

Abstract
Volvulus of transverse colon is a rare cause of large bowel obstruction. To our knowledge only 75 cases have been reported in the world literature and additionally only three cases of transverse colon volvulus with Chilaiditis syndrome have been reported to date. Because of its rarity here we report a case of transverse colon volvulus which was indeed associated with Chilaiditis syndrome. This is probably the fourth case of Chilaiditis syndrome caused by transverse colon volvulus.
Electronic supplementary material
The online version of this article (doi:10.1007/s12262-010-0130-4) contains supplementary material, which is available to authorized users.
Keywords: Transverse colon volvulus, Chilaiditis syndrome
Introduction
A volvulus is a twisting or axial rotation of a portion of bowel about its mesentery. Volvulus may be primary or secondary. A secondary volvulus is more common variety which occurs due to actual rotation of a piece of bowel around an acquired adhesion or stoma[1].Any portion of large bowel can torse if that segment is attached to a long and floppy mesentery that is fixed to the retro peritoneum by a narrow base of origin. The condition most commonly affects the colon [2]. Females seem to be affected more frequently than males and occasional cases in childhood have been recorded. Clinical features are indistinguishable from other causes of large bowel obstruction and radiological features are frequently misleading leading to difficulty in diagnosis of the condition preoperatively [3].
Case Report
A 27 years old male patient (mentally challenged) presented with severe abdominal pain, vomiting, distension and constipation since 1 day. Abdominal examination revealed distension, tenderness all over the abdomen with absent bowel sounds. Plain abdominal radiograph showed evidence of large bowel obstruction with Chilaiditis sign (Fig. 1). As it was acute situation gastrograffin enema was not done and patient was posted for emergency exploratory laparotomy.
Fig. 1.
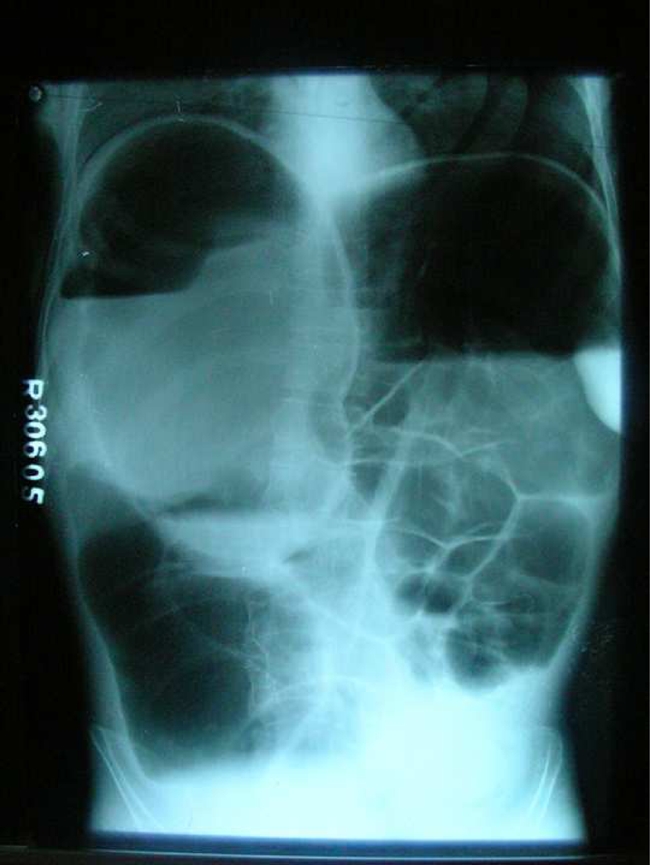
Photograph shows plain x-ray abdomen s/o large bowel obstruction with chilaiditis sign
On opening the abdomen volvulus of transverse colon with ischaemic necrosis was evident (Fig. 2). The area of ischaemia was limited to transverse colon but the ascending colon and caecum were markedly distended (Fig. 3). Rest of small and large bowel was normal and collapsed (Fig. 4). Considering the possibility of post operative anastomotic leakage decision was taken to resect the gangrenous segment of transverse colon and exteriorize both ends of colon, the ascending colon as an end colostomy and the proximal descending colon as a mucous fistula. Recovery was uneventful.
Fig. 2.

Photograph shows volvulus of transverse colon (Anticlockwise twist) with ischaemic necrosis
Fig. 3.

Photograph shows dilated caecum and collapsed terminal ileum (closed loop obstruction)
Fig. 4.

Photograph shows normal collapsed sigmoid colon holded with Babcock’s clamps
Discussion
Colonic volvulus is a well recognized cause of large bowel obstruction [4]. Volvulus of transverse colon is extremely rare its incidence being approximately 3% of all colonic volvulus [2, 3]. It tends to be associated with other abnormalities such as congenital bands, distal obstructing lesions and pregnancy [3]. Non-fixation of colon and chronic constipation with megacolon may predispose to transverse colon volvulus [5]. The mortality rate of transverse colon volvulus is 33% [4].
Chilaiditis sign is the description applied to the radiographic finding of the colon, typically the hepatic flexure, interposed between the liver and diaphragm falsely imitating pneumoperitoneum [6]. Chilaiditis sign is usually an incidental finding and most of these patients lack any clinical symptomatology. However Chilaiditis syndrome describes radiological evidence of Chilaiditis sign in addition to the symptoms of abdominal pain, nausea, vomiting, abdominal distension and constipation. Common etiologies for both Chilaiditis sign and Chilaiditis syndrome include increased colonic mobility or redundancy, congenital malrotation or malposition of colon, elevation of the right hemidiaphragm, enlargement of thoracic cage diameter and floating liver found in ascites [4].
Two separate clinical presentations have been described in the literature for transverse colon volvulus, acute fulminating and subacute progressive. Acute presentation typically has a sudden onset of severe abdominal pain, tenderness, vomiting, and little distension and rapid clinical deterioration. Vomiting is thought to occur earlier which may be due to twisting of the root of the mesocolon compressing the duodenojejunal flexure. Bowel sounds are initially hyperacute but later may become absent. Patient with subacute form has more gradual and intermittent onset of symptoms. Abdominal pain is less severe or often absent and distension is often more prominent [4].
Diagnosis of transverse colon volvulus is usually not made preoperatively. The radiologic findings are not really characteristic [7]. Plain abdominal radiographs show nonspecific colonic dilation and are frequently misread as a sigmoid volvulus due to variable position of the transverse colon [7]. The classic “birds beak” deformity in the area of transverse colon seen on contrast enema is diagnostic. However in acute situation surgery should not be delayed to perform the contrast study. Chilaiditis syndrome does not appear to be significant in diagnosing transverse colon volvulus but rather occurs as an occasional side effect [4].
Resection with or without primary anastomosis is the treatment of choice for transverse colon volvulus to prevent recurrence [4]. If there is ischaemic necrosis of colon two ends of resected colon should be exteriorized [3]. Successful decompression by means of the colonoscope has been recently described [7]. Because of rarity limited data is available regarding long term results following surgical treatment [8]. Uptill now the studies which are carried out there are no universal agreement that a particular surgical treatment option is superior to other. But there is equivocal agreement on increased recurrence following colopexy alone.
Electronic Supplementary Material
(PDF 28.4 kb)
References
- 1.Winslet MC. Intestinal obstruction. Bailey & love’s short practice of surgery. London: Arnold; 2008. p. 1191. [Google Scholar]
- 2.Fry RD, Mahmoud N, Maron DJ, Ross HM, Rombeau J. Colon and rectum. Sabiston textbook of surgery. Philadelphia: Saunders Elsevier; 2008. p. 1369. [Google Scholar]
- 3.Williams NS. Large bowel obstruction. Surgery of the anus, rectum and colon. London: W. B. SAUNDERS; 1993. p. 1852. [Google Scholar]
- 4.Ciraldo A, Thomas D, Schmidt S (2000) A case report: transverse colon volvulus associated with chilaiditis syndrome. The Internet J Gastroenterol 1(1)
- 5.Bullard KM, Rothenberger DA (2005) Colon, rectum and anus. Schwartz’s Principles of surgery. McGraw-Hill, p 1099
- 6.Plorde JJ, Raker EJ. Transverse colon volvulus and associated chilaiditis syndrome; case report and literature review. Am J Gastroentrol. 1996;91(12):2613–6. [PubMed] [Google Scholar]
- 7.Corman ML. Miscellaneous colon and rectal conditions. Colon and rectal surgery. Philadelphia: J. B. Lippincott Company; 1984. p. 715. [Google Scholar]
- 8.Boushey RP, Schoetz DJ., Jr . Colonic intussusception and volvulus. Shackelford’s surgery of the alimentary tract. Philadelphia: Saunders Elsevier; 2007. p. 1985. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
(PDF 28.4 kb)