

Abstract
Study Design
Prospective cohort study
Objective
This study was designed to neurophysiologically characterize spinal motor activity during recovery from spinal cord injury (SCI).
Setting
University of Louisville, Louisville, Kentucky, USA.
Material
Twenty five consecutive acute SCI admissions were recruited for this study.
Methods
The American Spinal Injury Association Impairment Scale (AIS) was used to categorize injury level and severity at onset. Surface EMG recording, was carried out initially between the day of admission and 17 days post onset (6.0 ± 4.3, mean ± SD days). Follow-up recordings were performed for up to 9 months after injury. Initial AIS distribution was: 7 AIS-A; 3 AIS-B; 2 AIS-C; 13 AIS-D.
Results
Twelve subjects (48%) showed long-duration involuntary motor unit activation during relaxation. This activity was seen on initial examination in nine and on follow-up by three months post-injury in three others. It was seen in muscles innervated from the injury zone in 11 and caudal to the lesion in 9 subjects. This activity was independent of the presence or absence of tendon reflexes and the ability to volitionally suppress plantar stimulation elicited reflex withdrawal.
Conclusions
The form of involuntary activity described here is the likely result of the altered balance of excitation and inhibition reaching spinal motor neurons due to the loss of inhibitory interneurons or their reduced activation by damaged supraspinal drive and the synaptic reorganization that follows SCI. As such, this activity may be useful for monitoring the effects of neuroprotective and restorative intervention strategies in persons with SCI.
Keywords: Spinal Cord Injury, Motor control, surface electromyography, Brain Motor Control Assessment, Spasticity
Introduction
People with spinal cord injury (SCI) have reported that “stiffness” due to ongoing muscle contraction, differentiated from episodic spasms, is a secondary complication that significantly impacts their quality of life.1, 2 Currently, involuntary motor activity that results from SCI is largely examined and treated based on rate-dependent responsiveness to passive stretch.3 Structured clinical examination scales, manual and isokinetic dynamometry and pendulum-test methods, and the documentation of spasm frequency do not fully characterize involuntary motor activity that occurs after SCI.4 Multi-muscle surface EMG (sEMG) recording during such motor tasks provides a quantifiable description of spinal motor output, its amplitude and distribution across muscles.5 Further, neurophysiological assessment has been used to demonstrate that spinal neural processing of exteroceptive input to the spinal cord, such as that brought by muscle stretch, is not the only mechanism involved in the production of involuntary muscle activation caudal to the lesion in chronic SCI.6
Animal models of experimental SCI have shown that spinal interneurons and motor neurons experience a partial, often severe, loss of input from peripheral nerve fibers and spinal tracts which can initiate a period of depressed responsiveness.7 This depressed responsiveness resolves over a period of days in a process that involves the elimination of synapses previously occupied by neurons lost or damaged in the injury and reorganization of the neighboring synaptic boutons of surviving cells.7 Additional synaptic replacement may occur as neurites were shown to ‘sprout’ from surviving peripheral nerves8 and descending spinal tracts9 reach spinal interneurons and motor neurons. In humans, it is presumed that such reorganization not only brings an end to ‘spinal shock’ and the return of reflex responsiveness but can also lead to the development of increased muscle tone and spasticity3. One of the forms of motor output that is can be seen in chronic SCI is the continuous motor unit activation in one or more muscles while the subject with SCI is in the supine position and under instruction to fully relax.5, 6 In truth, spinal motor responsiveness to episodic input may not be related to the mechanisms that bring the complaint of stiffness or this continuous motor unit activation. Therefore, the study reported here was undertaken to neurophysiologically examine and characterize the development of the long-lasting involuntary spinal motor output that can be present, independent of exteroceptive input or episodic spasms, and may be associated with the patient report of stiffness following SCI.
Methods
Material
All assessments were carried out after informed consent was obtained under the approval of the Institutional Review Board for human research of the University of Louisville. The 25 SCI subjects in this study were drawn from consecutive traumatic spinal cord injured admissions to the hospital (Table 1). Persons with clinically recognizable concomitant head injury were not enrolled in this study. All were alert and able to cooperate with the testing performed during this study. No changes were made in clinical management for this study. Nineteen underwent surgical intervention 2.0 ± 15.1 (mean ± SD) days after injury preceding initial assessment for this study in 16 subjects. Four of the 25 subjects were female and all were 22 to 84 (45.4 ± 15.4) years of age at the time of injury. The AIS distribution was: 7 AIS-A; 3 AIS-B; 2 AIS-C; 13 AIS-D. Twelve were clinically diagnosed as central cord syndromes. Four of the 25 subjects were taking Baclofen to control spasticity, 10 to 20 mg three to four times per day, at the time of neurophysiological assessment.
Table 1.
Clinical categorization, time of assessment, and muscles identified as showing long-lasting involuntary activation during relaxation.
| Subject Number | Injury Level | Initial AIS Category | Days post-onset | Active Muscles | |
|---|---|---|---|---|---|
| Cervical | Lumbosacral | ||||
| 1 | C4 | C | 3 | ||
| 15 | |||||
| 28 | |||||
| 40 | RTA. RSOL | ||||
| 51 | RWF | ||||
| 2 | C4 | C | 3 | RVL, RSOL | |
| 47 | RUT. RBB. RTB. RWE. RWF. LUT. LBB. LAPB | RVL, RADD, RH, RTA, RSOL, REDB, RAH, LVL LADD, LEDB, LAH | |||
| 180 | RUT, RBB, RTB, RWE, RWF, RADQ, LUT, LBB, LTB, LWE, LWF, LADQ | RVL, RH, RTA, RSOL, REDB, RAH, LVL, LADD, LH, LTA, LSOL, LEDB, LAH | |||
| 3 | C4,5 | D | 8 | RUT, RWE, RWF, RAPB, RADQ, LWF, LAPB, LADQ | RTA, RSOL, REDB, RAH, LADD, LH, LTA, LSOL, LEDB, LAH |
| 4 | C5 | A | 16 | ||
| 29 | RUT, RWF; LUT; LBB | ||||
| 52 | RUT; RWE; RWF; LUT; LBB; LWE; LWF | RVL, LADD, RH, RSOL, RAH | |||
| 5 | C5 | D | 1 | RUT, LUT, LBB | REDB, RAH, LAH |
| 90 | RBB, RWE, RWF, RAPB, LBB, LWE, LAPB | ||||
| 6 | C5 | D | 6 | RUT, LUT | RH, LAH |
| 34 | RUT, RBB, RTB, RWE, RWF, LUT | RAH, LEDB, LAH | |||
| 7 | C5,6 | D | 5 | RUT, LUT, LWE | RH, RTA, RSOL, RAH, LH, LSOL, LEDB, LAH |
| 8 | C6 | D | 3 | RUT, LUT, LBB, LTB | |
| 9 | C6,7 | D | 5 | LWF | RSOL, LAH |
| 150 | RWF, RAPB, RADQ, LUT | LAH | |||
| 330 | RUT, RTB, RAPB, RADQ, LUT, LEWE, LWF, LADQ | REDB, RAH, LEDB, LH | |||
| 10 | C6,7 | D | 6 | RTB, RWE, RWF, LTB, LWF | RH, LH |
| 11 | C6R, S1L | D | 3 | RUT | RAH, LADD, LH, LTA, LSOL, LEDB, LAH |
| 12 | T1 | A | 3 | LUT | |
| 25 | RUT, LUT | ||||
| 120 | RUT | RTA; RSOL; REDB; RAH; LTA; LEDB; LAH | |||
Clinical assessment
Clinical lesion severity was examined on admission to the hospital using the ASIA Impairment Scale (AIS)10. The AIS provides a subjective estimation of voluntary contraction strength for five upper limb (C5 to T1) and five lower limb (L2 to S1) muscles on each side along with the perception of light touch and pin prick for C2 through S5 dermatomes. The AIS was repeated at irregular intervals determined by subjects’ return to the spinal cord injury clinic.
Neurophysiological assessment
Using the functional EMG method, Brain Motor Control Assessment (BMCA),5 subjects were tested as soon post-onset as was judged medically appropriate by attending physicians. Initial recordings were made as early as the day of injury and as late as 17 days (6.0 ± 4.3) post onset. The BMCA is a protocol of volitional and reflex motor tasks rigorously carried out with the subject in the supine position using published standards for administration. Following standard skin preparation, pairs of surface EMG (sEMG) electrodes spaced 2 cm apart were placed over the muscle bellies of the right and left upper trapezius (UT), biceps brachi (BB), triceps brachi (TB), wrist extensors (WE), wrist flexors (WF), adductor policis brevis (APB), abductor digiti quinti (ADQ), rectus abdominus (RA) (para-umbilical), quadriceps (QD), adductor femoris (Add), hamstrings (H), tibialis anterior (TA), soleus (Sol), extensor digitorum brevis (EDB), and abductor hallicus (AH). The protocol begins with 5 minutes of relaxation followed by three repetitions each of: reinforcement maneuvers (deep breath, neck flexion, shoulder shrug); voluntary movements of arms and legs; passive movements of arms and legs; manual ankle clonus elicitation; suppression of plantar stimulation cutaneomuscular reflex response. Events were manually marked on the recording by the examiner using a hand-held button as the subject was instructed and audibly cued to attempt the required tasks. Surface EMG (sEMG) signals were recorded on a 32-channel Eclipse Neurological Workstation (AXON Systems, Inc.) with a sampling rate of 2 KHz per channel and a bandpass of 30 Hz to 2 KHz.
Data analysis
Quantification of the sEMG signals was accomplished using Windaq Waveform Browser software (Dataq Corporation, Akron, Ohio, USA) which applies a root-mean-square (RMS) algorithm to produce mean values for the selected time window expressed in μV/sec. Relaxation was quantified in 30-second epochs, ten per 5-minute relaxation period, for each muscle. Values presented here are the mean for the six 30-second epochs per relaxation period except for one subject in which movement artifacts were present. In order to be classified as long-duration activity, the recorded activity had to persist through at least 50% of the 5-minute relaxation period. It is important to note that activity in any particular muscle could not be qualified on the mean amplitude alone since voluntary events can occur during the 5-minute relaxation period producing a substantial contribution to the mean amplitude measured during the required 2.5 minutes, or that intermittent artifacts may be present. In fact, when only single or very few motor units are firing, the mean amplitude may be greater than instrumentation and environmental radiated noise background by only a small amount (Figure 1). Therefore, it was necessary to employ a combined qualitative and quantitative analysis approach, especially for very low amplitude activity. Cutaneomusclar withdrawal reflex responses from plantar surface stimulation were quantified as the peak RMS amplitude from the TA muscle.6 Values were averaged for three trials each under unsuppressed and volitionally suppressed conditions for individual subjects. Group mean amplitudes and paired t-test values were calculated with significance reached at p < 0.05.
Figure 1.
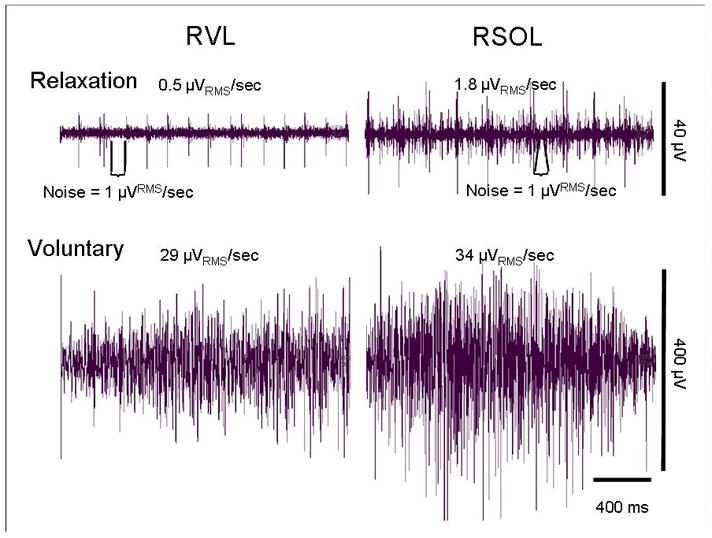
Measurement of surface EMG signals from the initial recording from a subject with a motor-incomplete C4 injury carried out 3 days post onset (Left), comparing activity observed in relaxation, measurement of noise level, activity of interest, and volitional activation of the Right Vastus Lateralis (RVL) and Soleus (RSOL) muscles. Note that the activity of interest during relaxation develops very little amplitude above noise when only a few motor units are firing (RVL) and is of much lower amplitude than volitional activation.
Results
Long-duration sEMG activity during relaxation
Initial recordings revealed that 9 of the 25 subjects (36%) had long-duration activity (Figure 2) in one or more muscles (Figure 3). This long-lasting spontaneous motor unit activity was more often seen in motor-incomplete subjects (68%) but could be found in motor-complete subjects (20%). The average time post-onset for the initial recording in the 9 subjects with this activity was 4.4 ± 2.1 days. An additional 3 subjects developed such activity on follow-up examinations carried out between 1 and 3 months post onset. Thus, 12 of the 25 total subjects, 48%, developed long-lasting non-volitional and non-reflex motor output (Table 1). The two initially AIS motor-complete subjects showing this long-lasting activity did so only after more than a month post injury (numbers 4 and 12, Table 1). Of the 13 who did not show this long-lasting spontaneous activity, 3 were AIS-D, two C4 and one T11 injury levels, and 9 were motor complete, 6 AIS-A and 3 AIS-B with C4 to T12 injury levels. From these 13, 4 were lost to follow-up and the other 9 were followed for 1 to 12 months without developing such activity.
Figure 2.

Surface EMG activity from the final 30 seconds of the 5-minute relaxation period from the Right and Left upper trapezius (UT), Biceps Brachii (BB), Triceps Brachii (TB), Wrist Extensor (WE), Wrist Flexor (WF), Adductor Policis Brevis (APB), Adductor Digiti Quinti (ADQ), Rectus Abdominus (RA), Vastus Lateralis (VL), Adductor (ADD), Hamstring (H), Ttibialis Anterior (TA), Soleus (SOL), Extensor Digitorum Brevis (EDB), Adductor Hallicus (AH) muscles. Shown are three serial recordings from a person with a C4 AIS category C spinal cord injury. Note the repeating single motor unit firing in the RSOL recorded 6 days after injury and the increasing number of muscles showing increasing motor unit activity 47 days and 6 months after onset.
Figure 3.
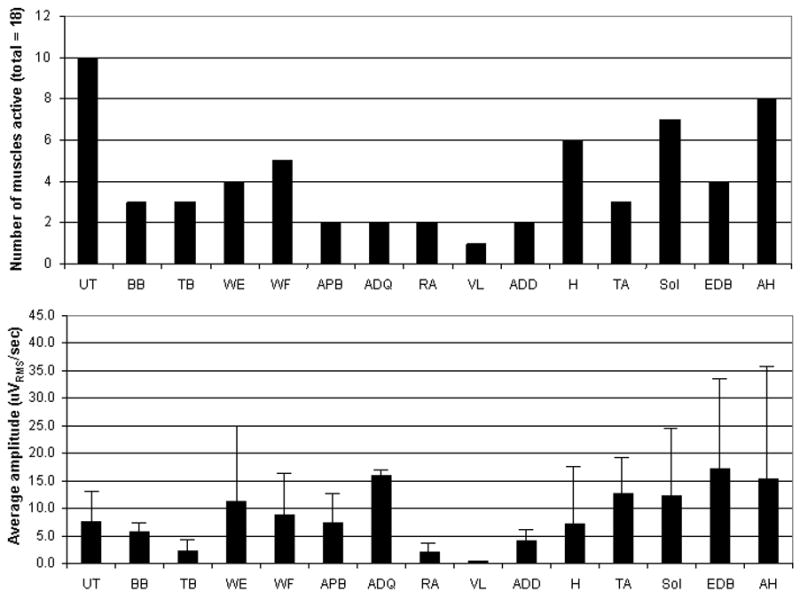
Results for 9 subjects in which long-lasting activation was observed during the initial recording: prevalence of activation from right and left sides in 9 subjects (top); group mean amplitudes ± SD for each muscle recorded (bottom).
Duration and distribution of long-lasting sEMG activity
Seventy-five percent of the active muscles remained activated throughout the 5-minute relaxation period. Activated muscles were innervated from cervical spinal motor neurons in 10 of these 12 subjects and from lumbosacral cord in nine (Table 1). In eight subjects, long-duration activation was seen in both upper and lower limb muscles. Ten of these 12 subjects, 82%, showed long-lasting activation in one or both upper trapezius muscles. Other than the upper trapezius, the distal muscles of the lower limbs, extensor digitorum brevis (8 of 12) and adductor hallicus (8 of 12), were most often active (Figure 3). Finally, in six of the seven subjects from whom follow-up data was available, there was an increase over time in the number of muscles showing this activity (Figure 4).
Figure 4.
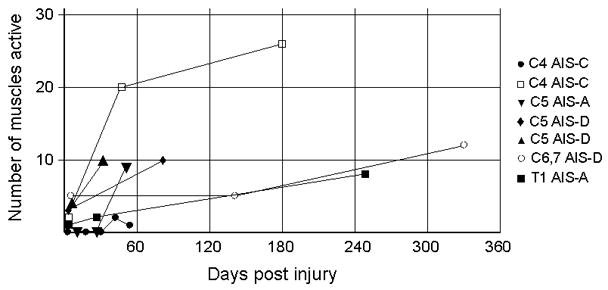
Number of muscles showing long-duration activation during relaxation in serial recordings from 7 subjects. Note the increase in number of muscles active with time.
Amplitude of long-duration sEMG activity
The presentation of this activity ranged from very low amplitude, regularly repeating firing, to multiple motor unit activation that produced average amplitudes that were still well below 10% of the amplitudes usually recorded during volitional activation in motor-incomplete SCI subjects (Figure 1). It should be noted that there was considerable amplitude variance across and within individuals.
Volitional activation and reflex responsiveness
For the 11 subjects in whom this long-duration activity was observed, differing degrees of responsiveness to muscle stretch and cutaneous stimulation were recorded. Responses to patellar or Achilles tendon taps were present in 3 of the 7 subjects in which they were tested in the initial examination. For the remaining 5 subjects, responses were still absent in 4 subjects on follow-up examinations carried out between 25 and 90 days after injury. Of the 166 recorded muscles which met the requirements for recognition of long-lasting activation during relaxation, 150 (90%) could be volitionally activated within the same recording session. Excluding the upper trapezius and rectus abdominus trunk muscles, 140 upper and lower limb muscles produced this long-lasting activity. Of these 140, 58 were tested for responsiveness to passive stretch during elbow and wrist flexion and extension, hip and knee flexion and extension, and ankle dorsal and plantar flexion. From these 58, only 17 (29%) responded and 12 (71%) of those 17 did so with only a few motor units firing. Finally, 7 (41%) of these 17 were paralyzed during volitional task attempts. Cutaneomuscular reflex responses were absent in 3 subjects, present in 8, and not tested in one in the initial examination. Follow-up examination in the one missed on initial examination showed no response to plantar stimulation at 25 days. Of the eight with responses, they habituated over three trials in one and could not be volitionally suppressed to any extent in another. Within those in whom withdrawal responses could be suppressed, the group mean TA peak RMS unsuppressed amplitude was (93.4 ± 90.9 μV) was significantly decreased (29.9 ± 38.7 μV) (p < 0.01) by volitional suppression.
Effects of anti-spasticity medication
Two of the 12 subjects with long-lasting activation during relaxation were taking 10 mg of Baclofen, numbers 6 (4 per day at the time of the initial examination only) and 9 (3 per day), to control spasms. Within the 13 without long-lasting spontaneous activity, two were taking Baclofen.
Discussion
Continuous motor unit activation has been reported in chronic, clinically motor-complete SCI subjects using the multi-muscle surface EMG recording technique applied here.5,6 Further, in unpublished data from a group of 25 chronic motor-incomplete SCI subjects, we observed that approximately 20% had continuous activation of muscles caudal to the lesion in the relaxation period of the BMCA protocol. Here, data is presented showing that such activity can develop very early after injury and often becomes more widespread over time. Also, it can appear in muscles that are innervated from near to, within, or caudal to the injury zone. Since non-injured people are able to achieve total cessation of motor unit firing under the same conditions,5 it should be expected that the inability to do so is indicative of one or more pathophysiological effects of the injury. In contrast to clinical spasticity which is measured as an excessive response to muscle stretch, the activity reported here was more often seen in muscles that did not respond to passive movement (tonic) or tendon-tap (phasic) stretch. In fact, the long-lasting activation reported here was closely associated with the ability to volitionally activate motor units that were not particularly responsive to muscle spindle input. Therefore, it is likely that such long-lasting activity in relaxation is indicative of an unbalanced, excitation-dominant, resting descending input to segmental motor circuitry. Further, the appearance of such activity in paralyzed muscles may herald the return of volitional excitatory capability.
The vast majority of human spinal cord injuries are ischemic in etiology and complete transactions are rare.10 Therefore, most SCI in humans leave some long-tract fibers intact. In 1959, Gelfan and Tarlov11 described similar continuous spinal motor output in an animal model of spinal cord ischemia. They suggested that the two most likely causes of such activity are the loss of inhibitory interneuronal circuitry within the injury zone and/or lost descending long-tract connections to those inhibitory interneuronal circuits. They also observed that, once present, neither deafferentation nor rostral spinal cord transection brought an end to their continuous activity. Therefore, it is likely that post-injury reorganization7 in which synapses vacated by lost interneurons or damaged long-tract fibers have been left vacant or become occupied by neurites from other peripheral nerves8 or interneurons connected to or surviving long-tract fibers.9
Other sources of spontaneous EMG signals must be considered beginning with muscle denervation potentials. In chronic SCI populations, needle-recorded fibrillation potentials, positive sharp waves, and slowed peripheral-nerve motor conduction velocities have been reported as electrophysiological signs of lower motor neuron degeneration.12 This spontaneous activity was present in both complete and incomplete injuries and there was no correlation with time since injury or degree of spasticity.12 In animal models, denervation and fibrillation potentials appeared in the acute phase but dissipated over a few weeks.13 The presence of these indicators of lower motor neuron dysfunction was thought to result from transynaptic degeneration of the alpha motor neuron due to a loss of trophic support from descending connections.14 Although this may be a contributing mechanism to the single or few-unit patterns recorded in some muscles, the complex activity observed in most of the muscles (Figure 2) must be due to mechanisms that centrally excite multiple motor units.
The second potential explanation for the spontaneous motor unit firing reported here to consider is the post-traumatic spinal motor organization in which one or more muscles become continuously active, producing dystonic posturing that may develop as a result of peripheral nerve injury15 which certainly may occur with SCI. For example, unilateral dystonic posturing was described in people with motor-incomplete SCI.16 Further, it was shown that central motor conduction times for the contralateral corticospinal system were prolonged, suggesting that selective damage to the contralateral corticospinal tract could result in cervical dystonia after SCI.16 However, in the current study, long-duration activity was present in some subjects with preserved inhibitory control over withdrawal from cutaneous stimulation. Therefore, the loss of corticospinal control over inhibitory spinal interneuronal circuitry may be one the mechanisms that produced the results discussed here but cannot be the only one to consider.
A third potential source of this continuous motor unit excitation can be derived from a chronic rat spinal cord transaction model in which sodium-channel persistent inward currents (PICs) are thought to be facilitated by residual endogenous serotonin leading to spontaneous repetitive motor neuron firing.17 In addition, calcium PICs have also been shown to raise motor neuron sensitivity to endogenous serotonin, producing repetitive motor neuron activation.18 Finally, a mouse model, genetically altered to under-express GABA, an inhibitory neurotransmitter, in comparison to wild type animals, exhibited long-duration motor neuron activation.19 This long-duration activation was found to be reduced by the administration of valium, a post-synaptic GABA receptor potentiator, or baclofen, a GABA agonist.19 Although the literature regarding the effectiveness of Baclofen as a treatment for SCI-induced spasticity is at best, mixed, its application in non-injured subjects has been show to reduce force production.20 Intrathecal infusion of Baclofen has been said to reduce spasticity and “acquired dystonia” in people with SCI.21 The current study does not decrease this ambiguity since, two who were taking Baclofen exhibited this long-lasting activity while two others did not. It could be that the dose levels were inadequate but further study is needed to evaluate the effects of current anti-spasticity intervention strategies on PIC duration and this form of involuntary activity.
The final sources to be considered here are those brought by secondary pathological processes. The several cases in which the prevalence of this activity increased over time suggested that one or more secondary process may have been at work. Reports in humans are rare but Nogues and coworkers22 described long-duration firing of motor units recorded from muscles of the upper limbs in patients with syringomyelia or syringobulbia which damages spinal gray matter. They postulated that at least two mechanisms could be responsible for the increased excitability of the motor neurons: loss of inhibitory interneurons within or adjacent to the syrinx and/or damage to interneurons mediating disynaptic inhibition.22 Since, in some subjects, this long-duration activity began as early as the day of injury, too early to be a result of syrinx or other space-occupying lesion development, this mechanism should be considered as a potential explanation for its later-development as was observed in some subjects.
In fact, all of the processes described above are potentially present in any person with SCI. Also, without the guidance provided within the developing nervous system during childhood, the recovery process might well cause codification of pathophysiological organizations in which the balance is skewed toward excitation, producing the dystonic activity described after sensory nerve damage15 or SCI as in this paper and damage produced by secondary processes.22 In the current study, long-lasting spontaneous motor activity was more often found in clinically motor-incomplete than complete lesions supporting the notion that a lesion-induced imbalance due to the loss of descending control over inhibitory spinal motor circuitry may be responsible. The presence or delayed emergence of such activity after clinically motor-complete SCI may suggest that, barring the development of a space-occupying secondary lesion, some long-tract fibers remain functional or are recovering functional status with time. Also, the persistent activity presented in the current data appeared both in muscles innervated from within the spinal cord injury zone and those innervated caudal to the injury, suggesting that both long-tract damage and interneuronal loss can, independently or in combination, produce such activity. However, it should be noted that the absence of this activity in three motor-incomplete subjects indicates that the pathophysiological conditions that generate it are not always present after injury. It could be that in those three subjects, the imbalance of excitation and inhibition at the motor neurons was inadequate to elicit depolarization or the activity was too small or distant to be picked up by the recording electrodes.
Although no direct link between the presence of this low amplitude, long-lasting, muscle activation and clinically measured function has been established in the literature, its reduction might improve the functional ability of the approximately 15% of persons with SCI who reported stiffness to be “moderately” or “greatly bothersome.”1 By reducing such stiffness, patients might experience less difficulty beginning each day, need less effort to perform daily activities, and participate longer and more effectively in their therapy. Also, activity such as is reported here might provide a ‘biomarker,’ indicative of immediate or ongoing pathophysiological changes indicative of a developing secondary injury processes such as syrinx formation, inflammation, or vascular occlusion. However, additional studies are needed to establish clinical relevance and elucidate the precise cellular mechanism or mechanisms that should be targeted to provide effective treatment without producing further impairment of volitional abilities.
Acknowledgments
The authors would like to express their appreciation to Anne Watson, RN for project management support and Renee Ford for obtaining informed consent and coordination of study scheduling. In addition, we would like to acknowledge the Neurosurgery Residents at the University of Louisville Hospital for providing the clinical assessments reported in this study. This study was supported by NIH NINDS funded project #NS049954-01.
Sponsorship: NIH NINDS funded project #NS049954-01
Footnotes
Conflict of interest
The authors declare no conflict of interest.
References
- 1.Dudley-Javoroski S, Shields RK. Assessment of physical function and secondary complications after complete spinal cord injury. Disability and Rehabilitation. 2006;28(2):103–110. doi: 10.1080/09638280500163828. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Mahoney JS, Engebretson JC, Cook KF, Hart KA, Robinson-Whelen S, Sherwood AM. Spasticity experience domains in persons with spinal cord injury. Arch Phys Med Rehabil. 2007;88:287–94. doi: 10.1016/j.apmr.2006.12.029. [DOI] [PubMed] [Google Scholar]
- 3.Adams AA, Hicks AL. Spasticity after spinal cord injury. Spinal Cord. 2005;43:577–586. doi: 10.1038/sj.sc.3101757. [DOI] [PubMed] [Google Scholar]
- 4.Sherwood AM, McKay WB. Assessment of spasticity and upper motor neuron dysfunction. In: Akay Metin., editor. Wiley Encyclopedia of Biomedical Engineering. Vol. 5. John Wiley & Sons, Inc; 2006. pp. 3306–3315. [Google Scholar]
- 5.Sherwood AM, McKay WB, Dimitrijevic MR. Motor control after spinal cord injury: assessment using surface EMG. Muscle Nerve. 1996;19(8):966–79. doi: 10.1002/(SICI)1097-4598(199608)19:8<966::AID-MUS5>3.0.CO;2-6. [DOI] [PubMed] [Google Scholar]
- 6.McKay WB, Lim HK, Priebe MM, Stokic DS, Sherwood AM. Clinical neurophysiological assessment of residual motor control in post-spinal cord injury paralysis. Neurorehabil Neural Repair. 2004;18(3):144–53. doi: 10.1177/0888439004267674. [DOI] [PubMed] [Google Scholar]
- 7.Illis LS. The motor neuron surface and spinal shock. In: Williams Denis., editor. Modern Trends in Neurology. 0. Vol. 4. Vol. 4. Appleton-Century-Crofts; 1967. pp. 53–68. [PubMed] [Google Scholar]
- 8.McCough GP, Austin GM, Liu CN, Liu CY. Sprouting as a cause of spasticity. J Neurophysiol. 1958 May;21(3):205–16. doi: 10.1152/jn.1958.21.3.205. [DOI] [PubMed] [Google Scholar]
- 9.Hill CE, Beattie MS, Bresnahan JC. Degeneration and sprouting of identified descending supraspinal axons after contusive spinal cord injury in the rat. Exp Neurol. 2001;171:153–169. doi: 10.1006/exnr.2001.7734. [DOI] [PubMed] [Google Scholar]
- 10.Kakulas BA. Neuropathology: the foundation for new treatments in spinal cord injury (Sir Ludwig Guttman Lecture) Spinal Cord. 2004;42:549–563. doi: 10.1038/sj.sc.3101670. [DOI] [PubMed] [Google Scholar]
- 11.Gelfan S, Tarlov IM. Interneurones and rigidity of spinal origin. J Physiol. 1959;146:594–617. doi: 10.1113/jphysiol.1959.sp006214. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Kirshblum S, Lim S, Garstang S, Millis S. Electrodiagnostic changes of the lower limbs in subjects with chronic complete cervical spinal cord injury. Arch Phys Med Rehabil. 2001;82:604–607. doi: 10.1053/apmr.2001.22348. [DOI] [PubMed] [Google Scholar]
- 13.Burns A, Lemay MA, Tessler A. Abnormal spontaneous potentials in distal muscles in animal models of spinal cord injury. Muscle Nerve. 2005;31:46–51. doi: 10.1002/mus.20229. [DOI] [PubMed] [Google Scholar]
- 14.Benecke R, Berthold A, Conrad B. Denervation activity in the EMG of patients with upper motor neuron lesions: time course, local distribution and pathogenetic aspects. J Neurol. 1983;230:143–51. doi: 10.1007/BF00313625. [DOI] [PubMed] [Google Scholar]
- 15.Jankovic J. Can peripheral trauma induce dystonia or other movement disorders? Yes! Mov Disord. 2001;16(1):7–12. doi: 10.1002/1531-8257(200101)16:1<7::aid-mds1005>3.0.co;2-0. [DOI] [PubMed] [Google Scholar]
- 16.Hiasa Y, Mitsui T, Kunishige M, Oshima Y, Matsumoto T. Central motor conduction in cervical dystonia with cervical spondylotic myelopathy. Clin Neurol Neurosurg. 2005;107:482–485. doi: 10.1016/j.clineuro.2004.12.006. [DOI] [PubMed] [Google Scholar]
- 17.Harvey PJ, Li X, Li Y, Bennett DJ. Endogenous monoamine receptor activation is essential for enabling persistent sodium currents and repetitive firing in rat spinal motoneurons. J Neurophysiol. 2006;96(3):1171–86. doi: 10.1152/jn.00341.2006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Li Y, Gorassini MA, Bennett DJ. Role of persistent sodium and calcium currents in motoneuron firing and spasticity in chronic spinal rats. J Neurophysiol. 2004;91(2):767–83. doi: 10.1152/jn.00788.2003. [DOI] [PubMed] [Google Scholar]
- 19.Gilbert SL, Zhang L, Forster ML, Anderson JR, Iwase T, Soliven B, et al. Trak1 mutation disrupts GABA(A) receptor homeostasis in hypertonic mice. Nat Genet. 2006;38(2):245–50. doi: 10.1038/ng1715. [DOI] [PubMed] [Google Scholar]
- 20.Hornby G, TG, Heckman CJ, Harvey RL, Rymer WZ. Changes in voluntary torque and electromyographic activity following oral baclofen. Muscle Nerve. 2004;30:784–795. doi: 10.1002/mus.20176. [DOI] [PubMed] [Google Scholar]
- 21.Burns AS, Meythaler JM. Intrathecal baclofen in tetraplegia of spinal origin: efficacy for upper extremity hypertonia. Spinal Cord. 2001;39:413–419. doi: 10.1038/sj.sc.3101178. [DOI] [PubMed] [Google Scholar]
- 22.Nogués MA, Leiguarda RC, Rivero AD, Salvat F, Manes F. Involuntary movements and abnormal spontaneous EMG activity in syringomyelia and syringobulbia. Neurology. 1999;52(4):823–34. doi: 10.1212/wnl.52.4.823. [DOI] [PubMed] [Google Scholar]