

Abstract
Background
Strategies are needed to improve the translation of clinical trial results into practice. We assessed the impact of the ALLHAT/JNC7 Dissemination Project’s academic detailing component on thiazide-type diuretic prescribing (ALLHAT indicates Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial: JNC7 indicates the Seventh Report of the Joint National Committee on Detection, Evaluation, and Treatment of High Blood Pressure).
Methods
We used two national databases available from IMS Health: a physician survey of medications reported for hypertension and a pharmacy dispensing database on antihypertensive medications. At a county level, we correlated medication data with Dissemination Project intensity. Practices before the Dissemination Project in 2004 were compared to those after its completion in 2007. We also examined 2000–2008 national trends.
Results
Academic detailing reached 18,524 physicians in 1698 venues via 147 investigator-educators. We noted an association between ALLHAT/JNC7 academic detailing activities and increased prescribing of thiazide-type diuretics. Physician survey data showed that the percentage of hypertension visits where the physician recorded where a thiazide-type diuretic was noted increased the most in counties with the greatest activities (8.6%, from 37.9% to 46.5%) compared to counties with moderate-level (2% change), low-level (−2%) and no activities (2%, p for trend <0.05). Pharmacy dispensing data showed that thiazide-type diuretic prescribing increased by 8.7% in counties with Dissemination Project activities compared to 3.9% in those without activities (p<0.001). Nationally, thiazide-type diuretic use did not increase between 2004 and 2008.
Conclusions
The ALLHAT/JNC7 Dissemination Project was associated with a small effect on thiazide-type diuretic use consistent with its small dose and the potential of external factors to diminish its impact. Academic detailing may increase physicians’ implementation of clinical trial results thereby making prescribing more consistent with evidence.
INTRODUCTION
Ensuring that important clinical trial findings are reflected in the practices of community physicians remains a substantial challenge. Many studies indicate that evidence-based recommendations diffuse into widespread community use only slowly and then incompletely (1–3). This failure to put scientific findings into practice not only compromises societal return on clinical trial investment, but also weakens the scientific basis of clinical care.
Evidence accumulated through national prescribing information suggests that the publication of the Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT) findings (4) had a significant initial impact on prescribing patterns. Following publication of the final ALLHAT results in 12/2002, thiazide-type diuretic use increased, calcium channel blocker (CCB) use declined, and angiotensin converting enzyme (ACE) inhibitor use failed to continue its previous upward trend (5). The incorporation of the ALLHAT results into the 12/2003 Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC7) further emphasized that relatively low levels of thiazide-type diuretic prescribing were at odds with evidence-based recommendations (6). Unfortunately, trends in antihypertensive prescribing behavior following ALLHAT and publication of guidelines may not have been sustained (5).
This experience, as well as information from other trials and guidelines, demonstrates that traditional, academically-focused modes of clinical trial result dissemination are inadequate. Additional strategies are needed to permanently alter practices to reflect new scientific evidence. A range of alternative approaches has been proposed, including clinical audit, patient empowerment, computerized reminders, pay-for-performance incentives, academic detailing, and continuing medical education (7). Numerous sources of information suggest that interventions focused on increasing physician knowledge through educational strategies are unlikely to be successful by themselves (8).
Academic detailing incorporates many of the approaches used in pharmaceutical marketing (9–11). By using persuasive, individualized small group or one-on-one communication of key points, detailing can summarize findings, suggest concrete changes in practice patterns, and explore potential barriers to change. In addition, by targeting specific physicians recognized as “opinion leaders,” resources can be concentrated on locally influential prescribers.
Several systematic reviews have examined the effectiveness of academic detailing in changing clinical practice and found this type of intervention to be effective (9,12–16). The effectiveness of academic detailing is described as ranging from small (9) to strong (17) with results that are consistently favorable (9,14,16). The effectiveness of academic detailing in affecting prescribing practices is particularly prominent (9,14,17). In this situation, even small changes in prescribing may be important when the population affected is large or where large cost differences exist between alternative medications (9).
We set out to evaluate the success of an academic detailing model, a component of the ALLHAT/JNC7 Dissemination Project, in changing national hypertension prescribing practices. Using national U.S. data on antihypertensive prescribing by county and measures of the intensity of ALLHAT/JNC7 academic detailing by county, we hypothesized the increasing local intensity of this intervention would be associated with increased prescribing of thiazide-type diuretics.
METHODS
To evaluate the impact of the ALLHAT/JNC7 Dissemination project, we analyzed the relationship between aggregate county information on the extent of academic detailing and temporal changes in thiazide-type diuretic use. Separate analyses were conducted using two national databases available from IMS Health (Plymouth Meeting PA): 1) a survey of office-based physicians and 2) pharmacy data on medication dispensing.
ALLHAT/JNC7 Dissemination Project
At the conclusion of the ALLHAT trial, a multi-component, joint dissemination project of ALLHAT and the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC7) was implemented. This project focused on extending traditional dissemination approaches by applying novel strategies based on intervention mapping theory (17,18) to health care provider persuasion, including local academic detailing and broader national scientific and media efforts. Further details of the JNC/ALLHAT Dissemination Project can be found in Bartholomew et al. (19).
The primary dissemination strategy was to reach medical care providers using 147 Investigator-educators at 1698 venues. Investigator-educators, mainly clinical investigators from ALLHAT, were chosen based on their ability to recruit and retain ALLHAT participants plus the input of the ALLHAT leadership, especially the regional coordinators. Investigator-educators were recruited to cover most of the US and to represent its demographic and geographic diversity. They were trained centrally to present ALLHAT results and the JNC7 guidelines (6) as the foundation for achieving blood pressure control. The main intervention messages were:
For most patients, blood pressure (BP) treatment goal is <140/90 mm Hg,
Most patients diagnosed with hypertension experience better BP control after adopting lifestyle modifications.
Most patients with Stage1 hypertension (BP 140-159/90-99) experience better BP control and better long term CVD risk when taking a thiazide-type diuretic.
Most patients with Stage 2 hypertension (BP>160/100) experience better BP control and better long term CVD risk when on a multi-drug regimen that includes a thiazide-type diuretic.
Most patients with uncontrolled BP benefit from the addition of a thiazide-type diuretic.
Each Investigator-educator’s goal was to make 12 presentations over a 12-month period to small, selected groups of key practitioners who prescribe medications for hypertension. At these encounters, the investigator-educators selected from centrally developed portfolio of training slides. Individualized communication with community physicians was encouraged, including specialized materials such as newsletters, pocket cards summarizing blood pressure control messages, JNC7 reference cards, and other items relevant to cardiovascular disease risk reduction (19). Press kits also were provided to Investigator-educators to use with community media. ALLHAT/JNC7 dissemination presentations took place beginning in 9/2004 and continued through 3/2007 and included sites in 41 states plus the District of Columbia. There was substantial variation in the geographic reach of the project, thus creating a natural experiment to explore the correlation between changes in prescribing practice and intervention intensity.
Several secondary project strategies for dissemination included reaching health care providers through professional associations and contacting formularies to encourage antihypertensive prescription according to JNC7 guidelines. Thus, the Dissemination project had both local and national components aimed at increasing thiazide-type diuretic prescribing.
Intervention Intensity
To evaluate the hypothesis that increasing intensity of the ALLHAT/JNC7 Dissemination Project was associated with increasing thiazide-type diuretic use, we identified the extent of local project activities. For each U.S. county, we identified whether any ALLHAT/JNC7 academic detailing efforts took place and, if so, the intensity (or dose) of those efforts. Intensity was measured as the number of physician participants contacted by the Investigator-educators per 100,000 population members aged 50 years and older based on year 2000 U.S. Census data (20). Nationally, the project made 1698 presentations to 18,524 physician contacts (19). This equates to a mean effort level of 24 contacts per 100,000 population members aged 50 years and older for the entire nation and 52 in those 368 counties where dissemination activities occurred. By county, efforts ranged from 0.3 to a high of 5546 with a median of 63.0. We categorized all U.S. counties into those receiving no efforts (2773 counties with 41.3 million individuals >50 yrs) and those that received any dissemination, among which we created three strata of counties by dissemination level. Low-level efforts occurred in 82 counties (12.2 million target population) with effort rates ranging from 0.3 to 15.9 clinician contacts per 100,000 population >50 yrs. (mean 5.5). Moderate-level efforts occurred in 79 counties (13.1 million target population) with effort rates ranging from 16 to 48 (mean 30). High-level efforts occurred in 207 counties (target population 10.2 million) with effort rates ranging from 50 to 5546 (mean 136).
Data Sources on Prescribing
National Disease and Therapeutic Index (NDTI)™
NDTI is a continuing physician survey conducted by IMS HEALTH. NDTI provides nationally representative diagnostic and prescribing information on patients treated by office-based physicians in the continental U.S. (21). A random sample of office-based physicians is selected through random stratified sampling by specialty and geographic region. Approximately 4,800 physicians participate each calendar quarter and each physician is randomly assigned two consecutive workdays per quarter for data collection. Physicians provide information on each patient encounter during their data collection period. Over 90% of the hypertension visits occurred in physician offices with the remaining being telephone calls, nursing home visits, and hospital visits. Medication reporting is diagnosis-specific and reflects the physician’s best knowledge of new or continuing medications intended to treat a specific diagnosis. Hypertension visits were reported under the International Classification of Diseases, Ninth Revision (ICD-9) diagnosis code 401 (22). We report national estimates that were extrapolated from the sample data for visits by patients of all ages with this diagnosis. With the exception of Hawaii and Alaska, data from at least one county was available for all states and the District of Columbia (DC) within NDTI. The sample of NDTI physicians overlapped with dissemination efforts in 176 counties, representing 38 states plus the District of Columbia. The county represents the location of the physician’s office. For each estimate, 95% confidence intervals were available via estimates of the relative standard error.
Xponent™
The IMS Health Xponent™ database consists of a national computerized sample of approximately 36,000 retail pharmacies (23). These stores, while not a randomly selected subset, are sampled from IMS Health’s pharmacy database, accounting for more than half of all retail pharmacies in the U.S. and are projected to nationally representative estimates. Pharmacy data are collected daily and reported in monthly aggregates with the prescription as the unit of analysis. The IMS Health Xponent database, covering approximately 70% of retail pharmacy dispensing, provided county-level geographic detail. Commercial mail order pharmacies, which represent 6% of total prescriptions, were not included. With the exception of Hawaii and Alaska, data were available from all states and the District of Columbia (DC), including data from 360 counties where dissemination efforts occurred, representing 41 states plus the District of Columbia. The county represents the location of the pharmacy. National estimates were available representing projections to a national level for drugs dispensed to patients of all ages regardless of diagnosis. For each estimate, 95% confidence intervals were available via estimates of the relative standard error. Of note, estimates from the Xponent were associated with less statistical uncertainty compared to NDTI.
Antihypertensive Medication Classes
We organized physician reporting of antihypertensive medications into 6 drug classes. In particular, we focused on the prescribing of thiazide-type diuretics, including these drugs alone or in combination products. Thiazide-type diuretics included products containing hydrochlorothiazide, chlorthalidone, metolazone, indapamide, methyclothiazide, chlorothiazide, benzthiazide, and trichlormethiazide. In the NDTI data, hydrochlorothiazide accounted for 89% of thiazide-type diuretic use in 2004 and 92% in 2007.
For each database, we used a different metric to assess changes in aggregate thiazide-type diuretic use. For the NDTI survey data, we assessed the likelihood that a patient with treated hypertension was receiving a thiazide-type diuretic: the denominator was the estimate of all visits by patients with hypertension where any treatment was reported and the numerator was the estimate of visits where a thiazide-type diuretic was reported as part of medication treatment (whether alone or as part of a multi-drug regimen). For the Xponent pharmacy dispensing data, we used the volume of thiazide-type diuretic prescriptions as the basis for measuring practice patterns. We calculated the mean number of thiazide-type prescriptions per day per person in the target population of those 50 years and older. For these calculations the number of thiazide-type diuretic prescriptions was divided by the number of days in the period of time being assessed. This quantity was, in turn, divided by the population 50 years and older to arrive at a rate of prescriptions per day per 1,000 persons.
While the metrics for assessing practice patterns in the NDTI and Xponent databases are quite distinct, they both aim to assess the use of thiazide-type diuretics relative to patients with hypertension or population-members at higher risk for hypertension. Both metrics contrast with alternatives that assess the fraction of all antihypertensive medications that are represented by thiazide-type diuretics. Our metrics, chosen a priori, are more consistent with guideline recommendations and the main message of the Dissemination Project that emphasized that diuretics would frequently be used in combination with other medications.
We also present trend data for all antihypertensive medication classes derived from the NDTI survey. For this analysis, we present the probability that a patient with treated hypertension will be receiving medications in the following classes: thiazide-type diuretics, calcium channel antagonists, beta-adrenergic antagonists, angiotensin-converting enzyme inhibitors, angiotensin II Type 1 receptor antagonists, and drugs in all other classes (including centrally acting agents, alpha-adrenergic antagonists and other non-thiazide diuretics).
Statistical Analysis
Although a graphical approach was used to evaluate trends in prescribing, we used a predetermined algorithm for evaluating whether the Dissemination Project had resulted in a change in thiazide-type diuretic prescribing. Specifically, we compared prescribing immediately prior to the intervention (1/2004 through 9/2004) to prescribing immediately after the completion of the intervention (3/2007 through 12/2007). We determined whether changes in pre- vs. post prescribing were correlated with the intensity of the intervention. Using SAS (24), we evaluated these differences by a Chi-square test for trend with a p < 0.05 as our level of significance for rejecting the null hypothesis that pre- vs. post-intervention change in thiazide-type diuretic prescribing did not differ by level of intervention intensity.
RESULTS
Academic detailing was conducted by 147 investigator educators in 1698 presentations to 18,524 participants in 41 states and the District of Columbia between September 2004 and March 2007 (19).
National Disease and Therapeutic Index (NDTI)
Among drug-treated visits for hypertension, the likelihood that a thiazide-type diuretic was present among reported therapies increased from 37.1% immediately prior to the intervention (1/2004 through 9/2004) to 39.6% following completion of the project (3/2007 through 12/2007). Those counties in the highest strata of dissemination efforts experienced the greatest increase in the report of thiazide-type diuretic use with an increase from 37.9% before the intervention to 46.5% after the intervention, a 23% relative increase (p<0.01). Those counties with lower rates of dissemination efforts were not statistically different from counties not receiving dissemination activities (Table 1). Patterns of thiazide-type diuretic use during the implementation of the intervention were generally intermediate to those observed before and after the intervention (Table 1).
Table 1.
Changes in Reported Thiazide-type Diuretics Among Visits by Patients with Treated Hypertension, IMS Health National Disease and Therapeutic Index
| Pre-Intervention Jan–Sept 2004 | During Intervention Oct 2004–Feb 2007 | Post-Intervention March–Dec 2007 | Change (Pre- vs. Post-Intervention) | |||||
|---|---|---|---|---|---|---|---|---|
| Visits by Patients with Treated Hypertension (in M) | Percentage of Treated Hypertension Patients on Thiazides | Visits by Patients with Treated Hypertension (in M) | Percentage of Treated Hypertension Patients on Thiazides | Visits by Patients with Treated Hypertension (in M) | Percentage of Treated Hypertension Patients on Thiazides | Change in Percentage on Thiazides | Percentage Change in Percent on Thiazides | |
| Counties with No JNC7/ALLHAT Dissemination | 19.1 | 37.1% | 59.9 | 38.9% | 18.5 | 39.4% | 2.3% | 6% |
| Counties with any JNC7/ALLHAT Dissemination | 18.8 | 37.1% | 57.9 | 37.8% | 20.8 | 39.7% | 2.6% | 7% |
| Lowest Intensity* | 6.2 | 38.3% | 19.0 | 35.1% | 6.6 | 36.7% | −1.6% | −4% |
| Moderate Intensity* | 6.2 | 35.2% | 21.4 | 36.2% | 8.1 | 37.1% | 1.9% | 6% |
| Highest Intensity* | 6.3 | 37.9% | 17.5 | 42.6% | 6.1 | 46.5% | 8.6% | 23% |
| All United States | 37.9 | 37.1% | 117.8 | 38.4% | 39.3 | 39.6% | 2.4% | 7% |
Lowest Intensity -- 0.3 to 15.9 clinician contacts per 100,000 population >50 yrs. (mean 5.5), Moderate Intensity -- 16 to 48 clinician contacts per 100,000 population >50 yrs. (mean 30), Highest Intensity -- 50 to 5546 clinician contacts per 100,000 population >50 yrs. (mean 136).
Trend data for the nation as a whole (Figures 1 and 2), indicate the sizable shift in the selection of medications for the treatment of hypertension following the 12/2002 publication of the ALLHAT results. Immediately after this time, there was an increase in thiazide-type diuretic use and a decline in ACE inhibitor use. Overall changes occurring in conjunction with the ALLHAT/JNC7 Dissemination Project suggest a small increase in the use of thiazide-type diuretics. But more prominent, however, are increases in the use of ARBs and decreases in the use of calcium channel antagonists and angiotensin-converting enzyme inhibitors.
Figure 1.
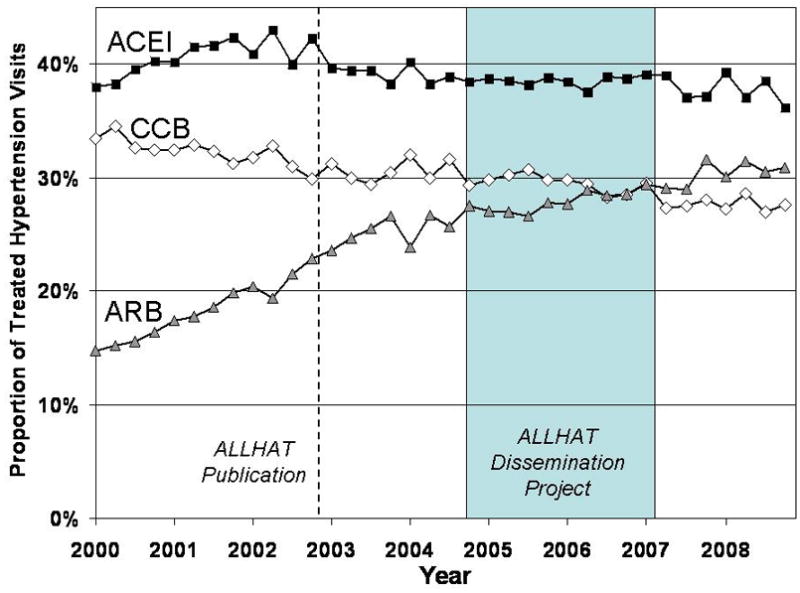
Proportion visits with a drug class reported among patients with drug-treated hypertension. IMS Health National Disease and Therapeutics Index, 2000 through 2008. ACEI = angiotensin-converting enzyme inhibitor; CCB = calcium channel blocker, ARB = angiotensin II Type 1 receptor blocker.
Figure 2.
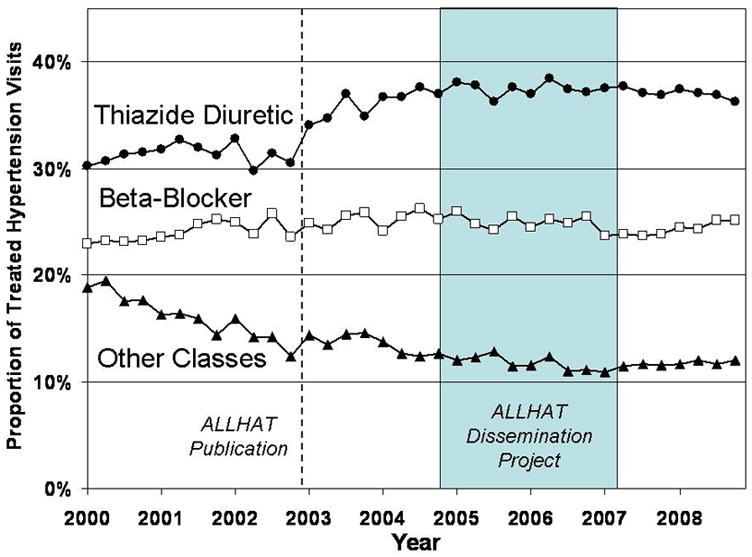
Proportion visits with a drug class reported among patients with drug-treated hypertension. IMS Health National Disease and Therapeutics Index, 2000 through 2008. Other classes = alpha adrenergic receptor blockers, potassium-sparing diuretics, loop diuretics, and centrally-acting agents.
Xponent Database
The number of thiazide-type diuretic prescriptions dispensed by pharmacists increased nationally from 4.13 prescriptions per day per 1000 persons prior to the Dissemination Project to 4.39 following the project. Those counties receiving any dissemination activities increased from 4.30 to 4.68 over this same time period, an increase of 8.7%. Those counties without activities experienced less marked growth in thiazide-type dispensing (from 3.99 to 4.15, a 3.9% increase, p<0.001 vs. those counties receiving services). There was no clear pattern differentiating changes that occurred among counties receiving different levels of dissemination activities (Table 2). In addition, patterns of dispensing during the intervention (October 2004 through February 2007) varied considerably (Table 2).
Table 2.
Changes in Thiazide-type Diuretic Pharmacy Dispensing, Thiazide-type Diuretic Prescriptions per Day per 1000 Persons, IMS Health Xponent Database
| Pre-Intervention Jan–Sept 2004 | During Intervention Oct 2004–Feb 2007 | Post-Intervention March–Dec 2007 | Change (Pre- vs. Post-Intervention) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Population ≥ 50 yrs (in M) | Thiazide Prescriptions per Day (in 1000s) | Rx per Day per 1000 persons | Thiazide Prescriptions per Day (in 1000s) | Rx per Day per 1000 persons | Thiazide Prescriptions per Day (in 1000s) | Rx per Day per 1000 persons | Change in Prescription Rate | Percentage Change in Rx rate | |
| Counties with No JNC7/ALLHAT Dissemination | 41.3 | 164.8 | 3.99 | 178.2 | 4.32 | 171.2 | 4.15 | 0.16 | 3.9% |
| Counties with any JNC7/ALLHAT Dissemination | 35.5 | 152.8 | 4.30 | 151.0 | 4.25 | 166.0 | 4.68 | 0.37 | 8.7% |
| Lowest Intensity* | 12.2 | 47.6 | 3.90 | 47.8 | 3.92 | 51.3 | 4.20 | 0.30 | 7.8% |
| Moderate Intensity* | 13.1 | 53.1 | 4.05 | 53.4 | 4.08 | 58.4 | 4.46 | 0.40 | 10.0% |
| Highest Intensity* | 10.2 | 52.1 | 5.11 | 49.7 | 4.87 | 56.4 | 5.53 | 0.42 | 8.1% |
| All United States | 76.9 | 317.5 | 4.13 | 329.2 | 4.28 | 337.2 | 4.39 | 0.26 | 6.2% |
Lowest Intensity -- 0.3 to 15.9 clinician contacts per 100,000 population >50 yrs. (mean 5.5), Moderate Intensity -- 16 to 48 clinician contacts per 100,000 population >50 yrs. (mean 30), Highest Intensity -- 50 to 5546 clinician contacts per 100,000 population >50 yrs. (mean 136).
DISCUSSION
We found evidence associating the ALLHAT/JNC7 Dissemination Project with increased use of thiazide-type diuretics in the U.S. Although we had hypothesized a graded relationship between intervention intensity and thiazide-type diuretic use, this pattern was evident only in the NDTI physician survey data. Nonetheless, both data sources indicate that diuretic prescribing increased nationally and that counties not receiving the intervention had slower growth in diuretic use when patterns before and after the time frame of the intervention are compared. We acknowledge that this is an ecological association and that counties selected for dissemination efforts may have differed from other counties.
The magnitude of change associated with the intervention is small, likely corresponding to the limited dose of the intervention. The observed pattern of change in thiazide-type diuretic prescribing also differs somewhat between the survey information on prescribing (NDTI) and pharmacy dispensing information (Xponent).
The intervention focused on persuasive communication about prescribing behavior presented by community colleagues, as distinct from an emphasis on clinician knowledge. This strategy used methods known to be effective in academic detailing, including role modeling by peers, visits to individuals or practice groups and careful delineation of the target behavior (19). While designed to be more intensive than continuing medical education, the intervention did not include individualized efforts to change prescribing, such as performance standards, behavioral feedback strategies, or practice-based redesign. Greater intensity and individualization might have had greater impact, but would have compromised the national reach of the Dissemination Project. Nonetheless, our findings are consistent with past studies of academic detailing and show its potential to motivate changes in physician practices.
Other issues may have blunted the ability of the ALLHAT/JNC7 Dissemination Project to convince community physicians of the relevance of ALLHAT’s population and methods, and the applicability of the trial’s findings. The intervention began nearly two years after the publication of the ALLHAT summary results and there was limited opportunity to generate media coverage that might have synergistically magnified the effect of the intervention. During the time period of the intervention, several other clinical trials were published that were promoted as casting doubt on the role of thiazide-type diuretics (25,26). This may have complicated the messages delivered by the intervention and reduced the likelihood of prescribing changes. Similarly, there was substantial questioning of the ALLHAT findings by recognized hypertension authorities, as well as by the pharmaceutical industry, that likely reduced the potential impact of the results on clinical practice (27). For example, unwarranted concerns regarding the use of thiazide-type diuretics in patients with diabetes may have hampered efforts to alter prescribing practices (28). ALLHAT leaders, however, have published multiple commentaries in high-prestige journals that enumerate counterarguments to such criticisms (29–31).
While the ALLHAT/JNC7 Dissemination Project may have increased the use of thiazide-type diuretics, other changes in prescribing practices are less consistent with evidence. In particular, the continued increase in the use of ARBs and the decrease in ACE inhibitors and calcium channel blockers represent trends that are not congruent with the accumulated evidence on outcomes. These changes add substantially to the cost of hypertension treatment, especially given the recent availability of multiple generic ACE inhibitors and calcium channel blockers.
Limitations
The findings of this study should be interpreted cautiously in the context of the following limitations. This was an ecological analysis conducted at the level of U.S. counties and any association does not necessarily imply a causal relationship between the Dissemination Project and changing patterns of thiazide-type diuretic use. Furthermore, the sites selected for Investigator-educator activities were not selected randomly and may differ from those in other geographic areas. Despite this potential, the non-random allocation of counties to differing intensity levels of the intervention is unlikely to explain our results. Investigator-educators were selected based on their interest and neither these physicians nor project staff were aware of baseline patterns of thiazide-type diuretic use. Specific efforts were made to select a geographically diverse panel of investigator-educators.
Use of the population aged 50+ years in the Xponent analysis provides an inexact proxy for the population with hypertension. There also may be substantial variation induced by other geographically-varying factors (e.g., drug promotion of non-thiazides), as well as variation connected with the measurement of prescribing patterns. This variation may have made it difficult to detect a more sizable effect of the Dissemination Project and may account, in part, for the differences in findings between the two data sources.
NDTI and Xponent are different data sources and represent distinct populations that might differ in their response to the intervention. NDTI data on office visits by patients with hypertension will over-represent patients making frequent doctor’s visits, including those requiring changes in their medications. Xponent, representing pharmacy data on new and refilled antihypertensive medications, will include patients treated with these drugs for reasons other than hypertension. To a greater extent than NDTI, Xponent will reflect patterns of refilling and discontinuation influenced by factors beyond physicians’ control. These two sources of information also differ in the metric of measuring diuretic use and potential biases. Dissemination efforts were coded by physician office location in NDTI and pharmacy location in Xponent. With their advantages and disadvantages, the use of NDTI and Xponent together provides some degree of cross-validation given their largely concordant results.
Conclusions
Although other explanations cannot be excluded, there was a statistically significant increase in thiazide-type diuretic prescribing that was geographically associated with clinical investigator centered academic detailing aimed at increasing use of thiazide-type diuretics. These dissemination efforts focused on the implementation of guidelines derived from the ALLHAT findings, but also emphasized the role of thiazide-type diuretics in patients requiring multiple medications. Corresponding to the minimal intervention dose, the effect of the ALLHAT/JNC7 Dissemination Project is small. In addition, other factors, including controversy regarding the appropriate role of thiazide-type diuretics, may have blunted the intervention’s impact. Academic detailing has the potential to improve prescribing patterns, but may require greater intensity to facilitate translation of clinical trials evidence into community practice.
Acknowledgments
Funding/Support: This study was supported by contract N01-HC-35130 from the National Heart, Lung, and Blood Institute, as well as a National Heart, Lung, and Blood Institute NHLBI mentoring award (RSS, K24HL086703). The ALLHAT investigators acknowledge contributions of study medications supplied by Pfizer, Inc. (amlodipine), AstraZeneca (atenolol and lisinopril) and Bristol-Myers Squibb (pravastatin) and financial support provided by Pfizer, Inc. The statements, findings, conclusions, views, and opinions contained and expressed in this article are based in part on data obtained under license from the following IMS Health Incorporated information services: National Disease and Therapeutic Index™ (2000–2008) and Xponent™ (2004–2007), IMS Health Incorporated. Disclaimer: The statements, findings, conclusions, views, and opinions contained and expressed herein are not necessarily those of IMS Health Incorporated or any of its affiliated or subsidiary entities.
Footnotes
Financial Disclosures (5 years): RSS has consulted for Bayer Corporation and has had grants/contracts with Procter and Gamble, GlaxoSmithKline, Toyo Shinyaku, and Wako. WCC has consulted for Abbott Laboratories, Bristol-Myers Squibb, Calpis, Daichi Sankyo, Forest Pharmaceuticals, Gilead Colorado, Johnson and Johnson, King, Myogen, Novartis, Pfizer, Pharmacopeia, Reddy Pharmaceuticals, Roche, Sankyo, Sanofi Aventis, Sanofi Synthelabo, Sciele, and Takeda; has received honoraria from Astra-Zeneca, Boehringer Ingelheim, Forest Pharmaceuticals, King, Novartis, Pfizer, Sankyo, Sanofi Aventis, and Sciele; and has had grants/contracts with Abbott Laboratories, Astra-Zeneca, Biovail, King, and Novartis. BRD has held financial interest in Amgen and has consulted for BioMarin, Forest Pharmaceuticals, GlaxoSmithKline, Merck, Proctor and Gamble, and Takeda. CDF has received honoraria from Novartis, Sanofi-Synthelabo, and Wyeth; has had grants/contracts with GlaxoSmithKline; and has been on the board of directors for Wyeth. LKB, JAC, GD, PTE, LBP, SLP, and PKW have no conflicts to report.
References
- 1.Lenfant C. Clinical research to clinical practice lost in translation? N Engl J Med. 2003;349:868–74. doi: 10.1056/NEJMsa035507. [DOI] [PubMed] [Google Scholar]
- 2.Woolf SH. The meaning of translational research and why it matters. JAMA. 2008;299:211–213. doi: 10.1001/jama.2007.26. [DOI] [PubMed] [Google Scholar]
- 3.Stafford RS, Radley DC. The underutilization of cardiac medications of proven benefit, 1990 to 2002. J Am Coll Cardiol. 2003;41:56–61. doi: 10.1016/s0735-1097(02)02670-0. [DOI] [PubMed] [Google Scholar]
- 4.ALLHAT. Major outcomes in high-risk hypertensive patients randomized to angiotensin-converting enzyme inhibitor or calcium channel blocker vs diuretic: The Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT) JAMA. 2002;288:2981–97. doi: 10.1001/jama.288.23.2981. [DOI] [PubMed] [Google Scholar]
- 5.Stafford RS, Monti V, Furberg CD, Ma J. Long-term and short-term changes in antihypertensive prescribing by office-based physicians in the U.S. Hypertension. 2006;48:213–8. doi: 10.1161/01.HYP.0000229653.73128.b6. [DOI] [PubMed] [Google Scholar]
- 6.Chobanian AV, Bakris GL, Black HR, et al. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure - The JNC-7 Report. JAMA. 2003;289(19):2560–2572. doi: 10.1001/jama.289.19.2560. [DOI] [PubMed] [Google Scholar]
- 7.Grimshaw J, Eccles M, Thomas R, et al. Toward evidence-based quality improvement. Evidence (and its limitations) of the effectiveness of guideline dissemination and implementation strategies 1966–1998. J Gen Intern Med. 2006;21 (Suppl 2):S14–20. doi: 10.1111/j.1525-1497.2006.00357.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Cabana MD, Rand CS, Powe NR, et al. Why don’t physicians follow clinical practice guidelines? A framework for improvement. JAMA. 1999;282:1458–65. doi: 10.1001/jama.282.15.1458. [DOI] [PubMed] [Google Scholar]
- 9.O’Brien MA, Rogers S, Jamtvedt G, et al. Cochrane Database Syst Rev. 2007;2007;4:CD000409.2007. doi: 10.1002/14651858.CD000409.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Soumerai SB, Avorn J. Principles of educational outreach (‘academic detailing’) to improve clinical decision making. JAMA. 1990;263:549–56. [PubMed] [Google Scholar]
- 11.Simon SR, Majumdar SR, Prosser LA, et al. Group versus individual academic detailing to improve the use of antihypertensive medications in primary care: a cluster-randomized controlled trial. Am J Med. 2005;118:521–8. doi: 10.1016/j.amjmed.2004.12.023. [DOI] [PubMed] [Google Scholar]
- 12.Grimshaw JM, Thomas RE, MacLennan G, et al. Effectiveness and efficiency of guideline dissemination and implementation strategies. Health Technology Assessment. 2004;8(6):iii–iv. 1–72. doi: 10.3310/hta8060. [DOI] [PubMed] [Google Scholar]
- 13.Grimshaw JM, Shirran L, Thomas R, et al. Changing provider behavior: an overview of systematic reviews of interventions. Medical Care. 2001;39(Suppl II):II2–II45. [PubMed] [Google Scholar]
- 14.Grindrod KA, Patel P, Martin JE. What interventions should pharmacists employ to impact health practitioners’ prescribing practices? Ann Pharmacother. 2006;40:1546–57. doi: 10.1345/aph.1G300. [DOI] [PubMed] [Google Scholar]
- 15.Smith WR. Evidence for the effectiveness of techniques to change physician behavior. Chest. 2000;118:8S–17S. doi: 10.1378/chest.118.2_suppl.8s. [DOI] [PubMed] [Google Scholar]
- 16.Davis DA, Taylor-Vaisey A. Translating guidelines into practice. A systematic review of theoretic concepts, practical experience and research evidence in the adoption of clinical practice guidelines. CMAJ. 1997;157:408–16. [PMC free article] [PubMed] [Google Scholar]
- 17.Bartholomew LK, Parcel GS, Kok G. Intervention mapping: A process for developing theory-and evidence-based health education programs. Health Education & Behavior. 1998;25:545–563. doi: 10.1177/109019819802500502. [DOI] [PubMed] [Google Scholar]
- 18.Bartholomew LK, Parcel GS, Ko G, Gottlieb NH. Intervention Mapping: Designing Theory-and Evidence-Based Health Promotion Programs. Mayfield Publishing; Thousand Oaks, CA: 2000. [Google Scholar]
- 19.Bartholomew LK, Cushman WC, Cutler JA, et al. Getting clinical trial results into practice: design, implementation, and process evaluation of the ALLHAT/JNC7 Dissemination Project. Clinical Trials. 2009;6:329–43. doi: 10.1177/1740774509338234. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.U.S. Bureau of the Census. Population Estimates: Annual Estimates of the Resident Population by Age, Sex, Race, and Hispanic Origin for Counties. [last accessed 10/8/2009]; Downloaded from: http://www.census.gov/popest/counties/asrh/CC-EST2008-alldata.html.
- 21.Source: National Disease and Therapeutic Index™, January 2000–December 2008, IMS Health Incorporated. All Rights Reserved.
- 22.World Health Organization. Manual of the International Statistical Classification of Diseases, Injuries, and Causes of Death: Based on the Recommendations of the Ninth Revision Conference, 1975, and Adopted by the Twenty-Ninth World Health Assembly. Geneva: World Health Organization; 1977. [Google Scholar]
- 23.Source: Xponent™, January 2004–September 2004 and January 2007–September 2007, IMS Health Incorporated. All Rights Reserved.
- 24.SAS Institute. SAS Software, Version 9.1. Cary, NC: SAS Institute; 2008. [Google Scholar]
- 25.Dahlöf B, Sever PS, Poulter NR, et al. Prevention of cardiovascular events with an antihypertensive regimen of amlodipine adding perindopril as required versus atenolol adding bendroflumethiazide as required, in the Anglo-Scandinavian Cardiac Outcomes Trial-Blood Pressure Lowering Arm (ASCOT-BPLA): a multicentre randomised controlled trial. Lancet. 2005;366:895–906. doi: 10.1016/S0140-6736(05)67185-1. [DOI] [PubMed] [Google Scholar]
- 26.Wing LM, Reid CM, Ryan P, et al. A comparison of outcomes with angiotensin-converting--enzyme inhibitors and diuretics for hypertension in the elderly. N Engl J Med. 2003;348:583–92. doi: 10.1056/NEJMoa021716. [DOI] [PubMed] [Google Scholar]
- 27.Furberg CD, Hall MA, Sevick MA. Balancing commercial and public interests. Curr Control Trials Cardiovasc Med. 2004;5:6. doi: 10.1186/1468-6708-5-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Barzilay JI, Davis BR, Cutler JA, et al. Fasting glucose levels and incident diabetes mellitus in older nondiabetic adults randomized to receive 3 different classes of antihypertensive treatment: a report from the Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT) Arch Intern Med. 2006;166:2191–201. doi: 10.1001/archinte.166.20.2191. [DOI] [PubMed] [Google Scholar]
- 29.Davis BR, Furberg CD, Wright JT, et al. ALLHAT: setting the record straight. Ann Intern Med. 2004;141:39–46. doi: 10.7326/0003-4819-141-1-200407060-00013. [DOI] [PubMed] [Google Scholar]
- 30.Cutler JA, Davis BR. Thiazide-type diuretics and beta-adrenergic blockers as first-line drug treatments for hypertension. Circulation. 2008;117:2691–704. doi: 10.1161/CIRCULATIONAHA.107.709931. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Wright JT, Jr, Probstfield JL, Cushman WC, et al. ALLHAT findings revisited in the context of subsequent analyses, other trials, and meta-analyses. Arch Intern Med. 2009;169:832–42. doi: 10.1001/archinternmed.2009.60. [DOI] [PMC free article] [PubMed] [Google Scholar]