

The use of hypothermia to promote neurologic recovery after cardiac arrest has been based on the belief that the efficacy of this therapy is due to the consequent reduction in cerebral edema.8, 10 If this were true, hypertonic urea, which has been shown by Javid1,2 to be a remarkably effective agent in the treatment of cerebral edema, would be expected to have a similarly beneficial effect upon recovery. The present study is concerned with the experimental evaluation of this drug in the treatment of simulated cardiac arrest in dogs and monkeys.
During the experimentations, considerable data were accumulated on the maximum tolerance to cardiac arrest of the normothermic dog and monkey brain under optimum prearrest and resuscitative circumstances. This material has been analyzed in some detail since the period of safe total cerebral ischemia in both species has been longer than previously reported.
METHODS
Experiments were performed on 60 mongrel dogs and 19 Macaca mulatta monkeys. The animals were anesthetized with 25 to 30 mg. per kilogram of sodium pentobarbital and placed on a respirator4 supplied with 100 per cent oxygen. The animal temperatures were maintained at 37° C. with heating blankets during and after operation. Except for maintenance of body temperature and treatment with urea† or placebo solution, no postoperative care was provided after the animals were removed from the respirator. Other specific details of methodology are presented under the appropriate sections.
OPERATIVE TECHNIQUE FOR SIMULATED CARDIAC ARREST
The operative procedure is essentially the same for dogs and monkeys (Fig. 1). A thoracotomy is performed through the left fourth intercostal space. The aortic arch and its 2 branches (brachiocephalic trunk and left subclavian artery) are dissected free. Tapes are passed about the aorta, above the level of the first intercostal artery, and around the 2 branches of the arch. The superior and inferior venae cavae are then encircled with tapes, the former above the entrance of the azygos vein. The venae cavae, aorta, and the 2 arch branches are then occluded simultaneously (Fig. 1). When occlusion is terminated, the clamps are released simultaneously and the chest closed immediately with water-seal drainage.
Fig. 1.
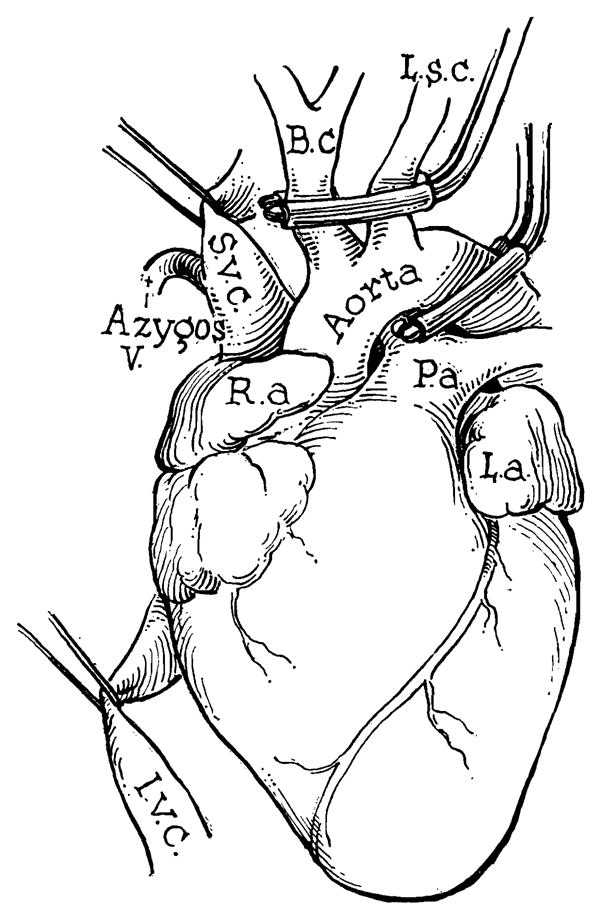
Method of simulated cardiac arrest. Operation is performed through the left chest. Note that circulation is retained to the coronary arteries.
During the period of cerebral ischemia, a diminutive systemic and pulmonary circulation is maintained. The only venous inflow to this system is from the azygos vein and the only systemic outflow is to the coronary arteries. In some cases the inflow appeared to be too great and vascular engorgement of the lungs slowly developed but, after release of the clamps, this disappeared immediately. The operative mortality rate in dogs was 5 per cent (due to ventricular fibrillation) and the procedure was especially well tolerated in monkeys in which there were no immediate deaths in 19 experiments. In 2 monkeys the occlusion was maintained for 60 and 90 minutes with maintenance of a strong heartbeat and restoration of normal circulation at the termination of occlusion.
Because the time of ischemia necessary to produce neurologic injury was longer than previously reported, a special effort was made to preclude the possibility that arterial blood was reaching the brain in some circuitous manner. In 2 monkeys, methylene blue was injected into the left ventricle. No dye reached either the spinal cord or brain. In 3 monkeys and several dogs, the brain was removed during occlusion so that the vertebral and cerebral arteries as well as the circle of Willis could be transected under direct vision. No arterial inflow whatever was present.
RESULTS
Factors That Influence the Period of Safe Occlusion in Dogs
Certain obvious factors will materially increase the period of occlusion necessary to cause permanent central nervous system damage. These include avoidance of partial occlusion of the venae cavae prior to complete test occlusion, insurance of a vigorous heartbeat at the conclusion of ischemia, and the use of 100 per cent oxygen. It was found, for example, that the time of ischemia necessary to produce brain injury was about 4 minutes less when the animal was respirated with compressed air than when oxygen was used.
More subtle influences were also important. At the beginning of the work a commercial respirator was used, supplied with 100 per cent oxygen. The necessary occlusion for brain injury in 10 dogs was 10½ minutes, a time comparable to that reported by Marshall5 and Zimmerman10 and their coworkers. Ultimately the electronic respirator designed by Lewis4 was employed, with the result that the time of ischemia for comparable injury was increased to 14 minutes. It was also found that efforts to promote early spontaneous respiration after the chest was closed led to a sharp rise in the mortality rate and an unpredictable reduction in the time necessary for occlusion. Consequently, the animals were maintained on the respirator for as long as 2 to 8 hours postoperatively and were removed only when they began to fight the mechanical control of their respiration.
Time of Complete Cerebral Ischemia in Dogs With Complete Recovery
Under the optimum conditions outlined above, 6 dogs were subjected to complete cerebral ischemia for 10 minutes. All recovered (Table I). Four dogs had occlusions for 11 minutes and 4 for 12 minutes. All of these animals eventually recovered but about one half required 24 to 48 hours before normal locomotor control was restored. Seven dogs were subjected to a period of occlusion for 13 minutes. Three of these did not recover completely, ataxia and drowsiness persisting for at least 1 week after operation. With occlusion for 14 minutes, two thirds of the animals either died from profound central nervous system injury (opisthotonus, extensor rigidity, coma) or manifested permanent neurologic deficit such as sleepfulness, ataxia, or head nodding (Table I).
Table I.
The Result of Different Periods of Complete Cerebral Ischemia in Dogs
| MINUTES OF OCCLUSION | NO. OF ANIMALS | RECOVERED | DIED OR PERMANENT INJURY |
|---|---|---|---|
| 10 | 6 | 6 | 0 |
| 11 | 4 | 4 | 0 |
| 12 | 4 | 4 | 0 |
| 13 | 7 | 4 | 3 |
| 14 | 18 | 4 | 14 |
Effect of Urea on Recovery After Cerebral Ischemia in Dogs
Thirty-seven dogs were subjected to 14 minutes of complete cerebral ischemia. Nineteen animals were given 30 per cent urea intravenously, made up in 5 per cent glucose/normal saline. The infusions were given 30 minutes after operation and every 12 hours thereafter until recovery was complete or until 3 days had passed. The dose was 1 Gm. of urea per kilogram and the infusions were given over a 30-minute period. Eighteen dogs were used for controls. Treatment was exactly the same in these animals except that 5 per cent glucose/normal saline infusions without urea were used.
The results with and without treatment with urea are shown in Table II. Six of the 19 dogs treated with urea recovered completely within 1 week. Three others recovered sufficiently to eat and survive indefinitely, but manifested ataxia and other findings of extrapyramidal injury. Ten of the 19 dogs died with profound neurologic injury.
Table II.
Effect of Treatment With Urea on Recovery After 14 Minutes of Cerebral Ischemia in Dogs
| TREATMENT WITH UREA | TREATMENT WITH PLACEBO | |
|---|---|---|
| No. of animals | 19 | 18 |
| Complete recovery | 6 | 4 |
| Permanent injury | 3 | 2 |
| Died | 10 | 12 |
In the untreated group, 4 of 18 controls recovered completely, 2 had incomplete recovery, and 12 died. Analysis of the results did not demonstrate statistically significant protection of the treated as compared to the untreated animals.
Time of Complete Cerebral Ischemia in Monkeys
Single monkeys were subjected to occlusion for 8, 10, and 12 minutes. Although recovery from anesthesia was slow, all animals were neurologically normal within 24 hours. Seven monkeys had occlusions for 14 minutes (Table III) with an immediate mortality rate of more than 50 per cent.
Table III.
The Result of Different Periods of Complete Cerebral Ischemia in Monkeys
| MINUTES OF OCCLUSION | NO. OF ANIMALS | RECOVERED | DIED OR PERMANENT INJURY |
|---|---|---|---|
| 8 | 1 | 1 | 0 |
| 10 | 1 | 1 | 0 |
| 12 | 4 | 1 | 0 |
| 14 | 7 | 2 | 5 |
The animals with 14 minutes of cerebral ischemia responded very sharply to this insult, either with complete recovery or with early death. In contrast to the dogs, in which a significant number of the animals lived despite serious neurologic deficit, none of the monkeys which did not recover normal locomotor control lived beyond 24 hours. These animals were obtunded or comatose, with sluggish or absent response to pain. Opisthotonus and extensor rigidity were occasionally seen but, generally, the stricken monkey was areflexic, with absent grasp and righting reflexes. In some cases, the monkeys could never be removed from the respirator, and in others they would assume an immobile position for many hours with increasing weakness and death.
Effect of Urea on Recovery After Cerebral Ischemia in Monkeys
Fourteen minutes of cerebral ischemia was imposed on 14 monkeys. Seven animals were treated with 30 per cent urea (1 Gm. per kilogram), and the other 7 with placebo injections. The results are shown in Table IV.
Table IV.
Effect of Treatment With Urea on Recovery After 14 Minutes of Cerebral Ischemia in Monkeys
| TREATMENT WITH UREA | TREATMENT WITH PLACEBO | |
|---|---|---|
| No. of animals | 7 | 7 |
| Complete recovery | 3 | 2 |
| Permanent injury | 0 | 1 |
| Died | 4 | 4 |
Four of the 7 controls died in from 7 to 24 hours after operation. Two of the controls recovered completely with no demonstrable harmful effects. One monkey apparently recovered completely, but a remarkable behavioral change soon became manifest. The animal had had a savage personality before operation, but postoperatively he was docile and affectionate. He soon developed an appetite for meat, a characteristic finding of bilateral temporal lobe destruction (Küver-Bucy syndrome3). At the autopsy 16 weeks after operation, no gross lesion of the temporal lobes was found.
Seven monkeys were treated with urea. Four animals died in from 8 to 16 hours. The other 3 recovered completely. Convalescence in the animals that recovered was characterized by a steady improvement in which there was no detectable change immediately after each urea injection. Similarly, urea produced no alteration in the state of wakefulness or responsiveness in the monkeys that died.
Autopsies were performed on all monkeys. The control animals all had cerebral edema with swollen gyri and tight approximation of the cortex to the dura. In the animals treated with urea the brains were slack and generally only remarkable for their lack of swelling.
DISCUSSION
Numerous methods have been used for experimental study of cerebral ischemia. Techniques which only involve occlusion of the vertebral and carotid arteries, either in the neck or the chest, provide inconstant results since an unknown quantity of blood reaches the brain through intercostal and other collateral pathways. The method used in the present study is a modification of the inflow-outflow occlusion method of Marshall and associates5 in which coronary arterial circulation is maintained during the time when all other systemic outflow is completely blocked. No arterial blood whatever reaches the brain during occlusion, and the test periods are sharply defined since the condition of the heart remains excellent before, during, and after occlusion. In our experience with occlusion through a right thoracotomy, as described by Marshall,5 the incidence of cardiac deterioration during the test period was high presumably because the aortic clamp must be applied too close to the coronary arteries. With inflow-outflow occlusion from a left approach, as employed in the present study, this complication was virtually eliminated.
In human beings the duration of cardiac arrest necessary to produce permanent neurologic injury is not known since the exact moment of arrest is difficult to determine, the catastrophe is usually preceded by variable periods of anoxia, shock, or other physiologic derangements, and the circulatory state is usually not ideal for some time after resuscitation has been completed.7 Many authors have stated that 3 to 5 minutes constitute the time limits beyond which cardiac arrest can be expected to cause neurologic sequellae. In the present study, it has been shown that complete cerebral ischemia can be tolerated in almost every case for 12 minutes by both the dog and monkey under the appropriate circumstances. These conditions include the presence of a normal cardiovascular state before and after ischemia, the use of oxygen, employment of an efficient respirator, and prolonged mechanical support of respiration postoperatively. The elimination of any one of these factors markedly reduces the period of cardiac arrest to which the brain can be safely subjected.
Recently, hypothermia has been proposed8,10 as adjunctive postoperative treatment for patients who have been resuscitated from cardiac arrest in an effort to forestall the neurologic sequellae which are so often a late cause of death. The efficacy of this therapy has been assumed to be due to a reduction in brain volume at the lowered temperature.8,10 Hypertonic urea has been shown by Javid2,9 to be an effective form of therapy for cerebral edema. Indeed, in the present study, animals treated with this agent did not have autopsy evidence of brain swelling and those not treated had clearly demonstrable evidence of cerebral edema. In spite of this successful treatment of cerebral edema, there was no material reduction in the mortality rate or neurologic disability in the treated animal. From this it is concluded that cerebral edema is an over-emphasized factor in the post-cardiac arrest neurologic syndrome, and that any benefits accruing from the use of hypothermia are due largely to other factors. Strong collateral evidence favoring this conclusion is provided by a recent work of Rosomoff and his co-workers.6 These authors demonstrated that hypothermia, if applied for a brief period within a few hours after acute experimental brain injury, resulted in a striking reduction in mortality. Evidence was presented6 that the efficacy of this treatment was not due to reduction of cerebral edema (and cerebrospinal fluid pressure) since both the treated and untreated animals had comparable cerebral edema.
SUMMARY
The value of hypertonic urea in forestalling the neurologic sequellae after cardiac arrest has been assessed in dogs and monkeys. Simulated cardiac arrest was produced with an inflow-outflow occlusion technique in which the blood supply to the heart was maintained during the period of complete cerebral ischemia.
A number of factors increase the duration of cardiac arrest which can be tolerated without gross neurologic sequellae. These include the presence of an effective circulatory state before and after the arrest, the administration of 100 per cent oxygen before and after the test period, the use of an efficient respirator, and avoidance of premature efforts to promote spontaneous respirations postoperatively.
Under optimum conditions almost all dogs and monkeys will recover completely after 12 minutes of simulated cardiac arrest. With longer occlusions, death and serious neurologic morbidity occur.
Monkeys and dogs were subjected to simulated cardiac arrest for 14 minutes. Hypertonic urea did not materially decrease either the mortality rate or neurologic morbidity in either species, as compared to the recovery rate in controls, despite the fact that the urea-treated animals had demonstrably less brain swelling.
From this it is concluded that cerebral edema is an overemphasized factor in the post-cardiac arrest syndrome, and that the principal deterrent to recovery is anoxic injury to the neurons which is not beneficially influenced by reduction of brain volume.
Acknowledgments
Aided by a grant from the American Heart Association and a grant from the Chicago Heart Association.
Footnotes
The urea used in this study was provided in crystalline form by the Abbott Laboratories, North Chicago, Ill.
References
- 1.Javid M. Urea: New Use of an Old Agent. S Clin North America. 1958;38:907. doi: 10.1016/s0039-6109(16)35526-8. [DOI] [PubMed] [Google Scholar]
- 2.Javid M, Settlage P, Monfore T. Urea in the Management of Increased Intracranial Pressure. S Forum. 1957;7:528. [PubMed] [Google Scholar]
- 3.Küver H, Bucy PC. Preliminary Analysis of Functions of the Temporal Lobes in Monkeys. Arch Neurol & Psychiat. 1939;42:979. doi: 10.1176/jnp.9.4.606. [DOI] [PubMed] [Google Scholar]
- 4.Lewis FJ. An Electronically Controlled Respirator for the Experimental Laboratory. J Thoracic & Cardiovasc Surg. 1959;38:408. [PubMed] [Google Scholar]
- 5.Marshall SB, Owens JC, Swan H. Temporary Circulatory Occlusion to the Brain of the Hypothermic Dog. A M A Arch Surg. 1956;72:98. doi: 10.1001/archsurg.1956.01270190100011. [DOI] [PubMed] [Google Scholar]
- 6.Rosomoff HL, Shulman K, Raynor R, Grainger W. Experimental Brain Injury and Delayed Hypothermia. Surg Gynec & Obst. 1960;110:27. [PubMed] [Google Scholar]
- 7.Stephenson HE. Cardiac Arrest and Resuscitation. St. Louis: The C. V. Mosby Company; 1958. [Google Scholar]
- 8.Williams GR, Spencer FC. The Clinical Use of Hypothermia Following Cardiac Arrest. Ann Surg. 1958;148:462. doi: 10.1097/00000658-195809000-00014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Young WP, Javid MJ. Study of the Use of Intravenous Urea After Simulated Cardiac Arrest in Dogs. S Forum. 1959;10:522. [PubMed] [Google Scholar]
- 10.Zimmerman JM, Spencer F. C: The Influence of Hypothermia on Cerebral Injury Resulting From Circulatory Occlusion. S Forum. 1958;9:216. [PubMed] [Google Scholar]