

Abstract
Children’s self-efficacy for fruit and vegetable consumption (FVC) and proxy efficacy to influence others to make fruit and vegetables (FV) available may influence their FVC. A previous investigation has demonstrated that self-efficacy for fruit consumption, self-efficacy for vegetable consumption, proxy efficacy to influence parents to make FV available, and proxy efficacy to influence after-school staff to make FV available can be measured with four independent but related scales. The purpose of the present investigation is to confirm this factor structure and determine if the scales were invariant across gender, ethnicity, and socioeconomic status (SES) subgroups of children attending after-school programs. Results provide further validity evidence for the four correlated scales. In addition, results confirm measurement invariance across gender, SES, and ethnicity, confirming the unbiased generalizability of the current measure to these demographic groups. Lastly, tests of population heterogeneity reveal no meaningful differences in self- and proxy efficacy among gender, SES, and ethnicity subgroups.
Keywords: fruit and vegetable consumption, self-efficacy, invariance
Social cognitive theory (SCT) is a predominant model to understand and positively affect health behaviors, such as fruit and vegetable consumption (FVC). Self-efficacy, a central influence on FVC according to the SCT, was defined as a child’s belief that he or she can execute a behavior at a necessary level in order to obtain a desired outcome (Bandura, 1986). Previous research has demonstrated a positive association between self-efficacy and FVC among elementary school–aged youth (Domel et al., 1996; Kratt, Reynolds, & Shewchuk, 2000; Perez-Lizaur, Kaufer-Horwitz, & Plazas, 2008; Reynolds et al., 1999; Reynolds, Yaroch, Franklin, & Maloy, 2002; Sharma, Wagner, & Wilkerson, 2005) and middle school–aged youth (Cullen, Bartholomew, Parcel, & Koehly, 1998).
According to the SCT, children have two ways of exerting control to reach a desired outcome: direct personal agency and proxy agency (Bandura, 2001). Measurement of children’s self-efficacy, or their personal estimate regarding their confidence to consume fruit and vegetables (FV), is primarily a reflection of beliefs about direct personal agency, but children’s self-efficacy judgments also tap beliefs about proxy agency. Proxy agency can also be assessed directly by obtaining children’s estimates of their belief that they can get others to act on their behalf to reach desired outcomes. To better distinguish between beliefs about these two forms of agency, researchers and practitioners may need to assess both self-efficacy beliefs and beliefs about proxy agency using scales that assess proxy efficacy judgments.
Previous FV research has reported some inconsistency in distinguishing between self-efficacy and proxy efficacy in measurement (Geller, Dzewaltowski, Rosenkranz, & Karteroliotis, 2009; Reynolds et al., 2002). In a research study measuring FV self-efficacy in elementary school–aged children, Reynolds and colleagues (2002) performed analyses and demonstrated that self-efficacy was best assessed as a single construct, with self- and proxy efficacy items loading on one factor.
However, a more recent exploratory factor analysis (EFA) illuminated that self- and proxy efficacy scales can assess independent but related constructs. This previous investigation identified four underlying self-efficacy FV factors: self-efficacy for fruit consumption, self-efficacy for vegetable consumption, proxy efficacy to influence parents to make FV available, and proxy efficacy to influence after-school staff to make FV available (Geller et al., 2009). Perhaps Geller and colleagues found different results than Reynolds because their scale was based on items generated specifically to assess direct personal agency and proxy agency independently. Thus, the initial objective of the current research is to further investigate if self- and proxy efficacy are multidimensional and best assessed through independent but related scales.
In addition to examining the theoretical framework of self- and proxy efficacy, a second objective was to determine the consistency of these scales across different subgroups of children. For example, Dishman and colleagues (2002) tested a measure of self-efficacy for physical activity, determining invariance across Caucasian and African American adolescent girls. Specifically, four questionnaires assessing determinants of physical activity had equivalent factor structure, factor loadings, and factor variance. Similarly, a measure of motivation for sport that included self-efficacy as an underlying construct demonstrated equal factor structure and factor covariance across gender and grade level among 12 to 18 year olds (Martin, 2008). Although there is some work for physical activity, there is no research examining the consistency of self- and proxy efficacy for FV scales across different groups that vary on gender, race/ethnicity, and socioeconomic status (SES).
The consequences of a measurement instrument that does not generalize to all demographic groups of a target population are problematic. For instance, when a measure is valid and accurate for one group but less valid for another, findings may demonstrate demographic differences where none exist. For example, Granner and colleagues (2004) reported no ethnic or gender differences in self-efficacy among 11- to 15-year-old children; however, research has demonstrated lower dietary self-efficacy among lower SES youth (6 to 18 years old; O’Dea & Wilson, 2006). Furthermore, Geller and colleagues (2009) reported higher proxy efficacy for FV from parents among children attending higher SES and less ethnically diverse schools compared to children attending lower SES and more ethnically diverse schools. But since the measurement invariance across subgroups on the scales used in these studies had not been determined, it is unclear if these are true mean differences between these subgroups or a consequence of shifts in measurement validity.
In summary, the current study had two primary aims: first, to confirm that self-efficacy is multidimensional, containing both direct and proxy constructs that can be assessed with independent but related scales, and second, to determine if the factor structure of self- and proxy efficacy scales were similar across subgroups from the same population of elementary school–aged children (gender, SES, and ethnicity), and to identify any subgroup mean differences.
Overall, we hypothesized that a multidimensional scale, containing self- and proxy efficacy items would be confirmed (Geller et al., 2009). Specifically, the self-efficacy scale would distinguish between self-efficacy for fruit consumption, self-efficacy for vegetable consumption, proxy efficacy for FV from parents, and proxy efficacy for FV from after-school staff. Furthermore, measurement invariance was expected across gender, SES, and ethnicity groups, supporting the unbiased generalizability of the current measure to different subgroups of elementary school–aged children.
Mean differences were not expected between gender, ethnicity, and SES subgroups for fruit self-efficacy, vegetable self-efficacy, and proxy efficacy from after-school staff because of previous reports of similar means among these subgroups on these constructs (Geller et al., 2009; Granner et al., 2004). However, proxy efficacy for FV from parents was expected to be higher among children categorized as higher SES and less ethnically diverse compared to their counterparts, paralleling previous research (Geller et al., 2009).
METHOD AND PROCEDURE
The current analyses drew data from the Healthy Opportunities for Physical Activity and Nutrition (HOP’N) project, a school-randomized controlled trial targeting the prevention of obesity. Prior to randomization, seven participating after-school sites located in Lawrence, Kansas, were categorized into two groups based on the concentration of both SES (based on free or reduced-price lunch status) and racial/ethnic diversity. The SES and race/ethnicity classifications were clustered; thus, four sites were categorized as lower SES, higher diversity, and the other three as higher SES, lower diversity. Data for the current analysis were drawn from both lower SES, higher diversity sites (69%) and higher SES, lower diversity sites (31%).
During after-school time, children were led through a paper-and-pencil survey in small groups assessing psychosocial variables related to physical activity and nutrition. Research assistants followed a verbatim script and read each question aloud to the participating children. Example questions with directions were displayed on a poster board and realistic FV food models were used to clarify serving sizes. The institutional review board at a U.S. midwestern university approved all procedures.
Measures
Four groups of items were developed based on SCT and previous FV literature (Reinaerts, Nooijer, Candel, & Vries, 2006; Vereecken, Van Damme, & Maes, 2005). The self-efficacy construct was assessed with three items representing self-efficacy for fruit consumption (SEFC) and three items representing self-efficacy for vegetable consumption (SEVC). Proxy efficacy from parents (PEFV-P) and proxy efficacy from after-school staff (PEFV-S) were each captured with four items. The separation of these four factors was suggested in a previous EFA study, which reported high internal consistency (α = .81, with subscale αs ranging from .75 to .84) and provided detailed information on each of the included items (Geller et al., 2009).
SEFC
The SEFC items were generated to correspond to the recommendation of one to three servings of fruit or 100% fruit juice each day (U.S. Department of Agriculture [USDA], 2005). Serving sizes were established from the food guide pyramid; therefore, one serving of fruit and one serving of fruit juice was defined to the children as “1 medium piece of fresh fruit, ½ cup of fruit salad, ¼ cup of raisins, apricots or other dried fruit, 6 oz. of 100% orange, apple or grape juice (Do not count fruit punch, lemonade, Gatorade, Sunny Delight or fruit drink).” Each question began with “How sure are you that you can eat … ,” assessing in three separate questions confidence to eat one, two, and three servings of fruit each day. Children responded using a 3-point scale, not sure at all, somewhat sure, and very sure.
SEVC
Similar to SEFC, SEVC items were generated based on the food guide pyramid (one to three servings each day; USDA, 2005). One serving of a vegetable was defined for the children as “1 medium carrot or other fresh vegetable, 1 small bowl of green salad, ½ cup of fresh or cooked vegetables, ¾ cup of vegetable soup (Do not count french fries, onion rings, potato chips or fried okra).” These questions were grouped with fruit consumption items and began with “How sure are you that you can eat ….” Three separate questions were included assessing children’s perceived ability to consume one, two, and three servings of vegetables. Children responded using the same 3-point scale: not sure at all, somewhat sure, and very sure.
PEFV-P
This measure was defined as children’s confidence in their skills and abilities to get their parent to make FV available. Specifically, PEFV-P accessed children’s confidence in having a parent or guardian provide FV opportunities for them. Each question began with “How sure are you that you can get your parents to … ,” with example questions including “buy fruit for a snack” and “fix your favorite vegetable dish.” Children responded to each item on a 3-point scale, not sure at all, somewhat sure, and very sure.
PEFV-S
This measure was defined as children’s confidence in their skills and abilities to get the after-school program staff members to make FV available. Each question began with “How sure are you that you can get the teachers or staff members of the after-school program to … ,” with example questions including “offer fruit and vegetable snack options” and “offer 100% real fruit juice.” Again, children responded to each item using a 3-point scale, not sure at all, somewhat sure, and very sure.
Statistical Analyses
Factorial structure of the current measure was evaluated with several confirmatory factor analyses (CFAs) using Mplus 4.2 (Muthen & Muthen, 2007) and a weighted least square with mean and variance correction (WLSMV) estimator function for categorical data. In addition to the overall fit of the hypothesized model, several nested model comparisons were made. Because of categorical data and WLSMV estimation, the χ2 difference test had to be calculated from the derivatives of each model (Brown, 2006). First, the baseline model was fitted to the data and the model derivatives saved for the nested χ2 test. Next, the more constrained model was fit to the data and the χ2 difference test calculated using the derivatives from both analyses.
Multigroup CFAs were conducted to analyze the across-group equivalence (measurement invariance) as well as the group concordance of structural parameters (population heterogeneity) for gender and SES subgroups. First, the baseline model was tested separately for each subgroup with no invariance constraints. Next, the χ2 difference test calculated from model derivatives was used to access possible degrade at each level of model constrain. If a new set of parameters was found to be noninvariant across subgroups, the constraint was lifted and the nonequivalent parameters were located in the model. If parameters were invariant, parameter equality constraints were cumulatively held in place and invariance tests continued.
Because of an inadequate sample of African American children (n = 50) for multigroup comparisons, a multiple-indicators, multiple-causes model (MIMC) was used to test invariance across Caucasian and African American subgroups. MIMC modeling began by confirming a sound CFA measurement model using a collapsed data set with both racial/ethnic subgroups. Next, the indicators and latent factors were regressed onto the ethnicity covariate (i.e., 0 = African American, 1 = Caucasian). By examining the direct effect of the race/ethnicity covariate on both the indicator variables and the latent variables, indicator thresholds and factor means were tested for invariance, respectively.
Beyond χ2, additional fit indices were used to determine adequacy of each model fit. The comparative fit index (CFI) was adequate at values above .90 (Bentler, 1990) and the Tucker–Lewis index (TLI; Bentler & Bonett, 1980) at values greater than or equal to .95 (Hu & Bentler, 1999). In addition, a root mean square error of approximation (RMSEA) value less than .05 was indicative of a close fit, less than .08 was considered reasonable, and between .08 and 1.00 was mediocre (Browne & Cudeck, 1993). Finally, the presence of localized areas of model strain was determined from standardized residuals greater than 2.00 and modification index (MI) values greater than 4.00.
RESULTS
Participants and Descriptive Statistics
Participants were elementary school–aged children attending seven after-school programs on elementary school sites. Of the 246 youth, 232 (94%) had complete self- and proxy efficacy scores. The children were among an after-school group primarily composed of fourth-graders but contained other grades of similar age (9% fifth grade and 3% sixth grade). The mean age of the 232 students during the time of questionnaire completion was 9.68 years, ranging from 8.00 to 12.55 years. Fifty-one percent were male, 39.2% were racially/ethnically diverse (African American, n = 50; Native American/Alaska Native, n = 19; Hispanic/Latino, n = 16; Asian, n = 3; other, n = 3), and 52.6% were considered lower SES (eligible for free or reduced-price lunch). Because χ2 is sensitive to sample size, random samples of males and lower SES children were taken to maintain an equal number of subgroup participants for the multigroup CFAs. Specifically, 94% of the male sample was randomly selected to equal the female sample (n = 119), and 90% of the lower SES sample was randomly selected to equal the higher SES sample (n = 110). In consideration of cultural differences and low sample sizes, analyses examining racial/ethnic differences only included Caucasian (n = 141) and African American children (n = 50).
Overall Model Fit
Figure 1 depicts the complete specification of the baseline model along with the means and standard deviations for the entire sample (N = 232) on each of the four latent constructs. The first indicator of each latent construct was used as a marker indicator for its corresponding latent construct. The measurement model contained no double loading indicators and all measurement error was presumed to be uncorrelated. Accordingly, the model was overidentified with 33 df.
Figure 1.
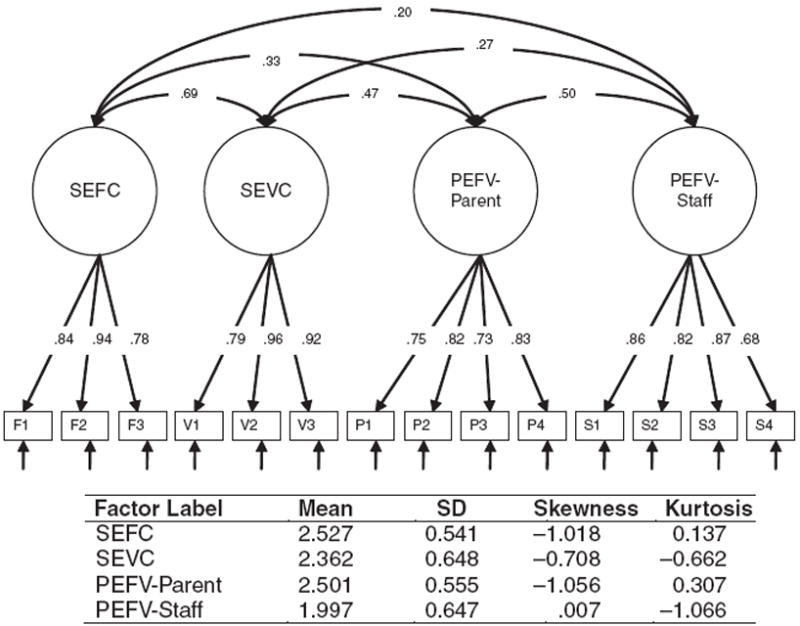
Path diagram of model, including standardized factor scores and correlations. NOTE: The table includes mean, standard deviation, skewness, and kurtosis statistics for self-efficacy for fruit (SEFC), self-efficacy for vegetables (SEVC), proxy efficacy from parent (PEFV-P) and proxy efficacy from after-school staff (PEFV-S). All indicators measured on scales ranging from 1 to 3 (higher scores reflect higher levels of the assessed latent construct); N = 232.
The baseline model fit well, χ2(33) = 62.025, p = .002, CFI = .979, TLI = .986, and RMSEA = .062. All freely estimated unstandardized parameters were statistically significant (ps < .001). Inspection of residual variances and modification indices indicated no ill fits within the solution, and factor loading estimates were strongly related to their supposed latent factors (R2s = .456-.918). Finally, the four latent constructs were moderately correlated (ranging from .145 to .458). Additional models were analyzed and compared to the baseline model. As depicted in Table 1, these models all fit the data poorly, demonstrating inadequate fit indices. Furthermore, χ2 difference tests revealed that all additional constraints significantly degraded the fit of the baseline model (all ps <.001). Latent construct means for the entire sample are depicted in Figure 1.
Table 1.
Model Fit and χ2 Difference Tests for One-Factor, Two-Factor, and Three-Factor Models
| χ2 | p value | CFI | TLI | RMSEA | |
|---|---|---|---|---|---|
| Four-factor | |||||
| Baseline | 62.025 | .002 | .979 | .986 | .062 |
| Two-factor | |||||
| Factor 1: SEFC, SEVC | |||||
| Factor 2: PEFV-P, PEFV-S | 165.874 | .000 | .898 | .917 | .152 |
| One-factor | 396.215 | .000 | .727 | .751 | .264 |
| Uncorrelated four-factor | 283.479 | .000 | .805 | .759 | .260 |
NOTE: All χ2 values for difference testing are statistically significant (ps < .001), indicating that the two-factor, one-factor, and uncorrelated four-factor mode l constraints significantly degrade the fit of the correlated three-factor model. CFI = comparative fit index; TLI = Tucker–Lewis index; RMSEA = root mean square error of approximation; SEFC = self-efficacy for fruit consumption; SEVC = self-efficacy for vegetable consumption; PEFV-P = proxy efficacy from parents; PEFV-S = proxy efficacy from after-school staff.
Baseline Model Fit Across Subgroups
Tables 2 and 3 provide latent construct means and baseline model fits for each subgroup, respectively. Ethnicity was controlled for in the model fit for SES subgroups and vice versa. As depicted, the baseline models fit well for all subgroups. For the gender subgroups, all freely estimated factor loadings were statistically significant (all ps < .001) and salient (R2s range = .377-.958), which also resulted for both SES subgroups (R2s range = .284-.933) and for the ethnicity group (R2s range = .321-.914). Lastly, there were no remarkable points of strain noted in any of the models. Thus, results provide strong support for the structure of the baseline model across each child subgroup.
Table 2.
Construct Means, Standard Deviations, Skewness, and Kurtosis Statistics for Gender, Socioeconomic Status, and Racial/Ethnic Subgroups
| Factor Label | Subgroup | M | SD | Skewness | Kurtosis |
|---|---|---|---|---|---|
| SEFC | |||||
| Male | 2.53 | 0.55 | −1.08 | 0.26 | |
| Female | 2.54 | 0.53 | −1.02 | 0.19 | |
| Low SES | 2.54 | 0.57 | −1.03 | 0.04 | |
| High SES | 2.51 | 0.51 | −1.02 | 0.38 | |
| Caucasian | 2.50 | 0.54 | −0.94 | −0.02 | |
| African American | 2.58 | 0.55 | −1.37 | 1.15 | |
| SEVC | |||||
| Male | 2.36 | 0.67 | −0.78 | −0.61 | |
| Female | 2.35 | 0.62 | −0.56 | −0.79 | |
| Low SES | 2.37 | 0.70 | −0.75 | −0.72 | |
| High SES | 2.36 | 0.59 | −0.70 | −0.44 | |
| Caucasian | 2.38 | 0.63 | −0.78 | −0.49 | |
| African American | 2.33 | 0.72 | −0.64 | −0.94 | |
| PEFV-P | |||||
| Male | 2.52 | 0.56 | −1.08 | 0.31 | |
| Female | 2.49 | .054 | −1.09 | 0.48 | |
| Low SES | 2.46 | 0.60 | −1.04 | 0.15 | |
| High SES | 2.53 | 0.50 | −1.04 | 0.41 | |
| Caucasian | 2.47 | 0.54 | −0.83 | −0.22 | |
| African American | 2.58 | 0.56 | −1.60 | 2.00 | |
| PEFV-S | |||||
| Male | 2.07 | 0.65 | −0.09 | −1.03 | |
| Female | 1.97 | 0.64 | 0.049 | −1.09 | |
| Low SES | 2.09 | 0.66 | −0.16 | −1.11 | |
| High SES | 1.92 | 0.63 | 0.12 | −0.96 | |
| Caucasian | 1.95 | 0.64 | 0.09 | −1.01 | |
| African American | 2.17 | 0.62 | −0.26 | −0.86 |
NOTE: Male, n = 119; female, n = 119; low SES, n = 110; high SES, n = 110; Caucasian, n = 141; African American, n = 50. SEFC = self-efficacy for fruit consumption; SEVC = self-efficacy for vegetable consumption; PEFV-P = proxy efficacy from parents; PEFV-S = proxy efficacy from after-school staff; SES = socioeconomic status.
Table 3.
Model Fit and χ2 Statistics Across Gender, Socioeconomic, and Racial/Ethnic Subgroups
| χ2 | p Value | CFI | TLI | RMSEA | χ2 Difference | Difference Test p Value | |
|---|---|---|---|---|---|---|---|
| Base model fit | |||||||
| Boys (n = 113) | 52.093 | .003 | .962 | .976 | .091 | ||
| Girls (n = 113) | 38.512 | .041 | .976 | .982 | .069 | ||
| Higher SES (n = 110) | 51.616 | .004 | .951 | .963 | .088 | ||
| Lower SES (n = 110) | 39.043 | .080 | .980 | .984 | .060 | ||
| Race/ethnicity (Caucasian, n =141; African American, n =50) | 65.648 | .002 | .975 | .983 | .066 | ||
| Measurement invariance | |||||||
| Model 1: Gender | |||||||
| Equal form | 88.670 | .002 | .972 | .981 | .075 | ||
| Model 2: Gender | |||||||
| Equal factor loadings and indicator thresholds | 90.615 | .003 | .973 | .983 | .072 | 7.858 | .448 |
| Model 1: SES | |||||||
| Equal form | 92.983 | .001 | .960 | .973 | .081 | ||
| Model 2: SES | |||||||
| Equal factor loadings and indicator thresholds | 91.663 | .002 | .963 | .976 | .076 | 5.490 | .704 |
| Population heterogeneity | |||||||
| Model 3: Gender | |||||||
| Equal factor variance | 90.738 | .004 | .973 | .984 | .071 | 10.686 | .383 |
| Model 4: Gender | |||||||
| Equal factor covariances | 60.154 | .034 | .985 | .987 | .062 | 9.112 | .427 |
| Model 5: Gender | |||||||
| Equal latent mean | 73.374 | .027 | .983 | .988 | .060 | 6.137 | .726 |
| Model 3A: SES | |||||||
| Equal factor variance | 101.611 | .000 | .954 | .971 | .084 | 21.723 | .017* |
| Model 3B: SES | |||||||
| Equal factor partial invariance (SEVC freed) | 94.929 | .001 | .961 | .975 | .078 | 11.544 | .240 |
| Model 4: SES | |||||||
| Equal factor covariance: partial invariance (SEVC freed) | 75.527 | .005 | .971 | .978 | .074 | 8.666 | .278 |
| Model 5: | |||||||
| Equal latent mean: partial factor variance and covariance (SEVC freed) | 76.555 | .004 | .970 | .977 | .076 | 14.285 | .160 |
NOTE: CFI = comparative fit index; TLI = Tucker–Lewis index; RMSEA = root mean square error of approximation; SES = socioeconomic status; SEVC = self-efficacy for vegetable consumption.
p < .05.
Measurement Invariance and Population Heterogeneity Across Gender Groups
Table 3 provides χ2 values for invariance testing across gender groups. Model 1 analyzed factor structure equality across gender (equal form), which fit the data well and served as the baseline model for subsequent tests of invariance, χ2 = 88.670, p = .002. Next, factor loadings and indicator thresholds were tested for equivalence (Model 2), determining whether the measures had the same meaning and structure for males compared to females. Model 2 had an overall good fit to the data and did not significantly degrade fit relative to the equal form solution, χ2(8)Diff = 7.858, p = .448.
To test population heterogeneity, three additional models were analyzed, progressively constraining factor variances, factor covariances, and factor means, respectively. Model 3 examined equality of variances among the four constructs across gender and did not degrade the model fit, χ2(10)Diff = 10.686, p = .383. Thus, each latent construct has equal within-variance dispersion across gender subgroups. Second, Model 4 constrained factor covariances to be equal, testing whether the latent variables are more strongly related to each other in one gender compared to the other. As shown, this constraint did not degrade the model, χ2(9)Diff = 9.112, p =.427. Finally, Model 5 constrained the factor means to equality, which again did not degrade model fit, indicating that males and females do not differ in their levels of the four latent constructs, χ2(9)Diff = 6.137, p = .726.
Measurement Invariance and Population Heterogeneity Across SES Groups
The models tested across SES subgroups are presented in Table 3. Model 1 examined equal form, providing an acceptable fit to the data, χ2 = 92.983, p = .001, CFI = .960, TLI = .973, and RMSEA = .081. Model 2 tested equality of factor loadings and indicator thresholds, which demonstrated good fit to the data and did not significantly degrade fit relative to the equal form solution, χ2(8)Diff = 5.490, p = .704. Thus, the indicators evidence comparable relationships to the four latent constructs in both SES subgroups.
Concerning population heterogeneity, the equal factor variance constraint did significantly degrade the fit of the model (p value < .05), indicating that the within-group dispersion of one or more of the constructs differs across the SES groups, χ2(10)Diff = 21.723, p = .017. To identify the unequal latent variable(s), constraints on factor variances with the highest modification index (MI) values were released consecutively until the partially unconstrained model did not significantly degrade model fit. The SEVC constraint had the highest MI value, which was released first and led to a nonsignificant degrade in model fit, χ2(9)Diff = 11.544, p = .240 (Model 3).
Nonequality of SEVC factor variances did not allow equality of factor covariance tests for this construct; however, constraints placed on the equality of the remaining three latent variable covariances did not degrade the fit of the model, χ2(7)Diff = 8.666, p = .278 (Model 4). This demonstrates equal factor covariances across SES groups for the latent constructs SEFC, PEFV-P, and PEFV-S. Model 5 examined equality latent construct means and did not degrade model fit, indicating that higher and lower SES children do not significantly differ in their average levels of the four latent factors, χ2(10)Diff = 14.285, p = .160.
Measurement Invariance and Population Heterogeneity Across Ethnicity Groups
The MIMC model, controlling for SES, provided a good fit to the data (Table 4), χ2(40) = 70.293, p = .004, CFI = .980, TLI = .986, and RMSEA = .054. Inclusion of the ethnicity covariate did not alter the factor structure, and all items remained significant indicators of their hypothesized latent factor (all ps < .001). Next, regression coefficients provided information regarding equal indicator thresholds across ethnicity groups. An invariant indicator was determined by fixing all the direct effects between the covariate and the indicators to zero and inspecting MI values. MI values for all fixed effects between ethnicity and each indicator were appropriately low, with the highest index equaling .773, demonstrating indicator invariance across Caucasian and African American children.
Finally, equality of the four latent factor means was analyzed. Specifically, any significant direct effect of the ethnicity covariate on any of the four latent factors represented population heterogeneity. Although the African American subgroup demonstrated higher mean scores on all latent variables except for SEVC (see Table 2), these differences were not significant (all ps >.05).
DISCUSSION
This study supported the hypothesis that self-efficacy is multidimensional among elementary school–aged children, characterized by self-efficacy for fruit consumption, self-efficacy for vegetable consumption, proxy efficacy to influence parents, and proxy efficacy to influence after-school staff. Second, the hypothesis that self- and proxy efficacy would be invariant across different demographic groups was also supported. Specifically, complete invariance was established across gender, SES, and ethnicity groups. Finally, population heterogeneity did not exist across gender and ethnicity groups and existed only minimally among SES subgroups. Several conclusions can be made from these findings.
First, the existence of four underlying factors representing self-efficacy for FVC suggests that self-efficacy can be assessed as an independent but related construct to proxy efficacy. This result supports findings from a previous EFA (Geller et al., 2009) and findings in the physical activity domain (Dzewaltowski et al., 2007) but refutes reports of self-efficacy for FVC as a unidimensional construct (Reynolds et al., 2002). An explanation for this contrast may be the face validity of the different measures used among these separate studies. Specifically, Reynolds and colleagues (2002) used 17 self-efficacy items targeting children’s self-efficacy (“I can …”) and only 4 proxy efficacy items (“I can ask my mom or dad …”). Thus, weak factor separation may have resulted from inclusion of more than 3 times as many self-efficacy items. Previous research (Geller et al., 2009) and the current study devoted specific attention to the conceptual distinction between self- and proxy efficacy, illuminating these to be independent but related constructs.
Second, there are additional latent constructs that define self- and proxy efficacy for FV. First, self-efficacy for fruit consumption is an independent but related construct to self-efficacy for vegetable consumption. This supports previous research, reporting that fruit consumption and vegetable consumption are independent behaviors (Gibson, Wardle, & Watts, 1998; Reinaerts et al., 2006; Vereecken et al., 2005). Thus, interventions should take into account that these are separate behaviors with different influencing factors. Second, two separate scales for proxy efficacy were also confirmed, capturing children’s proxy efficacy to influence both their parents and their after-school staff. Thus, children’s proxy efficacy to influence others to provide FV varies according to the authority figure in control of their environment.
Third, our findings indicate that the current measure is invariant across gender, SES, and ethnicity groups; thus, it is completely generalizable to these subgroups. This supports previous research reporting that self-efficacy is invariant across separate subgroups for physical activity, a related health behavior to FVC (Dishman et al., 2002; Martin, 2008; Paxton et al., 2008). Furthermore, all latent variable variances were equal for males and females; however, the latent variable SEVC was not invariant across SES subgroups. Specifically, the amount of variability in SEVC within the lower SES subgroup was significantly smaller, indicating more variability in SEVC among higher SES children. Finally, results also demonstrated that the covariance between all four of the latent constructs were equal for both genders, as were the relationships between the latent constructs SEFC, PEFV-P, and PEFV-S for both SES subgroups.
Established measurement invariance across subgroups allowed us to analyze equality of latent means. In other words, do subgroups differ in their levels of the latent variables? Results demonstrated that males and females had equal latent variable means, supporting previous research and our expectations (Geller et al., 2009; Granner et al., 2004). Therefore, in consideration of research reporting higher FVC among females compared to males (Bere, Brug, & Klepp, 2007; Lien, Jacobs, & Klepp, 2002; Lien, Lytle, & Klepp, 2001; Rasmussen et al., 2006; Sweeting, Anderson, & West, 1994), results here suggest that these gender differences in FVC are not resulting from differences in self- or proxy efficacy.
Furthermore, no latent mean differences were found between SES subgroups or between Caucasian and African American subgroups. This finding contradicts previous research, reporting differences in PEFV-P based on the SES and ethnic diversity classification of the children’s schools (Geller et al., 2009). However, in the current analyses, SES and ethnicity were looked at uniquely by covarying out the variance of SES in the ethnicity model and vice versa; thus, testing only the unique impact of SES and ethnicity may have reduced statistical strength. It is also possible that the school environment (i.e., concentration of high and low SES and racial/ethnic diversity) affects children’s proxy efficacy rather than individual-level demographic characteristics.
Study Limitations and Strengths
Limitations of this study should be noted. First, analyses relied on self-report data, which can result in numerous biases, such as social desirability bias, unwillingness to be truthful, and/or misunderstanding. Second, the subgroup sample sizes for ethnicity were not adequate to run a multigroup CFA, limiting invariance tests to equality of indicator loadings and equality of latent means. Lastly, the African American subgroup was considerably small and may not be representative of the larger population.
The main strength of the current analyses is the use of CFA to investigate differences in latent construct means. When using these modeling techniques to evaluate psychological measurements, detailed invariance information and population heterogeneity tests are provided that cannot be performed in more simplified analyses (i.e., ANOVA). For example, the incorporation of means in a CFA allows for the analysis of between-group indicator thresholds. Moreover, unlike simple mean comparisons, CFA comparisons are conducted within a measurement model that allows for the incorporation and adjustment of all measurement error.
Implications for Practitioners
A central mechanism of health behavior change according to SCT is children’s confidence to exert personal agency and proxy agency. Practitioners can assess children’s beliefs underlying this behavior change mechanism with the self- and proxy efficacy scale items validated in this study. Results demonstrated that constructs were assessed consistently among elementary school–aged children and across different demographic subgroups. This informs practitioners that these measures can be applied uniformly to all members of these subgroups. For example, a school nutritionist focused on increasing students’ FVC using self- and proxy efficacy components can apply and/or measure these constructs without the concern of biasing toward any one subgroup. Furthermore, considering subgroups demonstrated equal levels of self- and proxy efficacy (latent means), practitioners can apply self- and proxy efficacy strategies to members of these different subgroups using the same intensity.
This study illuminated that self-efficacy beliefs and proxy efficacy beliefs are independent and related constructs. Children who lack confidence to eat fruits may be confident to eat vegetables. As depicted in the Figure 1, children’s overall mean scores on the latent constructs self-efficacy to eat fruit (2.527) and self-efficacy to eat vegetables (2.362) were both high on a scale ranging from 1 to 3. In other words, on average, children are between somewhat sure and very sure that they can consume between 1 and 3 servings of both fruit and vegetables per day. The Centers for Disease Control and Prevention (2003) recommends that children aged 9 to 11 years consume 1.5 to 2 cups of fruit and 1.5 to 3 cups of vegetables per day; thus, practitioners are encouraged to continue the development of both children’s self-efficacy to consume fruit and their self-efficacy to consume vegetables in order to reach these goals.
Similarly, children’s confidence to influence after-school staff is not the same construct as their confidence to influence parents. Also in Figure 1 are children’s overall mean scores on these latent constructs. As seen, children report higher proxy efficacy from their parents (2.501) in comparison to proxy efficacy from their after-school staff (1.997) on a scale ranging from 1 to 3. This difference reflects children’s higher confidence to request FV availability from their parents compared to the authority figures during after-school time. Considering the amount of time children spend in school and the increasing use of after-school programs, practitioners should focus on increasing children’s confidence to request FV from authority figures who rule environments outside their home.
CONCLUSIONS
Overall, this research provides evidence supporting the factorial invariance of a theory-derived (SCT) measurement of self- and proxy efficacy for FVC across gender, SES, and ethnicity. This sanctions meaningful and truthful comparison of the latent constructs SEFC, SEVC, PEFV-P, and PEFV-S between male and female children, lower and higher SES children, and African American and Caucasian children. Research can now utilize these measurements in studies examining the potential impact of self- and proxy efficacy for FV on some additional variable(s) across subgroups of elementary school–aged children. Future research should apply these latent constructs into structural equation models to evaluate relationships with children’s FVC. Finally, interventions should be used to investigate if altering these identified latent constructs can cause increases in children’s FVC.
Acknowledgments
This study was supported by National Research Initiative grant (no. 2005-35215-15418) from the USDA Cooperative State Research, Education, and Extension Service Human Nutrition and Obesity Program. We thank Karla Bruggeman, Tanis Hastmann, Richard Rosenkranz, and Sara Rosenkranz for assisting with the development of the questionnaire and data collection.
Contributor Information
Karly S. Geller, Cancer Research Center of Hawaii, University of Hawaii at Manoa.
David A. Dzewaltowski, Department of Kinesiology and Community Health Institute, Kansas State University, Manhattan Kansas.
References
- Bandura A. Social foundations of thought and action: A social cognitive theory. Englewood Cliffs, NJ: Prentice-Hall; 1986. [Google Scholar]
- Bandura A. Social cognitive theory: An agentic perspective. Annual Review of Psychology. 2001;52:1–26. doi: 10.1146/annurev.psych.52.1.1. [DOI] [PubMed] [Google Scholar]
- Bentler PM. Comparative fit indexes in structural models. Psychological Bulletin. 1990;107(2):238–246. doi: 10.1037/0033-2909.107.2.238. [DOI] [PubMed] [Google Scholar]
- Bentler PM, Bonett DG. Significance tests and goodness of fit in the analysis of covariance structures. Psychological Bulletin. 1980;88:588–606. [Google Scholar]
- Bere E, Brug J, Klepp KI. Why do boys eat less fruit and vegetables than girls? Public Health Nutrition. 2007;11:321–325. doi: 10.1017/S1368980007000729. [DOI] [PubMed] [Google Scholar]
- Brown TA. Confirmatory factor analysis for applied research. New York: Guilford; 2006. [Google Scholar]
- Browne MW, Cudeck R. Alternate ways of assessing model fit. In: Bollen KA, Long JS, editors. Testing structural equation models. Newbury Park, CA: Sage; 1993. pp. 136–162. [Google Scholar]
- Centers for Disease Control and Prevention. Youth risk behavior surveillance—United States. Morbidity and Mortality Weekly Report. 2003;53(SS-05):1–108. [Google Scholar]
- Cullen KW, Bartholomew LK, Parcel GS, Koehly L. Measuring stage of change for fruit and vegetable consumption in 9- to 12-year-old girls. Journal of Behavioral Medicine. 1998;21(3):241–254. doi: 10.1023/a:1018764932609. [DOI] [PubMed] [Google Scholar]
- Dishman RK, Motl RW, Saunders RP, Dowda M, Felton G, Ward DS, et al. Factorial invariance and latent mean structure of questionnaires measuring social-cognitive determinants of physical activity among Black and White adolescent girls. Preventive Medicine. 2002;34(1):100–108. doi: 10.1006/pmed.2001.0959. [DOI] [PubMed] [Google Scholar]
- Domel SB, Baranowski T, Davis HC, Thompson WO, Leonard SB, Baranowski J. A measure of stages of change in fruit and vegetable consumption among fourth- and fifth-grade school children: Reliability and validity. Journal of the American College of Nutrition. 1996;15(1):56–64. doi: 10.1080/07315724.1996.10718565. [DOI] [PubMed] [Google Scholar]
- Dzewaltowski DA, Karteroliotis K, Welk G, Johnston JA, Nyaronga D, Estabrooks PA. Measurement of self-efficacy and proxy efficacy for middle school youth physical activity. Journal of Sport & Exercise Psychology. 2007;29(3):310–332. doi: 10.1123/jsep.29.3.310. [DOI] [PubMed] [Google Scholar]
- Geller KS, Dzewaltowski DA, Rosenkranz RR, Karteroliotis K. Measuring children’s self-efficacy and proxy efficacy related to fruit and vegetable consumption. Journal of School Health. 2009;79(2):51–57. doi: 10.1111/j.1746-1561.2008.00376.x. [DOI] [PubMed] [Google Scholar]
- Gibson EL, Wardle J, Watts CJ. Fruit and vegetable consumption, nutritional knowledge and beliefs in mothers and children. Appetite. 1998;31(2):205–228. doi: 10.1006/appe.1998.0180. [DOI] [PubMed] [Google Scholar]
- Granner ML, Sargent RG, Calderon KS, Hussey JR, Evans AE, Watkins KW. Factors of fruit and vegetable intake by race, gender, and age among young adolescents. Journal of Nutrition Education and Behavior. 2004;36(4):173–180. doi: 10.1016/s1499-4046(06)60231-5. [DOI] [PubMed] [Google Scholar]
- Hu L, Bentler PM. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural Equation Modeling. 1999;6:1–55. [Google Scholar]
- Kratt P, Reynolds K, Shewchuk R. The role of availability as a moderator of family fruit and vegetable consumption. Health Education & Behavior. 2000;27(4):471–482. doi: 10.1177/109019810002700409. [DOI] [PubMed] [Google Scholar]
- Lien N, Jacobs DR, Jr, Klepp KI. Exploring predictors of eating behaviour among adolescents by gender and socio-economic status. Public Health Nutrition. 2002;5(5):671–681. doi: 10.1079/PHN2002334. [DOI] [PubMed] [Google Scholar]
- Lien N, Lytle LA, Klepp KI. Stability in consumption of fruit, vegetables, and sugary foods in a cohort from age 14 to age 21. Preventive Medicine. 2001;33(3):217–226. doi: 10.1006/pmed.2001.0874. [DOI] [PubMed] [Google Scholar]
- Martin AJ. Motivation and engagement in music and sport: Testing a multidimensional framework in diverse performance settings. Journal of Personality. 2008;76(1):135–170. doi: 10.1111/j.1467-6494.2007.00482.x. [DOI] [PubMed] [Google Scholar]
- Muthen LK, Muthen B. Mplus user’s guide. 5. Los Angeles: Muthen & Muthen; 2007. [Google Scholar]
- O’Dea JA, Wilson R. Socio-cognitive and nutritional factors associated with body mass index in children and adolescents: Possibilities for childhood obesity prevention. Health Education Research. 2006;21(6):796–805. doi: 10.1093/her/cyl125. [DOI] [PubMed] [Google Scholar]
- Paxton RJ, Nigg CR, Motl RW, McGee K, McCurdy D, Matthai CH, et al. Are constructs of the transtheoretical model for physical activity measured equivalently between sexes, age groups, and ethnicities? Annals of Behavioral Medicine. 2008;35:308–318. doi: 10.1007/s12160-008-9035-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Perez-Lizaur AB, Kaufer-Horwitz M, Plazas M. Environmental and personal correlates of fruit and vegetable consumption in low income, urban Mexican children. Journal of Human Nutrition and Dietetics. 2008;21(1):63–71. doi: 10.1111/j.1365-277X.2007.00839.x. [DOI] [PubMed] [Google Scholar]
- Rasmussen M, Krolner R, Klepp KI, Lytle L, Brug J, Bere E, et al. Determinants of fruit and vegetable consumption among children and adolescents: A review of the literature. Part I: Quantitative studies. International Journal of Behavioral Nutrition and Physical Activity. 2006;3:22. doi: 10.1186/1479-5868-3-22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Reinaerts E, Nooijer J, Candel M, Vries N. Explaining school children’s fruit and vegetable consumption: The contributions of availability, accessibility, exposure, parental consumption and habit in addition to psychosocial factors. Appetite. 2006;48:248–258. doi: 10.1016/j.appet.2006.09.007. [DOI] [PubMed] [Google Scholar]
- Reynolds KD, Baranowski T, Bishop DB, Farris RP, Binkley D, Nicklas TA, et al. Patterns in child and adolescent consumption of fruit and vegetables: Effects of gender and ethnicity across four sites. Journal of the American College of Nutrition. 1999;18(3):248–254. doi: 10.1080/07315724.1999.10718859. [DOI] [PubMed] [Google Scholar]
- Reynolds KD, Yaroch AL, Franklin FA, Maloy J. Testing mediating variables in a school-based nutrition intervention program. Health Psychology. 2002;21(1):51–60. [PubMed] [Google Scholar]
- Sharma M, Wagner DI, Wilkerson J. Predicting childhood obesity prevention behaviors using social cognitive theory. International Quarterly of Community Health Education. 2005;24(3):191–203. doi: 10.2190/CPVX-075A-L30Q-2PVM. [DOI] [PubMed] [Google Scholar]
- Sweeting H, Anderson A, West P. Socio-demographic correlates of dietary habits in mid to late adolescence. European Journal of Clinical Nutrition. 1994;48(10):736–748. [PubMed] [Google Scholar]
- U.S. Department of Agriculture. Dietary guidelines for Americans. Washington, DC: Government Printing Office; 2005. [Google Scholar]
- Vereecken CA, Van Damme W, Maes L. Measuring attitudes, self-efficacy, and social and environmental influences on fruit and vegetable consumption of 11- and 12-year-old children: Reliability and validity. Journal of the American Dietetic Association. 2005;105(2):257–261. doi: 10.1016/j.jada.2004.11.008. [DOI] [PubMed] [Google Scholar]