

Abstract
Perioperative intraperitoneal chemotherapy in combination with cytoreductive surgery has been shown to be of benefit for treating selected patients with peritoneal surface malignancy. It has become a new standard of care in the management of diffuse malignant peritoneal mesothelioma and peritoneal dissemination of appendiceal malignancy. Numerous recent publications on carcinomatosis from colorectal cancer and gastric cancer identify groups of patients that would benefit from this local-regional approach for prevention and treatment of carcinomatosis. This review focuses on pharmacological information regarding intraperitoneal chemotherapeutic agents commonly used in gastrointestinal oncology.
Keywords: Intraperitoneal chemotherapy, Mitomycin C, Doxorubicin, Cisplatin 5-fluorouracil, Paclitaxel, Peritoneal surface
INTRODUCTION
In the past, pseudomyxoma peritonei, diffuse malignant peritoneal mesothelioma and peritoneal carcinomatosis from gastrointestinal cancer were considered lethal conditions without curative treatment options. Over the last two decades, multi-modality treatments have evolved. Increasing utilization of cytoreductive surgery combined with intraperitoneal chemotherapy as a treatment strategy for the management of peritoneal dissemination of these malignancies has been regularly reported[1-15]. Benefits have been universally documented in phase II studies. However, as of this point in time, a uniformity of the management for prevention or treatment of peritoneal surface malignancy using perioperative intraperitoneal chemotherapy has not been reached (Table 1). This review focuses on the pharmacological information available for intraperitoneal chemotherapeutic regimens.
Table 1.
Major series on IPHC and/or EPIC after cytoreductive surgery for PMP, DMPM, and CRPC
| Chief investigator | Year | Treatment center | Type | n | Intraperitoneal chemotherapy |
Survival (%) |
|
| 3-yr | 5-yr | ||||||
| Piso et al[1] | 2001 | Hanover, Germany | PMP | 17 | IPHC: cisplatin | 75 | - |
| Butterworth et al[2] | 2002 | Vancouver, Canada | PMP | 11 | EPIC: 5-FU + mitomycin | 60 | - |
| Witkamp et al[3] | 2001 | Amsterdam, Netherlands | PMP | 46 | IPHC: mitomycin | 81 | - |
| Sugarbaker et al[4] | 2001 | Washington, USA | PMP | 501 | EPIC: 5-FU + mitomycin | - | 80 |
| IPHC: mitomycin | |||||||
| Loggie et al[5] | 2001 | Winston-Salem, USA | DMPM | 12 | IPHC: mitomycin | 50 | - |
| Sebbag et al[6] | 2000 | Washington, USA | DMPM | 33 | IPHC: cisplatin + doxorubicin | 56 | 47 |
| Sugarbaker et al[7] | 2003 | Washington, USA | DMPM | 68 | IPHC: cisplatin + doxorubicin | 60 | 50 |
| EPIC: paclitaxel | |||||||
| Feldman et al[8] | 2003 | Bethesda, USA | DMPM | 49 | IPHC: cisplatin ± paclitaxel | - | 59 |
| Fujimura et al[9] | 1999 | Kanazawa, Japan | CRPC | 14 | IPHC: cisplatin + mitomycin + etoposide | 21 | - |
| Witkamp et al[10] | 2001 | Amsterdam, Netherlands | CRPC | 29 | IPHC: mitomycin | 23 | - |
| Elias et al[11] | 2001 | Villejuif, France | CRPC | 64 | IPHC: mitomycin ± cisplatin | 47 | 27 |
| EPIC: mitomycin + 5-FU | |||||||
| Pestieau et al[12] | 2000 | Washington, USA | CRPC | 104 | IPHC: mitomycin | 45 | 30 |
| EPIC: 5-FU | |||||||
| Zoetmulder et al[13] | 2002 | Amsterdam, Netherlands | CRPC | 94 | IPHC: mitomycin | - | 30 |
| Shen et al[14] | 2004 | Winston-Salem, USA | CRPC | 77 | IPHC: mitomycin | 25 | 17 |
| Glehen et al[15] | 2004 | Multi-institutions | CRPC | 506 | IPHC or EPIC | - | - |
IPHC: Intraperitoneal hyperthermic chemotherapy; EPIC: Early postoperative intraperitoneal chemotherapy; PMP: Pseudo-myxoma peritonei; DMPM: Diffuse malignant peritoneal mesothelioma; CRPC: Colo-rectal peritoneal carcinomatosis.
Both pseudomyxoma peritonei and diffuse malignant peritoneal mesothelioma tend to remain localized within the abdominopelvic cavities and extraperitoneal metastasis is rarely seen. Pseudomyxoma peritonei is characterized by abundant mucinous tumor masses combined with copious mucus ascites. The cancer cells accumulate at non-mobile anatomic sites or gravity dependent areas. In contrast, the surfaces of the small bowel and its mesentery may remain free of disease[16]. Diffuse malignant peritoneal mesothelioma arises from the serosal lining of the abdominal cavity[7]. It is characterized by a diffuse pattern of tumor nodules throughout the peritoneal cavity.
Peritoneal implants are present in 10% of patients with colorectal cancer at the time of diagnosis[17]. Isolated peritoneal carcinomatosis of colorectal cancer is a result of transcoelomic dissemination. The cancer cells penetrate through the full thickness of the colonic bowel wall, gain access to the peritoneal space, implant and grow on the peritoneum. Peritoneal involvement tends to be more extensive immediately surrounding the primary tumor.
Sugarbaker described the concept of “tumor cell entrapment”. In this hypothesis, cancer cells gain access to the peritoneal cavity as a result of surgical trauma to a cancer specimen. During the early postoperative period the cancer cells become entrapped by fibrin and are stimulated by inflammatory growth factors released during the healing process[18]. As a result of this mechanism of cancer dissemination, approximately 30% of gastric cancer patients after gastrectomy will develop resection site disease or peritoneal seeding.
RATIONALE FOR PERIOPERATIVE INTRAPERITONEAL CHEMOTHERAPY
Cytoreductive surgery combined with perioperative intraperitoneal chemotherapy is indicated in a majority of patients with diffuse malignant peritoneal mesothelioma and pseudomyxoma peritonei and in selected patients with peritoneal dissemination of colorectal cancer and gastric cancer. The fundamental goal of intraperitoneal chemotherapy administration is to maximize the total amount of drug delivered into the peritoneal tumor nodules while minimizing that delivered to the systemic circulation. The cytotoxic effects on peritoneal cancer nodules are the result of direct physical contact with intraperitoneal chemotherapy followed by penetration by diffusion. These events are influenced by the drug concentration in the chemotherapy solution, the ability of the drug to penetrate the tumor and the rate of elimination of the drug from the tumor nodules into the systemic circulation by capillary blood flow. Both natural or acquired drug resistance are important considerations in the long-term outcome of these treatments.
Physical properties of perioperative intraperitoneal chemotherapy
The physical-chemical properties of chemotherapeutic agents administered intraperitoneally should have larger, hydrophilic and ionized compounds. These molecules tend to clear more slowly from the peritoneal cavity than smaller, lipophilic and unionized compounds[19]. Therefore, the drugs selected for intraperitoneal administration tend to maintain a significantly greater concentration over a longer period of time in the peritoneal fluid than in plasma. This increases the exposure of the tumor nodules to a maximal dose of intraperitoneal chemotherapy, without necessarily an increase in systemic toxicity.
Mechanism of drug penetration
When drugs are delivered via the intraperitoneal route, they penetrate tumor nodules by passive diffusion. Active transport has not been shown to be important in intraperitoneal chemotherapy gaining access to the tumor nodules. The depth of penetration achieved by passive diffusion is limited. Experiments suggest that the depth of penetration may be only a few cell layers to perhaps 2 to 3 mm[20]. As a result, the greatest clinical benefit will only occur in patients having complete eradication of all macroscopic disease by surgery. The smallest possible tumor nodules remain to be eradicated by intraperitoneal chemotherapy.
Timing of perioperative intraperitoneal chemotherapy
The timing of intraperitoneal chemotherapy administration is critically important in achieving the best therapeutic outcomes. Currently, two time periods are utilized for intraperitoneal administration - intraoperative and early postoperative. Drugs selected for intraoperative use generally have three requirements. They are augmented by heat and can cause a cytotoxic effect to cancer cells within 60 to 90 min independent of cell division[21,22]. Heat is used because it has a direct cytotoxic effect on cancer cells. In addition, hyperthermia causes an important augmentation of cell kill by certain drugs; consequently it may markedly increase regional cytotoxicity of the chemotherapeutic agents (Figure 1). Third, and perhaps most importantly, heat increases the penetration of chemotherapy into cancer cells (Figure 2).
Figure 1.
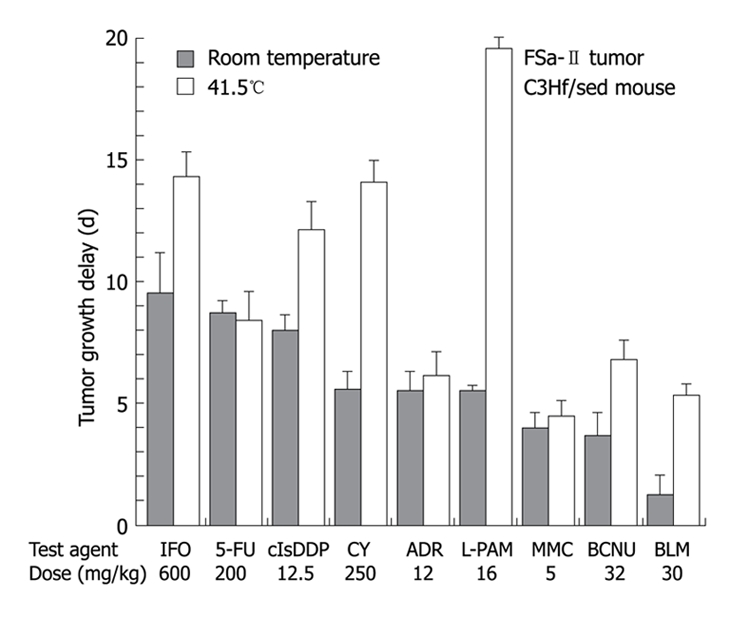
Tumor growth time with intraperitoneal chemotherapy alone vs heated intraperitoneal chemotherapy at 41.5°C. Tumor growth is delayed in heated intraperitoneal chemotherapy.
Figure 2.

Heat increases the penetration of intraperitoneal chemotherapy into tissues. Modified from reference[53].
The combination of intraperitoneal chemotherapy used in the operating room with hyperthermia has been referred to by many different names: Heated intraoperative intraperitoneal chemotherapy (HIIC); Intraperitoneal hyperthermic chemotherapy (IPHC); or Hyperthermic intraperitoneal chemotherapy (HIPEC). In this review, HIIC was used.
In the early postoperative period, before the inevitable postoperative intraabdominal adhesive process occurs, chemotherapy can be delivered and drained via intraperitoneal catheters. During the first 7 postoperative days the dwell may be continued for 12 to 24 h. Its distribution is relatively uniform throughout the abdominal cavity. This plan for chemotherapy administration is known as “early postoperative intraperitoneal chemotherapy (EPIC)”. The drugs should have a large molecular weight so that they are maintained within the peritoneal cavity for a longer period of time. EPIC is usually continued for several days, and consequently cell cycle specific drugs can be used[17].
HEATED INTRAOPERATIVE INTRAPERITONEAL CHEMOTHERAPY
Mitomycin C
Mitomycin C is the most common agent used for HIIC in the treatment of patients with peritoneal carcinomatosis from appendiceal and colorectal cancers and is used in conjunction with other drugs for gastric malignancy. It is an antitumor antibiotic, with approximately 90% of the drug absorbed within the 90-min intraperitoneal irrigation. Its molecular weight is 334 and the area under the curve ratio between intraperitoneal concentration over plasma concentration times time is approximately 30 (Figure 3)[23]. The depth of tissue penetration achieved by mitomycin C is up to 6 cell layers. It is rarely administered intravenously, as it has a high systemic toxicity profile. The renal toxicities of this drug can be prevented with forced diuresis intraoperatively and the hemolytic uremic syndrome has never been reported following intraperitoneal administration. Mitomycin C has potential adverse effects on wound healing, which can contribute to bowel perforation from anastomotic leak or fistula formation[24,25].
Figure 3.

HIIC with MMC. The area under the curve ratio of intraperitoneal concentration over plasma concentration times time of heated intraoperative intraperitoneal mitomycin C is approximately 30. HIIC: Heated intraoperative intraperitoneal chemotherapy.
Currently, there has been a standardized dosage of mitomycin C established. In Amsterdam, it is administered at 30 mg/m2 to 40 mg/m2 as a single agent. In Washington, when combined with EPIC 5-fluorouracil the dose is recommended at 15 mg/m2. Data regarding long-term survival reflecting the dose-response effects of intraperitoneal mitomycin C are difficult to interpret[26]. Some confusion regarding dosimetry and toxicity may be clarified by a recent study on pharmacokinetic changes induced by the volume of chemotherapy solution. In patients treated with hyperthermic intraperitoneal mitomycin C, the volume of carrier solution has a direct effect on systemic toxicity. Not only the dose of mitomycin C, but also the volume of chemotherapy solution should be determined by the patients’ body surface area (Figure 4)[27]. Based on this study, a standardized protocol involving 15 mg/m2 of mitomycin C in 1.5 L/m2 carrier solution for all patients has been implemented at the Washington Cancer Institute in order to achieve maximal therapeutic effects and more predictable systemic toxicities. This dose of HIIC mitomycin C is routinely combined with 600 mg/m2 per day for 5 d of 5-flourouracil.
Figure 4.

Absorption of mitomycin C from a hyperthermic solution containing 2, 4 or 6 L of 1.5% dextrose peritoneal dialysis solution. Cited form reference[27].
Results of treatment with mitomycin C
Xu and colleagues have recently suggested, in a meta-analysis, an improved management of advanced gastric cancer when HIIC is used in conjunction with complete resection (Hazard ratio: 0.51 and 95% confidence interval: 0.40-0.65)[28]. In 8 of the 11 studies, mitomycin C was used. Results of treatment with colorectal carcinomatosis patients who entered in a phase III randomized study of HIIC with mitomycin C have been reported by the Netherlands Cancer Center[15]. Patients with colorectal carcinomatosis were randomized to undergo systemic 5-fluorouracil/leucovorin therapy with or without palliative surgery versus cytoreduction, HIIC and systemic chemotherapy. A median survival of 12.6 mo was seen in the control arm, whereas the median survival of the HIIC arm was 22.3 mo (P = 0.032). The improved survival results from combined treatment with cytoreductive surgery and HIIC cannot be attributed to the effect of HIIC alone. However, at least in part, HIIC with mitomycin C has contributed to the prolonged median survival of colorectal carcinomatosis patients.
Doxorubicin
Doxorubicin is another antitumor antibiotic and is one of the earliest intraperitoneal chemotherapeutic agents used in clinical trials. Its molecular weight is 580 and the area under the curve ratio of intraperitoneal to intravenous concentration times time is 230. It is metabolized as a single pass through the liver so there is a low likelihood of systemic toxicities. Doxorubicin is augmented with heat and tissue penetration is at least five cell layers. This drug is ideally suited for intraperitoneal administration after a maximal attempt of cytoreduction[29,30]. It can also be used effectively with other intraperitoneal drugs, such as cisplatin and mitomycin C without pharmacological incompatibility.
Doxorubicin has a sclerosing effect on peritoneal surfaces. Sugarbaker and co-workers conducted a dose escalation study with pharmacokinetic monitoring of intraperitoneal doxorubicin and they demonstrated that a total dose of 15 mg/m2 results in a thin layering of fibrosis on the peritoneal surfaces. These adhesions are not extensive enough to cause abdominal pain or intestinal obstruction[31,32]. With the proper dosage, this sclerosing effect can be used for treating patients with debilitating ascites when combined with cisplatin (50 mg/m2). At the Washington Cancer Institute, this combination at 41.5°C in 1.5 L of chemotherapy solution is a standard regime for patients with diffuse malignant peritoneal mesothelioma[33].
Recent pharmacokinetic studies demonstrated that the doxorubicin content in small mesothelioma nodules far surpassed that measured in the peritoneal fluid (Figure 5). An active uptake of doxorubicin by mesothelioma tumor nodules was proposed and would be expected to result in a maximal response[34].
Figure 5.

Pharmacokinetic profile of heated intraoperative intraperitoneal doxorubicin showing that the doxorubicin concentration in the tumor nodule is higher than that in the peritoneal fluid.
Cisplatin
Cisplatin is an alkylating agent. It has been used by intraperitoneal administration for treating gastric cancer, ovarian cancer and diffuse malignant peritoneal mesothelioma[35]. Its molecular weight is 300 and the area under the curve ratio of intraperitoneal concentration to plasma concentration times time is approximately 10 (Figure 6). Although the area under the curve ratio is not as striking as some of the other intraperitoneal drugs, it can be used synchronously with many other agents. Its cytotoxicity is augmented by heat up to 3 times at 41.5°C[36]. It can effectively penetrate tumor nodules up to 3 mm. Currently, all patients with diffuse malignant peritoneal mesothelioma managed at our institution with cytoreductive surgery are given HIIC with doxorubicin and cisplatin.
Figure 6.

The area under the curve ratio of intraperitoneal concentration over plasma concentration times time of heated intraoperative intraperitoneal cisplatin is approximately 10.
Results of treatment with doxorubicin and cisplatin
The most recent update has shown that the median survival of 100 consecutive patients with diffuse malignant peritoneal mesothelioma was 50 mo and the 5-year survival rate was 44%. This survival statistic should be compared to historical controls with this disease who have a median survival of one year. In this study, all patients were given a combination of cisplatin plus doxorubicin. It is not possible to show the isolated effect of cisplatin in a majority of reports.
Melphalan
Melphalan is a well-known antineoplastic alkylating agent that has been used to treat cancer patients for over 50 years and it remains the most effective single drug used in heated limb perfusion for in-transit metastases from melanomas and advanced primary or recurrent extremity soft tissue sarcomas[37-39]. Its molecular weight is 334 and the area under the curve ratio of intraperitoneal concentration to plasma concentration times time is approximately 93. It has remarkably increased pharmacological activity with heat in both in vitro and in vivo studies[22,40,41]. Glehen and colleagues showed that hyperthermia has little effect on intraperitoneal or plasma concentration of melphalan, and there was a significant increase in tissue penetration of this drug with heat[40]. Melphalan exerts its antineoplastic effect through the formation of interstrand DNA cross-links. It is believed that the formation of these DNA cross-links is promoted at increased temperatures, leading to enhanced cell killing. Recent phase I/II clinical trials using melphalan in patients with small volume residual carcinomatosis post cytoreductive surgery at a dose of 70 mg/m2 have been completed at our institution.
Figure 7 shows the pharmacokinetic profile of melphalan given intraperitoneally at 70 mg/m2 in 3 L of 1.5% dextrose peritoneal dialysis solution at 42°C for 90 min. Pharmacokinetic studies showed that the drug concentration in the tumor nodules was approximately 30% of the intraperitoneal concentration and 10 times the plasma concentration[41].
Figure 7.

Pharmackinetics of HIIC with melphalan. Pharmacokinetic profile of melphalan given intraperitoneally at 70 mg/m2 in 3 L of 1.5% dextrose peritoneal dialysis solution at 42°C for 90 min. Pharmacokinetic studies showed that the drug concentration in the tumor nodules was approximately 30% of the intraperitoneal concentration and 10 times the plasma concentration.
EARLY POSTOPERATIVE INTRAPERITONEAL CHEMOTHERAPY
5-Fluorouracil
5-Fluorouracil is routinely used with EPIC for peritoneal carcinomatosis from numerous gastrointestinal malignancies. It is an antimetabolite that is incorporated into the DNA, which then causes chain termination. Its molecular weight is 130 and the area under the curve is 250. It is metabolized by a single pass through the liver, so that the systemic toxicity is very limited. Caution must be used in patients having liver dysfunction. When used as a single agent, the dose can be as high as 800 mg/m2 per day for 5 d. When administered in patients after having had HIIC with mitomycin C, the dose is reduced to 650 mg/m2[30]. Pestieau and colleagues demonstrated that the clearance of 5-FU from the peritoneal cavity could be significantly reduced with using hypertonic and high molecular weight carrier solutions[42]. This would, in turn, prolong 5-FU availability in the peritoneal cavity. It has also been reported that intraperitoneal 5-FU may play a role in preventing postoperative intraperitoneal adhesions and the clinical implications of this finding deserves more attention[43].
Paclitaxel
Paclitaxel is an antimitotic drug that stabilizes microtubules and inhibits their depolymerization for free tubulin. Its molecular weight is 862 and the area under the curve ratio is 1000. It can penetrate more than 80 cell layers and is extremely favorable for intraperitoneal use[44]. At our institution, EPIC with paclitaxel has been routinely used since 1998 for patients with diffuse malignant peritoneal mesothelioma. It is instilled as a lavage into the peritoneal cavity; gravity distribution is encouraged by the patient’s movement from side to side for the first 6 h of the 23 h dwelling[33]. This treatment is repeated daily for the first 5 postoperative days. By the intention to treat principle, all patients are to receive EPIC with paclitaxel, unless they experience perioperative complications early in the postoperative period.
Mohamed and co-workers studied the use of 6% hetastarch as the carrier solution for paclitaxel. Because hetastarch is a larger molecule, its clearance from the peritoneal cavity was reduced, as compared to peritoneal dialysis solution. By maintaining an artificial ascites, hetastarch increased the exposure of peritoneal surfaces to paclitaxel; the volume of carrier solution was increased and the drug concentration remained unchanged (Figure 8)[45].
Figure 8.

Mean total drug remaining in peritoneal cavity at 23 h. Hypertonic carrier solutions maintain the artificial ascites and paclitaxel concentrations, during early postoperative intraperitoneal paclitaxel instillation. Cite from reference[45].
This is likely to further increase the tumor response to paclitaxel.
Stuart and colleagues recently found that the carcinogen diethylhexylphthalate (DEHP) is leached by a paclitaxel chemotherapy solution from polyvinyl chloride based containers. Because DEHP is present in all soft plastic tubing, precautionary steps must be taken or the carcinogen may be transferred to patients receiving intraperitoneal paclitaxel[46]. They recommended using non-DEHP containing plastic for paclitaxel delivery.
FUTURE DIRECTIONS
Neoadjuvant intraperitoneal chemotherapy for gastric cancer
Recently, Yonemura and co-workers reported using combined systemic and intraperitoneal chemotherapy (bi-directional) for patients with gastric peritoneal carcinomatosis who were unable to have a complete cytoreduction due to the extensive nature of their disease[47]. Subsequently, they selected patients who responded to the neoadjuvant chemotherapy to undergo further cytoreductive surgery. The concept of this new approach, using neoadjuvant intraperitoneal chemotherapy to downstage those patients who are chemosensitive, is appealing. They reported that a complete cytoreduction was achieved in 25% of treated patients and this resulted in a prolonged survival.
As in many different peritoneal surface malignancies, completeness of cytoreduction was an important factor determining overall survival. It is related to the pretreatment tumor load, aggressiveness of the tumor and surgeon’s technical ability. In patients with peritoneal dissemination involving the small bowel and small bowel mesenteric surfaces, it is almost impossible to remove all visible tumor nodules, and at the same time to preserve sufficient length of small bowel to ensure adequate nutrition. Neoadjuvant chemotherapy may have a useful role in this subgroup of patients to downstage the tumor load on the small bowel and its mesentery. Selecting those who responded to the intraperitoneal chemotherapy to undergo further cytoreduction may result in an improved overall survival.
Bi-directional intraoperative chemotherapy
Another use of bi-directional chemotherapy delivery has been proposed by Elias and colleagues. This involves the administration of intravenous chemotherapy simultaneous with HIIC[48]. The intravenous drug that is chosen is also augmented by heat and is delivered to the peritoneal tumor nodules through capillary flow. This is “hyperthermic targeting” of intravenous chemotherapy to the peritoneal surface. In this concept, tumor nodule penetration is not only from the surface by passive diffusion, but also from within by capillary flow. A study has been initiated to investigate HIIC of cisplatin and doxorubicin combined with intravenous ifosfamide after cytoreductive surgery for peritoneal dissemination of advanced or recurrent epithelial ovarian cancer and papillary serous carcinoma. It is hoped that this bi-directional hyperthermic local-regional treatment will result in improved survival of these patients. The agents most recommended for heat synergy are melphalan, ifosfamide and cyclophosphamide. These drugs may double their cytotoxicity for cancer cells when used with hyperthermia[36].
Adjuvant intraperitoneal chemotherapy
Surgery for gastrointestinal cancer is associated with an extremely high local recurrence rate. The mechanism whereby a large proportion of patients have disease recurrence confined to the resection site and peritoneal surfaces is related to traumatic dissemination of tumor emboli within the peritoneal cavity, and the implantation of these tumor emboli within the fibrinous exudates that accumulate at the resection site and on abraded peritoneal surfaces. Sources for these intraabdominal tumor emboli include coelomic perforation at the primary cancer site, severed lymphatic channels during surgery and disrupted tissue emboli within the blood loss from tumor specimen. Yu and co-workers reported an improved survival in patients who received adjuvant intraperitoneal chemotherapy for advanced gastric cancer[18,49]. It is likely that both HIIC and EPIC will benefit these patients with a high risk of intraperitoneal recurrence.
Standardization of treatment regimens for multi-institutional studies
Other drugs have been used for HIIC or EPIC by other groups around the world. Also, two chemotherapy agents have been approved by the FDA for intraperitoneal administration. These drugs are cyclophosphamide and nitrogen mustard. Currently, neither of these drugs are used regularly for treating patients with peritoneal surface malignancy. A new drug that has been piloted in Villejuif by Elias and his colleagues is oxaliplatin[48]. Pharmacologic doses are used over a short time period in an attempt to increase drug penetration into the tumor. DeBree and colleagues have used docetaxel with heat[50]. Although docetaxel is not heat-augmented, it is possible that the hyperthermia will increase drug penetration into tumor nodules. Groups in Japan have used mitomycin C, cisplatin and etoposide, as a multi-drug chemotherapy solution[51]. Mitoxantrone has also been used by Link and colleagues in Wiesbaden in order to control debilitating ascites[52].
Although the rationale of cytoreductive surgery combined with perioperative intraperitoneal chemotherapy is appealing, local-regional recurrence is common following this comprehensive treatment strategy. With new development and continuous evolution of treatment plans, reduced perioperative morbidity and mortality, along with increased disease-free survival and overall survival results are possible. A change in the management approach for patients with peritoneal surface malignancy is necessary. In contrast to the historical data, where the survival for patients with peritoneal dissemination was uniformly disappointing, survival has markedly improved with the new comprehensive treatments. It is necessary to form a multidisciplinary approach to assess patients with peritoneal surface malignancy. A medical oncologist should consult a surgeon in regard to the management of these patients before initiating a palliative approach with systemic chemotherapy. Systemic chemotherapy has been repetitively shown to be of no survival benefit. For future studies, many important issues, such as selection of drugs, potency of multiple agents, optimal degree of hyperthermia, concentration and duration of intraperitoneal chemotherapy, need to be clarified.
Footnotes
Peer reviewer: Tomomitsu Tahara, MD, PhD, Department of Gastroenterology, Fujita Health University, Dengakugakubo, Kutsukakecyo, Toyoake, Aichi 470-1192, Japan
S- Editor Li LF L- Editor Lutze M E- Editor Lin YP
References
- 1.Piso P, Bektas H, Werner U, Schlitt HJ, Kubicka S, Bornscheuer A, Manns M, Klempnauer J. Improved prognosis following peritonectomy procedures and hyperthermic intraperitoneal chemotherapy for peritoneal carcinomatosis from appendiceal carcinoma. Eur J Surg Oncol. 2001;27:286–290. doi: 10.1053/ejso.2000.1095. [DOI] [PubMed] [Google Scholar]
- 2.Butterworth SA, Panton ON, Klaassen DJ, Shah AM, McGregor GI. Morbidity and mortality associated with intraperitoneal chemotherapy for Pseudomyxoma peritonei. Am J Surg. 2002;183:529–532. doi: 10.1016/s0002-9610(02)00843-7. [DOI] [PubMed] [Google Scholar]
- 3.Witkamp AJ, de Bree E, Kaag MM, van Slooten GW, van Coevorden F, Zoetmulder FA. Extensive surgical cytoreduction and intraoperative hyperthermic intraperitoneal chemotherapy in patients with pseudomyxoma peritonei. Br J Surg. 2001;88:458–463. doi: 10.1046/j.1365-2168.2001.01701.x. [DOI] [PubMed] [Google Scholar]
- 4.Sugarbaker PH. Cytoreductive surgery and peri-operative intraperitoneal chemotherapy as a curative approach to pseudomyxoma peritonei syndrome. Eur J Surg Oncol. 2001;27:239–243. doi: 10.1053/ejso.2000.1038. [DOI] [PubMed] [Google Scholar]
- 5.Loggie BW, Fleming RA, McQuellon RP, Russell GB, Geisinger KR, Levine EA. Prospective trial for the treatment of malignant peritoneal mesothelioma. Am Surg. 2001;67:999–1003. [PubMed] [Google Scholar]
- 6.Sebbag G, Yan H, Shmookler BM, Chang D, Sugarbaker PH. Results of treatment of 33 patients with peritoneal mesothelioma. Br J Surg. 2000;87:1587–1593. doi: 10.1046/j.1365-2168.2000.01571.x. [DOI] [PubMed] [Google Scholar]
- 7.Sugarbaker PH, Welch LS, Mohamed F, Glehen O. A review of peritoneal mesothelioma at the Washington Cancer Institute. Surg Oncol Clin N Am. 2003;12:605–621, xi. doi: 10.1016/s1055-3207(03)00045-0. [DOI] [PubMed] [Google Scholar]
- 8.Feldman AL, Libutti SK, Pingpank JF, Bartlett DL, Beresnev TH, Mavroukakis SM, Steinberg SM, Liewehr DJ, Kleiner DE, Alexander HR. Analysis of factors associated with outcome in patients with malignant peritoneal mesothelioma undergoing surgical debulking and intraperitoneal chemotherapy. J Clin Oncol. 2003;21:4560–4567. doi: 10.1200/JCO.2003.04.150. [DOI] [PubMed] [Google Scholar]
- 9.Fujimura T, Yonemura Y, Fujita H, Michiwa Y, Kawamura T, Nojima N, Sato T, Fushida S, Nishimura G, Miwa K, et al. Chemohyperthermic peritoneal perfusion for peritoneal dissemination in various intra-abdominal malignancies. Int Surg. 1999;84:60–66. [PubMed] [Google Scholar]
- 10.Witkamp AJ, de Bree E, Kaag MM, Boot H, Beijnen JH, van Slooten GW, van Coevorden F, Zoetmulder FA. Extensive cytoreductive surgery followed by intra-operative hyperthermic intraperitoneal chemotherapy with mitomycin-C in patients with peritoneal carcinomatosis of colorectal origin. Eur J Cancer. 2001;37:979–984. doi: 10.1016/s0959-8049(01)00058-2. [DOI] [PubMed] [Google Scholar]
- 11.Elias D, Blot F, El Otmany A, Antoun S, Lasser P, Boige V, Rougier P, Ducreux M. Curative treatment of peritoneal carcinomatosis arising from colorectal cancer by complete resection and intraperitoneal chemotherapy. Cancer. 2001;92:71–76. doi: 10.1002/1097-0142(20010701)92:1<71::aid-cncr1293>3.0.co;2-9. [DOI] [PubMed] [Google Scholar]
- 12.Pestieau SR, Sugarbaker PH. Treatment of primary colon cancer with peritoneal carcinomatosis: comparison of concomitant vs. delayed management. Dis Colon Rectum. 2000;43:1341–1346; discussion 1347-1348. doi: 10.1007/BF02236627. [DOI] [PubMed] [Google Scholar]
- 13.Zoetmulder FA, Verwaal V, Ruth S. General Poster: Hyperthermic intra peritoneal chemotherapy with mitomycin C significantly improves survival in patients with peritoneal carcinomatosis of colorectal origin. Abstract 586. Proc Am Soc Clin Oncol. 2002;21:147a. [Google Scholar]
- 14.Shen P, Hawksworth J, Lovato J, Loggie BW, Geisinger KR, Fleming RA, Levine EA. Cytoreductive surgery and intraperitoneal hyperthermic chemotherapy with mitomycin C for peritoneal carcinomatosis from nonappendiceal colorectal carcinoma. Ann Surg Oncol. 2004;11:178–186. doi: 10.1245/aso.2004.05.009. [DOI] [PubMed] [Google Scholar]
- 15.Glehen O, Kwiatkowski F, Sugarbaker PH, Elias D, Levine EA, De Simone M, Barone R, Yonemura Y, Cavaliere F, Quenet F, et al. Cytoreductive surgery combined with perioperative intraperitoneal chemotherapy for the management of peritoneal carcinomatosis from colorectal cancer: a multi-institutional study. J Clin Oncol. 2004;22:3284–3292. doi: 10.1200/JCO.2004.10.012. [DOI] [PubMed] [Google Scholar]
- 16.Carmignani CP, Sugarbaker TA, Bromley CM, Sugarbaker PH. Intraperitoneal cancer dissemination: mechanisms of the patterns of spread. Cancer Metastasis Rev. 2003;22:465–472. doi: 10.1023/a:1023791229361. [DOI] [PubMed] [Google Scholar]
- 17.Sugarbaker PH, Graves T, DeBruijn EA, Cunliffe WJ, Mullins RE, Hull WE, Oliff L, Schlag P. Early postoperative intraperitoneal chemotherapy as an adjuvant therapy to surgery for peritoneal carcinomatosis from gastrointestinal cancer: pharmacological studies. Cancer Res. 1990;50:5790–5794. [PubMed] [Google Scholar]
- 18.Sugarbaker PH, Yu W, Yonemura Y. Gastrectomy, peritonectomy, and perioperative intraperitoneal chemotherapy: the evolution of treatment strategies for advanced gastric cancer. Semin Surg Oncol. 2003;21:233–248. doi: 10.1002/ssu.10042. [DOI] [PubMed] [Google Scholar]
- 19.Torres IJ, Litterst CL, Guarino AM. Transport of model compounds across the peritoneal membrane in the rat. Pharmacology. 1978;17:330–340. doi: 10.1159/000136874. [DOI] [PubMed] [Google Scholar]
- 20.Los G, Mutsaers PH, Lenglet WJ, Baldew GS, McVie JG. Platinum distribution in intraperitoneal tumors after intraperitoneal cisplatin treatment. Cancer Chemother Pharmacol. 1990;25:389–394. doi: 10.1007/BF00686048. [DOI] [PubMed] [Google Scholar]
- 21.Hahn GM. Potential for therapy of drugs and hyperthermia. Cancer Res. 1979;39:2264–2268. [PubMed] [Google Scholar]
- 22.Mohamed F, Marchettini P, Stuart OA, Urano M, Sugarbaker PH. Thermal enhancement of new chemotherapeutic agents at moderate hyperthermia. Ann Surg Oncol. 2003;10:463–468. doi: 10.1245/aso.2003.08.006. [DOI] [PubMed] [Google Scholar]
- 23.Fernández-Trigo V, Stuart OA, Stephens AD, Hoover LD, Sugarbaker PH. Surgically directed chemotherapy: heated intraperitoneal lavage with mitomycin C. Cancer Treat Res. 1996;81:51–61. doi: 10.1007/978-1-4613-1245-1_6. [DOI] [PubMed] [Google Scholar]
- 24.Stephens AD, Alderman R, Chang D, Edwards GD, Esquivel J, Sebbag G, Steves MA, Sugarbaker PH. Morbidity and mortality analysis of 200 treatments with cytoreductive surgery and hyperthermic intraoperative intraperitoneal chemotherapy using the coliseum technique. Ann Surg Oncol. 1999;6:790–796. doi: 10.1007/s10434-999-0790-0. [DOI] [PubMed] [Google Scholar]
- 25.Glehen O, Osinsky D, Cotte E, Kwiatkowski F, Freyer G, Isaac S, Trillet-Lenoir V, Sayag-Beaujard AC, François Y, Vignal J, et al. Intraperitoneal chemohyperthermia using a closed abdominal procedure and cytoreductive surgery for the treatment of peritoneal carcinomatosis: morbidity and mortality analysis of 216 consecutive procedures. Ann Surg Oncol. 2003;10:863–869. doi: 10.1245/aso.2003.01.018. [DOI] [PubMed] [Google Scholar]
- 26.van Ruth S, Verwaal VJ, Zoetmulder FA. Pharmacokinetics of intraperitoneal mitomycin C. Surg Oncol Clin N Am. 2003;12:771–780. doi: 10.1016/s1055-3207(03)00031-0. [DOI] [PubMed] [Google Scholar]
- 27.Sugarbaker PH, Stuart OA, Carmignani CP. Pharmacokinetic changes induced by the volume of chemotherapy solutions in patients treated with hyperthermic intraperitoneal mitomycin C. Cancer Chemother Pharmacol. 2005;11:1–6. doi: 10.1007/s00280-005-0074-8. [DOI] [PubMed] [Google Scholar]
- 28.Xu DZ, Zhan YQ, Sun XW, Cao SM, Geng QR. Meta-analysis of intraperitoneal chemotherapy for gastric cancer. World J Gastroenterol. 2004;10:2727–2730. doi: 10.3748/wjg.v10.i18.2727. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Jacquet P, Stuart OA, Chang D, Sugarbaker PH. Effects of intra-abdominal pressure on pharmacokinetics and tissue distribution of doxorubicin after intraperitoneal administration. Anticancer Drugs. 1996;7:596–603. doi: 10.1097/00001813-199607000-00016. [DOI] [PubMed] [Google Scholar]
- 30.Ozols RF, Locker GY, Doroshow JH, Grotzinger KR, Myers CE, Young RC. Pharmacokinetics of adriamycin and tissue penetration in murine ovarian cancer. Cancer Res. 1979;39:3209–3214. [PubMed] [Google Scholar]
- 31.Sugarbaker PH. Early postoperative intraperitoneal Adriamycin as an adjunctive treatment for advanced gastric cancer with lymph node or serosal invasion. In: Sugarbaker PH, ed , editors. Management of Gastric Cancer. Boston: Kluwer Academic Publishers; 1991. pp. 277–284. [DOI] [PubMed] [Google Scholar]
- 32.Sugarbaker PH. Early postoperative intraperitoneal Adriamycin as an adjunctive treatment for visceral and retroperitoneal sarcoma. In: Sugarbaker PH, ed , editors. Management of Gastric Cancer. Boston: Kluwer Academic Publishers; 1996. pp. 7–14. [DOI] [PubMed] [Google Scholar]
- 33.Sugarbaker PH. Management of peritoneal surface malignancy using intraperitoneal chemotherapy and cytoreductive surgery. A Manual for Physicians ans Nurses. 3rd ed. Grand Rapids, MI: The Ludann Company; 1998. [Google Scholar]
- 34.Stephens AD, Belliveau JF, Sugarbaker PH. Intraoperative hyperthermic lavage with cisplatin for peritoneal carcinomatosis and sarcomatosis. In: Sugarbaker , ed , editors. Peritoneal carcinomatosis drugs and diseases. Boston: Kluwer Academic Publishers; 1996. pp. 15–30. [DOI] [PubMed] [Google Scholar]
- 35.Berthet B, Sugarbaker TA, Chang D, Sugarbaker PH. Quantitative methodologies for selection of patients with recurrent abdominopelvic sarcoma for treatment. Eur J Cancer. 1999;35:413–419. doi: 10.1016/s0959-8049(98)00375-x. [DOI] [PubMed] [Google Scholar]
- 36.Urano M, Kuroda M, Nishimura Y. For the clinical application of thermochemotherapy given at mild temperatures. Int J Hyperthermia. 1999;15:79–107. doi: 10.1080/026567399285765. [DOI] [PubMed] [Google Scholar]
- 37.Sarosy G, Leyland-Jones B, Soochan P, Cheson BD. The systemic administration of intravenous melphalan. J Clin Oncol. 1988;6:1768–1782. doi: 10.1200/JCO.1988.6.11.1768. [DOI] [PubMed] [Google Scholar]
- 38.Liénard D, Eggermont AM, Kroon BB, Schraffordt Koops H, Lejeune FJ. Isolated limb perfusion in primary and recurrent melanoma: indications and results. Semin Surg Oncol. 1998;14:202–209. doi: 10.1002/(sici)1098-2388(199804/05)14:3<202::aid-ssu3>3.0.co;2-c. [DOI] [PubMed] [Google Scholar]
- 39.Schraffordt Koops H, Eggermont AM, Liénard D, Kroon BB, Hoekstra HJ, Van Geel AN, Nieweg OE, Lejeune FJ. Hyperthermic isolated limb perfusion for the treatment of soft tissue sarcomas. Semin Surg Oncol. 1998;14:210–214. doi: 10.1002/(sici)1098-2388(199804/05)14:3<210::aid-ssu4>3.0.co;2-b. [DOI] [PubMed] [Google Scholar]
- 40.Glehen O, Stuart OA, Mohamed F, Sugarbaker PH. Hyperthermia modifies pharmacokinetics and tissue distribution of intraperitoneal melphalan in a rat model. Cancer Chemother Pharmacol. 2004;54:79–84. doi: 10.1007/s00280-004-0779-0. [DOI] [PubMed] [Google Scholar]
- 41.Sugarbaker PH, Stuart OA. Pharmacokinetic and phase II study of heated intraoperative intraperitoneal melphalan. Cancer Chemother Pharmacol. 2007;59:151–155. doi: 10.1007/s00280-006-0238-1. [DOI] [PubMed] [Google Scholar]
- 42.Pestieau SR, Schnake KJ, Stuart OA, Sugarbaker PH. Impact of carrier solutions on pharmacokinetics of intraperitoneal chemotherapy. Cancer Chemother Pharmacol. 2001;47:269–276. doi: 10.1007/s002800000214. [DOI] [PubMed] [Google Scholar]
- 43.Pestieau SR, Marchettini P, Stuart OA, Chang D, Sugarbaker PH. Prevention of intraperitoneal adhesions by intraperitoneal lavage and intraperitoneal 5-fluorouracil: experimental studies. Int Surg. 2002;87:195–200. [PubMed] [Google Scholar]
- 44.Kuh HJ, Jang SH, Wientjes MG, Weaver JR, Au JL. Determinants of paclitaxel penetration and accumulation in human solid tumor. J Pharmacol Exp Ther. 1999;290:871–880. [PubMed] [Google Scholar]
- 45.Mohamed F, Marchettini P, Stuart OA, Yoo D, Sugarbaker PH. A comparison of hetastarch and peritoneal dialysis solution for intraperitoneal chemotherapy delivery. Eur J Surg Oncol. 2003;29:261–265. doi: 10.1053/ejso.2002.1397. [DOI] [PubMed] [Google Scholar]
- 46.Stuart OA, Knight C, Sugarbaker PH. Avoiding carcinogen exposure with intraperitoneal paclitaxel. Oncol Nurs Forum. 2005;32:44–48. doi: 10.1188/05.ONF.44-48. [DOI] [PubMed] [Google Scholar]
- 47.Yonemura Y, Bandou E, Sawa T, Yoshimitsu Y, Endou Y, Sasaki T, Sugarbaker PH. Neoadjuvant treatment of gastric cancer with peritoneal dissemination. Eur J Surg Oncol. 2006;32:661–665. doi: 10.1016/j.ejso.2006.03.007. [DOI] [PubMed] [Google Scholar]
- 48.Elias DM, Sideris L. Pharmacokinetics of heated intraoperative intraperitoneal oxaliplatin after complete resection of peritoneal carcinomatosis. Surg Oncol Clin N Am. 2003;12:755–769, xiv. doi: 10.1016/s1055-3207(03)00051-6. [DOI] [PubMed] [Google Scholar]
- 49.Yu W, Whang I, Chung HY, Averbach A, Sugarbaker PH. Indications for early postoperative intraperitoneal chemotherapy of advanced gastric cancer: results of a prospective randomized trial. World J Surg. 2001;25:985–990. doi: 10.1007/s00268-001-0067-7. [DOI] [PubMed] [Google Scholar]
- 50.de Bree E, Rosing H, Michalakis J, Romanos J, Relakis K, Theodoropoulos PA, Beijnen JH, Georgoulias V, Tsiftsis DD. Intraperitoneal chemotherapy with taxanes for ovarian cancer with peritoneal dissemination. Eur J Surg Oncol. 2006;32:666–670. doi: 10.1016/j.ejso.2006.03.008. [DOI] [PubMed] [Google Scholar]
- 51.Yonemura Y, Kawamura T, Bandou E, Takahashi S, Sawa T, Matsuki N. Treatment of peritoneal dissemination from gastric cancer by peritonectomy and chemohyperthermic peritoneal perfusion. Br J Surg. 2005;92:370–375. doi: 10.1002/bjs.4695. [DOI] [PubMed] [Google Scholar]
- 52.Link KH, Roitman M, Holtappels M, Runnebaum I, Urbanzyk H, Leder G, Staib L. Intraperitoneal chemotherapy with mitoxantrone in malignant ascites. Surg Oncol Clin N Am. 2003;12:865–872, xvi-xvi. doi: 10.1016/s1055-3207(03)00050-4. [DOI] [PubMed] [Google Scholar]
- 53.Jaquet P, Averbach A, Stuart AO, Chang D, Sugarbaker PH. Hyperthermic intraperitoneal doxorubicin: pharmacokinetics, metabolism and tissue distribution in a rate model. Cancer Chemother Pharmacol. 1998;41:147–154. doi: 10.1007/s002800050721. [DOI] [PubMed] [Google Scholar]