

Abstract
Background:
We have previously shown that children with autism spectrum disorder (ASD) have specific handwriting deficits consisting of poor form, and that these deficits are predicted by their motor abilities. It is not known whether the same handwriting impairments persist into adolescence and whether they remain linked to motor deficits.
Methods:
A case-control study of handwriting samples from adolescents with and without ASD was performed using the Minnesota Handwriting Assessment. Samples were scored on an individual letter basis in 5 categories: legibility, form, alignment, size, and spacing. Subjects were also administered an intelligence test and the Physical and Neurological Examination for Subtle (Motor) Signs (PANESS).
Results:
We found that adolescents with ASD, like children, show overall worse performance on a handwriting task than do age- and intelligence-matched controls. Also comparable to children, adolescents with ASD showed motor impairments relative to controls. However, adolescents with ASD differ from children in that Perceptual Reasoning Indices were significantly predictive of handwriting performance whereas measures of motor skills were not.
Conclusions:
Like children with ASD, adolescents with ASD have poor handwriting quality relative to controls. Despite still demonstrating motor impairments, in adolescents perceptual reasoning is the main predictor of handwriting performance, perhaps reflecting subjects' varied abilities to learn strategies to compensate for their motor impairments.
GLOSSARY
- ASD
= autism spectrum disorder;
- DSM-IV
= Diagnostic and Statistical Manual of Mental Disorders, 4th edition;
- PANESS
= Physical and Neurological Examination for Subtle (Motor) Signs;
- PRI
= Perceptual Reasoning Index;
- WASI
= Wechsler Abbreviated Scale of Intelligence;
- WISC
= Wechsler Intelligence Scale for Children IV.
Autism spectrum disorder (ASD) is diagnosed based on poor social and communicative abilities, as well as repetitive and limited behaviors and interests.1 We recently showed that children with ASD also demonstrate worse overall handwriting than controls.2 Moreover, children with ASD demonstrate motor impairments, and these impairments were predictive of handwriting quality while age, gender, and intelligence were not. Given the importance of handwriting for academic progress and social and communicative development,3 that study suggested that handwriting problems may be contributing to the developmental struggle of children with ASD and that impaired motor control may be a driving factor behind these problems. In this study, we assessed whether handwriting impairments in ASD persist through adolescence and, if so, whether impairments are also predicted by motor abilities or if different factors drive performance in older subjects.
METHODS
Subjects.
Twenty-four subjects between 12 and 16 years of age participated in the study: 12 with ASD (1 female) and 12 typically developing controls (1 female). Based on performance on either the Wechsler Intelligence Scale for Children IV (WISC) or the Wechsler Abbreviated Scale of Intelligence (WASI), all subjects had Perceptual Reasoning Indices (PRI) greater than 90. Research suggests that task-specific measures of intelligence provide more appropriate assessments of intellectual abilities in children with ASD than general measures.4 Here, the PRI was used as the primary intelligence measure since the study involved nonverbal, perceptually based motor tasks. While the PRI in both the WISC and the WASI consists of the block design and matrix reasoning subtests, the PRI in the WISC additionally consists of the picture concepts subtest. Within the ASD group and control group, however, subjects who received the WISC did not have significantly different PRI or total handwriting scores than subjects who received the WASI.
All subjects with ASD met DSM-IV criteria for ASD1 according to the Autism Diagnostic Observation Schedule-Generic and the Autism Diagnostic Interview-Revised: 9 were diagnosed at the Kennedy Krieger Institute and 3 received diagnoses elsewhere (diagnoses were confirmed by the Social Responsiveness Scale and observation by a medical doctor). Subjects with identifiable causes of autism and known neurologic disorders were excluded.
Standard protocol approvals, registrations, and patient consents.
Written assent to participate was obtained from participants, and written consent was obtained from a parent. Protocols were approved by the Johns Hopkins Institutional Review Board.
Procedure.
Subjects were administered the Minnesota Handwriting Assessment.5 The assessment presents the following words: “The brown jumped lazy fox quick dogs over.” Subjects were instructed to copy the words on a test sheet, making their letters the same size as the sample and using their best handwriting.
Subjects' motor skills were assessed using the revised Physical and Neurological Examination for Subtle (Motor) Signs (PANESS),6 which tests stressed gaits, balance, and timed movements. Since the assessment was scored during administration and researchers were aware of the diagnosis of subjects during testing, the PANESS was unable to be scored blind to group.
Analysis.
Letters were scored, blind to group, on an individual basis in 5 categories according to the Minnesota Handwriting Assessment scoring protocol5:
Category 1: Legibility—Letters must be present, recognizable out of context, have all parts complete, and be lowercase. If these criteria are not met, the letter is marked as an error in all 5 categories.
Category 2: Form—Overall letter quality must be good. Letters must not have gaps or extensions greater than one-sixteenth of an inch. Curved segments cannot have sharp points, and pointed segments cannot be curved. Letters must not contain extra lines.
Category 3: Alignment—Letters must rest within one-sixteenth of an inch above or below the baseline.
Category 4: Size—The tops of letters with ascenders (e.g., k) must be within one-sixteenth of an inch of the top solid line. The tops of letters without ascenders (e.g., a) must be within one-sixteenth of an inch of the middle dotted line. The bottoms of letters with tails (e.g., g) must be within one-sixteenth of an inch of the bottom dotted line.
Category 5: Spacing—Letters within words can be neither touching nor over one-quarter of an inch apart. The distance between words must be at least one-quarter of an inch.
Subjects also received a rate score, earning 1 point for each letter completed within the first 2.5 minutes. Combining the 5 qualitative scores with the rate score, each of the 34 letters can earn up to 6 points, for a maximum total score of 204.
Mean total handwriting scores and mean scores in each category were compared between ASD and control groups with 2-tailed Student t tests. Student t tests were also used to compare age, PRI, and PANESS scores between groups. Within- and across-group stepwise multiple regressions were performed with handwriting scores as the dependent variables and age, PRI, and PANESS scores as predictor variables.
RESULTS
There was no significant difference between groups in age, full-scale IQ, Verbal Comprehension Index, or PRI. Consistent with previous studies, a difference was found for performance on the PANESS, with the control group performing better than the ASD group (table).
Table Demographics and scores
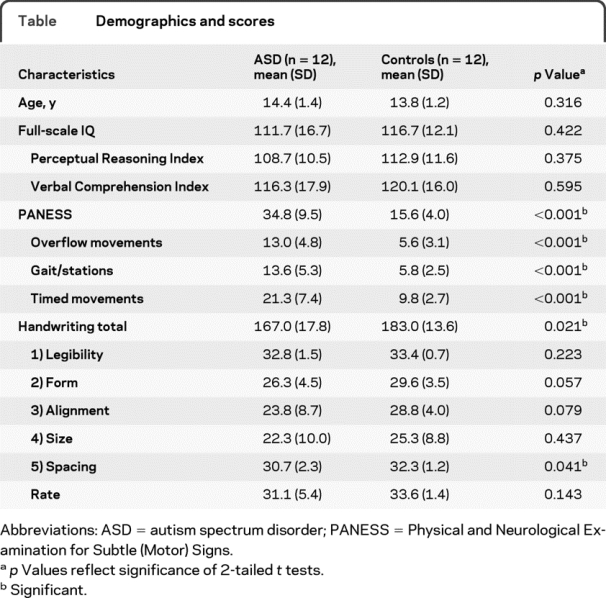
Total handwriting scores were lower in the ASD group than the control group (p = 0.021, figure 1). Within the assessment's subcategories, ASD subjects scored lower in spacing (p = 0.041) and showed a trend toward lower scores in form (p = 0.057, figure 1) and alignment (p = 0.079). No group differences were found for any other category (table).

Figure 1 Average total and form handwriting scores across groups
The control group averaged higher total (A) and form (B) handwriting scores than the autism spectrum disorder (ASD) group. Error bars represent standard error. *p = 0.021; **p = 0.057.
Unlike what was observed previously in children with ASD,2 within this adolescent ASD group we found no relationship between handwriting scores and PANESS scores (figure 2A). Only PRI predicted any handwriting scores in the ASD group (legibility: R2 = 0.39, p = 0.040; size: R2 = 0.79, p < 0.001; total: R2 = 0.59, p = 0.006). Figure 2B shows the relationship between PRI and total handwriting scores within the ASD group. Here we see that PRI explains differing handwriting performance in 2 ASD subjects who have the same PANESS total score. Scores on the Block Design Test, a component of the PRI that measures visuospatial abilities, correlated with total handwriting scores in the ASD group (r = 0.73, p = 0.011). When both were entered into a stepwise multiple regression as predictors of total handwriting scores, however, PRI was the significant predictor, suggesting that perceptual reasoning beyond just visuospatial abilities is the best tested predictor of handwriting performance in ASD. In contrast, within the control group, PANESS total scores predicted total handwriting performance (R2 = 0.39, p = 0.030); no other scores were predicted by any parameters.

Figure 2 Perceptual Reasoning Index (PRI) predicts handwriting performance in adolescents with autism spectrum disorder (ASD)
Total Physical and Neurological Examination for Subtle (Motor) Signs (PANESS) scores did not predict total handwriting scores within the ASD group (A). However, PRI predicted total handwriting scores (R2 = 0.61, p = 0.007) (B). The subjects represented by filled-in circle in (A) have the same total PANESS score but very different total handwriting scores. In (B) we see that their handwriting performance is predicted by their PRI (bold circles represent multiple subjects). These subjects' samples are shown in (C): the lower scoring subject's sample is above the higher scoring subject. Higher handwriting scores represent better performance; lower PANESS scores represent better performance; and higher PRIs represent better performance. Lines represent the least squares fits.
Collapsing subjects across groups, the only predictor of handwriting performance was PANESS total score, which predicted legibility (R2 = 0.17, p = 0.048), form (R2 = 0.25, p = 0.019), and total scores (R2 = 0.32, p = 0.005).
DISCUSSION
Here we show that adolescents with ASD have lower overall handwriting quality relative to age-, gender-, and intelligence-matched controls.
A number of studies have demonstrated that individuals with ASD have problems with motor functions, and performance on the PANESS in particular has revealed impairments.7 In children, these impairments are predictive of poor handwriting quality.2 Here, when ASD and control groups are collapsed, motor abilities predict handwriting performance. This effect is driven by the ASD group's worse motor and handwriting performance and the control group's better performance on both measures.
Interestingly, while handwriting performance in children with ASD was predicted by motor performance,2 we found that within adolescents with ASD PRIs predict handwriting performance. The PRI reflects a person's ability to organize and reason through problems with visually presented, nonverbal material. In our previous study, we noted that children with ASD who used strategies to compensate for their motor impairments performed best on the handwriting assessment.2 Since older individuals have more experience writing and likely have had more therapy, the ability of reasoning skills to predict handwriting performance may reflect the ability of adolescents with ASD to learn and utilize compensatory strategies to overcome motor impairments. In addition to more rigorous training of fine motor control, strategies for improving handwriting may include adjusting pencil grip, stabilizing the writing hand with the opposite hand, or forming letters in a more piecemeal fashion. Further research is necessary to confirm this hypothesis since in this study the amount of therapy and accommodations each ASD subject received is unknown. The hypothesis is in line, however, with a previous study that found that individuals with ASD demonstrated motor impairments and within the group IQ was predictive of motor performance.8 These new results reveal that handwriting is still a problem in ASD through adolescence and support the importance of training individuals with ASD, as well as other populations with motor impairments, to overcome or compensate for motor control deficits.
ACKNOWLEDGMENT
The authors thank Lauren Dowell and Lindsay Koenig for their assistance in subject recruitment and data collection. They also thank the Interactive Autism Network as well as all participants in this research study.
DISCLOSURE
Dr. Fuentes reports no disclosures. Dr. Mostofsky has served on a scientific advisory for Bristol-Myers Squibb; serves on the editorial board of Neurocase; and receives research support from the NIH (NINDS R01 NS047781-04 [PI], NINDS R01 NS048527 [PI], NIMH 5 R01 MH078160-03 [PI], and NICHD P50 HD052121-03 [coinvestigator]) and Autism Speaks. Dr. Bastian serves as an Associate Editor for the Journal of Neurophysiology and receives research support from the NIH (NICHD/NCMRR R01 HD040289 [PI], NICHD/NCMRR R01 HD048741 [PI], NINDS R21 NS061189 [coinvestigator], and NICHD/NCMRR R21 HD060169 [coinvestigator]), the Johns Hopkins Brain Sciences Institute, and Autism Speaks.
Address correspondence and reprint requests to Dr. Amy Bastian, Kennedy Krieger Institute, 707 N Broadway-G05, Baltimore, MD 21205 bastian@kennedykrieger.org
Study funding: Supported by an Autism Speaks Pre-Doctoral Fellowship (A.J.B. and C.T.F.), Basic Clinical Science awards (S.H.M.), and NIH Grant R01 NS048527 (S.H.M.).
Disclosure: Author disclosures are provided at the end of the article.
Received May 5, 2010. Accepted in final form July 26, 2010.
REFERENCES
- 1.American Psychiatric Association. Pervasive developmental disorders. In: Diagnostic and Statistical Manual of Mental Disorders: DSM-IV: Text Revision, 4th ed. Washington, DC: American Psychiatric Association; 2000:69–70. [Google Scholar]
- 2.Fuentes CT, Mostofsky SH, Bastian AJ. Children with autism show specific handwriting impairments. Neurology 2009;73:1532–1537. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Feder KP, Majnemer A. Handwriting development, competency, and intervention. Dev Med Child Neurol 2007;49:312–317. [DOI] [PubMed] [Google Scholar]
- 4.Mottron L. Matching strategies in cognitive research with individuals with high-functioning autism: current practices, instrument biases, and recommendations. J Autism Dev Disord 2004;34:19–27. [DOI] [PubMed] [Google Scholar]
- 5.Reisman J. Minnesota Handwriting Assessment. San Antonio, TX: The Psychological Corporation; 1999. [Google Scholar]
- 6.Denckla MB. Revised neurological examination for subtle signs (1985). Psychopharmacol Bull 1985;21:773–800. [PubMed] [Google Scholar]
- 7.Jansiewicz EM, Goldberg MC, Newschaffer CJ, Denckla MB, Landa R, Mostofsky SH. Motor signs distinguish children with high functioning autism and Asperger's syndrome from controls. J Autism Dev Disord 2006 Jul;36:613–621. [DOI] [PubMed]
- 8.Ghaziuddin M, Butler F. Clumsiness in autism and Asperger syndrome: a further report. J Intellect Disabil Res 1998;42:43–48. [DOI] [PubMed] [Google Scholar]