

Abstract
Clinical natural orifice surgery has been applied to abdominal surgery in recent years, mostly using transvaginal and transgastric access. Rectal and transcolonic natural orifice transluminal endoscopic surgery (NOTES) were tested in animal and cadaver models by a few research groups. Despite the potential advantages of transcolonic NOTES for colorectal diseases, it has not yet been clinically applied. The first successful series of human applications of transcolonic NOTES in the literature from the NOTES Research Group in Brazil provide new possibilities in the field in new transrectal procedures for rectal cancer and benign disease. Successful first human reports on Transcolonic NOTES potentially brings new frontiers and applications for minimally invasive surgery. The treatment of colorectal diseases through flexible Perirectal NOTES Access is a promising new approach alongside existing laparoscopic and open surgery to improve patient care.
Keywords: Rectal cancer, Total mesorectal excision, Colorectal surgery, Natural orifice surgery, Natural orifice transluminal endoscopic surgery, Minimally invasive surgery.
INTRODUCTION
Natural orifice surgery has emerged in recent years as a promising new alternative to open and laparoscopic abdominal surgery. Potential benefits in avoiding surgical incision complications led to the first successful series of clinical applications in the literature for transvaginal and transgastric natural orifice transluminal endoscopic surgery (NOTES)[1,2].
Transcolonic NOTES surgery was the subject of a few recent experimental studies that suggested that the access could be an attractive option for treating colonic and abdominal diseases[3-8]. Technical obstacles such as the risk of infection, safe entrance in the abdominal cavity and reliable colonic closure remain as issues preventing transcolonic clinical applications in the same time frame as vaginal and transoral access. The research group at our institution effectively developed new flexible techniques on transcolonic studies in an animal set and a transcolonic perirectal access was designed to allow access and therapy in the abdominal cavity and retroperitoneal space. Transcolonic NOTES has the potential to diagnose intra abdominal diseases and promote cancer staging, as well as representing a direct access to left colon diseases such as rectal and sigmoid cancer, diverticular disease and ulcerative colitis.
A technique developed at our institution and tested in an animal model, Perirectal NOTES Access (PNA), was used to start clinical applications. In 2009 this research enabled the performing of the first transcolonic NOTES human series in the literature using flexible endoscopic instruments to allow rectosigmoidectomy and total mesorectal excision (TME) for rectal cancer and applications for other benign diseases such as diverticulosis (Figures 1, 2 and 3).
Figure 1.
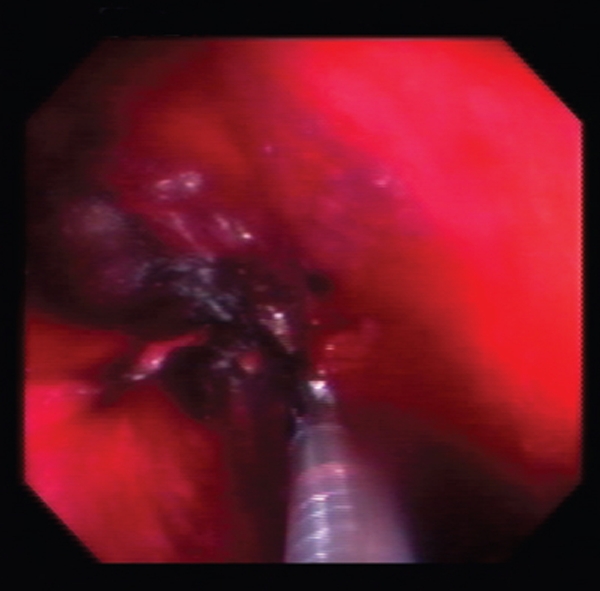
Total mesorectal resection using perirectal natural orifice transluminal endoscopic surgery (NOTES) access (PNA) was progressively accomplished using endoscopic monopolar scissors (ApolloEndosurgery, Austin, TX, USA) inside the ideal oncologic plane of dissection. The endoscope is inserted directly in the presacral space, from an incision above the dentate line, allowing flexible dissection in the anatomic oncologic plane from below. (Courtesy Brazilian NOTES Research Group).
Figure 2.

Full transanal extraction of the specimen with intact mesorectal resection in Transcolonic NOTES. The colonoscope is inserted directly in the perirectal retroperitoneal space through the incision, paralel to rectal lumen. (Courtesy Brazilian NOTES Research Group).
Figure 3.

Postoperative aspect of the abdomen of patient submitted to rectossigmoidectomy. (Courtesy Brazilian NOTES Research Group).
EVOLUTION OF THE COLORECTAL NOTES CONCEPT
In the last few years, there has been an increase in interest in the surgical community in even lesser invasive procedures to diagnose and treat abdominal diseases since the evolution of laparoscopy[9]. Natural orifice surgery, other than promising potential advantages and enthusiasm, had not yet been seen as superior to standard surgical therapy for any medical indication. Experimental and clinical studies still demonstrate that evolution of technology is needed to expand the possibilities of the new field to allow safety and efficiency of NOTES techniques.
Publications and presentations from scientific meetings since 2007 have described the first clinical human applications of the new method following IRB approval for human trials on NOTES in different countries. Since Zorrón et al[10], Marescaux et al[11], Zornig et al[12] and Branco Filho et al[13] described successful NOTES transvaginal cholecystectomy in early 2007, other groups followed and published their initial clinical results of the techniques, mostly assisted by laparoscopy for retraction or for camera purposes[14-24]. Transgastric NOTES was first performed by Rao and Reddy[25]. A large multicenter trial on NOTES (IMTN trial) describes the results of 362 cases with results similar to laparoscopy and longer operative times[26].
Whereas most investigators have chosen to gain peritoneal access via a vaginal or an oral transgastric route, few have investigated the transcolonic route[3-8]. The transcolonic approach has several theoretic advantages over the transgastric route. By eliminating the need for scope retroflection for upper abdominal surgery, it allows a more direct access and closer route than a transgastric approach and the anorectum allows passage of larger diameter instrumentation and retrieval of larger specimens[27]. Transcolonic and transvaginal extractions of specimens in laparoscopic surgery have been more constantly used in recent years to allow larger organs such as the spleen, kidney and colon to be retrieved avoiding an abdominal incision. These techniques, classified as NOSE (natural orifice specimen extraction[28]), showed good results with few complications reported. NOTES Transvaginal colectomy assisted by minilaparoscopy was first described in clinical setting by Lacy et al[29], naming the technique as MA-NOS in a patient for sigmoid cancer. Burghardt et al[30] reported a case of hybrid transvaginal right colectomy.
Transanally Endoscopic Microsurgery, developed and described by Buess et al[31,32] in the early 1980s, is currently a minimally invasive alternative for most benign lesions of the rectum and represents pioneer efforts in the field of natural orifice surgery. Resection of tumors in the upper rectum with entry into the suture closure of the peritoneum has recently been described without an increase in infectious postoperative complications[33].
Transcolonic NOTES using rigid transanal systems was the subject of research in recent experimental and cadaver studies. Whiteford et al[27] showed the feasibility of rigid NOTES sigmoid resection in three cadavers using transanal endoscopic microsurgery and allowing en-bloc lymphadenectomy and transanal retrieval and anastomosis. They found that the main obstacles for the use of rigid systems in colorectal surgery are the acute angle created by the sacral promontory and the limited reach of current instruments. Sylla et al[34] successfully performed a technique using rigid transanal resection of the colon and sometimes a transgastric flexible access to allow mobilization of the colon in a set of 14 non-survival and cadaver animal experiment. Leroy et al[35] described a combined technique using flexible and rigid transrectal and flexible transgastric accesses to perform sigmoidectomy in a pig model. The technique using the concept of Totally NOTES resulted in survival of all 5 pigs and no signs of peritonitis or intra abdominal abscess was found either in laparoscopy or by laparotomy on the 14th postoperative day. The authors pointed to the possibility of performing colorectal natural orifice surgery using available instruments.
TME with high lymphadenectomy is the standard of care for curative resection of rectal cancer[36], and minimally invasive surgery is showing growing evidence of being similar to open surgery in treating the disease[37]. The Brazilian NOTES Research Group, using the PNA, performed radical TME in the opposite of laparoscopic and open direction (from anal to rectosigmoid junction) performed along embryologic fusion planes, beginning the dissection by gaining access to the presacral plane located between the mesorectum and the presacral fascia (Figures 1-3). Entry and subsequent dissection in this avascular plane using flexible endoscopic equipment was more hazardous than formal laparoscopy due to limited instrumentation, but retropneumoperitoneum improved the exposure and dissection inside the anatomic plane. The new access provided safe entry and closure also for benign colorectal disease (diverticulosis) and as access for appendectomy and liver biopsy (Figures 4 and 5).
Figure 4.

Transcolonic retroperitoneal access (PNA) in animal model. (Courtesy Brazilian NOTES Research Group).
Figure 5.

Transcolonic liver biopsy in animal model. (Courtesy Brazilian NOTES Research Group).
Naturally, transrectal access raises concerns of infection control and still requires the need for secure closure of the colorectum[38,39]. However, a low entry point, as described in this human series using a retroperitoneal tunnel instead of puncturing the recto sigmoid junction, previously closing the proximal rectum allowed for a relatively isolated field that can be adequately disinfected. Despite the need of a colorectal perforation, choosing the entry point in the exact planned line of anastomosis minimizes the fear of unnecessary viscerotomy. The original transcolonic PNA allows a low and safe perforation of the rectum with ease and a safe entrance and closure under direct view. Former studies also described use of natural orifice surgery for cancer staging, using a transgastric[40] or a transvaginal approach[41]. Retroperitoneal insufflation and retroperitoneoscopy also represents original access to perform transcolonic retroperitoneal lymph node biopsies and even pancreatic, renal or adrenal surgery[42]. The PNA promotes a fast and easy access to abdominal cavity, avoiding the need of expensive technology for access.
The described new NOTES access for rectal cancer adhere to the principles of oncologic resection and opens a wide range of possibilities of future applications of transcolonic NOTES for colorectal surgery. Advantages over existing laparoscopic and open methods cannot be distinguished in this early concept; however flexible transorificial performance of colorectal operations seems promising.
Footnotes
Peer reviewers: Rungsun Rerknimitr, MD, Division of Gastroenterology, Internal Medicine, King Chulalongkorn Memorial Hospital, Rama IVC Rd, Lumpini, Bangkok 10310, Thailand; Tsuyoshi Konishi, MD, PhD, Department of Gastroenterological Surgery, Cancer Institute Hospital, 3-10-6 Ariake, Koto-ku, Tokyo 135-8550, Japan; Akira Tsunoda, MD, PhD, Professor Chief, Department of Surgery, Kameda Medical Center 929 Higashi-cho, Kamogawa City, Chiba 296-8602, Japan
S- Editor Li LF L- Editor Roemmele A E- Editor Yang C
References
- 1.Sodergren MH, Clark J, Athanasiou T, Teare J, Yang GZ, Darzi A. Natural orifice translumenal endoscopic surgery: critical appraisal of applications in clinical practice. Surg Endosc. 2009;23:680–687. doi: 10.1007/s00464-008-0278-1. [DOI] [PubMed] [Google Scholar]
- 2.Jay Pasricha P, Krummel TM. NOTES and other emerging trends in gastrointestinal endoscopy and surgery: the change that we need and the change that is real. Am J Gastroenterol. 2009;104:2384–2386. doi: 10.1038/ajg.2009.150. [DOI] [PubMed] [Google Scholar]
- 3.Pai RD, Fong DG, Bundga ME, Odze RD, Rattner DW, Thompson CC. Transcolonic endoscopic cholecystectomy: a NOTES survival study in a porcine model (with video) Gastrointest Endosc. 2006;64:428–434. doi: 10.1016/j.gie.2006.06.079. [DOI] [PubMed] [Google Scholar]
- 4.Wilhelm D, Meining A, von Delius S, Fiolka A, Can S, Hann von Weyhern C, Schneider A, Feussner H. An innovative, safe and sterile sigmoid access (ISSA) for NOTES. Endoscopy. 2007;39:401–406. doi: 10.1055/s-2007-966438. [DOI] [PubMed] [Google Scholar]
- 5.Ryou M, Fong DG, Pai RD, Sauer J, Thompson CC. Evaluation of a novel access and closure device for NOTES applications: a transcolonic survival study in the porcine model (with video) Gastrointest Endosc. 2008;67:964–969. doi: 10.1016/j.gie.2007.12.047. [DOI] [PubMed] [Google Scholar]
- 6.Ryou M, Thompson CC. Techniques for transanal access to the peritoneal cavity. Gastrointest Endosc Clin N Am. 2008;18:245–260; viii. doi: 10.1016/j.giec.2008.01.014. [DOI] [PubMed] [Google Scholar]
- 7.Sporn E, Bachman SL, Miedema BW, Loy TS, Calaluce R, Thaler K. Endoscopic colotomy closure for natural orifice transluminal endoscopic surgery using a T-fastener prototype in comparison to conventional laparoscopic suture closure. Gastrointest Endosc. 2008;68:724–730. doi: 10.1016/j.gie.2008.02.019. [DOI] [PubMed] [Google Scholar]
- 8.Bachman SL, Sporn E, Furrer JL, Astudillo JA, Calaluce R, McIntosh MA, Miedema BW, Thaler K. Colonic sterilization for natural orifice translumenal endoscopic surgery (NOTES) procedures: a comparison of two decontamination protocols. Surg Endosc. 2009;23:1854–1859. doi: 10.1007/s00464-008-0295-0. [DOI] [PubMed] [Google Scholar]
- 9.Kalloo AN, Singh VK, Jagannath SB, Niiyama H, Hill SL, Vaughn CA, Magee CA, Kantsevoy SV. Flexible transgastric peritoneoscopy: a novel approach to diagnostic and therapeutic interventions in the peritoneal cavity. Gastrointest Endosc. 2004;60:114–117. doi: 10.1016/s0016-5107(04)01309-4. [DOI] [PubMed] [Google Scholar]
- 10.Zorrón R, Filgueiras M, Maggioni LC, Pombo L, Lopes Carvalho G, Lacerda Oliveira A. NOTES. Transvaginal cholecystectomy: report of the first case. Surg Innov. 2007;14:279–283. doi: 10.1177/1553350607311090. [DOI] [PubMed] [Google Scholar]
- 11.Marescaux J, Dallemagne B, Perretta S, Wattiez A, Mutter D, Coumaros D. Surgery without scars: report of transluminal cholecystectomy in a human being. Arch Surg. 2007;142:823–826; discussion 826-827. doi: 10.1001/archsurg.142.9.823. [DOI] [PubMed] [Google Scholar]
- 12.Zornig C, Emmermann A, von Waldenfels HA, Mofid H. Laparoscopic cholecystectomy without visible scar: combined transvaginal and transumbilical approach. Endoscopy. 2007;39:913–915. doi: 10.1055/s-2007-966911. [DOI] [PubMed] [Google Scholar]
- 13.Branco Filho AJ, Noda RW, Kondo W, Kawahara N, Rangel M, Branco AW. Initial experience with hybrid transvaginal cholecystectomy. Gastrointest Endosc. 2007;66:1245–1248. doi: 10.1016/j.gie.2007.10.003. [DOI] [PubMed] [Google Scholar]
- 14.Ramos AC, Murakami A, Galvão Neto M, Galvão MS, Silva AC, Canseco EG, Moyses Y. NOTES transvaginal video-assisted cholecystectomy: first series. Endoscopy. 2008;40:572–575. doi: 10.1055/s-2008-1077398. [DOI] [PubMed] [Google Scholar]
- 15.Decarli LA, Zorron R, Branco A, Lima FC, Tang M, Pioneer SR, Sanseverino JI, Menguer R, Bigolin AV, Gagner M. New hybrid approach for NOTES transvaginal cholecystectomy: preliminary clinical experience. Surg Innov. 2009;16:181–186. doi: 10.1177/1553350609339375. [DOI] [PubMed] [Google Scholar]
- 16.Forgione A, Maggioni D, Sansonna F, Ferrari C, Di Lernia S, Citterio D, Magistro C, Frigerio L, Pugliese R. Transvaginal endoscopic cholecystectomy in human beings: preliminary results. J Laparoendosc Adv Surg Tech A. 2008;18:345–351. doi: 10.1089/lap.2007.0203. [DOI] [PubMed] [Google Scholar]
- 17.Zorron R, Maggioni LC, Pombo L, Oliveira AL, Carvalho GL, Filgueiras M. NOTES transvaginal cholecystectomy: preliminary clinical application. Surg Endosc. 2008;22:542–547. doi: 10.1007/s00464-007-9646-5. [DOI] [PubMed] [Google Scholar]
- 18.Gumbs AA, Fowler D, Milone L, Evanko JC, Ude AO, Stevens P, Bessler M. Transvaginal natural orifice translumenal endoscopic surgery cholecystectomy: early evolution of the technique. Ann Surg. 2009;249:908–912. doi: 10.1097/SLA.0b013e3181a802e2. [DOI] [PubMed] [Google Scholar]
- 19.Horgan S, Cullen JP, Talamini MA, Mintz Y, Ferreres A, Jacobsen GR, Sandler B, Bosia J, Savides T, Easter DW, et al. Natural orifice surgery: initial clinical experience. Surg Endosc. 2009;23:1512–1518. doi: 10.1007/s00464-009-0428-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Fischer LJ, Jacobsen G, Wong B, Thompson K, Bosia J, Talamini M, Horgan S. NOTES laparoscopic-assisted transvaginal sleeve gastrectomy in humans--description of preliminary experience in the United States. Surg Obes Relat Dis. 2009;5:633–636. doi: 10.1016/j.soard.2009.04.015. [DOI] [PubMed] [Google Scholar]
- 21.de Sousa LH, de Sousa JA, de Sousa Filho LH, de Sousa MM, de Sousa VM, de Sousa AP, Zorron R. Totally NOTES (T-NOTES) transvaginal cholecystectomy using two endoscopes: preliminary report. Surg Endosc. 2009:[Epub ahead of print]. doi: 10.1007/s00464-009-0453-z. [DOI] [PubMed] [Google Scholar]
- 22.Noguera J, Dolz C, Cuadrado A, Olea J, Vilella A, Morales R. Hybrid transvaginal cholecystectomy, NOTES, and minilaparoscopy: analysis of a prospective clinical series. Surg Endosc. 2009;23:876–881. doi: 10.1007/s00464-008-0288-z. [DOI] [PubMed] [Google Scholar]
- 23.Palanivelu C, Rajan PS, Rangarajan M, Prasad M, Kalyanakumari V, Parthasarathi R, Senthilnathan P. NOTES: Transvaginal endoscopic cholecystectomy in humans-preliminary report of a case series. Am J Gastroenterol. 2009;104:843–847. doi: 10.1038/ajg.2009.1. [DOI] [PubMed] [Google Scholar]
- 24.Davila F, Tsin DA, Dominguez G, Davila U, Jesús R, Gomez de Arteche A. Transvaginal cholecystectomy without abdominal ports. JSLS. 2009;13:213–216. [PMC free article] [PubMed] [Google Scholar]
- 25.Rao GV, Reddy DN, Banerjee R. NOTES: human experience. Gastrointest Endosc Clin N Am. 2008;18:361–370; x. doi: 10.1016/j.giec.2008.01.007. [DOI] [PubMed] [Google Scholar]
- 26.Zorron R. Techniques of transvaginal access for NOTES. Tech Gastrointest Endosc. 2009;11:75–83. [Google Scholar]
- 27.Whiteford MH, Denk PM, Swanström LL. Feasibility of radical sigmoid colectomy performed as natural orifice translumenal endoscopic surgery (NOTES) using transanal endoscopic microsurgery. Surg Endosc. 2007;21:1870–1874. doi: 10.1007/s00464-007-9552-x. [DOI] [PubMed] [Google Scholar]
- 28.Palanivelu C, Rangarajan M, Jategaonkar PA, Anand NV. An innovative technique for colorectal specimen retrieval: a new era of "natural orifice specimen extraction" (N.O.S.E) Dis Colon Rectum. 2008;51:1120–1124. doi: 10.1007/s10350-008-9316-2. [DOI] [PubMed] [Google Scholar]
- 29.Lacy AM, Delgado S, Rojas OA, Almenara R, Blasi A, Llach J. MA-NOS radical sigmoidectomy: report of a transvaginal resection in the human. Surg Endosc. 2008;22:1717–1723. doi: 10.1007/s00464-008-9956-2. [DOI] [PubMed] [Google Scholar]
- 30.Burghardt J, Federlein M, Müller V, Benhidjeb T, Elling D, Gellert K. [Minimal invasive transvaginal right hemicolectomy: report of the first complex NOS (natural orifice surgery) bowels operation using a hybrid approach] Zentralbl Chir. 2008;133:574–576. doi: 10.1055/s-2008-1076992. [DOI] [PubMed] [Google Scholar]
- 31.Buess G, Kipfmüller K, Ibald R, Heintz A, Hack D, Braunstein S, Gabbert H, Junginger T. Clinical results of transanal endoscopic microsurgery. Surg Endosc. 1988;2:245–250. doi: 10.1007/BF00705331. [DOI] [PubMed] [Google Scholar]
- 32.Buess G, Becerra-Garcia F, Misra MC. Instruments for transluminal laparoscopic surgery or "NOTES". Minim Invasive Ther Allied Technol. 2008;17:331–335. doi: 10.1080/13645700802528041. [DOI] [PubMed] [Google Scholar]
- 33.Gavagan JA, Whiteford MH, Swanstrom LL. Full-thickness intraperitoneal excision by transanal endoscopic microsurgery does not increase short-term complications. Am J Surg. 2004;187:630–634. doi: 10.1016/j.amjsurg.2004.01.004. [DOI] [PubMed] [Google Scholar]
- 34.Sylla P, Willingham FF, Sohn DK, Gee D, Brugge WR, Rattner DW. NOTES rectosigmoid resection using transanal endoscopic microsurgery (TEM) with transgastric endoscopic assistance: a pilot study in swine. J Gastrointest Surg. 2008;12:1717–17123. doi: 10.1007/s11605-008-0637-1. [DOI] [PubMed] [Google Scholar]
- 35.Leroy J, Cahill RA, Perretta S, Forgione A, Dallemagne B, Marescaux J. Natural orifice translumenal endoscopic surgery (NOTES) applied totally to sigmoidectomy: an original technique with survival in a porcine model. Surg Endosc. 2009;23:24–30. doi: 10.1007/s00464-008-0102-y. [DOI] [PubMed] [Google Scholar]
- 36.Heald RJ, Husband EM, Ryall RD. The mesorectum in rectal cancer surgery--the clue to pelvic recurrence? Br J Surg. 1982;69:613–616. doi: 10.1002/bjs.1800691019. [DOI] [PubMed] [Google Scholar]
- 37.Lujan J, Valero G, Hernandez Q, Sanchez A, Frutos MD, Parrilla P. Randomized clinical trial comparing laparoscopic and open surgery in patients with rectal cancer. Br J Surg. 2009;96:982–989. doi: 10.1002/bjs.6662. [DOI] [PubMed] [Google Scholar]
- 38.Rattner D, Kalloo A. ASGE/SAGES Working Group on Natural Orifice Translumenal Endoscopic Surgery. October 2005. Surg Endosc. 2006;20:329–333. doi: 10.1007/s00464-005-3006-0. [DOI] [PubMed] [Google Scholar]
- 39.Kantsevoy SV. Infection prevention in NOTES. Gastrointest Endosc Clin N Am. 2008;18:291–296; ix. doi: 10.1016/j.giec.2008.01.004. [DOI] [PubMed] [Google Scholar]
- 40.Hazey JW, Narula VK, Renton DB, Reavis KM, Paul CM, Hinshaw KE, Muscarella P, Ellison EC, Melvin WS. Natural-orifice transgastric endoscopic peritoneoscopy in humans: Initial clinical trial. Surg Endosc. 2008;22:16–20. doi: 10.1007/s00464-007-9548-6. [DOI] [PubMed] [Google Scholar]
- 41.Zorrón R, Soldan M, Filgueiras M, Maggioni LC, Pombo L, Oliveira AL. NOTES: transvaginal for cancer diagnostic staging: preliminary clinical application. Surg Innov. 2008;15:161–165. doi: 10.1177/1553350608320553. [DOI] [PubMed] [Google Scholar]
- 42.Zorron R, Goncalves L, Leal D, Kanaan E, Cabral I, Saraiva P. Transvaginal hybrid natural orifice transluminal endoscopic surgery retroperitoneoscopy--the first human case report. J Endourol. 2010;24:233–237. doi: 10.1089/end.2009.0230. [DOI] [PubMed] [Google Scholar]