

Abstract
Bilateral parietal thinning is an uncommon condition. We present a 72 year-old female with no history of head injury, inflammatory or malignant disease who presented with painless scalp depression in bilateral parietal regions. The skull radiography and computed tomography findings are presented.
Key words: Parietal bones, bilateral thinning, radiology, Hong Kong
Background
Bilateral parietal thinning is an uncommon condition. We present a 72 year-old female with no history of head injury, inflammatory or malignant disease who presented with painless scalp depression in bilateral parietal regions. The skull radiography and computed tomography findings are presented.
Patient and case report
A 72 year-old Chinese female complained of occasional dizziness during her routine follow-up for bilateral total hip replacement. She was noted to have painless bilateral scalp depressions in the parietal regions during physical examination. She had no history of head injury. She had past medical history of Parkinson’s disease, thyrotoxicosis treated with radio-isotope therapy (Iodine-131) 9 years ago and currently in remission, bilateral hip dysplasia with bilateral total hip replacement done 8 years and 2 years ago, and depression.
Blood results showed normal renal and liver functions with normal serum calcium level, in addition to normal thyroxine level and thyroid stimulating hormone level. Computed Tomography demonstrated bilateral symmetrical thinning of the parietal bones attributed to loss of diploe and thinning of the outer table (Figure 1). The inner table was intact without associated soft tissue mass or vascular lesions. Underlying brain parenchyma was also intact.
Figure 1:
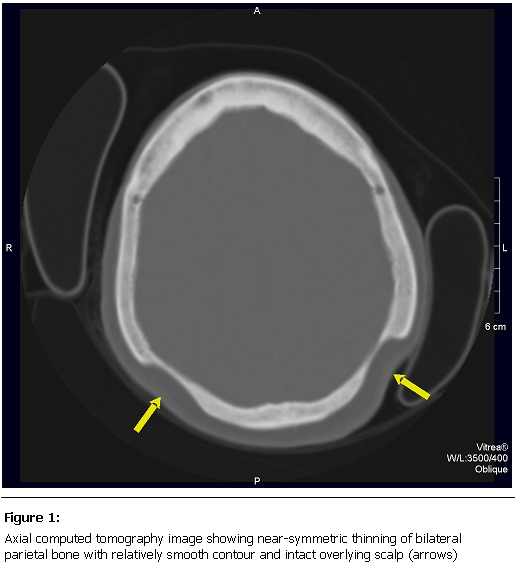
Axial computed tomography image showing near-symmetric thinning of bilateral parietal bone with relatively smooth contour and intact overlying scalp (arrows)
The patient had radiographs of the skull taken at the age of 66 years old when she presented with depression over the scalp in bilateral parietal region. The skull radiographs was regarded as normal on this occasion. Review of the anteroposterior radiograph of the skull (Figure 2) demonstrated symmetrical smooth depression in each parietal bone. In the centre of the depression there was a lack of diploic bone and of the outer table. Lateral radiograph of the skull (Figure 3) demonstrated a large, homogenous radiolucent area without marginal osteosclerotic changes in the upper parietal region.
Figure 2:
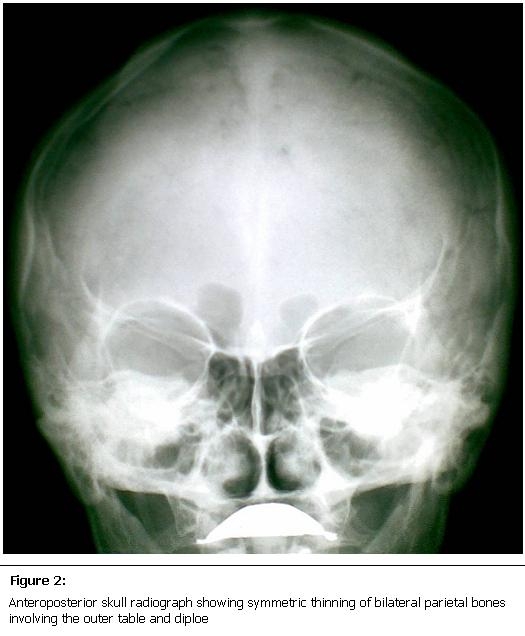
Anteroposterior skull radiograph showing symmetric thinning of bilateral parietal bones involving the outer table and diploe
Figure 3:
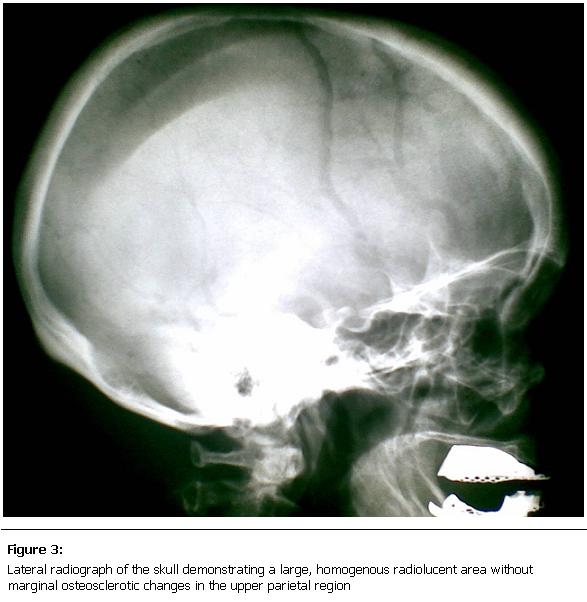
Lateral radiograph of the skull demonstrating a large, homogenous radiolucent area without marginal osteosclerotic changes in the upper parietal region
Discussion
Bilateral thinning of the parietal bones is a condition known since the 18th century [1]. Some have considered this as a non-progressive congenital dysplasia of the diploe [2]. Others have postulated that the thinning may be due to an acquired and progressive disease and not an anatomic variant or congenital dysplasia of the diploe [2]. These diseases include acute inflammatory atrophy associated with trauma, primary and metastatic tumors, Gorham-Stout disease, diabetes mellitus, and prolonged steroid therapy [3].
Some have concluded that bilateral parietal thinning is associated with post-menopausal and senile osteoporosis [2]. Histopathologic studies have demonstrated a lack of osteoclasts, suggesting that parietal thinning may be related to osteoporosis with decreased bone formation rather than increased bone destruction [1]. Some have concluded that bilateral parietal thinning may be due to continuous pressure from the exterior, with its resultant interference with the blood supply to the parietal bone [4]. It has been postulated that senile changes in the temporal artery is a possible cause of bilateral parietal thinning [4]. There was also suggestion that this condition is hereditary [4].
Parietal thinning is an uncommon condition, with prevalence of 0.25 – 0.8% [1]. It is more common in women than in men [5]. The characteristic site of bilateral parietal thinning is the area between the sagittal suture and the parietal prominence. Imaging features in skull radiograph include symmetrical thinning of bilateral parietal bones involving the outer table and diploe of the skull, giving rise to the scalloped appearance [5]. The inner table is usually intact [1].
Features in bone scintigraphy include symmetric, well-defined photon defects in both parietal regions [5]. Clinical presentation varies from palpable painless scalp depressions to pain on the areas of parietal thinning and even death following fracture through the thinned areas [1, 3]. Cases of progressive bilateral parietal thinning have been reported [1]. It is possible that if this condition is progressive, it may result in symmetrical perforations [4]. Cases of parietal perforations have been reported [4]. In cases of slowly progressive bony thinning, cranioplasty may be required to prevent exposure of the brain to atmospheric pressure [3].
Conclusion
Bilateral parietal thinning is an uncommon condition. This report highlights the possible progressive nature of this condition and its radiological features.
Conflict of interest
The authors declared they have no conflicts of interest.
References
- 1.Cederlund C. G., Adnren L, Olivecrona H. Progressive Bilateral Thinning of the Parietal Bones. Skeletal Radiol. 1982;8:29–33. doi: 10.1007/BF00361365. http://www.ncbi.nlm.nih.gov/pubmed/7079780 This article on PubMed. [DOI] [PubMed] [Google Scholar]
- 2.Dutta Pratap C. Bilateral Parietal Thinning in Bronze Age Skull. British Medical Journal. Br Med J. 1969 Jan 4;1(5635):55. doi: 10.1136/bmj.1.5635.55. http://www.ncbi.nlm.nih.gov/pubmed/5761910 This article on PubMed. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Tsutsumi Satoshi, Yasumoto Yukimasa, Ito Masanori. Idiopathic Calvarial Thinning. Neurol Med Chir (Tokyo) 2008 Jun;48(6):275–8. doi: 10.2176/nmc.48.275. http://www.ncbi.nlm.nih.gov/pubmed/18574336 This article on PubMed. [DOI] [PubMed] [Google Scholar]
- 4.Durward Archibald. A note on symmetrical Thinning of the Parietal Bones. J Anat. 1929 Apr;63(Pt 3):356–62. http://www.ncbi.nlm.nih.gov/pubmed/17104234 This article on PubMed. [PMC free article] [PubMed] [Google Scholar]
- 5.Lim Seok Tae, Sohn Myung-Hee. Bilateral Symmetric Photon Defects in the Parietal Bones on Tc-99m MDP Bone Scintigraphy – Bilateral Parietal Thinning. Clinical Nuclear Medicine. 2001;26:570–571. doi: 10.1097/00003072-200106000-00027. http://www.ncbi.nlm.nih.gov/pubmed/11353318 This article on PubMed. [DOI] [PubMed] [Google Scholar]