

Abstract
Objective
To assess the efficacy of moderate aerobic physical activity with sleep hygiene education to improve sleep, mood and quality of life in older adults with chronic insomnia.
Methods
Seventeen sedentary adults aged ≥55 years with insomnia (mean age 61.6 (SD±4.3) years; 16 female) participated in a randomized controlled trial comparing 16 weeks of aerobic physical activity plus sleep hygiene to non-physical activity plus sleep hygiene. Eligibility included primary insomnia for at least 3 months, habitual sleep duration < 6.5 hours and a Pittsburgh Sleep Quality Index (PSQI) score > 5. Outcomes included sleep quality, mood and quality of life questionnaires (PSQI, Epworth Sleepiness Scale [ESS], Short-form 36 [SF-36], Center for Epidemiological Studies Depression Scale [CES-D]).
Results
The physical activity group improved in sleep quality on the global PSQI (p<0.0001), sleep latency (p=0.049), sleep duration (p=0.04), daytime dysfunction (p=0.027), and sleep efficiency (p=0.036) PSQI sub-scores compared to the control group. The physical activity group also had reductions in depressive symptoms (p=0.044), daytime sleepiness (p=0.02) and improvements in vitality (p=0.017) compared to baseline scores.
Conclusion
Aerobic physical activity with sleep hygiene education is an effective treatment approach to improve sleep quality, mood and quality of life in older adults with chronic insomnia.
Keywords: Sleep, physical activity, quality of life, depression, insomnia
Introduction
Chronic sleep disturbance is reported by nearly 50% of the elderly population [1]. Particularly common in this age group is chronic insomnia, characterized by fragmented sleep and early morning awakening [2-4]. Insomnia in older adults is associ ated with mood and anxiety disorders [5-6], falls [7-9] and cognitive impairment [10]. The significant morbidity associated with insomnia coupled with the potential adverse effects of commonly prescribed sedative medications creates the need to develop non-pharmacological treatment approaches for the management of insomnia in older adults.
The sedentary lifestyle of older adults may contribute to the decline in health that often accompanies aging. The maintenance of high physical function is one of the key factors for successful aging [11]. Staying physically and mentally active can not only delay the development of some chronic illnesses and disabilities, but also improve mental and physical health in older adults [12-17].
Recent studies from our group indicate that increased levels of structured social and physical activity have positive effects on sleep and performance in older adults [18-19]. In addition, participation in a regular exercise program can also have positive effects on sleep quality [16, 20-22], mood [16], and cognitive abilities [20-23]. A meta-analysis of 12 studies indicates that regular exercise increases total sleep time and, in some studies, slow wave sleep (SWS) [24]. In addition, epidemiological data based on self-reports consistently support the view that acute and chronic exercise promotes sleep [20]. Furthermore data suggest that higher levels of physical activity in older adults is protective against incident and chronic insomnia [25].
Most studies examining the effects of exercise on sleep have focused on young good sleepers or fit athletes [20, 26]. The limited data available in older adults also indicate an association between physical activity level and sleep quality. For example, older physically fit men had shorter sleep onset latencies, less wake time after sleep onset, higher sleep efficiency and more total slow wave sleep than sedentary older men.[27] There is also evidence that increasing physical activity level can improve sleep quality in older adults [19, 21, 27-30]. For example, in sedentary older adults, a 16 week program of mild to moderate intense physical activity improved self-rated sleep quality [21]. In another study, exposure to daily physical and social activity for just 2 weeks also had positive effects on sleep quality in older adults [19]. Furthermore, in older adults with depression, progressive weight training significantly improved measures of both subjective sleep quality and depression [16].
Taken together, these results indicate a potential for exercise as a means to improve sleep quality and comorbid depressive symptoms in older adults with insomnia. However, the efficacy of exercise to improve sleep quality in older adults with chronic insomnia has not been established. Therefore, the aim of this study was to test the hypothesis that a structured physical exercise program can improve self-reported sleep quality, mood, daytime function and quality of life in late middle age and older adults with chronic insomnia.
Methods
Design
This study used a randomized parallel pre-post design. Participants were randomly assigned to either an aerobic physical activity or non-physical activity intervention group and measurements were collected at baseline and post treatment (16 weeks). Data from this study are part of a larger ongoing study on the effects of exercise as a countermeasure for sleep loss in aging. This report presents only the results of self-reported sleep quality, quality of life, and mood at baseline and post intervention. This study was approved by the Northwestern University Institutional Review Board (IRB). All participants provided written informed consent.
Participants
Participants included 23 healthy community dwelling sedentary men and women who were 55 years or older with symptoms of difficulty falling asleep and/or staying asleep, given the opportunity to sleep, accompanied by impairment in daytime functioning for at least 3 months. In addition, participants were required to be: 1) independent in activities of daily living and without significant cognitive deficits as determined by a MMSE score ≥ 26; 2) a sleep efficiency (SE) less than 80% and/or awakening earlier than desired if before 6 AM; and a total sleep time of less than 6.5 hours, as determined by actigraphy and sleep diary for a period of 7 days; 3) sedentary, defined as participation in exercise of mild to moderate intensity for less than 30 minutes per day and less than two times per week on a regular basis. Exclusionary criteria included the following: 1) other sleep disorders by history or documented on screening polysomnography (apnea index > 10, periodic leg movement arousal index > 15, or REM behavior disorder; 2) history of cognitive or other neurological disorders; 3) history of DSM-IV criteria for any major psychiatric disorder, including mania or alcohol or substance abuse; 4) significant depressive symptoms as assessed by the Center for Epidemiological Studies Depression Scale (CES-D score > 22); 5) unstable or serious medical conditions or cardiopulmonary disease that contraindicate exercise; 6) current use or use within the past month of psychoactive, hypnotic, stimulant or analgesic medications; 7) shift work or other types of self imposed irregular sleep schedules; 8) BMI > 35 Kg/m2; 9) history of habitual smoking (3 or more cigarettes per week); or 10) caffeine consumption greater than 300 mg per day.
Participants were recruited via advertisements in community based publications, flyers and presentations by study staff on sleep and aging given at community centers, assisted living facilities and YMCA’s.
Five participants withdrew or were excluded following randomization. The reason given for withdrawal by the four in the non-physical activity group was that they wanted to be in the exercise condition and the one participant from the activity group was withdrawn due to non-compliance.
Procedure
All eligible participants were screened for other sleep disorders (sleep apnea, PLMS) with overnight polysomnography, depression (CES-D), cognitive function (MMSE), sleep quality (PSQI) and 7 days of activity monitoring using wrist actigraphy and a sleep log. Participants were randomized to aerobic physical activity plus sleep hygiene education or a non-physical activity and sleep hygiene education. At baseline and at the end of the 16-week intervention period, participants were admitted to the Clinical Research Unit (CRU) for a four day baseline admission which involved, questionnaires, nocturnal polysomnography, physiological/hormonal measures, and neuropsychological testing. Cardiopulmonary function testing was conducted during the same visits at the Rehabilitation Institute of Chicago. Baseline exercise testing was performed on all participants to determine exercise capacity and to tailor the exercise intervention to each participant assigned to the physical activity intervention. A symptom-limited maximal ergometer test with a 10 to 40 watt/minute-step protocol was used to measure VO2 max for each subject. The exercise intervention was designed for each participant to reach their anaerobic threshold between 5 and 15 minutes. Anaerobic threshold was determined by measurements of oxygen consumption and end tidal CO2. Continuous EKG recording during cardiopulmonary testing was used to determine maximum heart rate during exercise. Findings for V02 max and maximum heart rate were corroborated by physician review.
Interventions
Sleep hygiene education
All participants received sleep hygiene education which consisted of an appointment with a board certified sleep specialist who provided verbal and written sleep hygiene instructions and counseling according to materials published by the American Academy of Sleep Medicine (including “Behaviors that help promote sound sleep” and “Sleep as we grow older - learning how aging affects sleep”). Patients were given a sleep hygiene checklist and were encouraged by research staff to continue practicing sleep hygiene instructions during bi-weekly visits for the entire duration of the study.
Aerobic physical activity (exercise)
The conditioning period (the first 4-6 weeks) of the exercise intervention was under the supervision of an exercise physiologist. The conditioning protocol included exercise sessions four times per week with the following specifications: Week 1) 10 – 15 minutes per day at 55% max HR as measured with a heart rate monitor (Protrainer, Polar Electro Inc., Port Washington , NY); Week 2) 15 – 20 minutes per day at 60% max HR; Week 3) 20 – 25 minutes per day at 65% max HR; Week 4) 25 – 30 minutes per day at 70% Max HR; Week 5 - 6) attaining 75% of max HR for 30 – 40 minutes.
After completion of the conditioning period, participants exercised for either two 20 minute sessions or one 30 – 40 minute session at 75% of their maximum HR, 4 times per week for the duration of the study. Exercise sessions were conducted in the afternoon or evening (1-7PM). The exercise program included at least two of three aerobic activities (walking, stationary bicycle, or treadmill) with a similar level of exertion for each activity, as measured by the BORG scale of Perceived Exertion and heart rate monitor.
Non-physical activity
Participants in this condition selected recreational or education activities (e.g., parks and recreation, YMCA, museum lectures, church activities) which met for approximately 45 minutes, 3 to 5 times per week, for 16 weeks. Participants were provided with a list of suggested activities to assist with meeting the requirements for the intervention. For example, a participant could attend a cooking class at the YMCA, a lecture at the museum, and a bible study group.
Compliance was defined as a minimum of 3 exercise or non physical activity sessions per week and was monitored using daily exercise and activity (non-physical activity) logs in which information on the type of physical or non-physical activity, duration, time of day, and location of the activity was recorded. In addition, compliance was verified by the research staff during the bi-weekly meetings with the participants.
Measures
Questionnaires were administered at baseline and post-treatment (16 weeks). Sleep quality was measured by The Pittsburgh Sleep Quality Index (PSQI). This 19-item measure assessed sleep quality and disturbances over a 1-month time interval; from these items 7 sub-scores are calculated including sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, sleep medication use, and daytime dysfunction [31]. Daytime sleepiness was measured by The Epworth Sleepiness Scale (ESS). This 8-item measure assesses the likelihood the individual will fall asleep during different situations (e.g., passenger in a car, sitting quietly after lunch).[32] Health related quality of life was measured by the SF-36.[33-34] Depressive symptoms were measured by the CES-D [35]. This 19-item measure assesses depressive symptoms over the past 2 week period. Wrist activity monitoring was conducted for 1 week of screening and 1 week at baseline using the Actiwatch system (Minimittter, Respironics). Sleep parameters calculated by the software analysis program (Actiware v 3.4) included the following: total sleep time, sleep efficiency, sleep latency, wake after sleep onset and fragmentation index.
Analysis
Data were analyzed using SPSS version 16.0 (SPSS Inc., Chicago, IL). Data were analyzed using descriptive statistics, t-tests for independent means, repeated measures ANOVA, and regression. Statistical significance was defined as p<.05 using two tailed tests. Data were analyzed for 17 of 18 participants that completed the study. Data from one participant was removed due to an acute stressful event (de ath in the family) at the end of the study.
Results
Participants
Participant characteristics are described in Table 1. Rest/activity recorded from actigraphy (average of 7 days) and sleep parameters from PSG (night 2) are presented in Table 2. There were no significant differences in any of the sleep parameters between the two groups.
Table 1.
Baseline characteristics of the sample
| Variables | Exercise (N=10) | Non-Physical Activity (N=7) |
|---|---|---|
| Gender | 10 Women, 0 Men | 6 Women, 1 Men |
| Age, y (SD) | 62(4.5) | 63.5(4.3) |
| % white, non-hispanic race | 40% | 57% |
| V02 max | 24.9 (5.4) | 23.9(7.4) |
| Max HR | 159.4(16.3) | 150.2(17.2) |
| BMI | 26.5(4.9) | 26.5(4.6) |
Table 2.
Mean and Standard Deviation (SD) of Baseline Sleep Characteristics from Wrist Actigraphy and Polysomnography
| Actigraphy | Physical Activity | Non-Physical Activity |
|---|---|---|
| M (SD) | M (SD) | |
| Sleep onset latency, min | 21.60 (19.5) | 25.98 (18.17) |
| Assumed sleep, min | 411.60 (41.4) | 439.20 (77.4) |
| Actual sleep, min | 355.80 (37.8) | 376.80 (78.0) |
| Wake after sleep onset, min | 61.20 (24.53) | 59.74 (35.53) |
| Sleep efficiency, % | 79.75 (9.36) | 78.86 (10.14) |
| Fragmentation Index | 34.29 I10.43) | 34.17 (14.88) |
|
Polysomnography |
||
| Sleep onset latency, min | 6.20 (3.95) | 8.71 (9.09) |
| Stage N 1, % | 10.71 (4.83) | 10.29 (4.44) |
| Stage N2,% | 59.33 (8.12) | 55.35 (6.64) |
| Stage N3, % | 10.87 (8.43) | 13.19 (10.18) |
| REM, % | 19.10 (4.02) | 21.17 (2.80) |
| Wake, % | 14.69 (11.39) | 11.30 (9.71) |
| Wake after sleep onset, min | 65.40 (40.81) | 55.21 (38.79) |
| Total sleep time, min | 422.05 (58.88) | 446.86 (51.29) |
| Sleep efficiency, % | 85.87 (8.39) | 86.67 (8.87) |
| Arousal index | 12.95 (5.56) | 13.16 (8.31) |
Note: p>.1 for all comparisons between physical activity groups for all baseline objective sleep characteristics.
Compliance
Physical activity compliance
On average participants exercised 3.27 (±0.52) times a week for an average of 32.3(±12.5) minutes each session. Exercise was mostly completed in a gym or recreation center (76.7%) or at home or work (17.6%); the remainder was outdoors or in public locations (4.3%) or unspecified (1.4%). The majority of exercise sessions included walking or jogging (70.6%) and the remainder included a variety of exercises including, for example, elliptical, Stairmaster, bicycle, swimming, or exercise video.
Structured non-physical activity compliance
On average participants completed 4.2 (±0.73) sessions a week for an average of 139 (±64.4) minutes each session. Participants chose a variety of social, religious, intellectual and cultural activities, including lectures at museums and libraries (31.5%), cultural pursuits at museums and concerts (20.9%), participation in community boards and meetings (15.3%), organized social events such as bingo nights (15.3%), and religious activities (14.7%). Two participants participated in activities with some degree of physical activity during the first week of the study (e.g., ballroom dancing), and these participants were asked to change to another activity for the remainder of the study.
Sleep Quality
Sleep quality was determined using the PSQI. There was a significant effect for time (F (1,15)= 9.96, p=.007), as well as a time by group interaction for global PSQI scores (F (1,15)= 20.49, p<. 001; Figure 1a). The time by condition interaction plus the error for this effect accounted for 57.7% of the variance on change in PSQI scores (partial η2 = .577). In follow-up pre-post comparisons for each group, participants in the exercise group demonstrated significant improvement in global PSQI scores (t(15)= -5.62, p< 0.0001) while participants in the non-physical activity group did not demonstrate improvement. Descriptive statistics, significance values, and effect sizes for the PSQI sub-scores are listed in Table 3. Among the sub-scores, there was a significant effect for time on subjective sleep quality (F(1,15)= 26.09, p< .001), a significant time by condition interaction for sleep onset latency (F(1,15)=5.39, p= .035), a significant time and time by condition interaction for sleep duration (time F(1,15)=4.59 p=.049, time × condition F(1,15)=4.59, p= .049), and for daytime dysfunction (time F (1,15)= 12.32, p= .003, time × condition F(1,15)= 5.98, p= .03). There was also a significant time by condition interaction for sleep latency (F (1,15) = 5.39, p= .04) and sleep efficiency (F (1,15)= p= .036). When sleep time variables were analyzed as continuous variables (rather than sub-scores), there was a significant time effect for sleep duration and a trend toward a time by condition interaction for sleep duration (time F(1,15) = 6.44, p=.02, time by condition F(1,15) = 3.22, p=.09). There was not a significant time or time by condition effect for sleep latency measured as a continuous variable.
Figure 1.
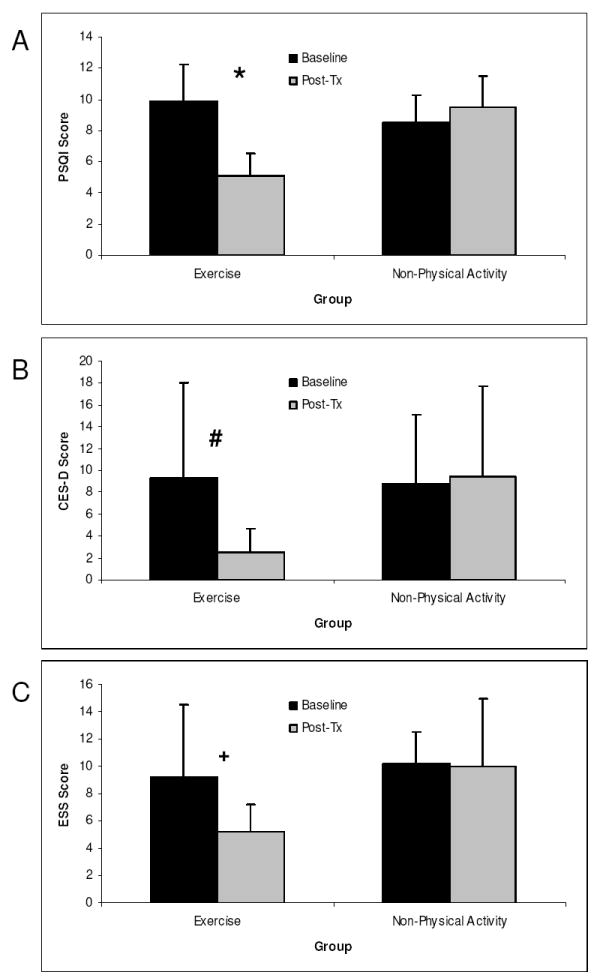
Mean and standard deviation for subjective sleep quality (PSQI), depressive symptom (CES-D) and daytime sleepiness (ESS) for the exercise and Non-Physical Activity groups. Post hoc analysis indicates * p<0.0001, # p=0.044, + p=0.02
Table 3.
Mean (M) and standard deviation (SD) for subjective sleep quality and quality of life variables
| Exercise | Non-Physical Activity | |||||
|---|---|---|---|---|---|---|
| Pre | Post | Pre | Post | Session × Condition | ||
| PSQI Subscores | M (SD) | M (SD) | M (SD) | M (SD) | P value | Partial η2 |
| Subjective Sleep Quality | 1.90 (.57) | .08 (.63) | 1.71 (.49) | 1.14 (.69) | .127 | .15 |
| Sleep Latency | 1.60 (1.27) | 1.00 (.94) | 0.43 (.79) | .86 (.69) | .035 | .26 |
| Sleep Duration | 2.00 (.67) | 1.10 (.74) | 1.86 (.70) | 1.86 (1.09) | .049 | .23 |
| Habitual Sleep Efficiency | 1.20 (1.13) | 0.70(1.0) | 1.57 (.97) | 2.71 (.75) | .036 | .26 |
| Sleep Disturbance | 1.50 (.71) | 1.00 (.00) | 1.43 (.53) | 1.43 (.53) | .144 | .14 |
| Use of Sleeping Medications | .40 (.70) | .00 (.00) | 0.00 (.00) | 0.00 (.00) | .155 | .13 |
| Daytime dysfunction | 1.30 (.48) | .50 (.53) | 1.14 (.39) | 1.00(.58) | .027 | .29 |
| Reported sleep duration (hrs) | 5.60 (.99) | 6.85(.74) | 5.79 (.99) | 6.00 (1.41) | .093 | .18 |
| Reported SOL (mins) | 24.20(18.27) | 19.00(12.87) | 12.14 (9.51) | 17.86(10.31) | .122 | .15 |
| SF-36 | ||||||
| Physical Function | 83.50 (17.49) | 93.00 (5.87) | 64.30 (24.57) | 77.10 (13.18) | .760 | .01 |
| Role Emotional | 76.67 (35.31) | 96.67 (10.54) | 80.95 (37.80) | 61.90 (44.84) | .058 | .22 |
| Bodily Pain | 70.80 (25.55) | 88.80 (7.73) | 64.71 (20.40) | 73.14 (25.39) | .381 | .05 |
| Vitality | 55.00 (21.60) | 80.50 (10.92) | 54.39 (16.94) | 54.27 (11.70) | .017 | .33 |
| General Health | 74.00 (17.92) | 82.50 (13.18) | 75.71 (13.36) | 72.14 (8.59) | .111 | .16 |
| Social Function | 90.00 (23.42) | 98.75 (3.95) | 76.79 (8.63) | 85.71 (15.19) | .987 | < .01 |
| Mental Health | 79.60 (10.41) | 88.00 (7.30) | 84.00 (8.64) | 82.86 (9.72) | .084 | .19 |
| Role Physical | 80.00(36.89) | 92.50 (23.72) | 60.71(37.80) | 67.86(34.50) | .776 | .01 |
Depressive Symptoms
Depressive symptoms were assessed using the CES-D. For the CES-D, there was not a significant time or time by condition effect (Figure 1b). However, pre-post comparisons for each group demonstrated significant improvements in CES-D scores for the exercise group (t (9)= 2.34, p=.04) but not for the non-physical activity group.
Quality of life
The SF-36 was used to assess quality of life. The physical activity intervention was associated with improvements or trends toward improvement among several domains of quality of life (see Table 3). There was an effect for time on vitality (F(1,15), 7.207, p= .02) and a trend toward improvement over time in physical function (F (1,15)= 4.309, p=.056). There was a significant time by condition effect for vitality (F (1,15)= 7.207, p= .017) and a trend for time by condition effects in role emotional (F (1,15)= 4.214, p= .058) and mental health (F (1,15) 3.44, p = .08). There were no significant time or time by condition effects for role physical, general health, or social functioning.
Daytime Sleepiness
Daytime sleepiness was evaluated using the ESS. For ESS there was a trend of an effect for time (F (1, 15)= 3.18, p= .09), but there was not a time by condition interaction (F (1, 15)= 2.8, p= .12). In follow-up pre-post comparisons for each group, there was a significant reduction in the ESS score for the exercise group (t(9)= -2.75, p=0.02) but not in the non-physical activity group (Figure 1c).
Fitness Level
There was a trend toward an effect for time on maximum heart rate (F (1,15)= 3.51, p= .08) but no time by condition effect. There were no effects of time or time by condition on V02max or maximum heart rate. Pre-post comparisons for each group demonstrated a trend toward improvements in V02max for the exercise group (t(9) -1.93, p= .08) but not for the non-physical activity group. Neither group demonstrated significant pre-post changes in maximum heart rate.
Relationship between improvements in sleep, sleepiness, mood and fitness
Reductions in global PSQI scores were not associated with greater improvements in maximum heart rate or VO2max. However, when the physical activity group was analyzed alone, there was a trend for a correlation between change in maximum HR and PSQI scores (r=0.671, p=0.058). A reduction in global PSQI scores was also associated with a greater reduction in depressive symptoms on the CES-D (r=0.487, p=0.048). The change in global PSQI was not related to change in daytime sleepiness measured by the ESS.
In exploratory analyses, we constructed a mediational model to test if exercise was associated with a change in PSQI scores above and beyond the change in depressive symptoms. After controlling for depression, there continued to be a significant relationship between physical activity group and change in PSQI scores (B= 5.003, p=0.002).
Discussion
Results from this study indicate that a sixteen week program of moderate intensity aerobic physical activity plus sleep hygiene education is effective in improving self reported sleep quality, mood and quality of life in older adults with chronic insomnia. These results highlight the potential of structured physical activity programs to improve the effectiveness of standard behavioral approaches for the treatment of insomnia, particularly in a sedentary older adult population.
The effect size for the improvements in sleep duration and subjective sleep quality in this study were similar or even greater than that reported for cognitive behavioral intervention and other physical activity studies [18, 30, 36-38]. Improvements were seen in global PSQI score and sleep duration, with most of the exercise group having a score of 5 or below following treatment, indicating good overall sleep quality. Compared to a 25 week Tai Chi study that reported a significant decrease in PSQI score of 1.8 points [39], the current study achieved an average 4.8 point reduction in PSQI score. In a previous study, our group, reported a 1.1 drop in PSQI score for morning and a 1.5 drop for evening structured activity following two weeks of intervention [18]. The larger effect seen in our study may be due to differences in the duration and intensity of the physical activity level and the characteristics of the participants.
The increase in self reported sleep duration by 1.25 hours in the exercise plus sleep hygiene education group is higher than what has been reported for other non-pharmacological interventions for insomnia [30, 40] This large increase in sleep duration may be in part due to the inclusion criteria of having a habitual sleep duration of less than 6.5 hours a night, which was verified with wrist actigraphy and sleep log. In addition, the elevated baseline WASO as measured by actigraphy and PSG indicate that this group of patients had sleep maintenance insomnia type. Thus, improved sleep continuity may also have contributed to the self reported increase in sleep duration.
There was also a significant reduction in the sleep latency sub-score of the PSQI but not in sleep latency measured as a continuous variable. This apparent difference could be because the PSQI sleep latency sub-score reflects both sleep latency and the frequency of being unable to fall asleep within 30 minutes [31]. Therefore, while there may not have been a reduction in the actual time to fall asleep, there was likely a decrease in the number of times per week in which the participants experienced the problem.
It has been suggested that physical activity may improve sleep via improvements in depressive symptoms in those with depression [41]. Consistent with this hypothesis, in our study, there was a significant association between improvements in depressive symptoms and improvements in subjective sleep quality in the whole group. However, the improvements in subjective sleep quality (PSQI score) associated with exercise remained after adjusting for depressive symptoms (CES-D score), indicating that the positive effect of exercise on sleep quality is also independent of depressive symptoms.
At baseline, SF-36 scores in this study were similar to those previously reported for people with mild-severe insomnia [42-44]. One of the largest improvements following exercise intervention was observed in vitality, a high vitality score means that in the past 4 weeks the person feels full of “pep” and energy all the time [33]. For the exercise group the vitality measure from the SF-36 improved substantially by 25.5 points following intervention compared to a 0.12 reduction for the non-physical activity group. In comparison with pharmacological therapies, in a study of the hypnotic eszopiclone over a 1-6 month period there was a 15 point increase in vitality [45]. Furthermore, the degree of change in vitality in the current study was greater than the differences seen between people with insomnia and controls (16 points) or patients with depression and controls (13 points) [44].
There was a positive relationship between improvements in sleep quality and improvements in fitness level as determined by maximum heart rate in the exercise group, although this was only a trend (p=0.058). However, a similar correlation between sleep quality and V02 max was not seen. This may in part be due to the limited ability of older adults to readily augment O2 uptake in response to exercise [46-47]. These results suggest that the effect of exercise on sleep quality, mood and sleepiness may be mediated via mechanism other than only cardiopulmonary fitness.
There are several potential limitations in this study, including the reliance on self- reported sleep quality measures, the relatively small number of participants and the female preponderance of the sample. The baseline PSG parameters demonstrate relatively short sleep latencies and preserved slow wave sleep which may be in part due to the female preponderance of the sample and/ or the paradoxical effect of sleeping in the laboratory in patients with psychophysiological insomnia. Although the gender imbalance may affect the generalizability of the study, our findings remain relevant to patients with insomnia because insomnia is more prevalent among women than men [48]. Another limitation was the higher dropout rate in the non-physical activity group. This may have been due in part to the desire of some participants to be randomized to the exercise condition. The internal validity of the study may be affected if those with low expectations for the non-physical activity intervention selectively dropped out after randomization.
However, these results are of clinical importance because self-reported measures of overall sleep quality, sleep latency, sleep duration, alertness and quality of life are the most widely used measure of insomnia treatment effectiveness in clinical practice. Therefore, the demonstration of the feasibility and ability of a program of exercise and sleep hygiene education to improve sleep quality in older adults with insomnia, together with the other known positive effects of physical activity on cardiopulmonary, metabolic and cognitive health, underscores the importance of incorporating structured physical activity in any comprehensive program for the management of insomnia in older adults.
Acknowledgments
The authors would like to thank all of the study participants for their participation and Rosemary Ortiz for assistance with data collection. This research was supported by a National Institute of Aging grant P01 AG11412, General Clinical Research Center grant M01 RR00048, K23 HL091508, T32AG020506.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- 1.Foley DJ, Monjan AA, Brown SL, Simonsick EM, Wallace RB, Blazer DG. Sleep complaints among elderly persons: an epidemiologic study of three communities. Sleep. 1995;18(6):425–32. doi: 10.1093/sleep/18.6.425. [DOI] [PubMed] [Google Scholar]
- 2.Middelkoop HA, Smilde-van den Doel DA, Neven AK, Kamphuisen HA, Springer CP. Subjective sleep characteristics of 1,485 males and females aged 50-93: effects of sex and age, and factors related to self-evaluated quality of sleep. J Gerontol A Biol Sci Med Sci. 1996;51(3):M108–15. doi: 10.1093/gerona/51a.3.m108. [DOI] [PubMed] [Google Scholar]
- 3.Gislason T, Reynisdottir H, Kristbjarnarson H, Benediktsdottir B. Sleep habits and sleep disturbances among the elderly--an epidemiological survey. J Intern Med. 1993;234(1):31–9. doi: 10.1111/j.1365-2796.1993.tb00701.x. [DOI] [PubMed] [Google Scholar]
- 4.Webb WB, Campbell SS. Awakenings and the return to sleep in an older population. Sleep. 1980;3(1):41–6. [PubMed] [Google Scholar]
- 5.Stewart R, Besset A, Bebbington P, Brugha T, Lindesay J, Jenkins R, et al. Insomnia comorbidity and impact and hypnotic use by age group in a national survey population aged 16 to 74 years. Sleep. 2006;29(11):1391–7. doi: 10.1093/sleep/29.11.1391. [DOI] [PubMed] [Google Scholar]
- 6.Ancoli-Israel S. Insomnia in the elderly: a review for the primary care practitioner. Sleep. 2000;23(Suppl 1):S23–30. discussion S6-8. [PubMed] [Google Scholar]
- 7.Stone KL, Ewing SK, Lui LY, Ensrud KE, Ancoli-Israel S, Bauer DC, et al. Self-reported sleep and nap habits and risk of falls and fractures in older women: the study of osteoporotic fractures. J Am Geriatr Soc. 2006;54(8):1177–83. doi: 10.1111/j.1532-5415.2006.00818.x. [DOI] [PubMed] [Google Scholar]
- 8.Avidan AY, Fries BE, James ML, Szafara KL, Wright GT, Chervin RD. Insomnia and hypnotic use, recorded in the minimum data set, as predictors of falls and hip fractures in Michigan nursing homes. J Am Geriatr Soc. 2005;53(6):955–62. doi: 10.1111/j.1532-5415.2005.53304.x. [DOI] [PubMed] [Google Scholar]
- 9.Brassington GS, King AC, Bliwise DL. Sleep problems as a risk factor for falls in a sample of community-dwelling adults aged 64-99 years. J Am Geriatr Soc. 2000;48(10):1234–40. doi: 10.1111/j.1532-5415.2000.tb02596.x. [DOI] [PubMed] [Google Scholar]
- 10.Cricco M, Simonsick EM, Foley DJ. The impact of insomnia on cognitive functioning in older adults. J Am Geriatr Soc. 2001;49(9):1185–9. doi: 10.1046/j.1532-5415.2001.49235.x. [DOI] [PubMed] [Google Scholar]
- 11.Rowe JW, Kahn RL. Successful aging. Gerontologist. 1997;37(4):433–40. doi: 10.1093/geront/37.4.433. [DOI] [PubMed] [Google Scholar]
- 12.Clarkson-Smith L, Hartley AA. Relationships between physical exercise and cognitive abilities in older adults. Psychol Aging. 1989;4(2):183–9. doi: 10.1037//0882-7974.4.2.183. [DOI] [PubMed] [Google Scholar]
- 13.Department of Health and Human Services US. Exercise: A guide from the National Institute on Aging2001. Report No.: NIH Publication No 01-4258. [Google Scholar]
- 14.Dustman RE, Ruhling RO, Russell EM, Shearer DE, Bonekat HW, Shigeoka JW, et al. Aerobic exercise training and improved neuropsychological function of older individuals. Neurobiol Aging. 1984;5(1):35–42. doi: 10.1016/0197-4580(84)90083-6. [DOI] [PubMed] [Google Scholar]
- 15.Kramer AF, Hahn S, Cohen NJ, Banich MT, McAuley E, Harrison CR, et al. Ageing, fitness and neurocognitive function. Nature. 1999;400(6743):418–9. doi: 10.1038/22682. [DOI] [PubMed] [Google Scholar]
- 16.Singh NA, Clements KM, Fiatarone MA. A randomized controlled trial of the effect of exercise on sleep. Sleep. 1997;20(2):95–101. doi: 10.1093/sleep/20.2.95. [DOI] [PubMed] [Google Scholar]
- 17.Stevenson JS, Topp R. Effects of moderate and low intensity long-term exercise by older adults. Res Nurs Health. 1990;13(4):209–18. doi: 10.1002/nur.4770130403. [DOI] [PubMed] [Google Scholar]
- 18.Benloucif S, Orbeta L, Ortiz R, Janssen I, Finkel SI, Bleiberg J, et al. Morning or evening activity improves neuropsychological performance and subjective sleep quality in older adults. Sleep. 2004;27(8):1542–51. doi: 10.1093/sleep/27.8.1542. [DOI] [PubMed] [Google Scholar]
- 19.Naylor E, Penev PD, Orbeta L, Janssen I, Ortiz R, Colecchia EF, et al. Daily social and physical activity increases slow-wave sleep and daytime neuropsychological performance in the elderly. Sleep. 2000;23(1):87–95. [PubMed] [Google Scholar]
- 20.Driver HS, Taylor SR. Exercise and sleep. Sleep Med Rev. 2000;4(4):387–402. doi: 10.1053/smrv.2000.0110. [DOI] [PubMed] [Google Scholar]
- 21.King AC, Oman RF, Brassington GS, Bliwise DL, Haskell WL. Moderate-intensity exercise and self-rated quality of sleep in older adults. A randomized controlled trial. Jama. 1997;277(1):32–7. [PubMed] [Google Scholar]
- 22.Trinder J, Paxton SJ, Montgomery I, Fraser G. Endurance as opposed to power training: their effect on sleep. Psychophysiology. 1985;22(6):668–73. doi: 10.1111/j.1469-8986.1985.tb01665.x. [DOI] [PubMed] [Google Scholar]
- 23.O’Connor PJ, Crowley MA, Gardner AW, Skinner JS. Influence of training on sleeping heart rate following daytime exercise. Eur J Appl Physiol Occup Physiol. 1993;67(1):39–42. doi: 10.1007/BF00377702. [DOI] [PubMed] [Google Scholar]
- 24.Kubitz KA, Landers DM, Petruzzello SJ, Han M. The effects of acute and chronic exercise on sleep. A meta-analytic review. Sports Med. 1996;21(4):277–91. doi: 10.2165/00007256-199621040-00004. [DOI] [PubMed] [Google Scholar]
- 25.Morgan K. Daytime activity and risk factors for late-life insomnia. J Sleep Res. 2003;12(3):231–8. doi: 10.1046/j.1365-2869.2003.00355.x. [DOI] [PubMed] [Google Scholar]
- 26.Youngstedt SD. Effects of exercise on sleep. Clin Sports Med. 2005;24(2):355–65. xi. doi: 10.1016/j.csm.2004.12.003. [DOI] [PubMed] [Google Scholar]
- 27.Edinger JD, Morey MC, Sullivan RJ, Higginbotham MB, Marsh GR, Dailey DS, et al. Aerobic fitness, acute exercise and sleep in older men. Sleep. 1993;16(4):351–9. doi: 10.1093/sleep/16.4.351. [DOI] [PubMed] [Google Scholar]
- 28.Bliwise DL, King AC, Harris RB, Haskell WL. Prevalence of self-reported poor sleep in a healthy population aged 50-65. Soc Sci Med. 1992;34(1):49–55. doi: 10.1016/0277-9536(92)90066-y. [DOI] [PubMed] [Google Scholar]
- 29.Van Someren EJ, Lijzenga C, Mirmiran M, Swaab DF. Long-term fitness training improves the circadian rest-activity rhythm in healthy elderly males. J Biol Rhythms. 1997;12(2):146–56. doi: 10.1177/074873049701200206. [DOI] [PubMed] [Google Scholar]
- 30.King AC, Pruitt LA, Woo S, Castro CM, Ahn DK, Vitiello MV, et al. Effects of moderate-intensity exercise on polysomnographic and subjective sleep quality in older adults with mild to moderate sleep complaints. J Gerontol A Biol Sci Med Sci. 2008;63(9):997–1004. doi: 10.1093/gerona/63.9.997. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Buysse DJ, Reynolds CF, 3rd, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28(2):193–213. doi: 10.1016/0165-1781(89)90047-4. [DOI] [PubMed] [Google Scholar]
- 32.Johns MW. A new method for measuring daytime sleepiness: the Epworth sleepiness scale. Sleep. 1991;14(6):540–5. doi: 10.1093/sleep/14.6.540. [DOI] [PubMed] [Google Scholar]
- 33.Ware JE, Sherbourne CD. The MOS 36-item short-form health survey (SF-36): I. Conceptual framework and item selection. Medical Care. 1992;30:473–83. [PubMed] [Google Scholar]
- 34.McHorney CA, Ware JE, Jr, Raczek AE. The MOS 36-Item Short-Form Health Survey (SF-36): II Psychometric and clinical tests of validity in measuring physical and mental health constructs. Med Care. 1993;31(3):247–63. doi: 10.1097/00005650-199303000-00006. [DOI] [PubMed] [Google Scholar]
- 35.Radloff LS. The CES-D Scale: A self-report depression scale for research in the general population. Applied Psychological Measurement. 1977;3:385–401. [Google Scholar]
- 36.Currie SR, Wilson KG, Curran D. Clinical significance and predictors of treatment response to cognitive-behavior therapy for insomnia secondary to chronic pain. J Behav Med. 2002;25(2):135–53. doi: 10.1023/a:1014832720903. [DOI] [PubMed] [Google Scholar]
- 37.Morgan K, Dixon S, Mathers N, Thompson J, Tomeny M. Psychological treatment for insomnia in the regulation of long-term hypnotic drug use. Health Technol Assess. 2004;8(8):iii–iv. 1–68. doi: 10.3310/hta8080. [DOI] [PubMed] [Google Scholar]
- 38.Irwin MR, Cole JC, Nicassio PM. Comparative meta-analysis of behavioral interventions for insomnia and their efficacy in middle-aged adults and in older adults 55+ years of age. Health Psychol. 2006;25(1):3–14. doi: 10.1037/0278-6133.25.1.3. [DOI] [PubMed] [Google Scholar]
- 39.Irwin MR, Olmstead R, Motivala SJ. Improving sleep quality in older adults with moderate sleep complaints: A randomized controlled trial of Tai Chi Chih. Sleep. 2008;31(7):1001–8. [PMC free article] [PubMed] [Google Scholar]
- 40.Morin CM, Hauri PJ, Espie CA, Spielman AJ, Buysse DJ, Bootzin RR. Nonpharmacologic treatment of chronic insomnia. An American Academy of Sleep Medicine review. Sleep. 1999;22(8):1134–56. doi: 10.1093/sleep/22.8.1134. [DOI] [PubMed] [Google Scholar]
- 41.Montgomery P, Dennis J. Physical exercise for sleep problems in adults aged 60+ Cochrane Database Syst Rev. 2002;(4):CD003404. doi: 10.1002/14651858.CD003404. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Zammit GK, Weiner J, Damato N, Sillup GP, McMillan CA. Quality of life in people with insomnia. Sleep. 1999;22(Suppl 2):S379–85. [PubMed] [Google Scholar]
- 43.Leger D, Scheuermaier K, Philip P, Paillard M, Guilleminault C. SF-36: evaluation of quality of life in severe and mild insomniacs compared with good sleepers. Psychosom Med. 2001;63(1):49–55. doi: 10.1097/00006842-200101000-00006. [DOI] [PubMed] [Google Scholar]
- 44.Katz DA, McHorney CA. The relationship between insomnia and health-related quality of life in patients with chronic illness. J Fam Pract. 2002;51(3):229–35. [PubMed] [Google Scholar]
- 45.Walsh JK, Krystal AD, Amato DA, Rubens R, Caron J, Wessel TC, et al. Nightly treatment of primary insomnia with eszopiclone for six months: effect on sleep, quality of life, and work limitations. Sleep. 2007;30(8):959–68. doi: 10.1093/sleep/30.8.959. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Ogawa T, Spina RJ, Martin WH, 3rd, Kohrt WM, Schechtman KB, Holloszy JO, et al. Effects of aging, sex, and physical training on cardiovascular responses to exercise. Circulation. 1992;86(2):494–503. doi: 10.1161/01.cir.86.2.494. [DOI] [PubMed] [Google Scholar]
- 47.DeLorey DS, Kowalchuk JM, Paterson DH. Effects of prior heavy-intensity exercise on pulmonary O2 uptake and muscle deoxygenation kinetics in young and older adult humans. J Appl Physiol. 2004;97(3):998–1005. doi: 10.1152/japplphysiol.01280.2003. [DOI] [PubMed] [Google Scholar]
- 48.Ohayon MM. Epidemiology of insomnia: what we know and what we still need to learn. Sleep Med Rev. 2002;6(2):97–111. doi: 10.1053/smrv.2002.0186. [DOI] [PubMed] [Google Scholar]