control can generalize to specific domains of functioning. Because control beliefs can be modified through intervention,43 future physical activity interventions may benefit from targeting control beliefs.
Education
While the effect size was small, the results from the present investigation demonstrate that older adults with at least some college education reported more physical activity than older adults with less education. Therefore, higher education may be protective against age-related declines in physical activity. These results need to be confirmed in longitudinal studies, but they are consistent with previous work reporting a positive association between education and physical activity.20,21 Adults with higher educational attainment may be more aware of the health benefits of physical activity, especially in later life, and may therefore be more likely to maintain physical activity across the lifespan. Furthermore, adults with higher education may be more aware of how to exercise appropriately. In addition, adults with higher education may hold jobs with higher pay, and may therefore have more economic opportunity to become and remain physically active (eg, access to fitness facilities, biking and walking trails, child care).
Social Relations
Consistent with predictions and previous research,28 results revealed that higher social support was associated with more frequent physical activity for all age groups, suggesting that social support does not need to be domain-specific to promote adaptive health behaviors. On the contrary, the general feeling of being supported by others may inspire health-promoting behaviors. However, just as we found for control beliefs, the association of general social support and physical activity was weaker than the associations that have been reported using domain-relevant measures of social support.28
To our knowledge, this is the first study to examine the relationship of social strain to physical activity in a Western sample, and contrary to our hypothesis, we found that higher social strain was related to higher physical activity. Again, while the effect size was small, there may be something about experiencing social strain that leads older adults to engage in physical activity. For example, people who perceive more negative social interactions may engage in physical activity to escape their straining social partners, distract themselves from their negative affect, and experience the endorphin high that usually accompanies exercise.44
Alternatively, social control may explain the positive relationship of strain to physical activity.36 Many social interactions that are intended as support can be perceived as strain. For example, a wife who wants her husband to start exercising may hide his television remote control so that he is forced to exert physical effort by looking for it before he can relax in front of the TV. These interactions, while intended as social support, may be perceived as nagging or demanding, and thus interpreted as social strain. The negative feelings induced by these strained social interactions may provide motivation to engage in health-changing behaviors to relieve the negative emotional state induced, like annoyance, anger, and irritation. Consistent with this example, Krause et al35 found that negative social interaction predicted more frequent exercise among Japanese older adults, demonstrating that social sanctions can influence health behavior.
The interaction between age and social strain on physical activity supports the explanation that social strain may actually be misinterpreted social support: Social strain moderated the relationship of age to physical activity such that older adults reporting higher social strain were more physically active than older adults reporting lower social strain. Older adults report fewer social control agents and fewer social control attempts.45 Thus, the older adults who do experience these interactions may be more likely to engage in physical activity. Health is a major concern among older adults,12 and older adults who receive more encouragement toward health and health behaviors (possibly interpreted as social strain) may engage in more healthy behaviors, including physical activity.
Furthermore, older adults may be better at emotion regulation.46 Socioemotional Selectivity Theory states that when time is perceived as limited, people are motivated to make themselves feel good. Thus, older adults, who are further along in the life course than younger adults, are theoretically more motivated to regulate their emotions. While older adults do not exercise as much as younger adults, those older adults who are physically active may engage in physical activity behavior because it helps them to manage their negative emotions and distracts or removes them from socially straining partners.
While unpleasant to experience, social strain may provide the constructive criticism necessary to inspire health behavior change. For example, receiving negative feedback may indicate to a person that he or she has a problem or needs to make a change. Furthermore, experiencing social strain may arouse negative emotions that can be reduced by engaging in physical activity. Thus, while social strain has negative direct effects on health and well-being (24), it may provide the motivation necessary to improve health-promoting behaviors.
Limitations
Use of the rich MIDUS data set provides an opportunity to examine many questions of interest with impressive statistical power. In fact, examining age interactions with psychosocial and behavioral variables is difficult in smaller samples that are not likely to include participants in the outer ranges of the distribution where the interaction effect can be detected; they lack power to detect interactions.47 Therefore, in the current study we examined data from a sample that was large enough to have sufficient power to detect interaction effects. However, the effect sizes were consistently small, and results with small effect sizes must be interpreted with caution, as they may not be clinically significant.
Furthermore, the variables only accounted for 13.6% of the variance in physical activity frequency. We chose to focus on control beliefs and social relationships because they have consistently been demonstrated as strong predictors of physical activity15–18,28 they are modifiable and thus amenable to intervention,15–19 and they are also directly related to health outcomes.12,14,23,25–27,31–35 We chose to examine more general social relations and control beliefs, as opposed to domain-specific, due to their potential for more effective and thorough intervention. It is likely due to the general nature, however, that we were only able to account for 13% of the variance in physical activity frequency. While this is a small percentage of variance, general social relationships and control beliefs may still be effective targets for intervention. For example, both are amenable to educational intervention, which can be a simple and inexpensive method to reach adults (eg, mailed pamphlets or magazines), and may especially appeal to the older cohorts who are at most risk for physical inactivity. In addition, modifying global beliefs may lead to improvements in multiple outcome domains, as opposed to just 1 or a few outcome domains.19 Thus, interventions focusing on general social relations and control beliefs may be more efficient and cost-effective than domain-specific interventions for promoting health, health behaviors, and independence across the lifespan.
In addition to the limitations described above, all variables were measured with a self-report survey method. Therefore, shared method variance may have played a role in the relationships. Finally, the use of longitudinal data is imperative for deciphering causal relationships. Unfortunately, the physical activity measure assessed in the current study was only administered at MIDUS II (a different measure of physical activity was used for the first occasion), and therefore the results from the current study are cross-sectional.
Conclusion
In conclusion, individuals with higher education, social support, social strain, and control beliefs tend to be more physically active across the lifespan, and having higher education and higher social strain may even attenuate age-related declines in physical activity participation. Given that general control beliefs and social relationship quality are related to exercise, especially for older adults, there is reason to focus on these modifiable psychosocial factors to help promote increased physical activity. Future investigations should aim to replicate the associations presented here with longitudinal studies. Furthermore, future research would benefit from including measures of both general and domain-specific control beliefs and social relations to compare the influences of the two. Finally, we found an unexpected relationship between social strain and physical activity frequency, such that higher social strain was related to more frequent physical activity. This result may inspire an interesting new area of scientific exploration with implications for how we understand our social relationships and their impact on our behavior.
Acknowledgments
This research was supported by a grant from the National Institute on Aging (P01-AG020166) to conduct a longitudinal follow-up of the MIDUS (Midlife in the U.S.) investigation. The original study was supported by the John D. and Catherine T. MacArthur Foundation Research Network on Successful Midlife Development. This research is based on the first author's doctoral dissertation.
Appendix
The next section asks about various “levels” of physical activity (vigorous, moderate, light)—while at your job, while at home, and during your leisure/free time. Please answer each question thinking first about summertime, and then about wintertime. (If the question does not apply to you, for example, because you do not have a paid job or are retired, please circle 0 for “Never.”)
A30. How often do you engage in vigorous physical activity that causes your heart to beat so rapidly that you can feel it in your chest and you perform the activity long enough to work up a good sweat and are breathing heavily? (Examples: competitive sports like running, vigorous swimming, or high intensity aerobics; digging in the garden, or lifting heavy objects)
5 = Several times a week, 4 = Once a week, 3 = Several times a month, 2 = Once a month, 1 = Less than once a month, 0 = Never
While at your paid job …
-
a
During the Summer? 0 1 2 3 4 5
-
b
During the Winter? 0 1 2 3 4 5
While performing chores in and around your home …
-
c
During the Summer? 0 1 2 3 4 5
-
d
During the Winter? 0 1 2 3 4 5
During your leisure or free time …
-
e
During the Summer? 0 1 2 3 4 5
-
f
During the Winter? 0 1 2 3 4 5
A31. How often do you engage in moderate physical activity, that is not physically exhausting, but it causes your heart rate to increase slightly and you typically work up a sweat? (Examples: leisurely sports like light tennis, slow or light swimming, low impact aerobics, or golfing without a power cart; brisk walking, mowing the lawn with a walking lawnmower.)
5 = Several times a week, 4 = Once a week, 3 = Several times a month, 2 = Once a month, 1 = Less than once a month, 0 = Never
While at your paid job …
-
a
During the Summer? 0 1 2 3 4 5
-
b
During the Winter? 0 1 2 3 4 5
While performing chores in and around your home …
-
c
During the Summer? 0 1 2 3 4 5
-
d
During the Winter? 0 1 2 3 4 5
During your leisure or free time …
-
e
During the Summer? 0 1 2 3 4 5
-
f
During the Winter? 0 1 2 3 4 5
Contributor Information
Kelly A. Cotter, Dept of Psychology, Sacramento State University, Sacramento, CA
Margie E. Lachman, Dept of Psychology, Brandeis University, Waltham, MA
References
- 1.American College of Sports Medicine. Exercise and physical activity for older adults. Med Sci Sports Exerc. 1998;30:992–1008. [PubMed] [Google Scholar]
- 2.Pleis JR, Lethbridge-Cejku M. Summary health statistics for U.S. adults: National Health Interview Survey, 2005. 2006;10:232. [PubMed] [Google Scholar]
- 3.Centers for Disease Control and Prevention. Physical activity for everyone. [June 24, 2008]; Available at: http://www.cdc.gov/nccdphp/dnpa/physical/everyone/recommendations/
- 4.Sechrist KR, Walker SN, Pender NJ. Development and psychometric evaluation of the Exercise Benefits/Barriers Scale. Res Nurs Health. 1987;10:357–365. doi: 10.1002/nur.4770100603. [DOI] [PubMed] [Google Scholar]
- 5.Cohen-Mansfield J, Marx MS, Guralnik JM. Motivators and barriers to exercise in an older community-dwelling population. J Aging Phys Act. 2003;11:242–253. [Google Scholar]
- 6.Ebrahim S, Rowland L. Towards a new strategy for health promotion for older women: determinants of physical activity. Psychol Health Med. 1996;1:29–40. [Google Scholar]
- 7.Myers RS, Roth DL. Perceived benefits of and barriers to exercise and stage of exercise adoption in young adults. Health Psychol. 1997;16:277–283. doi: 10.1037//0278-6133.16.3.277. [DOI] [PubMed] [Google Scholar]
- 8.Lees FD, Clark PG, Nigg CR, Newman P. Barriers to exercise behavior among older adults: a focus group study. J Aging Phys Act. 2005;13:23–33. doi: 10.1123/japa.13.1.23. [DOI] [PubMed] [Google Scholar]
- 9.Lachman ME. Locus of control in ageing research: a case for multidimensional and domain-specific assessment. Psychol Aging. 1986;1:34–40. doi: 10.1037//0882-7974.1.1.34. [DOI] [PubMed] [Google Scholar]
- 10.Lachman ME. Perceived control over memory ageing: developmental and intervention perspectives. J Soc Issues. 1991;47:159–175. [Google Scholar]
- 11.Lachman ME, Jette AM, Tennstedt S, Howland J, Harris BA, Peterson E. A cognitive-behavioral model for promoting regular physical activity in older adults. Psychol Health Med. 1997;2:251–261. [Google Scholar]
- 12.Lachman ME, Firth KM. The adaptive value of feeling in control during midlife. In: Brim OG, Ryff CD, Kessler R, editors. How healthy are we?: A national study of well-being at midlife. Chicago: University of Chicago Press; 2004. pp. 320–349. [Google Scholar]
- 13.Abramson LY, Seligman MEP, Teasdale JD. Learned helplessness: critique and reformulation. J Abnorm Psychol. 1978;87:49–74. [PubMed] [Google Scholar]
- 14.Rodin J. Aging and health: effects of the sense of control. Science. 1986;233:1271–1276. doi: 10.1126/science.3749877. [DOI] [PubMed] [Google Scholar]
- 15.Bandura A. Self-Efficacy: the exercise of control. New York: W. H. Freeman and Company; 1997. [Google Scholar]
- 16.Ajzen I. The Theory of Planned Behavior. Organ Behav Hum Decis Process. 1991;50:179–211. [Google Scholar]
- 17.Prochaska JO, DiClemente CC, Norcross JC. In search of how people change: applications to addictive behaviors. Am Psychol. 1992;47:1102–1114. doi: 10.1037//0003-066x.47.9.1102. [DOI] [PubMed] [Google Scholar]
- 18.Armitage CJ, Conner M. Efficacy of the Theory of Planed Behavior: a meta-analytic review. Br J Soc Psychol. 2001;40:471–499. doi: 10.1348/014466601164939. [DOI] [PubMed] [Google Scholar]
- 19.Lachman ME, Weaver SL. The sense of control as a moderator of social class differences in health and well-being. J Pers Soc Psychol. 1998;74:763–773. doi: 10.1037//0022-3514.74.3.763. [DOI] [PubMed] [Google Scholar]
- 20.Dowda M, Ainsworth BE, Addy CL, Saunders R, Riner W. Correlates of physical activity among U.S. young adults, 18 to 30 years of age, from NHANES III. Ann Behav Med. 2003;26:15–23. doi: 10.1207/S15324796ABM2601_03. [DOI] [PubMed] [Google Scholar]
- 21.U.S. Department of Health and Human Services. Physical Activity and health: a report of the surgeon general. Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion; 1997. [Google Scholar]
- 22.U.S. Census Bureau. Census 2000 Summary File 3 (SF 3) - Sample Data, Detailed Tables. [March 14, 2009]; Available at: http://factfinder.census.gov/servlet/DTTable?_bm=y&-geo_id=01000US&-ds_name=DEC_2000_SF3_U&-_lang=en&-redoLog=false&-mt_name=DEC_2000_SF3_U_PCT025&-CONTEXT=dt.
- 23.Cohen S. Social relationships and health. Am Psychol. 2004;59:676–684. doi: 10.1037/0003-066X.59.8.676. [DOI] [PubMed] [Google Scholar]
- 24.Rook KS. Detrimental aspects of social relationships: Taking stock of an emerging literature. In: Veiel HOF, Bauman U, editors. The meaning and measurement of social support. Washington, DC: Hemisphere Publishing Corp; 1992. pp. 157–169. [Google Scholar]
- 25.Walen HR, Lachman ME. Social support and strain from partner, family, and friends: Costs and benefits for men and women in adulthood. J Soc Pers Relat. 2000;17:5–30. [Google Scholar]
- 26.Berkman LF, Glass T, Brissette I, Seeman TE. From social integration to health: Durkheim in the new millennium. Soc Sci Med. 2000;51:843–857. doi: 10.1016/s0277-9536(00)00065-4. [DOI] [PubMed] [Google Scholar]
- 27.Heller K, Rook KS. Distinguishing the theoretical functions of social ties: implications for support interventions. In: Sarason BR, Duck S, editors. Personal relationships: Implications for clinical and community psychology. Chichester, England: John Wiley & Sons; 2001. pp. 119–139. [Google Scholar]
- 28.Carron AV, Hausenblas HA, Mack D. Social influence and exercise: a meta-analysis. J Sport Exer Psychol. 1996;18:1–16. [Google Scholar]
- 29.McAuley E, Jerome GJ, Elavsky S, Marquez DX, Ramsey SN. Predicting long-term maintenance of physical activity in older adults. Prev Med. 2003;37:110–118. doi: 10.1016/s0091-7435(03)00089-6. [DOI] [PubMed] [Google Scholar]
- 30.McAuley E, Jerome GJ, Marquez DX, Elavsky S, Blissmer B. Exercise self-efficacy in older adults: Social, affective, and behavioral influences. Ann Behav Med. 2003;25:1–7. doi: 10.1207/S15324796ABM2501_01. [DOI] [PubMed] [Google Scholar]
- 31.Antonucci TC, Akiyama H, Lansford JE. The negative effects of close social relations among older adults. Fam Relat. 1998;47:379–384. [Google Scholar]
- 32.Davis MC, Swan PD. Association of negative and positive social ties with fibrinogen levels in young women. Health Psychol. 1999;18:131–139. doi: 10.1037//0278-6133.18.2.131. [DOI] [PubMed] [Google Scholar]
- 33.Rook KS. Parallels in the study of social support and social strain. J Soc Clin Psychol. 1990;9:118–132. [Google Scholar]
- 34.Cotter KA, Sherman AM. Social relations and exercise self-efficacy in older adults with osteoarthritis. J Aging Phys Act. 2008;16:465–483. doi: 10.1123/japa.16.4.465. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Krause N, Goldenhar L, Liang J, Jay G, Maeda D. Stress and exercise among the Japanese elderly. Soc Sci Med. 1993;36:1429–1441. doi: 10.1016/0277-9536(93)90385-h. [DOI] [PubMed] [Google Scholar]
- 36.Tucker JS. Health-related social control within older adults' relationships. Journal of Gerontology: Psychological Sciences. 2002;57B:387–395. doi: 10.1093/geronb/57.5.p387. [DOI] [PubMed] [Google Scholar]
- 37.Lewis MA, Rook KS. Social control in personal relationships: Impact on health behaviors and psychological distress. Health Psychol. 1999;18:63–71. doi: 10.1037//0278-6133.18.1.63. [DOI] [PubMed] [Google Scholar]
- 38.Hughes M, Gove WR. Living alone, social integration, and mental health. Am J Sociol. 1981;87:48–74. doi: 10.1086/227419. [DOI] [PubMed] [Google Scholar]
- 39.Cotter KA, Lachman ME. Psychosocial and behavioral contributors to health: age-related increases in physical disability are reduced by physical fitness. Psychol Health. doi: 10.1080/08870440902883212. In press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Lachman ME, Weaver SL. The sense of control as a moderator of social class differences in health and well-being. J Pers Soc Psychol. 1998;74:763–773. doi: 10.1037//0022-3514.74.3.763. [DOI] [PubMed] [Google Scholar]
- 41.Prenda KM, Lachman ME. Planning for the future: a life management strategy for increasing control and life satisfaction in adulthood. Psychol Aging. 2001;16:206–216. [PubMed] [Google Scholar]
- 42.Brim OG, Ryff CD, Kessler RC. The MIDUS National Survey: an overview. In: Brim OG, Ryff CD, Kessler RC, editors. How healthy are we? A national study of well-being at midlife. Chicago: University of Chicago Press; 2004. pp. 1–34. [Google Scholar]
- 43.Lachman ME, Weaver SL, Bandura M, Elliott E, Kewkowicz C. Improving memory and control beliefs through cognitive restructuring and self-generated strategies. Journals of Gerontology: Psychological Sciences. 1992;47:293–299. doi: 10.1093/geronj/47.5.p293. [DOI] [PubMed] [Google Scholar]
- 44.Thoren P, Floras JS, Hoffmann P, Seals DR. Endorphins and exercise: physiological mechanisms and clinical implications. Med Sci Sports Exerc. 1990;22:417–428. [PubMed] [Google Scholar]
- 45.Tucker JS, Klein DJ, Elliot MN. Social control of health behaviors: a comparison of young, middle-aged, and older adults. Journal of Gerontology: Psychological Science. 2002;59B:147–150. doi: 10.1093/geronb/59.4.p147. [DOI] [PubMed] [Google Scholar]
- 46.Carstensen LL, Isaacowitz DM, Charles ST. Taking time seriously: a theory of socioemotional selectivity. Am Psychol. 1999;54:165–181. doi: 10.1037//0003-066x.54.3.165. [DOI] [PubMed] [Google Scholar]
- 47.McClelland GH, Judd CM. Statistical difficulties of detecting interactions and moderator effects. Psychol Bull. 1993;114:376–390. doi: 10.1037/0033-2909.114.2.376. [DOI] [PubMed] [Google Scholar]