

Abstract
Clinical implementation and widespread application of natural orifice translumenal surgery (NOTES) has been limited by the lack of specialized endoscopic equipment, which has prevented the ability to perform complex procedures including colorectal resections. Relative to other types of translumenal access, transanal NOTES using transanal endoscopic microsurgery (TEM) provides a stable platform for endolumenal and direct translumenal access to the peritoneal cavity, and specifically to the colon and rectum. Completely NOTES transanal rectosigmoid resection using TEM, with or without transgastric endoscopic assistance, was demonstrated to be feasible and safe in a swine survival model. The same technique was successfully replicated in human cadavers using commercially available TEM, with endoscopic and laparoscopic instrumentation. This approach also permitted complete rectal mobilization with total mesorectal excision to be performed completely transanally. As in the swine model, transgastric and/or transanal endoscopic assistance extended the length of proximal colon mobilized and overcame some of the difficulties with TEM dissection including limited endoscopic visualization and maladapted instrumentation. This extensive laboratory experience with NOTES transanal rectosigmoid resection served as the basis for the first human NOTES transanal rectal cancer excision using TEM and laparoscopic assistance. Based on this early clinical experience, NOTES transanal approach using TEM holds significant promise as a safe and substantially less morbid alternative to conventional colorectal resection in the management of benign and malignant colorectal diseases. Careful patient selection and substantial improvement in NOTES instrumentation are critical to optimize this approach prior to widespread clinical application, and may ultimately permit completely NOTES transanal colorectal resection.
Keywords: Colorectal diseases, Transanal endoscopic microsurgery, Natural orifice translumenal endoscopic surgery
INTRODUCTION
Since the report of the first human transgastric endoscopic appendectomy in India in 2004, natural orifice translumenal surgery (NOTES) has represented the next step in the evolution of minimally invasive surgery since laparoscopy. Given the right translumenal route, endoscopic platform and instrumentation, surgical procedures ranging in complexity from cholecystectomy to colorectal resections could theoretically be performed entirely endoscopically without the need for abdominal incisions[1,2]. The advantages of such an approach include reduced incisional pain, decreased wound complications including infection and hernias, improved cosmetic results, and faster recovery and return to work. Until recently, endoscopic access to the abdominal cavity using transoral/transgastric route was the most intensely investigated type of translumenal access. However, this type of access has been hampered by difficulties in achieving easily reproducible and secure gastrotomy closure. Over the last few years, significant effort has been spent exploring alternate access routes such as transesophageal, transvaginal, transvesical and transcolonic/transanal access. Of all these approaches, transvaginal access has become the preferred type of access for NOTES procedures and has rapidly evolved from the experimental setting to human application with the first human cases described in 2007[3,4]. The international experience now counts several hundred cases of successfully performed hybrid transvaginal NOTES procedures including cholecystectomy, nephrectomy, and sleeve gastrectomy[5-9]. Access through and closure of the vagina is routinely performed by gynecologists, and when performed to access the peritoneal cavity for NOTES procedures, it is relatively safe. Downsides of this approach include the fact that it is restricted to female patients. The long-term effects of vaginal access have not yet been investigated.
ADVANTAGES OF TRANSCOLONIC/TRANSANAL NOTES ACCESS
Relative to other types of translumenal access, transcolonic/transanal NOTES has been described in few reports, mainly due to concerns related to fecal contamination of the abdominal cavity and the potential for infectious complications. The first reports described transcolonic peritoneoscopy[10,11] (n = 6) and cholecystectomy[12] (n = 5) in swine survival models with septic complications occurring in 1 animal (9%) following incomplete closure of the anterior colotomy[12]. Subsequent reports have described transcolonic surgical procedures of increasing complexity such as ventral hernia repair[13] and distal pancreatectomy[14] in survival swine models with good results. The cited advantages of the transrectal approach include the relative ease of colotomy creation and closure, and the ability to visualize abdominal organs in line with the endoscope without the need for retroflexion[13,14]. All authors agree that the viability of this approach relies on the adequacy of the colotomy closure, with the incidence of septic complications directly correlating with the integrity of the closure.
Another advantage of NOTES transcolonic/transanal access to the peritoneal cavity is the current availability of a specialized platform to perform endorectal and transrectal procedures. As described by Wilhelm et al[10], transcolonic peritoneoscopy is facilitated by the use of the transanal endoscopic microsurgery (TEM) platform through which specialized instruments can be introduced. TEM was first introduced in 1983 as a technique to excise mid- to high rectal adenomas not amenable to colonoscopic or transanal resection due to location, size, or risk of incomplete resection or colonic perforation. The platform consists of a 4-cm wide rigid beveled proctoscope sealed with a face plate with several air-tight ports through which an angled scope and adapted dissecting instruments can be inserted and CO2 insufflated to distend the rectum and create a working space. TEM permits precise endoscopic mucosal or full-thickness excision of mid- and high rectal lesions following which the rectal defect can be closed with a suturing device. It represents an attractive minimally invasive alternative to more radical resection of solitary rectal ulcers, adenomas and carcinoid tumors as well as early rectal cancers[15].
Based on series published over the past two decades, conversion rates to open surgery during TEM procedures have remained below 1% with a less than 5% incidence of major complications[16]. The latter include inadvertent entry into the peritoneal cavity during full-thickness excision of high rectal lesions located above the peritoneal reflection[17]. While this occurrence was originally considered a major complication of TEM and was managed by conversion to laparotomy in an effort to prevent intraabdominal infection[18], a study comparing the morbidity associated with full-thickness excision with and without peritoneal entry in 34 TEM full-thickness excisions demonstrated that in all 11 cases where the peritoneal cavity was inadvertently entered and subsequently closed, no infectious complications were noted[19]. In addition, no significant differences in the complication rates were noted between the groups with or without peritoneal entry[19]. These results strongly support the concept that purposeful entry into the peritoneal cavity during transcolonic/transanal NOTES procedures is safe, granted adequate closure of the enterotomy can be achieved.
Despite these findings, most surgeons remain significantly more reluctant to puncture the colon or rectum than the vagina to perform intraabdominal NOTES procedures. With regards to the applicability of NOTES in the field of colorectal surgery however, transcolonic/transanal access is intuitively better suited than other access routes. First, rather than creating an opening through an otherwise healthy organ to perform transgastric and transvaginal cholecystectomy, the enterotomy is created through the diseased organ itself. Second, the enterotomy created is ultimately closed by incorporating it into a standard colorectal anastomosis, which would be required regardless of whether the procedure was achieved via NOTES or standard surgery. Finally, a NOTES approach can be anticipated to have substantial benefits over a standard transabdominal approach. Despite significantly reducing incisional pain and recovery time relative to open surgery, standard and single port laparoscopic colorectal resections still require one or more sizeable abdominal incisions to exteriorize specimens, with various degrees of incisional pain and substantial incidence of short and long-term wound complications. Based on the published colorectal literature comparing outcomes following perineal proctosigmoidectomy vs abdominal approaches in the management of full-thickness rectal prolapse, perineal repair is associated with a higher incidence of recurrence but significantly less pain and peri- and postoperative morbidity[20]. Hence, the potential benefits of a transanal NOTES approach over standard colorectal resections can be extrapolated from this experience, particularly if a pure transanal endoscopic approach can be used.
TRANSCOLONIC/TRANSANAL NOTES COLORECTAL RESECTION: EXPERIMENTAL EVIDENCE
Radical sigmoidectomy using a pure NOTES transanal approach was first described in 3 human cadavers in 2007 by Whiteford et al[21] who used TEM as an endoscopic platform without the need for any abdominal incisions. Although adequate colon and mesenteric dissection could be achieved transanally, the authors were limited in the length of sigmoid colon that could be mobilized due to difficulties in overcoming the acute angle at the sacral promontory with TEM instrumentation. Based on this preliminary experience, a pure transanal NOTES approach to colorectal resection was further investigated in an experimental model using swine. In a pilot study using swine cadavers and non-survival animals, transanal endoscopic rectosigmoid resection using TEM could be replicated in that model[22]. Purse String closure of the distal rectum at the start of the procedures was effective at preventing fecal outflow and contamination during the procedure. Following full-thickness incision of the rectal wall, the presacral space could be entered and circumferential en-bloc resection of the rectosigmoid colon and its mesentery could be performed endoscopically. The peritoneal reflection was reached and the peritoneal cavity entered, and dissection of the sigmoid was continued proximally until further advancement of the proctoscope into the pelvis was limited by the narrow size of the swine pelvis. The colon was subsequently pulled out through the anus, transected, and stapled colorectal anastomosis was performed. In an attempt to overcome difficulties negotiating the sharp angle of the sacral promontory and narrow swine pelvis, dual transanal and transgastric endoscopic access was used to improve visualization, retraction, and mobilization of the proximal colon. Relative to a transanal approach alone, combined transgastric and transanal endoscopic dissection prolonged operative time but permitted additional length of sigmoid colon to be mobilized and resected transanally[22].
The safety of this NOTES approach was recently demonstrated in a 2-wk survival study using 20 swine that evaluated and compared outcomes of pure transanal endoscopic rectosigmoid resection versus combined transanal and transgastric rectosigmoid resection[23]. All procedures were completed successfully without transabdominal assistance and pneumoperitoneum was closely monitored and titrated intraoperatively using the CO2 insufflator connected to the TEM platform. There were no mortalities in either group and two major complications were noted at necropsy in the combined transanal/transgastric group which included an abdominal abscess and abdominal wall hematoma resulting from a T-tag misfire during gastrotomy closure. Again, combined transgastric and transanal endoscopic rectosigmoid mobilization was demonstrated to significantly prolong the operative time but extend the length of rectosigmoid mobilized transanally (Figure 1), where transgastric endoscopic assistance extended the average length of specimen mobilized by 54% and resected by 45% relative to a pure transanal NOTES approach[23]. All specimens resected were grossly intact with respect to the integrity of the colonic wall, attached mesentery and lymph nodes (Figure 1), which suggests that this approach could be a viable alternative to open or laparoscopic rectosigmoid resection in the clinical setting.
Figure 1.
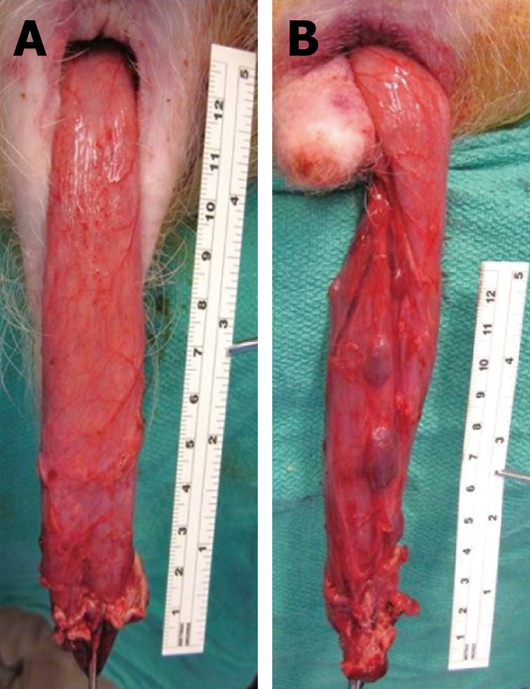
Transanal exteriorization of the rectosigmoid colon mobilized using transanal endoscopic microsurgery (TEM) only (A), and TEM with transgastric endoscopic assistance (B) in a swine survival model. Transgastric endoscopic assistance significantly increased the length of specimen that could be mobilized transanally.
An alternative NOTES approach to sigmoid resection that also combines transgastric and transcolonic access was described by Leroy et al[24] and shown to be both feasible and safe in a 2-wk survival study using 5 swine. Endolumenal access was used to retract the colon during transgastric endoscopic sigmoid dissection, and introduce the anvil of the circular stapler into the proximal colon. Transcolonic access was subsequently obtained to introduce an endoscopic linear stapler into the peritoneal cavity and divide the colon. Of note, a transabdominal Berci needle (2.7 mm) was still required to establish and monitor pneumoperitoneum and to assist with anvil positioning during completion of the intracorporeal stapled anastomosis[24].
TRANSCOLONIC/TRANSANAL NOTES COLORECTAL RESECTION: TRANSITIONING TO CLINICAL PRACTICE
In preparation for transitioning to human application, the same completely NOTES approach described in swine
was successfully replicated in human cadavers using commercially available TEM, laparoscopic and NOTES instrumentation. In a series of 7 male and female cadavers, our group demonstrated that transanal NOTES rectosigmoid resection could be achieved using the same steps as described in swine, with the added benefit of being able to complete a totally endoscopic mesorectal excision transanally with TEM[25]. Circumferential dissection of the rectum was initiated at the level of the anorectal ring, above the anal sphincter complex, and posterior entry into the presacral space with mesorectal dissection was greatly facilitated by CO2 insufflation and the use of flexible instruments (Figure 2A). Following posterior and lateral dissection of the rectum and mesorectum, the peritoneal reflection was divided after carefully mobilizing the posterior vagina or prostate from the anterior rectal wall (Figure 2B). Once the peritoneal cavity was entered, more cephalad colon mobilization required longer and more flexible optics and instruments to improve visualization of pelvic and abdominal structures and provide effective bowel retraction, tissue manipulation, vascular division and hemostasis respectively.
Figure 2.
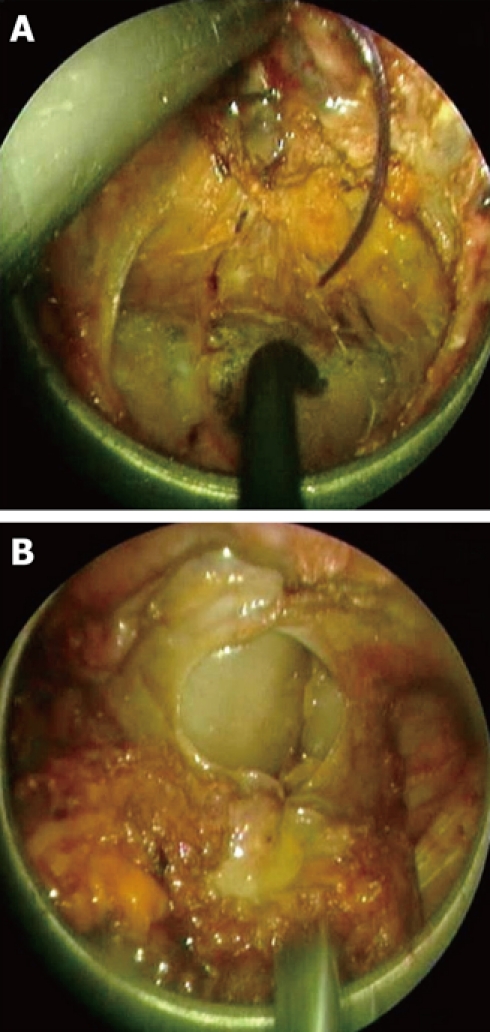
Transanal endoscopic rectal dissection using TEM in a male human cadaver. A: Following full-thickness transection of the rectal wall, the presacral plane was entered posteriorly and total mesorectal excision was completed; B: Following mobilization of the anterior rectal wall from the posterior aspect of the prostate, the peritoneal cavity was entered.
Commercially available TEM, laparoscopic, single-port and endoscopic instrumentation is currently maladapted for this type of NOTES approach and is the major limiting factor for achieving more proximal colon mobilization and splenic flexure takedown transanally. Combining transgastric and/or transanal endoscopic assistance by inserting flexible endoscopes through a gastrotomy and/or the TEM faceplate, was found to overcome some of those technical limitations by improving endoscopic visualization and assisting with endoscopic dissection (Figure 3). Overall, the average length of rectosigmoid colon mobilized transanally in this series of 7 human cadavers was 38.7 cm (range, 15-75 cm, Figure 4)[25]. Other important technical limitations encountered with this approach in this model include morbid obesity and adhesions from prior abdominal or pelvic surgery. Both factors were found to markedly increase the difficulty of the dissection, risk of bowel perforation, and limit the proximal extent of colon mobilized[25].
Figure 3.

Transanal endoscopic mobilization of the rectosigmoid colon using TEM with combined transgastric endoscopic assistance in a human cadaver. A double channel colonoscope was inserted transgastrically and used to help dissect the peritoneal attachments of the sigmoid colon.
Figure 4.

Specimen exteriorization following transanal endoscopic mobilization of the rectosigmoid colon using TEM in a male human cadaver. Total mesorectal excision and sigmoid mesenteric dissection could be achieved.
Although the experimental experience described has demonstrated that transgastric access and gastrotomy closure using T-tags is feasible and safe in a survival study in swine, the consensus remains that until significant technological improvements are made to standardize techniques for and ensure safety of gastrotomy closure, early clinical application of NOTES rectosigmoid resection should employ either pure transanal endoscopic access or a hybrid approach with laparoscopic assistance. This will ensure that the procedures are performed safely, are technically easier to perform during the steep portion of the learning curve, and simpler to standardize for potential widespread application. In addition, all NOTES colorectal procedures should be performed under IRB protocol at centers with experience with NOTES and TEM.
TRANSCOLONIC/TRANSANAL NOTES: HUMAN EXPERIENCE
In addition to the growing international experience with single-port laparoscopic colorectal resection, laparoscopic colorectal resection using transrectal assistance, where transrectal access is used for specimen extraction[26], insertion of the anvil of a circular stapler for intracorporeal double-stapled anastomosis[27,28], or both[29] has been described. Transvaginal access has also been used as an extraction site following colorectal resection[30] as well part of a hybrid NOTES laparoscopic rectosigmoid dissection[31] where significant portions of the dissection are performed transvaginally.
A pure NOTES approach to colorectal resection, either using transvaginal or transanal/transcolonic access, has not been reported to date. However, the first clinical case of a NOTES transanal resection for rectal cancer using TEM and laparoscopic assistance was just recently performed at the Hospital Clinic in Barcelona[32]. After obtaining institutional review board approval, transanal endoscopic rectal resection with total mesorectal excision using the TEM platform was performed in a 76-year-old female with a T2N1 mid-rectal cancer treated with preoperative chemoradiation. Laparoscopic visualization and assistance with retraction and exposure during rectosigmoid mobilization was provided through one 5-mm right lower quadrant port which was later used as the stoma site for a diverting loop ileostomy and two 2-mm needle ports, one of which was later used as a drain site. The specimen was transected transanally followed by hand-sewn coloanal anastomosis. The total procedure time was under 5 h, the patient’s recovery was uneventful, and she was discharged on the fifth postoperative day. The final pathology demonstrated a ypT1N0 tumor with intact mesorectum that included 23 negative lymph nodes and negative proximal, distal and radial margins[32].
TRANSCOLONIC/TRANSANAL NOTES COLORECTAL RESECTION: FUTURE DIRECTIONS
Based on this first clinical report, NOTES transanal endoscopic rectal cancer resection using TEM appears to be feasible and safe in the clinical setting. Careful patient selection with respect to pathology and patient characteristics will be critical for the technical success of these procedures. Major rate-limiting factors in the widespread applicability of this approach include: (1) the lack of specialized equipment required to perform transanal NOTES procedures; and (2) experience with TEM and advanced endoscopic skills. Until substantial improvement in NOTES instrumentation is made to optimize this approach, these procedures should be completed under laparoscopic assistance.
With respect to indications for transanal NOTES procedures, this approach is an attractive minimally invasive alternative for the management of benign and pre-malignant lesions of the rectum and sigmoid colon such as large unresectable polyps, dysplastic lesions, and resectable cancers of the rectum. Complete or partial mesorectal excision with lymph node sampling can be achieved, which is a significant advantage relative to transanal local excisions and TEM. Because this approach involves initial full-thickness circumferential rectal and mesorectal dissection starting 4-5 cm from the anal verge, patients selected for this approach should have clear indications for low anterior resection with a low colorectal anastomosis, which is associated with a worse functional outcome than if the rectum was preserved. This is particularly important when evaluating patients with benign pathology. The potential deleterious effect of prolonged placement of the 4-cm wide TEM platform on anal sphincter function and fecal continence will also need to be investigated. With respect to potential oncologic applications of this approach in rectal cancer, although our experience with human cadavers and this first clinical case demonstrate that an adequate oncologic rectal resection can be achieved, the long-term oncologic outcomes of this approach, in terms of local recurrence and survival, need to be formally evaluated. Until such results are available, this approach for rectal cancer should be considered investigational and be performed under IRB protocol by colorectal surgeons with extensive NOTES and TEM experience.
CONCLUSION
Review of the experimental evidence to date suggests that completely NOTES rectosigmoid resection using transanal access with TEM with or without transgastric endoscopic assistance, is feasible and safe. The importance of developing better adapted tools such as a modified flexible transanal endoscopic platform, longer and more flexible dissecting instruments, and staplers and hemostatic devices to permit safe completion of these procedures without the need for transabdominal assistance is critical. As demonstrated with the clinical case of NOTES transanal rectal cancer resection using TEM, laparoscopic assistance is currently needed to compensate for the limitations in NOTES instrumentations and to ensure safety. Based on this preliminary clinical experience, NOTES transanal approach with TEM has significant potential applications in the treatment of both benign and malignant colorectal diseases, as well as potential advantages over conventional colorectal resection. With respect to oncologic applications, careful patient selection is critical and oncologic outcomes will need to be followed closely.
Footnotes
Peer reviewers: Wai Lun Law, MS, FRCS, FACS, Professor, Chief, Division of Colorectal Surgery, Queen Mary Hospital, The University of Hong Kong, Pokfulam Road, Hong Kong, China; Marcus Vinicius Motta Valadão, MD, Instituto Nacional de Câncer, Hospital do Cancêr Unidade I, Hc2., Rua do Equador 831, Santo Cristo, Rio de Janeiro 20220-410, RJ, Brasil
S- Editor Li LF L- Editor Hughes D E- Editor Yang C
References
- 1.Rattner D, Kalloo A. ASGE/SAGES Working Group on Natural Orifice Translumenal Endoscopic Surgery. October 2005. Surg Endosc. 2006;20:329–333. doi: 10.1007/s00464-005-3006-0. [DOI] [PubMed] [Google Scholar]
- 2.ASGE , SAGES ASGE/SAGES Working Group on Natural Orifice Translumenal Endoscopic Surgery White Paper October 2005. Gastrointest Endosc. 2006;63:199–203. doi: 10.1016/j.gie.2005.12.007. [DOI] [PubMed] [Google Scholar]
- 3.Marescaux J, Dallemagne B, Perretta S, Wattiez A, Mutter D, Coumaros D. Surgery without scars: report of transluminal cholecystectomy in a human being. Arch Surg. 2007;142:823–826; discussion 826-827. doi: 10.1001/archsurg.142.9.823. [DOI] [PubMed] [Google Scholar]
- 4.Bessler M, Stevens PD, Milone L, Parikh M, Fowler D. Transvaginal laparoscopically assisted endoscopic cholecystectomy: a hybrid approach to natural orifice surgery. Gastrointest Endosc. 2007;66:1243–1245. doi: 10.1016/j.gie.2007.08.017. [DOI] [PubMed] [Google Scholar]
- 5.Ramos AC, Zundel N, Neto MG, Maalouf M. Human hybrid NOTES transvaginal sleeve gastrectomy: initial experience. Surg Obes Relat Dis. 2008;4:660–663. doi: 10.1016/j.soard.2008.06.009. [DOI] [PubMed] [Google Scholar]
- 6.Zorron R, Maggioni LC, Pombo L, Oliveira AL, Carvalho GL, Filgueiras M. NOTES transvaginal cholecystectomy: preliminary clinical application. Surg Endosc. 2008;22:542–547. doi: 10.1007/s00464-007-9646-5. [DOI] [PubMed] [Google Scholar]
- 7.Gumbs AA, Fowler D, Milone L, Evanko JC, Ude AO, Stevens P, Bessler M. Transvaginal natural orifice translumenal endoscopic surgery cholecystectomy: early evolution of the technique. Ann Surg. 2009;249:908–912. doi: 10.1097/SLA.0b013e3181a802e2. [DOI] [PubMed] [Google Scholar]
- 8.Horgan S, Cullen JP, Talamini MA, Mintz Y, Ferreres A, Jacobsen GR, Sandler B, Bosia J, Savides T, Easter DW, et al. Natural orifice surgery: initial clinical experience. Surg Endosc. 2009;23:1512–1518. doi: 10.1007/s00464-009-0428-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Salinas G, Saavedra L, Agurto H, Quispe R, Ramírez E, Grande J, Tamayo J, Sánchez V, Málaga D, Marks JM. Early experience in human hybrid transgastric and transvaginal endoscopic cholecystectomy. Surg Endosc. 2010;24:1092–1098. doi: 10.1007/s00464-009-0733-7. [DOI] [PubMed] [Google Scholar]
- 10.Wilhelm D, Meining A, von Delius S, Fiolka A, Can S, Hann von Weyhern C, Schneider A, Feussner H. An innovative, safe and sterile sigmoid access (ISSA) for NOTES. Endoscopy. 2007;39:401–406. doi: 10.1055/s-2007-966438. [DOI] [PubMed] [Google Scholar]
- 11.Fong DG, Pai RD, Thompson CC. Transcolonic endoscopic abdominal exploration: a NOTES survival study in a porcine model. Gastrointest Endosc. 2007;65:312–318. doi: 10.1016/j.gie.2006.08.005. [DOI] [PubMed] [Google Scholar]
- 12.Pai RD, Fong DG, Bundga ME, Odze RD, Rattner DW, Thompson CC. Transcolonic endoscopic cholecystectomy: a NOTES survival study in a porcine model (with video) Gastrointest Endosc. 2006;64:428–434. doi: 10.1016/j.gie.2006.06.079. [DOI] [PubMed] [Google Scholar]
- 13.Fong DG, Ryou M, Pai RD, Tavakkolizadeh A, Rattner DW, Thompson CC. Transcolonic ventral wall hernia mesh fixation in a porcine model. Endoscopy. 2007;39:865–869. doi: 10.1055/s-2007-966916. [DOI] [PubMed] [Google Scholar]
- 14.Ryou M, Fong DG, Pai RD, Tavakkolizadeh A, Rattner DW, Thompson CC. Dual-port distal pancreatectomy using a prototype endoscope and endoscopic stapler: a natural orifice transluminal endoscopic surgery (NOTES) survival study in a porcine model. Endoscopy. 2007;39:881–887. doi: 10.1055/s-2007-966908. [DOI] [PubMed] [Google Scholar]
- 15.Cataldo PA. Transanal endoscopic microsurgery. Surg Clin North Am. 2006;86:915–925. doi: 10.1016/j.suc.2006.06.004. [DOI] [PubMed] [Google Scholar]
- 16.Swanstrom L. Transanal endoscopic microsurgery: current indications and techniques. J Gastrointest Surg. 2000;4:342–343. doi: 10.1016/s1091-255x(00)80007-4. [DOI] [PubMed] [Google Scholar]
- 17.de Graaf EJ, Doornebosch PG, Stassen LP, Debets JM, Tetteroo GW, Hop WC. Transanal endoscopic microsurgery for rectal cancer. Eur J Cancer. 2002;38:904–910. doi: 10.1016/s0959-8049(02)00050-3. [DOI] [PubMed] [Google Scholar]
- 18.Smith LE, Ko ST, Saclarides T, Caushaj P, Orkin BA, Khanduja KS. Transanal endoscopic microsurgery. Initial registry results. Dis Colon Rectum. 1996;39:S79–S84. doi: 10.1007/BF02053811. [DOI] [PubMed] [Google Scholar]
- 19.Gavagan JA, Whiteford MH, Swanstrom LL. Full-thickness intraperitoneal excision by transanal endoscopic microsurgery does not increase short-term complications. Am J Surg. 2004;187:630–634. doi: 10.1016/j.amjsurg.2004.01.004. [DOI] [PubMed] [Google Scholar]
- 20.Tou S, Brown SR, Malik AI, Nelson RL. Surgery for complete rectal prolapse in adults. Cochrane Database Syst Rev. 2008:CD001758. doi: 10.1002/14651858.CD001758.pub2. [DOI] [PubMed] [Google Scholar]
- 21.Whiteford MH, Denk PM, Swanström LL. Feasibility of radical sigmoid colectomy performed as natural orifice translumenal endoscopic surgery (NOTES) using transanal endoscopic microsurgery. Surg Endosc. 2007;21:1870–1874. doi: 10.1007/s00464-007-9552-x. [DOI] [PubMed] [Google Scholar]
- 22.Sylla P, Willingham FF, Sohn DK, Gee D, Brugge WR, Rattner DW. NOTES rectosigmoid resection using transanal endoscopic microsurgery (TEM) with transgastric endoscopic assistance: a pilot study in swine. J Gastrointest Surg. 2008;12:1717–1723. doi: 10.1007/s11605-008-0637-1. [DOI] [PubMed] [Google Scholar]
- 23.Sylla P, Sohn DK, Cizginer S, Konuk Y, Turner BG, Gee DW, Willingham FF, Hsu M, Mino-Kenudson M, Brugge WR, et al. Survival study of natural orifice translumenal endoscopic surgery for rectosigmoid resection using transanal endoscopic microsurgery with or without transgastric endoscopic assistance in a swine model. Surg Endosc. 2010:Epub ahead of print. doi: 10.1007/s00464-010-0898-0. [DOI] [PubMed] [Google Scholar]
- 24.Leroy J, Cahill RA, Perretta S, Forgione A, Dallemagne B, Marescaux J. Natural orifice translumenal endoscopic surgery (NOTES) applied totally to sigmoidectomy: an original technique with survival in a porcine model. Surg Endosc. 2009;23:24–30. doi: 10.1007/s00464-008-0102-y. [DOI] [PubMed] [Google Scholar]
- 25.Sylla P, Kim MC, Dursun A, Sohn DK, Ajari I, Konuk Y, Turner BG, Gee D, Brugge WR, Rattner DW. Completely NOTES rectosigmoid resection using Transanal Endoscopic Microsurgery (TEM): Experience in human cadavers. Poster presentation at the ASCRS meeting; 2010 May; Minneapolis, USA [Google Scholar]
- 26.Franklin ME, Kazantsev GB, Abrego D, Diaz-E JA, Balli J, Glass JL. Laparoscopic surgery for stage III colon cancer: long-term follow-up. Surg Endosc. 2000;14:612–616. doi: 10.1007/s004640000169. [DOI] [PubMed] [Google Scholar]
- 27.Cheung HY, Leung AL, Chung CC, Ng DC, Li MK. Endo-laparoscopic colectomy without mini-laparotomy for left-sided colonic tumors. World J Surg. 2009;33:1287–1291. doi: 10.1007/s00268-009-0006-6. [DOI] [PubMed] [Google Scholar]
- 28.Leroy J, Cahill RA, Asakuma M, Dallemagne B, Marescaux J. Single-access laparoscopic sigmoidectomy as definitive surgical management of prior diverticulitis in a human patient. Arch Surg. 2009;144:173–179; discussion 179. doi: 10.1001/archsurg.2008.562. [DOI] [PubMed] [Google Scholar]
- 29.Akamatsu H, Omori T, Oyama T, Tori M, Ueshima S, Nakahara M, Abe T, Nishida T. Totally laparoscopic sigmoid colectomy: a simple and safe technique for intracorporeal anastomosis. Surg Endosc. 2009;23:2605–2609. doi: 10.1007/s00464-009-0406-6. [DOI] [PubMed] [Google Scholar]
- 30.Franklin ME Jr, Kelley H, Kelley M, Brestan L, Portillo G, Torres J. Transvaginal extraction of the specimen after total laparoscopic right hemicolectomy with intracorporeal anastomosis. Surg Laparosc Endosc Percutan Tech. 2008;18:294–298. doi: 10.1097/SLE.0b013e3181772d8b. [DOI] [PubMed] [Google Scholar]
- 31.Lacy AM, Delgado S, Rojas OA, Almenara R, Blasi A, Llach J. MA-NOS radical sigmoidectomy: report of a transvaginal resection in the human. Surg Endosc. 2008;22:1717–1723. doi: 10.1007/s00464-008-9956-2. [DOI] [PubMed] [Google Scholar]
- 32.Sylla P, Rattner DW, Delgado S, Lacy AM. NOTES transanal rectal cancer resection using transanal endoscopic microsurgery and laparoscopic assistance. Surg Endosc. 2010;24:1205–1210. doi: 10.1007/s00464-010-0965-6. [DOI] [PubMed] [Google Scholar]