

Abstract
Endoscopic ultrasound allows transmural access to the bile or pancreatic ducts and subsequent contrast injection to provide ductal drainage under fluoroscopy using endoscopic retrograde cholangiopancreatography (ERCP)-based techniques. Differing patient specifics and operator techniques result in six possible variant approaches to this procedure, known as endosonography-guided cholangiopancreatography (ESCP). ESCP has been in clinical use for a decade now, with over 300 cases reported. It has become established as a salvage procedure after failed ERCP in the palliation of malignant biliary obstruction. Its role in the management of clinically severe chronic/relapsing pancreatitis remains under scrutiny. This review aims to clarify the concepts underlying the use of ESCP and to provide technical tips and a detailed step-by-step procedural description.
Keywords: Endosonography, Drainage, Endoscopy, Digestive system, Therapeutics, Endoscopic ultrasound, Endoscopic retrograde cholangiopancreatography
INTRODUCTION
Endoscopic retrograde cholangiopancreatography (ERCP) has become the mainstay of therapy for biliary or pancreatic duct disease. ERCP is increasingly available, safe and effective[1]. Despite all this progress, there remains a patient subset in which ERCP is not possible (e.g. bariatric biliopancreatic diversion, duodenal stent across an intact papilla) or highly challenging (e.g. Roux-en-Y, gastric outlet obstruction[2]). In addition to these circumstances, which can be anticipated and may lead to alternative ductal decompression options from the outset, ERCP can fail unexpectedly for technical reasons, such as failed cannulation (owing to diverticula, tumor infiltration or with a normal papilla), failed guidewire access beyond a stricture, or even failed stent insertion despite adequate guidewire access. Finally, unfavorable clinical outcomes may occur following an apparently technically successful ERCP, such as persistent jaundice after stenting of malignant hilar strictures[3].
The full spectrum of ERCP failure (patients not amenable to ERCP, technical failures and clinical failures) is therefore broader than just “failed cannulation”. Its incidence can be estimated at 3%-5% of all ERCPs, even in expert settings. This puts a considerable burden on patients, since alternative ductal decompression options involve either percutaneous transhepatic cholangiography (PTC) or surgery[4]. PTC and surgery carry higher morbidity and mortality rates than ERCP, and are not a viable option for all patients (e.g. for the percutaneous approach, those with ascites and/or nondilated bile or pancreatic ducts; high risk surgical candidates). Thus, the common statement that unsuccessful ERCP leads to either PTC or surgery is not always borne out in practice, and some patients are inevitably left without optimal treatment.
A salvage drainage technique for failed ERCP is therefore most welcome. Endoscopic ultrasound (EUS) has been used over the last decade to accomplish this goal. Using linear-array echoendoscopes, either a needle or a diathermy catheter can be advanced into the biliary or pancreatic duct under real-time ultrasound guidance. Contrast injection under fluoroscopic monitoring allows cholangiography or pancreatography, a technique originally named endosonography-guided cholangiopancreatography[5] (ESCP). Once the ductogram is obtained, ERCP accessories (guidewires, dilators, stents) are used through the echoendoscope working channel to carry out drainage. ESCP thus represents a hybrid between EUS-guided fine-needle-aspiration (EUS-FNA) and ERCP in terms of equipment, devices and operator skill set. Whereas these two backgrounds are critical to the success of this challenging procedure, it is debatable which one contributes more. It can be argued that ductal access under EUS is just the beginning and the easier part of the procedure[6]. Patient population, sedation requirements, procedure room set-up, and assistant(s) expertise also make ESCP belong in the ERCP realm, as opposed to EUS-guided injection therapies.
ESCP: ORIGIN, EVOLUTION AND DEFINITION OF A UNIFIED CONCEPT
The concept of ESCP as a salvage procedure after failed ERCP was formally proposed in 1996 by Wiersema et al[5]. It was also implicit in three other contemporary reports on EUS-guided pancreatography[7-9]. These authors demonstrated the feasibility and safety of ductal puncture and contrast injection under EUS guidance in 11 patients, with success in 7 out of 10 attempted transduodenal cholangiographies, and one transgastric pancreatography. While the main patient selection criterion for ESCP was failed cannulation, most had only mild obstructive symptoms, final diagnoses that can nowadays be reached at by either MRCP or EUS itself, and eventually successful repeat ERCPs when the diagnosis afforded by ESCP warranted it. This important study however, laid the ground for the subsequent therapeutic use of ESCP.
Giovannini et al[10] were the first to report what later became known as “EUS-guided choledochoduodenostomy”, that is, transmural placement of a biliary stent across the duodenal and distal common bile duct (CBD) walls. Their patient had a pancreatic head mass and two prior ERCPs with failed cannulation. The CBD was imaged from the duodenal bulb with a linear echoendoscope, and entered under EUS guidance with a needle-knife, through which a guidewire was advanced into the CBD under fluoroscopy. The needle-knife was replaced over the wire by a dilator, and the echoendoscope removed over it and exchanged for a duodenoscope, through which a 10F plastic stent was eventually deployed transmurally.
Within four years of this pioneering report, a handful of case reports from a few tertiary referral institutions (six in Europe and three in the USA) described all the 9 different approaches used for ESCP nowadays all over the world[11-22] (Table 1). A total of 39 patients were reported, 13 with chronic/relapsing pancreatitis or transected pancreatic ducts of various etiologies, and 26 with biliary obstruction of predominantly malignant origin (only 6 had benign disease: 3 CBD stones, 2 transected ducts, and 1 primary sclerosing cholangitis). Examining their differing patient populations, minor variations in technique, and the confusing plethora of terms they used to refer to this new procedure, a clear picture emerges of the variables that currently define ESCP. These relate to the patient characteristics, the location of the EUS entry point into the duct, and the access route for ductal decompression - retrograde, antegrade or combined.
Table 1.
The nine different ESCP approaches as defined by the first 39 patients reported from 9 institutions
|
Transpapillary |
Transmural | ||
| Rendezvous | Antegrade | ||
| Pancreatic duct | 1 Bataille et al[11] | 2 Kahaleh et al[13] | 4 François et al[12] |
| 4 Mallery et al[16] | |||
| 1 DeWitt et al*[18] | |||
| 1 Will et al[22] | |||
| Intrahepatic bile duct | 5 Kahaleh et al[21] | 1 Puspok et al[20] | 2 Burmester et al[15] |
| 1 Giovannini et al[10] | |||
| Extrahepatic bile duct | 2 Mallery et al[16] | 1 Puspok et al[20] | 1 Giovannini et al[14] |
| 1 Lai et al[19] | 2 Burmester et al[15] | ||
| 4 Kahaleh et al[17] | 4 Puspok et al[20] | ||
| 1 Kahaleh et al[17] | |||
| 1 Kahaleh et al[21] | |||
Numbers before each author’s name express number of patients reported with a given individual ESCP approach by the author in the referenced article. A total of 19 patients were drained by transpapillary ESCP rendezvous (7 pancreatic, 12 biliary) and 16 transmurally (4 pancreatic, 12 biliary). The dominant approaches were pancreatic rendezvous (7 patients from 4 centers) and chole-dochoduodenstomy (9 patients from 4 centers). *Methylene-blue EUS-guided pancreatography with subsequent non rendezvous ERCP.
It is important to recognize the common ground in which the seemingly different approaches encompassed by ESCP are rooted. This common ground is ductal (biliary or pancreatic) access from the gastrointestinal (GI) tract under EUS guidance, followed by instrumentation under fluoroscopy with the intent to effect drainage, usually - but not necessarily - by means of stent insertion. Initial access is most commonly achieved by needle puncture (EUS-FNA component of the procedure). A guidewire is passed into the duct through the FNA needle, which is then exchanged over the access-keeping wire for the flexible ERCP devices used for drainage. There is a clearer demarcation for access to the bile duct than for pancreatic duct access, between the extrahepatic (CBD) and intrahepatic site. The CBD is best imaged and accessed from the duodenum or distal antrum[5,15-17,19,20], whereas for the left intrahepatic bile duct this is best accomplished from below the cardia[14,15,20,21] (proximal stomach, or jejunum in patients with total gastrectomy and esophago-jejunostomy). Access to the main pancreatic duct (MPD) is usually gained from the stomach[7-9,11-13,16,18,22], although individual operator preference or patient anatomy may make transduodenal MPD puncture the favored option[23]. Whatever the needle entry point into the duct, the guidewire may or may not go through the papilla (or bilio-enterostomy) into the duodenum (or small bowel). Depending on a number of factors, a transpapillary wire thus placed under EUS ductal puncture may be used for retrograde cannulation of the duct of interest through the papilla, and decompression achieved with standard ERCP techniques via the so-called “rendezvous”[4,11,16,17,21,22]. Alternatively, “antegrade” stent insertion through the puncture site and across the papilla is also possible[13,20]. An intraductal guidewire (i.e. not exiting antegradely from the puncture site through the papilla) can be used to decompress the duct towards the GI lumen from the access site by transmural (across the duct and GI walls) stent placement. Transmural stent placement is given a variety of names depending on the anatomic location (i.e. the organs whose walls the stent pierces). The three most common ones are “choledocho-duodenostomy”[24-30], “hepatico-gastrostomy”[14,31,32] and “pancreatico-gastrostomy”[12,23,33].
Although patient selection, intraprocedural technical steps, success and complication rates may vary greatly depending on the target duct (biliary or pancreatic), the concepts and definitions outlined above remain constant. All different ESCP approaches reported to date can be easily categorized with the transmural versus transpapillary drainage route, regardless of the target duct and initial EUS access site. Although transpapillary drainage is most commonly accomplished retrogradely via rendezvous ERCP, antegrade transmural stent insertion also results in transpapillary drainage when the stent is deployed across the papilla or intraductally (i.e. above the papilla) across a distal stricture[20,34,35]. Antegrade transmural intervention combines the ESCP challenges of both transpapillary retrograde access (i.e. guidewire passage across the papilla and/or stricture) and transmural drainage (i.e. puncture tract dilation). Antegrade transmural ESCP might thus be considered a third hybrid category on its own. However, the more defining variable of guidewire placement across the papilla, allows it to be classified as a variant approach for transpapillary drainage. As stated above, the second defining variable is intrahepatic versus extrahepatic access to the bile duct. These two entry routes can, again, be used with transmural and/or transpapillary drainage, giving rise to six possible combinations (Figure 1). This taxonomy and nomenclature are far from perfect. The most obvious inconsistency is that some patients typically drained by ESCP do not actually have a papilla, but a duct-enteric anastomosis (e.g. MPD after Whipple resection or hepatic duct after hepatico-jejunostomy), and hence “transpapillary” is not semantically accurate. Aside from that, this is a comprehensive and clear categorization of ESCP as a unified concept for ductal access and drainage. The many alternative terms put forward are perhaps more confusing.
Figure 1.

The three potential ESCP access routes: intrahepatic (1, 2), extrahepatic (3, 4) and pancreatic (5, 6). After ductal access through any of them, drainage can be accomplished transmurally over an intraductal guidewire (1, 3, 6) via hepaticogastrostomy (1), choledochoduodenostomy (3) or pancreaticogastrostomy (6). Transpapillary guidewire placement (2, 4, 5) allows both retrograde access via rendezvous ERCP and antegrade stent placement for biliary (2, 4) or pancreatic duct drainage (5). Rendezvous requires an accessible papilla and is preferable in benign disease. Antegrade transpapillary ESCP suits complex postoperative anatomy, particularly when performed for palliation of malignant obstruction.
To further complicate matters, transpapillary drainage, wheter antegrade or via rendezvous, is occasionally combined with transmural stent placement, again with two possible variations. A single long plastic stent bridges both the papilla and the transmural puncture site[13]. Alternatively, dual drainage can be carried out by serially inserting one transpapillary stent (usually metal) and a second transmural stent (usually plastic) or drain[20,32]. Transmural stent placement may be the end result of either failure to maneuver the guidewire across the papilla[27,34,36,37], or the initially chosen approach[24,38]. In the former case, temporary transmural stenting can be converted at a follow-up session to transpapillary drainage[17,20,35].
PATIENT SELECTION
Patients reported in the various ESCP series share two important features: (1) Symptomatic disease of proven biliary or pancreatic ductal origin; and (2) Impossible ERCP despite thorough cannulation attempts, including pre-cut, by highly experienced endoscopists. ESCP should not therefore be used for diagnosis in certain settings where ERCP might still be rightly considered (e.g. high level of suspicion of CBD stones in a patient with a low risk of post-ERCP complications)[36]. In patients with low-grade or transient biliary obstruction, complete imaging work-up, including diagnostic EUS and MRCP, is warranted before proceeding to ESCP[37]. Similarly, pancreatic patients subjected to ESCP have been highly selected, based both on the anatomy (pancreatic duct dilation, transection or fistula) and on clinical grounds (intractable pain, recurrent pancreatitis). In other words, since the threshold for ERCP is lower, ESCP is not necessarily justified in all patients in whom ERCP has been unsuccessful. The threshold for ESCP should at least be the same as for PTC, and clinical follow-up as opposed to aggressive repeat attempts at ductal access is advisable in those patients with mild symptoms and negative or inconclusive imaging work-up.
ESCP should not be used as a shortcut for gaining ductal access in the setting of only moderately difficult cannulation. This is in contrary to some optimistic views based on the fact that the papilla is not manipulated during ESCP, which have led to speculation that it may offer a potentially less invasive biliary drainage option than ERCP[20,39]. This view underestimates the difficulty and risks of ESCP. The toughest ERCP might be preferable to the easiest ESCP. The anatomic problems precluding ERCP in the ESCP literature range from complex postoperative anatomy (Roux-en-Y, Whipple) and severe tumor infiltration with or without duodenal stenosis, to high-grade hilar strictures and complete duct transections. Patients with lesser degrees of difficulty may be better served by a repeat attempt at ERCP, whether this is performed by the same or by a more experienced operator.
Biliary versus pancreatic indications
Biliary ESCP has been reported in well over 300 cases[10,15-21,23-35,39-42], whereas approximately only 130 pancreatic ESCP cases have been published[11,13,16-22,43-46]. This is despite the fact that percutaneous duct access with or without rendezvous is more readily available for biliary than pancreatic duct decompression. There is a fourfold explanation for this. Firstly, biliary obstruction is a more frequent and usually more pressing clinical problem than pancreatic duct obstruction, the latter typically presenting as chronic or relapsing pain in the setting of chronic pancreatitis. Secondly, the technical challenges in accessing the MPD through a hard, fibrotic pancreatic parenchyma, and successfully negotiating a guidewire through a tortuous duct with many side branches, are much greater than those involved in biliary ESCP. Thirdly, the risks involved in pancreatic ESCP appear to be greater than those of biliary ESCP[45]. Finally, whereas the clinical response to drainage is easily assessed for biliary obstruction (resolution of jaundice or stone removal), it is less obvious for refractory pain caused by chronic pancreatitis, just as the clinical outcomes of pancreatic ERCP are somewhat less favorable than those of biliary ERCP.
These factors are reflected in the relative clinical success and complication rates for biliary (75%-100% success and 10%-36% complications) versus pancreatic (25%-100% success and 15%-50% complications) ESCP. These are summarized in Tables 2 and 3. Whereas biliary ESCP is gradually gaining acceptance in many tertiary endoscopy units, pancreatic ESCP remains confined to very select units with special expertise in pancreatic endotherapy[37].
Table 2.
Major series on EUS-guided biliary drainage
| Year | Author | n (malignant/benign) | Access route | Drainage success - Drainage route | Complications |
| 2009 | Horaguchi[35] | 16 (15/1) | 8 EH 8 IH | 15/16 (94%) - 8 TD - 6 TG - 2 TE | 2 (12. 50%) - 1 bile peritonitis - 1 stent migration |
| 2009 | Brauer[26] | 12 (8/4) | 12 EH | 11/12 (92%) - 7 TP - 4 TD | 2 (10%) - 1 pneumoperitoneum and peritonitis - 1 cardiopulmonary failure |
| 2009 | Maranki[25] | 49 (35/14) | 35 IH 14 EH | Overall: 41/49 (84%) | Total: 8 (16%) IH: 5/35 (14%) - pneumoperitoneum (3) - bleeding (1), - pneumonia (1) EH: 3/14 (21%) - bile peritonitis (1) - pain (1) - pneumoperitoneum (1) |
| IH: 29/40 (73%) - 26 TP, 3 TG | |||||
| EH: 12/14 (86%) - 8 TP, 4 TD | |||||
| 2008 | Tarantino[24] | 8 (7/1) | 9 EH | 8/8 (100%) - 4 TP, 4 TD | Not procedure related - 1 death after 15 d (hepatic failure, cirrhosis) |
| 2008 | Yamao[32] | 5 (5/0) | 5 EH | 5/5 (100%) - 5 TD | 1 (20%) - pneumoperitoneum |
| 2008 | Itoi[33] | 4 (4/0) | 4 EH | 4/4 (100%) - 4 TD | 1 (25%) - bleeding and bile peritonitis |
| 2007 | Bories[30] | 11 (8/3) | 11 IH | 10/11 (91%) - 10 TG | 4 (36%) - ileus - early stent occlusion - biloma - cholangitis |
| 2007 | Will[31] | 8 (7/1) | 8 IH | 6/8 (75%) - 1 TE, 4 TG, 3 TJ | 2 (25%) - cholangitis, pain |
| 2005 | Püspök[20] | 6 (4/2) | 5 EH 1 IH | 5/6 (83%) - 3 TB, 1 TD, 1 TJ | 1 (17%) - cholecystitis |
| 2003 | Burmester[15] | 4 (4/0) | 2 EH 2 IH | 3/4 (75%) - 1 TD, 2 TJ, 1 TG | 1 (25%) - cholangitis, sepsis death (failed procedure) |
TG: Transgastric; TD: Transduodenal, TP: Transpapillary; TE: Transesophageal; TJ: Transjejunal; EH: Extrahepatic; IH: Intrahepatic.
Table 3.
Major series on EUS-guided pancreatic duct drainage
| Year | Author | N | Access route | Technical success - Drainage route | Clinical success | Complications |
| 2009 | Brauer[26] | 8 | TG – TD | 7/8 (88%) - 3 TG, 1 TD, 3 TP | 4/8 (50%) | No complications - Pain evaluation: non significant improvement |
| 2007 | Tessier[43] | 36 | 29 TG 7 TD | 33/36 (92%) - 26 TG, 7 TD | 25/36 (69%) | 5 (13%) - 2 severe (5%): hematoma, pancreatitis - 3 mild (8%) |
| Total or significant pain relief | Stent dysfunction: 20 pt (55%) = 29 new endoscopic procedures | |||||
| 2007 | Kahaleh[44] | 13 | 13 TG | 10/13 (77%) - 10 TG | 10/13 (77%) < score pain < pancreatic duct diameter = narcotic use | 2 (15%) - bleeding, perforation |
| 2007 | Will[45] | 12 | 12 TG | 9/12 (75%) - 5 TG, 4 TP | - 5 pt (42%): pain relief, fistula closure - 4 pt: surgery - 3 pt: endoscopy | 6 (43%) - 2 severe (14%): bleeding, perforation - 4 mild (29%): pain |
| 2004 | Mallery[16] | 4 | 4 TG | 1/4 (25%) - TP | 1/4 (25%) | 2 (50%) - mild pancreatitis - fever |
| 2002 | Francoise[12] | 4 | 4 TG | 4/4 (100%) | 3/4 (75%) | No complications |
TG: Transgastric; TD: Transduodenal; TP: Transpapillary.
Most patients drained by ESCP have had malignant biliary obstruction not amenable to standard ERCP palliation[6,38,39]. A minority of those with malignant jaundice has been decompressed preoperatively, and fewer still have had benign disease - stones or strictures. There are two obvious explanations for this. Firstly, severe anatomic distortion (caused by tumor infiltration or by prior pancreaticobiliary/upper GI surgery) is more frequently associated with malignancy, and hence the chances for unsuccessful ERCP are higher. Secondly, surgery may have been preferred as a more definitive salvage therapy after failed ERCP in operative candidates with benign strictures or CBD stones and in situ gallbladders.
General requirements and patient preparation
As mentioned above, the procedure room and assistant expertise requirements are the same as those for ERCP. Although ESCP has occasionally been performed with small channel EUS scopes, large-channel therapeutic echoendoscopes are clearly preferable[37,38]. Similarly, EUS needles of a smaller calibre than 19G represent an unnecessary burden, since the 0.018-inch wires they allow are strongly associated with failed ESCPs, repeat 19G punctures for larger wire passage, and the need for cautery access due to insufficient support for mechanical dilation. The endoscopist’s background expertise must include proficiency in EUS-FNA (preferably with a large 19G needle) and a high-volume ERCP practice. Ideally, before attempting ESCP the endoscopist should have gained some experience with EUS-guided pancreatic pseudocyst drainage. The two procedures are technically related[39] although pseudocyst EUS-guided drainage is less challenging, since its target for drainage is a much larger anatomic structure, usually adherent (by virtue of its inflammatory nature) to the GI wall[40]. Nonetheless, EUS-guided pseudocyst drainage still entails a learning curve, estimated at 25 cases for endosonographers with prior therapeutic ERCP training[41].
Whereas most authors have so far used anesthesia back up, endoscopist-directed propofol sedation has been used by others[38]. Whatever the sedation choice, it is important to remember that standard conscious sedation with midazolam and meperidine may well fall short of the requirements. Minor degrees of patient movement that might not represent a problem during standard ERCP or EUS-FNA, may result in guidewire dislodgment during ESCP and jeopardize the whole procedure since reattempted guide wire access is not as straightforward as in ERCP.
The coagulation status of the patient should be checked, and prophylactic oral or intravenous antibiotics are customarily given. Subcutaneous octeotride is administered by some authors selectively after failed pancreatic duct access[16]. The aim is to minimize pancreatic secretion and prevent retroperitoneal leakeage through the puncture track. Although its efficacy has not been proven, this pharmacologic strategy seems very sensible. The consent process is increasingly being incorporated into the consent for ERCP, especially in cases of anticipated difficulty at centers where ESCP is becoming common. Otherwise, it requires a separate discussion considering alternative drainage options.
CHOICE OF APPROACH AND TIPS ON TECHNIQUE
Choice of access site
There is a choice between intrahepatic or extrahepatic bile duct puncture in about 20% of biliary ESCP patients. For the remaining 80% the EUS access site is determined by the level of obstruction (hilar versus distal), and by the feasibility of imaging the CBD under EUS (difficult to impossible in patients with prior gastrectomy or indwelling duodenal stents) or the intrahepatic bile duct (which needs some degree of dilatation) (Figure 2)[25,37,38]. Similarly, for the pancreatic duct there is limited choice between transgastric access, usually the most straightforward[43,44], and transduodenal (impossible in those with prior pancreatoduodenectomy). To a great extent, this is influenced by the location of the obstruction and the reason for unsuccessful ERCP (cannulation versus access across a duct disruption/stricture), as well as by the intended route for drainage (transpapillary rendezvous versus transmural pancreatigastrostomy).
Figure 2.
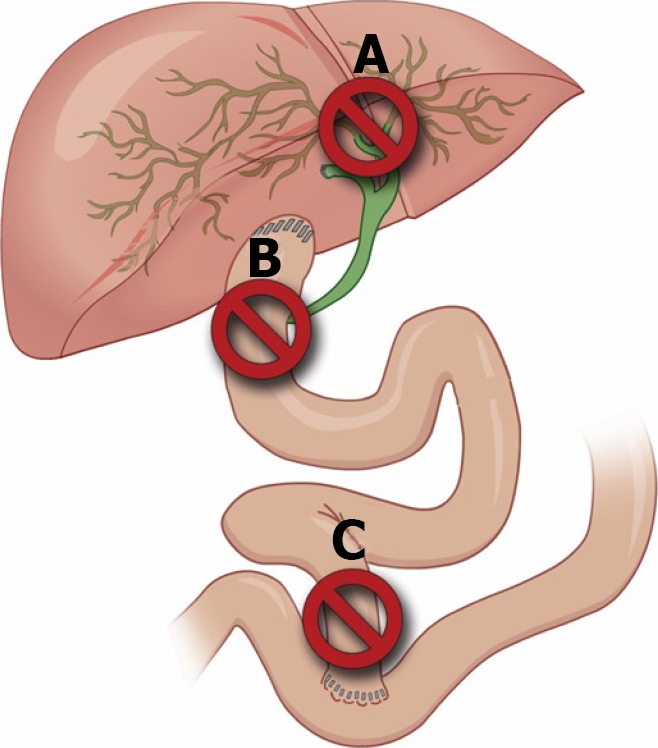
A hilar stricture with dilatation of the left ductal system (A) requires intrahepatic access. Extrahepatic access is suitable for distal biliary obstruction in patients with native antroduodenal anatomy despite the presence of ascites or non-dilated intrahepatic ducts (B). Any prior surgery involving distal gastrectomy with gastrojejunostomy (C) precludes EUS imaging of the CBD. Some of these factors are present in 80% of carefully selected ESCP candidates, which limits the issue of “operator’s choice of approach” to 20% of cases.
Choice of drainage route
The choice between transpapillary and transmural drainage is also determined to some degree by the patient’s anatomy and diagnosis (e.g. CBD stone versus malignant stricture). It is obviously also influenced by the operator’s preference.
Transpapillary drainage: For rendezvous, endoscopic access to the papilla is unanimously considered a pre-requisite[4,16]. For any kind of transpapillary drainage (antegrade or rendezvous) antegrade guidewire passage from the puncture site into the small bowel is usually necessary, requiring a non transected duct. As an exception, successful rendezvous drainage of a transected bile duct overcome with cautery has been reported in a single case[17].
The limiting step for transpapillary drainage is guidewire manipulation[38,39]. A needle does not allow the same free interplay over a guidewire as flexible ERCP catheters do. The needle is rigid and has a sharply cutting edge. If to and fro movements of the needle over the wire are attempted either briskly or repeatedly, the needle may easily puncture its way out of the duct or shear the guidewire and render it useless. Therefore, when aiming for rendezvous, EUS and fluoroscopy should be used to seek an access site as close to the papilla as possible, with a tangential needle orientation to the duct, before the actual puncture[4,16]. Post-puncture repositioning of the echoendoscope may also be possible in cases with a largely dilated duct (e.g. CBD above distal malignancy), although this carries the risk of loosing needle access, associated in turn with the need for re-puncture and with procedural failure. Transpapillary guidewire passage is understandably much more demanding from an intrahepatic than an extrahepatic access site[39]. After extrahepatic access, the guidewire can only go either up or down the CBD. In contrast, after intrahepatic access it may go peripherally to another left branch at every confluence, or to the right lobe ducts at the confluence of the right and left main hepatic ducts. So, transpapillary guidewire passage with intrahepatic ESCP often requires dilation of the puncture track to a degree similar to that required for transmural drainage, in order to allow intraductal passage of catheters or sphincterotomes[21,38]. These more manageable devices help to direct the guidewire effectively towards the CBD and across the stricture and/or papilla, a challenging step in itself. Crossing the papilla (or anastomosis) antegradely with a guidewire often takes repeat needle puncture and reorientation, trying different types of guidewires, or even cautery. Despite all this instrumentation, the process may end up in failure[48]. When guidewire passage across the papilla is nevertheless successful, it is customary to advance into the bowel lumen as many (three or four) loops as possible to prevent dislodgement during antegrade or rendezvous stent placement. For rendezvous, the echoendoscope (with the needle attached) is carefully removed while the assistant feeds the wire into the needle at the same rate that the endoscopist removes the scope-needle assembly[16]. The position of the guidewire is monitored fluoroscopically to prevent both looping in the stomach and dislodgment of the transpapillary looped wire. After EUS scope removal, a duodenoscope is advanced side by side with the guidewire while the assistant holds it under gentle traction from the patient’s mouth, again to prevent looping. Once the papilla is reached with a duodenoscope (or a longer endoscope in some cases with altered anatomy)[48], the transpapillary guidewire can be grasped with a polypectomy snare and retrieved through the working channel while the assistant feeds it into the patient’s mouth in coordination. Standard ERCP devices can then be threaded over the wire once it has exited from the endoscope channel (classic rendezvous)[4]. Alternatively, once the duodenoscope reaches the papilla, a sphincterotome can be used for cannulation alongside the ESCP placed wire (parallel rendezvous)[16,49]. Parallel rendezvous thus saves the cumbersome step of guidewire retrieval through the endoscope. The disadvantage is that dual traction (from the mouth end and from the endoscope end of the wire) is not possible with parallel rendezvous. Dual traction is usually performed with the wire inside a catheter, to prevent so-called “cheese-cutter” injury to the parenchyma. For some of the very tight strictures (hilar bile duct or MPD) typically stented by ESCP, dual traction is a very useful adjunct technique that saves labor-intensive dilation before stenting[38]. Instances of failed transpapillary stenting after a fastidious pancreatic EUS rendezvous which might have been prevented by using dual traction have been reported[26].
Finally, there is a simpler, still relatively overlooked, approach to achieving retrograde transpapillary ductal access by ESCP. In some cases, either free-hand or standard wire-guided cannulation (i.e. no rendezvous) can be achieved despite prior unsuccessful ERCP once the obstructed duct has been injected by ESCP with contrast medium or a mixture of contrast medium and methylene-blue. Contrast injection ESCP has recently been proposed formally[26] - although the technique was described in prior reports[17]. It consists of a “salvage” repeat ERCP after failed ESCP, coming full circle from use of ESCP after failed ERCP. This is rendered possible after ductal injection by a double mechanism: a) making an inconspicuous (e.g. intradiverticular) papilla patulous and thus more evident; and b) providing a “road map” for cannulation. Methylene-blue injection ESCP has been reported for minor papilla cannulation[18] and in related settings with an unidentifiable MPD orifice[50]. The “road map” strategy is accidental (i.e., not the intended initial approach for drainage). There is no reason why it can not be intentionally combined with methylene-blue injection into the bile duct, perhaps thereby increasing its efficacy.
Transmural drainage: For transmural drainage, the limiting step is the creation of a fistulous track between the puncture site on the GI wall and the duct, to allow stent placement (plastic for benign disease and pancreatic ESCP; plastic or metal for malignant biliary ESCP). This requires at least bougie (stepped dilating catheters) or balloon dilation, and sometimes cautery with a needle-knife or a fistulotome. Cautery is felt to pose an increased risk for complications although some authors favor it for transduodenal access to the CBD, particularly when transmural drainage (choledochoduodenostomy) is the final goal[51]. A needle-knife (or fistulotome) is advanced either free-hand or wire-guided into the CBD. In the former case, prior finer (22G) needle ESCP cholangiography may or may not be performed to allow the added benefit of fluoroscopy during access to the CBD (since cautery creates EUS artifacts). In the latter case, ESC is routinely used for intraductal placement of the wire. Since the driving mechanism for fistula formation is cautery (as opposed to mechanical, pushing force), a 0.018-inch or 0.021-inch guidewire is sufficient[24]. Given that 22G needles can take these thiner wires, cautery access obviates the need to use the stiff, larger 19G needles. 19G needles may become cumbersome during transduodenal access, since the echoendoscope is in a longer, looped position compared to intrahepatic access. Whatever the modality, cautery access avoids the somewhat awkward transition from the rigid, sharp needle to the flexible ERCP catheters and dilators, while at the same time providing an initial step for fistula formation. Whereas cautery may be necessary in some select instances for access (e.g. a hardened fibrotic parenchyma), it is probably best avoided[47]. In order to create a tract without cautery, using only mechanical dilation, it is important to maintain the endosonographic plane of view[34,47]. This is a technical tip whose implications have not yet been fully spelled out. The EUS plane is easily lost if the operator shifts from US monitoring of ductal access to endoscopic control once the guidewire is inside the duct, as one would do for transgastric pseudocyst drainage with the classic “blind” (i.e. no EUS guidance) approach. In other words, to keep the US plane and guidewire axis of approach, the echoendoscope tip must remain throughout the processes of fistula track dilation and stent insertion in the same position where it was when the needle first punctured the duct. If this technique is carefully adhered to, only a minority of patients will fail mechanical track dilation and require additional cautery access with an over-the-wire device, be it a needle-knife or a fistulotome[34]. This concept does take, however, some effort on the part of the operator, as there is a deep-seated therapeutic endoscopy impulse to keep in endoscopic view a guidewire over which a device or stent is being advanced. This impulse should be deliberately ignored and re-educated towards EUS monitoring. Only for the final step of stent deployment is the echoendoscope slightly withdrawn to gain an endoscopic view[38]. This allows endoscopic control of the deployment of the intraluminal end of the transmural stent, a step that requires greater care than stent deployment at ERCP. The EUS scope is gently removed (approximately 2-3 cm) by an assistant carefully coordinated with the endoscopist, who is simultaneously advancing the stent-delivery catheter under fluoroscopy and endoscopy, so as to maintain the half-deployed stent at the exact (fluoroscopic) point inside the duct where it was before scope withdrawal began. The intraluminal (GI) end of a transmural metal stent should be at least 2 cm in length, much longer than in standard transpapillary placement at ERCP. This is a critical point, since metal stents foreshorten (up to 30% in some cases) upon full expansion, which takes hours. If the intraluminal segment is shorter than 2 cm, the stent may easily foreshorten towards the duct beyond the GI wall, resulting in free intra- or retro-peritoneal leakage hours to days after placement[30,38]. Another option is to use forced balloon expansion immediately following initial placement and thus control the otherwise blind process of stent expansion. If after forceful balloon expansion the intraluminal stent end looks too close to the GI wall, an overlapping second metal stent can be placed inside the first one more proximally (towards the EUS scope). A simple additional anchoring technique is to place a 7F double pig-tail inside the metal stent as a safeguard against both postprocedure dislocation and late migration. Adequate traction of the guidewire is needed as the first (biliary) pig-tail goes through the metal stent to prevent its tip impacting against the struts. The nuances of metal stent expansion and foreshortening. the actual distance between the US transducer and the echoendoscope lens, and the potential for the virtual space between the GI wall and the target duct becoming a real space, explain why despite ductal access distances measuring less than 2 cm, metal stents of 6 cm or longer should be used. Shorter metal stents, despite looking adequate immediately after initial “self-expanding” (i.e. non balloon expanded) deployment, may easily result in dislocation (foreshortening and/or migration) after the procedure. When these tedious technical tips are observed, transmural metal stenting provides immediate large-caliber drainage, with the added bonus of a much more effective sealing of the fistulous track than plastic stents[34].
In summary, there are two factors in choosing an approach, patient-related and operator technique-related. The former cannot be altered in a given case other than by abandoning the procedure (i.e. considering ESCP a failure if transpapillary guide wire passage is unsuccessful and rendezvous the only approach considered) and opting for alternative therapies. Technique and operator skill can evolve and improve with practice. Whereas some authors stick to a single approach, such as rendezvous-drainage-only or transduodenal-access-only, those with a modus operandi which includes alternative approaches, may be able to salvage a greater proportion of failed ERCPs by means of ESCP.
ESCP: STEP BY STEP PROCEDURE
Location of entry point
Bearing in mind the patient’s anatomy (level of obstruction and type of prior surgeries if any), the closest dilated segment of duct at a position where the echoendoscope is stable and without intervening vessels is sought. These can be readily identified with color Doppler-[37,38]. After a general EUS overview to confirm known patient specifics from prior imaging and to locate the access area, it is useful to have the needle already inside the echoendoscope working channel before focusing on the exact entry point. The preferred 19G needles are stiff and tend to change the position of the echoendoscope tip by a small but significant amount once they are in the working channel. The more obvious the dilatation and the closer the duct is to the echoendoscope, the greater the chances of success. Although ducts as small as 2 mm in diameter have been successfully accessed by ESCP, a minimum size of 4-5 mm within 15-20 mm range of the transducer is more typically associated with success. As stated above, if rendezvous is intended, a puncture site as close as possible to the papilla, and a needle axis tangential to the projected duct course, pointing the needle tip antegradely, is sought by repositioning the echoendoscope under fluoroscopy. This is easier said than done. Despite claims that this was the chosen technique, ductograms published in some reports often show a fairly perpendicular entry angle between the needle and the duct, particulary for transduodenal CBD access[38,41]. This is a telltale sign of the serendipitous factor in rendezvous despite posthoc rationalization.
Puncture and ductography
When the optimal access point has been identified, the needle is advanced into the duct. Once puncture begins, the procedure takes on a rapid pace and no time should be wasted. The lesser the manipulation, the smaller the chance of incurring bile leakage, extraductal needle passage, guidewire dislodgment from the duct or any other potential mishaps. It is advisable that the assistant has all the devices (guidewires, catheters, dilators, stents) ready at hand before puncture. Similarly, fluoroscopy is focused on the echoendoscope and needle tip, to avoid having to move the fluoroscopy table or adjust the zoom once the needle is inside the duct. With current generation EUS needles, removing the stylet does not compromise the ability to puncture a small target. So, it is useful to do this beforehand. Some authors even preflush the needle with contrast medium through a side adaptor and have the guidewire in place[16]. However, having a guidewire in place does not allow aspiration through the needle. Aspiration is a very useful way to have confirmation of ductal access, particularly when smaller calibre ducts (e.g. MPD, intrahepatics) are targeted. In these cases, despite an intraductal ultrasound appearance, the needle might be on a different plane. If aspiration is skipped before injecting there is small but definite risk of intraparenchymal injection. A hyperechoic cloud will then appear, preventing needle access at the selected (optimal) entry point, and thus greatly compromising success. A bloody return may be obtained during intrahepatic access. It is important not to mistake very dark colored bile for blood. Adequate visual inspection of the aspirate in the syringe may require turning the procedure room lights on. If there is no fluid return, or it is clearly blood, the needle is slightly repositioned (back or forth), or a new needle pass made. After an inadvertent vessel puncture and aspiration of blood, it is advisable to flush the needle with saline into the GI lumen, or the aspirate will clog it. Secondary benefits of fluid aspiration before injection are decreasing intraductal pressure (which might help decrease the risk of leakage) and allowing microbiological sampling (which may be useful to guide antibiotic coverage). After a fluid (bile or pancreatic juice) return, contrast medium is gently injected until the targeted duct is outlined. A complete ductogram is usually not necessary (unless a methylene-blue-like ESCP approach is intended).
Initial guidewire placement
A 0.035-inch guidewire is advanced by the assistant while the endoscopist keeps the needle still (coupled to the patient’s respiratory motion) to prevent damage to the guidewire. The restrictions to maneuvering a wire within a needle have been described above. Greater care is needed in smaller calibre ducts, where the needle tip abuts the duct wall more easily than in the CBD. If the targeted duct is small, and the initial length of wire inside the duct is too short or markedly unsatisfactory (e.g. goes towards the more peripheral bile duct), a very cautious attempt at guidewire repositioning from the same puncture site can be made. The wire can be pulled back inside the needle, asking the assistant to stop the backward wire movement if any resistance is met. Once the guidewire is back inside the needle, it may be removed and replaced for a different one (e.g. 0.025-inch wire, Terumo-coated, or angled-tip). Alternatively, insertion of the same wire into the duct may be tried again after changing slightly the angle of the needle tip and, more importantly, the speed with which the assistant feeds the wire into the needle. These are virtually the only adjustments afforded by the needle-wire assembly. Further advancement of the needle over the wire (as one might try with a flexible ERCP device) to change the angle of approach, or forceful removal of the wire through the needle, are strongly discouraged. The opportunity for repeat ductal puncture is limited, particularly after contrast medium has been injected. Again, this limitation is maximal for the intrahepatic access, where small ducts collapse upon the initial puncture and the ultrasound window is quickly lost by contrast extravasation. At the other end of the spectrum, the CBD may be more forgiving to repeat punctures during the same procedure. If at this point in the procedure the guidewire crosses the ductal stricture and the papilla, transpapillary drainage can be carried out via rendezvous ERCP in those patients with endoscopically accessible papillae, or antegradelly in those without. However, transpapillary guidewire placement often requires manipulation with a flexible catheter, particularly in the presence of a very tight distal stricture with a massively dilated bile duct above, where the guidewire tends to coil back. The next common procedural step to most ESCPs is thus ductal access over the wire with a flexible catheter (cannula, dilator, sphincterotome, needle-knife or fistulotome).
Guidewire manipulation and fistulous track formation
This is the key step in which the final approach to be used is defined (transpapillary/transmural) and which determines whether the procedure is more likely to result in success or failure. It is a truly defining step, characterized by the transition from rigid and cutting (EUS needles) to flexible (ERCP devices). The bulk of the instrumentation is carried out under fluoroscopy. However, it is crucial to maintain both the ultrasound plane and the guidewire axis throughout. As the endoscopist is looking at fluoroscopy, an assistant at the patient’s head holds the echoendoscope in place while watching the ultrasound monitor. If at any point the assistant looses the ultrasound view of the guidewire, he or she warns the endoscopist of this, so that the wire is brought back into view by slight scope repositioning before attempting any further instrumentation. A single ERCP stepped dilating catheter (5 or 6 Fr), followed by a 4-6 mm biliary balloon dilator affords transmural insertion of a metal stent, which can be passed through the echoendoscope working channel. The flexible over-the-wire device may bounce off the GI wall or (more typically) CBD wall/parenchyma, as it lacks the stiffness and cutting tip of a needle, and the support provided by the guidewire is often insufficient. Sticking to fluoroscopy and EUS monitoring only (i.e. no endoscopic view) is, as stated above, crucial at this stage. The tip of the echoendoscope pressing the GI wall serves the double purpose of preserving the access axis and preventing the creation of a space between the CBD, liver or pancreas and the GI wall (which risks extraluminal guidewire looping), or between the EUS scope and the GI wall (risking intraluminal looping). This is just as gastric distention is maintained throughout percutaneous puncture during a percutaneous endoscopic gastrostomy procedure to prevent the separation between the gastric and abdominal walls. To enhance dilation in difficult cases, the endoscopist may resort to a stiffer flexible device and/or try to enhance the coordination with their assistants in a carefully choreographed swift, hard pushing motion. At the count of three, the assistant at the patient’s head holds firm inward pressure on the EUS scope shaft, and the second assistant applies maximal traction on the wire (short of ductal dislodgment), while the endoscopist pushes forward the dilating device in a whipping stroke. This can be repeated, taking care to prevent looping at any point (which invariably results in guidewire dislodgment and seriously compromises success) until a yield is felt, and the intraductal position of the dilating device is confirmed by fluoroscopy. If mechanical dilation over the wire nevertheless fails, a needle-knife can be threaded over it, and cautery applied when resistance to advancement is met. It is important that the full length of the needle-knife cutting-wire is not exposed, because it may then bend at a 90º angle and cut through the walls sideways. A more ad hoc device for cautery access is a 6.5Fr wire-guided fistulotome, used for transmural pseudocyst drainage. The cutting piece is a metal cone at the tip and its body firmer than the body of a needle-knife catheter. Once the puncture track has been enlarged by whatever means, a sphincterotome, balloon catheter or any other ERCP device can be advanced into the duct and be used to attempt guidewire passage across the papilla.
Stent insertion and deployment
A stent is advanced over the wire under fluoroscopy (the EUS plane kept in sight by the assistant) through the echoendoscope for both transmural and transpapillary antegrade drainage. The transmural insertion technique has been described above. For antegrade insertion, only fluoroscopic monitoring (as in percutaneous stent insertion) is used. For retrograde stent insertion, rendezvous ERCP is performed as detailed earlier. It is also possible to perform rendezvous with the echoendoscope itself, although it is unclear if this approach is reproducible or less cumbersome than the scope exchange it saves. As it is standard for ERCP drainage, plastic stents are used in benign disease. A 7F calibre is much more manageable through the echoendoscope (especially with a pig-tail design) than the customary 10F which is also possible. Metal stents, partially or fully covered if transmural, are preferred for malignant disease. An initial plastic stent may be exchanged over-the-wire at a follow-up session for a metal one, using a duodenoscope. Free-hand plastic stent removal may result in fistula track disruption when re-attempting guidewire duct access. The longer and curved position of the echoendoscope inherent to the transduodenal access route makes plastic stents easier to insert than the stiffer delivery systems for metal stents. On the other hand, their stiff delivery systems make metal stents better suited for the intrahepatic approach.
CONCLUSION
ESCP is a relatively novel technique that allows biliary and pancreatic duct drainage in a very select patient subset in which this cannot be accomplished by ERCP. ESCP is a hybrid technique requiring expertise in both EUS-FNA and therapeutic ERCP. It has matured over the last decade and is nowadays increasingly replacing PTC in the palliation of malignant obstructive jaundice after failed ERCP. Its role in managing anatomically complex chronic/relapsing pancreatitis is less well defined, but is based on the same technical grounds as biliary ESCP and the same clinical grounds as pancreatic ERCP. The many possible variant ESCP approaches are largely determined by patients’ anatomy and, to a lesser degree, by operator preference. Careful planning and attention to minute details concerning needles, guidewires, dilators and stents are advisable before every case. High expectations are placed on the development of newer devices that may potentially simplify ESCP in the future. This should not obscure the fact that ESCP has a significant learning curve, failure and complication rates. However, ESCP successfully provides adequate therapy to very challenging patients in a minimally invasive fashion, and its use is expected to grow in clinical practice with the increasing availability of trained operators in both EUS and ERCP.
Footnotes
Peer reviewer: Ka-Ho Lok, MBChB, Associate Consultant, Department of Medicine and Geriatrics, Tuen Mun Hospital, Tsing Chung Koon Road, Tuen Mun, Hong Kong, China
S- Editor Zhang HN L- Editor Hughes D E- Editor Liu N
References
- 1.Colton JB, Curran CC. Quality indicators, including complications, of ERCP in a community setting: a prospective study. Gastrointest Endosc. 2009;70:457–467. doi: 10.1016/j.gie.2008.11.022. [DOI] [PubMed] [Google Scholar]
- 2.Mutignani M, Tringali A, Shah SG, Perri V, Familiari P, Iacopini F, Spada C, Costamagna G. Combined endoscopic stent insertion in malignant biliary and duodenal obstruction. Endoscopy. 2007;39:440–447. doi: 10.1055/s-2007-966327. [DOI] [PubMed] [Google Scholar]
- 3.Paik WH, Park YS, Hwang JH, Lee SH, Yoon CJ, Kang SG, Lee JK, Ryu JK, Kim YT, Yoon YB. Palliative treatment with self-expandable metallic stents in patients with advanced type III or IV hilar cholangiocarcinoma: a percutaneous versus endoscopic approach. Gastrointest Endosc. 2009;69:55–62. doi: 10.1016/j.gie.2008.04.005. [DOI] [PubMed] [Google Scholar]
- 4.Gupta K, Mallery S, Hunter D, Freeman ML. Endoscopic ultrasound and percutaneous access for endoscopic biliary and pancreatic drainage after initially failed ERCP. Rev Gastroenterol Disord. 2007;7:22–37. [PubMed] [Google Scholar]
- 5.Wiersema MJ, Sandusky D, Carr R, Wiersema LM, Erdel WC, Frederick PK. Endosonography-guided cholangiopancreatography. Gastrointest Endosc. 1996;43:102–106. doi: 10.1016/s0016-5107(06)80108-2. [DOI] [PubMed] [Google Scholar]
- 6.Fujita N, Noda Y, Kobayashi G, Ito K, Horaguchi J, Takasawa O, Nakahara K. Endosonography-guided biliary drainage. Dig Endosc. 2008;20:55–60. [Google Scholar]
- 7.Koito K, Nagakawa T, Murashima Y, Suga T, Yaosaka T, Imamura A, Fujinaga A, Miyakawa H, Tochihara M, Higashino K. Endoscopic ultrasonographic-guided punctured pancreatic ductography: an initial and successful trial. Abdom Imaging. 1995;20:222–224. doi: 10.1007/BF00200400. [DOI] [PubMed] [Google Scholar]
- 8.Harada N, Kouzu T, Arima M, Asano T, Kikuchi T, Isono K. Endoscopic ultrasound-guided pancreatography: a case report. Endoscopy. 1995;27:612–615. doi: 10.1055/s-2007-1005769. [DOI] [PubMed] [Google Scholar]
- 9.Gress F, Ikenberry S, Sherman S, Lehman G. Endoscopic ultrasound-directed pancreatography. Gastrointest Endosc. 1996;44:736–739. doi: 10.1016/s0016-5107(96)70064-0. [DOI] [PubMed] [Google Scholar]
- 10.Giovannini M, Moutardier V, Pesenti C, Bories E, Lelong B, Delpero JR. Endoscopic ultrasound-guided bilioduodenal anastomosis: a new technique for biliary drainage. Endoscopy. 2001;33:898–900. doi: 10.1055/s-2001-17324. [DOI] [PubMed] [Google Scholar]
- 11.Bataille L, Deprez P. A new application for therapeutic EUS: main pancreatic duct drainage with a “pancreatic rendezvous technique”. Gastrointest Endosc. 2002;55:740–743. doi: 10.1067/mge.2002.123621. [DOI] [PubMed] [Google Scholar]
- 12.François E, Kahaleh M, Giovannini M, Matos C, Devière J. EUS-guided pancreaticogastrostomy. Gastrointest Endosc. 2002;56:128–133. doi: 10.1067/mge.2002.125547. [DOI] [PubMed] [Google Scholar]
- 13.Kahaleh M, Yoshida C, Yeaton P. EUS antegrade pancreatography with gastropancreatic duct stent placement: review of two cases. Gastrointest Endosc. 2003;58:919–923. doi: 10.1016/s0016-5107(03)02297-1. [DOI] [PubMed] [Google Scholar]
- 14.Giovannini M, Dotti M, Bories E, Moutardier V, Pesenti C, Danisi C, Delpero JR. Hepaticogastrostomy by echo-endoscopy as a palliative treatment in a patient with metastatic biliary obstruction. Endoscopy. 2003;35:1076–1078. doi: 10.1055/s-2003-44596. [DOI] [PubMed] [Google Scholar]
- 15.Burmester E, Niehaus J, Leineweber T, Huetteroth T. EUS-cholangio-drainage of the bile duct: report of 4 cases. Gastrointest Endosc. 2003;57:246–251. doi: 10.1067/mge.2003.85. [DOI] [PubMed] [Google Scholar]
- 16.Mallery S, Matlock J, Freeman ML. EUS-guided rendezvous drainage of obstructed biliary and pancreatic ducts: reports of 6 cases. Gastrointest Endosc. 2004;59:100–107. doi: 10.1016/s0016-5107(03)02300-9. [DOI] [PubMed] [Google Scholar]
- 17.Kahaleh M, Yoshida C, Kane L, Yeaton P, Interventional EUS cholangiography: a report of five cases. Gastrointest Endosc. 2004;60:138–142. doi: 10.1016/s0016-5107(04)01528-7. [DOI] [PubMed] [Google Scholar]
- 18.Dewitt J, McHenry L, Fogel E, Leblanc J, McGreevy K, Sherman S. EUS-guided methylene blue pancreatography for minor papilla localization after unsuccessful ERCP. Gastrointest Endosc. 2004;59:133–136. doi: 10.1016/s0016-5107(03)02278-8. [DOI] [PubMed] [Google Scholar]
- 19.Lai R, Freeman ML. Endoscopic ultrasound-guided bile duct access for rendezvous ERCP drainage in the setting of intradiverticular papilla. Endoscopy. 2005;37:487–489. doi: 10.1055/s-2005-861250. [DOI] [PubMed] [Google Scholar]
- 20.Püspök A, Lomoschitz F, Dejaco C, Hejna M, Sautner T, Gangl A. Endoscopic ultrasound guided therapy of benign and malignant biliary obstruction: a case series. Am J Gastroenterol. 2005;100:1743–1747. doi: 10.1111/j.1572-0241.2005.41806.x. [DOI] [PubMed] [Google Scholar]
- 21.Kahaleh M, Wang P, Shami VM, Tokar J, Yeaton P. EUS-guided transhepatic cholangiography: a report of 6 cases. Gastrointest Endosc. 2005;61:307–313. doi: 10.1016/s0016-5107(04)02585-4. [DOI] [PubMed] [Google Scholar]
- 22.Will U, Meyer F, Manger T, Wanzar I. Endoscopic ultrasound-assisted rendezvous maneuver to achieve pancreatic duct drainage in obstructive chronic pancreatitis. Endoscopy. 2005;37:171–173. doi: 10.1055/s-2004-826151. [DOI] [PubMed] [Google Scholar]
- 23.Kahaleh M, Hernandez AJ, Tokar J, Adams RB, Shami VM, Yeaton P. Interventional EUS-guided cholangiography: evaluation of a technique in evolution. Gastrointest Endosc. 2006;64:52–59. doi: 10.1016/j.gie.2006.01.063. [DOI] [PubMed] [Google Scholar]
- 24.Tarantino I, Barresi L, Repici A, Traina M. EUS-guided biliary drainage: a case series. Endoscopy. 2008;40:336–339. doi: 10.1055/s-2007-995455. [DOI] [PubMed] [Google Scholar]
- 25.Maranki J, Hernandez AJ, Arslan B, Jaffan AA, Angle JF, Shami VM, Kahaleh M. Interventional endoscopic ultrasound-guided cholangiography: long-term experience of an emerging alternative to percutaneous transhepatic cholangiography. Endoscopy. 2009;41:532–538. doi: 10.1055/s-0029-1214712. [DOI] [PubMed] [Google Scholar]
- 26.Brauer BC, Chen YK, Fukami N, Shah RJ. Single-operator EUS-guided cholangiopancreatography for difficult pancreaticobiliary access (with video) Gastrointest Endosc. 2009;70:471–479. doi: 10.1016/j.gie.2008.12.233. [DOI] [PubMed] [Google Scholar]
- 27.Yamao K, Sawaki A, Takahashi K, Imaoka H, Ashida R, Mizuno N. EUS-guided choledochoduodenostomy for palliative biliary drainage in case of papillary obstruction: report of 2 cases. Gastrointest Endosc. 2006;64:663–667. doi: 10.1016/j.gie.2006.07.003. [DOI] [PubMed] [Google Scholar]
- 28.Ang TL, Teo EK, Fock KM. EUS-guided transduodenal biliary drainage in unresectable pancreatic cancer with obstructive jaundice. JOP. 2007;8:438–443. [PubMed] [Google Scholar]
- 29.Artifon EL, Chaves DM, Ishioka S, Souza TF, Matuguma SE, Sakai P. Echoguided hepatico-gastrostomy: a case report. Clinics (Sao Paulo) 2007;62:799–802. doi: 10.1590/s1807-59322007000600023. [DOI] [PubMed] [Google Scholar]
- 30.Bories E, Pesenti C, Caillol F, Lopes C, Giovannini M. Transgastric endoscopic ultrasonography-guided biliary drainage: results of a pilot study. Endoscopy. 2007;39:287–291. doi: 10.1055/s-2007-966212. [DOI] [PubMed] [Google Scholar]
- 31.Will U, Thieme A, Fueldner F, Gerlach R, Wanzar I, Meyer F. Treatment of biliary obstruction in selected patients by endoscopic ultrasonography (EUS)-guided transluminal biliary drainage. Endoscopy. 2007;39:292–295. doi: 10.1055/s-2007-966215. [DOI] [PubMed] [Google Scholar]
- 32.Yamao K, Bhatia V, Mizuno N, Sawaki A, Ishikawa H, Tajika M, Hoki N, Shimizu Y, Ashida R, Fukami N. EUS-guided choledochoduodenostomy for palliative biliary drainage in patients with malignant biliary obstruction: results of long-term follow-up. Endoscopy. 2008;40:340–342. doi: 10.1055/s-2007-995485. [DOI] [PubMed] [Google Scholar]
- 33.Itoi T, Itokawa F, Sofuni A, Kurihara T, Tsuchiya T, Ishii K, Tsuji S, Ikeuchi N, Moriyasu F. Endoscopic ultrasound-guided choledochoduodenostomy in patients with failed endoscopic retrograde cholangiopancreatography. World J Gastroenterol. 2008;14:6078–6082. doi: 10.3748/wjg.14.6078. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Park do H, Koo JE, Oh J, Lee YH, Moon SH, Lee SS, Seo DW, Lee SK, Kim MH. EUS-guided biliary drainage with one-step placement of a fully covered metal stent for malignant biliary obstruction: a prospective feasibility study. Am J Gastroenterol. 2009;104:2168–2174. doi: 10.1038/ajg.2009.254. [DOI] [PubMed] [Google Scholar]
- 35.Horaguchi J, Fujita N, Noda Y, Kobayashi G, Ito K, Obana T, Takasawa O, Koshita S, Kanno Y. Endosonography-guided biliary drainage in cases with difficult transpapillary endoscopic biliary drainage. Dig Endosc. 2009;21:239–244. doi: 10.1111/j.1443-1661.2009.00899.x. [DOI] [PubMed] [Google Scholar]
- 36.Sawhney R, Speer T. Patients with a high probability of choledocholithiasis are best managed with ERCP without EUS. Gastrointest Endosc. 2009;69:982–983. doi: 10.1016/j.gie.2008.07.048. [DOI] [PubMed] [Google Scholar]
- 37.Shami VM, Kahaleh M. Endoscopic ultrasonography (EUS)-guided access and therapy of pancreatico-biliary disorders: EUS-guided cholangio and pancreatic drainage. Gastrointest Endosc Clin N Am. 2007;17:581–593, vii-viii. doi: 10.1016/j.giec.2007.05.015. [DOI] [PubMed] [Google Scholar]
- 38.Will U, Meyer F. Endoscopic ultrasound-guided cholangiodrainage. In: Mönkemüller K, Wilcox CM, Muñoz-Navas M, editors. Interventional and Therapeutic Gastrointestinal Endoscopy. Front Gastrointest Res. Basel, Karger; 2010. pp. 522–535. [Google Scholar]
- 39.Savides TJ, Varadarajulu S, Palazzo L. EUS 2008 Working Group document: evaluation of EUS-guided hepaticogastrostomy. Gastrointest Endosc. 2009;69:S3–S7. doi: 10.1016/j.gie.2008.10.060. [DOI] [PubMed] [Google Scholar]
- 40.Mangiavillano B, Arcidiacono PG, Carrara S, Masci E, Testoni PA. EUS-guided rendezvous technique for difficult cannulation of an intradiverticular papilla. Endoscopy. 2008;40 Suppl 2:E87–E88. doi: 10.1055/s-2007-995548. [DOI] [PubMed] [Google Scholar]
- 41.Larghi A, Lecca PG, Mutignani M, Costamagna G. EUS-directed transpapillary self-expandable metallic stent placement after successful interventional EUS-guided cholangiography. Gastrointest Endosc. 2008;67:996–998. doi: 10.1016/j.gie.2007.10.004. [DOI] [PubMed] [Google Scholar]
- 42.Fujita N, Sugawara T, Noda Y, Kobayashi G, Ito K, Obana T, Horaguchi J, Takasawa O. Snare-over-the-wire technique for safe exchange of a stent following endosonography-guided biliary drainage. Dig Endosc. 2009;21:48–52. doi: 10.1111/j.1443-1661.2008.00821.x. [DOI] [PubMed] [Google Scholar]
- 43.Tessier G, Bories E, Arvanitakis M, Hittelet A, Pesenti C, Le Moine O, Giovannini M, Devière J. EUS-guided pancreatogastrostomy and pancreatobulbostomy for the treatment of pain in patients with pancreatic ductal dilatation inaccessible for transpapillary endoscopic therapy. Gastrointest Endosc. 2007;65:233–241. doi: 10.1016/j.gie.2006.06.029. [DOI] [PubMed] [Google Scholar]
- 44.Kahaleh M, Hernandez AJ, Tokar J, Adams RB, Shami VM, Yeaton P. EUS-guided pancreaticogastrostomy: analysis of its efficacy to drain inaccessible pancreatic ducts. Gastrointest Endosc. 2007;65:224–230. doi: 10.1016/j.gie.2006.05.008. [DOI] [PubMed] [Google Scholar]
- 45.Will U, Fueldner F, Thieme AK, Goldmann B, Gerlach R, Wanzar I, Meyer F. Transgastric pancreatography and EUS-guided drainage of the pancreatic duct. J Hepatobiliary Pancreat Surg. 2007;14:377–382. doi: 10.1007/s00534-006-1139-8. [DOI] [PubMed] [Google Scholar]
- 46.Săftoiu A, Dumitrescu D, Stoica M, Gheonea DI, Ciurea T, Georgescu A, Andrei E. EUS-assisted rendezvous stenting of the pancreatic duct for chronic calcifying pancreatitis with multiple pseudocysts. Pancreatology. 2007;7:74–79. doi: 10.1159/000101881. [DOI] [PubMed] [Google Scholar]
- 47.Varadarajulu S, Tamhane A, Blakely J. Graded dilation technique for EUS-guided drainage of peripancreatic fluid collections: an assessment of outcomes and complications and technical proficiency (with video) Gastrointest Endosc. 2008;68:656–666. doi: 10.1016/j.gie.2008.03.1091. [DOI] [PubMed] [Google Scholar]
- 48.Kinney TP, Li R, Gupta K, Mallery S, Hunter D, Jensen E, Vickers S, Freeman ML. Therapeutic pancreatic endoscopy after Whipple resection requires rendezvous access. Endoscopy. 2009;41:898–901. doi: 10.1055/s-0029-1215081. [DOI] [PubMed] [Google Scholar]
- 49.Dickey W. Parallel cannulation technique at ERCP rendezvous. Gastrointest Endosc. 2006;63:686–687. doi: 10.1016/j.gie.2005.10.029. [DOI] [PubMed] [Google Scholar]
- 50.Barkay O, Sherman S, McHenry L, Yoo BM, Fogel EL, Watkins JL, Sherman S, DeWitt J, Al-Haddad MA, Lehman GA. Therapeutic EUS-assisted endoscopic retrograde pancreatography after failed pancreatic duct cannulation at ERCP. Gastrointest Endosc. 2010;71:1166–1173. doi: 10.1016/j.gie.2009.10.048. [DOI] [PubMed] [Google Scholar]
- 51.Yamao K. EUS-guided choledochoduodenostomy. Gastrointest Endosc. 2009;69:S194–S199. doi: 10.1016/j.gie.2008.12.028. [DOI] [PubMed] [Google Scholar]