

Abstract
Background
Tibial stress fractures, which are among the most common running related injuries, have been associated with increased lower extremity loading (i.e., peak positive acceleration of the tibia, vertical force impact peak, and average and instantaneous vertical force loading rates) during initial contact. This study was conducted to evaluate the efficacy of a gait retraining program designed to reduce this loading during running and to assess the short-term persistence of these reductions.
Methods
Ten runners (six females and four males) with peak positive tibial acceleration greater than 8 g, measured in an initial screening, participated in the retraining program. During the retraining sessions, subjects ran on a treadmill and received real-time visual feedback from an accelerometer attached to their distal tibias. Tibial acceleration and vertical ground reaction force data were collected from subjects during overground data collection sessions held pre-training, post-training, and at a 1-month follow-up.
Findings
Peak positive acceleration of the tibia, vertical force impact peak, and average and instantaneous vertical force loading rates were all reduced immediately following the gait retraining. The decrease in tibial acceleration was nearly 50%. The reductions in vertical force loading rates and vertical force impact peak were approximately 30% and 20%, respectively. These reductions were maintained at the 1-month follow-up.
Interpretation
Subjects were able to run with reduced tibial acceleration and vertical force loading immediately following completion of the gait retraining program and at the 1-month follow-up evaluation. This may reduce their risk of stress fractures.
Keywords: Feedback, Loading rate, Stress fracture, Tibial acceleration
1. Introduction
Tibial stress fractures are among the top 10 overuse injuries that civilian runners and military recruits sustain (Taunton et al., 2002; Rauh et al., 2006). In addition, the recurrence rate for stress fractures ranges from 10.6% (Milgrom et al., 1985) to 36% (Hauret et al., 2001) for military recruits. Stress fractures are also among the most serious of overuse injuries as one must refrain from running and other impact related activities during the recovery time, which averages 8 weeks (Beck, 1998; Bennell and Brukner, 2005). An 8-week period of reduced training has been shown to result in significant decrements in cardiovascular and muscular function (Coyle et al., 1984; Coyle et al., 1985). For the US military, stress fractures pose an additional burden because of the costs involved. Hauret et al., (2001) reported that in one year, 86 of 222 Army recruits (39%) who sustained just a single stress fracture during basic combat training (BCT) at Fort Jackson, SC were discharged. Since only half of all Army recruits who attended BCT were trained at Fort Jackson that year, it can be estimated that at least 172 recruits are discharged per year because of stress fractures. The cost for recruitment and BCT is $36,000 per recruit (United States General Accounting Office, 1998). Therefore, stress fractures cost the Army at least $6.2 M per year. This estimate does not include the cost of medical treatment and rehabilitation, and it does not account for recruits with multiple stress fractures who were discharged. In addition, it only considers stress fractures sustained during BCT for enlisted Soldiers. Thus, the total cost of stress fractures to the military (Army, Navy, Air Force, Marines, and Coast Guard) is probably tens of millions of dollars.
There are many factors associated with the development of stress fractures. These include such things as training regimen, fitness, running surface, and diet (Jones et al., 2002; Pepper et al., 2006). Studies also suggest that running mechanics are a risk factor for stress fractures. In a preliminary, prospective report by Davis et al. (2004), runners who developed tibial stress fractures or tibial stress reactions (a precursor to tibial stress fractures (Jones et al., 1989; Anderson and Greenspan, 1996)) had higher peak positive acceleration of the tibia and higher average and instantaneous vertical ground reaction force loading rates than a group of age and mileage matched control subjects. Similarly, in a retrospective study, subjects who had sustained a stress fracture had higher average peak positive acceleration of the tibia. These subjects also had higher average and instantaneous vertical ground reaction force loading rates than a group of age and mileage matched control subjects. In addition, there was a trend toward higher impact peak in the group that had a stress fracture compared to the control group (Milner et al., 2006a). In other studies, free moment (Milner et al., 2006b; Pohl et al., 2008) and angle of the vertical ground reaction force vector in the frontal plane (Creaby and Dixon, 2008) were also associated with the occurrence of tibial stress fractures. These variables all influence the loading of the lower extremity. Therefore, modifying these loading mechanics may decrease a runner’s risk for stress fractures.
The idea of altering the mechanics of locomotion is not new. Gait retraining, using real-time feedback has been used successfully to alter loading mechanics in a number of conditions. Limb-load monitors, which measure the forces under the feet, have been used to improve walking symmetry in children with cerebral palsy (Seeger et al., 1981) and adults with fractures, amputations, total hip replacements, and chronic pain (Gapsis et al., 1982). Real-time feedback from instrumented treadmills has helped trans-tibial amputees (Dingwell et al., 1996) and individuals with total hip replacements (White and Lifeso, 2005) to improve their symmetry of loading. Real-time feedback of tibial acceleration has been used by subjects in a study to reduce the loading on their lower extremities for a short period of time (Crowell et al., 2010).
While it appears that gait mechanics can be altered through training, these changes will not be meaningful unless they persist beyond the training sessions. Motor learning occurs through practice such that the motor skill being practiced becomes a permanent capability (Lee and Schmidt, 2008). The retention of a motor skill beyond the training is an indication that learning has occurred (Salmoni et al., 1984). Seeger and colleagues (1981) reported that improvements in gait symmetry attained through retraining were retained at a 1-month follow-up. However, most of the gait retraining studies, to date, have not re-assessed mechanics beyond the end of the training.
In addition to practice, motor skill learning is influenced by the type of feedback provided (Swinnen et al., 1990; Winstein and Schmidt, 1990; Doyon et al., 2003; Korman et al., 2003). For example, feedback should be gradually removed so that the individual learns to rely on internal cues. This has been shown to facilitate the learning process and improve the persistence of the motor pattern (Winstein, 1991). Therefore, gait retraining that includes multiple practice sessions in which feedback is gradually removed may result in persistence of gait changes.
The current study builds on the results of the single-session retraining study conducted by Crowell et al. (2010). The purpose of this study was to examine the efficacy of a gait retraining program that included multiple sessions in which the amount of feedback was gradually reduced. This retraining program was designed to reduce tibial acceleration and lower extremity loading during early stance. We hypothesized that peak positive acceleration, vertical force loading rates, and vertical force impact peak would be reduced following the retraining program and that these changes would persist at a 1-month follow-up.
2. Methods
2.1. Subjects
An a priori power analysis was conducted with the program GPOWER (Faul and Erdfelder, 1992) to determine the sample size needed to examine the efficacy of the gait retraining program. Based on preliminary data for the primary variables of interest, (peak positive acceleration and instantaneous loading rate), α = 0.05, and power of 0.8, ten subjects were needed to adequately power the study. We recruited athletes from the University of Delaware along with recreational runners from the university and the surrounding area to participate in this study. To qualify for the study, subjects had to be rearfoot strikers, running at least 16 km per week. They also had to be free of injuries or other conditions that would affect their gait. In addition, they had to undergo an initial screening to determine if their tibial acceleration was above normal when they ran.
2.2. Initial Screening
Before participating, each subject read and signed an informed consent form approved by the Human Subjects Review Board at the University of Delaware. During the initial screening, the subject’s right and left sides were tested separately. A lightweight accelerometer (model 356A32, measurement range: ± 50 g, mass: 5.4 gram, PCB Piezotronics, Inc., Depew, NY, USA) was aligned with the long axis of the subject’s tibia, and it was securely taped to the anteromedial aspect of the distal tibia (Figure 1). Subjects wore standard, neutral running shoes (Air Pegasus, Nike, Inc., Beverton, OR, USA) during the screening and all subsequent data collections. They ran at 3.7 m/s (±5%) across a force plate (Bertec Corp, Worthington, OH, USA) located in the center of a 23 meter runway. Accelerometer and ground reaction force data were sampled at 1080 Hz. A custom program written in LabVIEW™ (National Instruments, Austin, TX, USA) was used to process the data. A second order, recursive, Butterworth, lowpass filter was used to filter the force plate data at 50 Hz. A threshold of 10 N in the vertical ground reaction force was used to determine foot strike and toe off. The accelerometer data were filtered at 75 HZ with a second order, recursive, Butterworth, lowpass filter. Any offset in the signal was removed by subtracting the average of the signal. The peak positive tibial acceleration during stance phase was then identified. Any subjects with peak positive tibial acceleration greater than 8 g were invited into the retraining study. This value of tibial acceleration was one standard deviation above the mean of 171 uninjured runners from an ongoing study being conducted in the Motion Analysis Laboratory at the University of Delaware.
Fig. 1.

Accelerometer taped to the anteromedial aspect of the subject’s distal tibia.
The first ten subjects who met the screening criteria and agreed to participate were entered into the retraining phase of the study. These included six females and four males who were, on average, 26 (SD 7) years old, 1.72 (SD 0.07) m tall, and weighed 81.5 (SD 21) kg. In the case of bilateral elevation of tibial acceleration, the leg with the highest value was addressed in the retraining.
2.3. Pre-training Data Collection
A pre-training instrumented gait analysis was conducted. Tibial acceleration and ground reaction forces were collected as described in the screening. In addition, kinematic data were collected with a Vicon motion capture system (Vicon, Oxford, UK) as part of a larger study but will not be presented here. The custom LabVIEW program was used to process the data. The variables of interest: peak positive acceleration (PPA) of the tibia, vertical instantaneous loading rate (VILR), vertical average loading rate (VALR), and vertical impact peak (VIP) were extracted from the processed data. The PPA was the maximum positive acceleration that occurred during the early stance phase of running (Figure 2a). Generally, this occurred within 50 ms of foot strike. The VIP was the local maximum between foot strike and maximum force on the vertical ground reaction force curve. This, too, usually occurred within the first 50 ms of stance phase (Figure 2b). The VILR was the maximum slope of the vertical ground reaction force curve between successive data points in the region from 20% of the VIP to 80% of the VIP (Figure 2b). This was the most linear portion of the curve in the early part of stance. The VALR was the slope of the line through the 20% point and the 80% point. Therefore, all variables were associated with the impact phase of running. The data from five trials were processed and averaged for each subject.
Fig. 2.
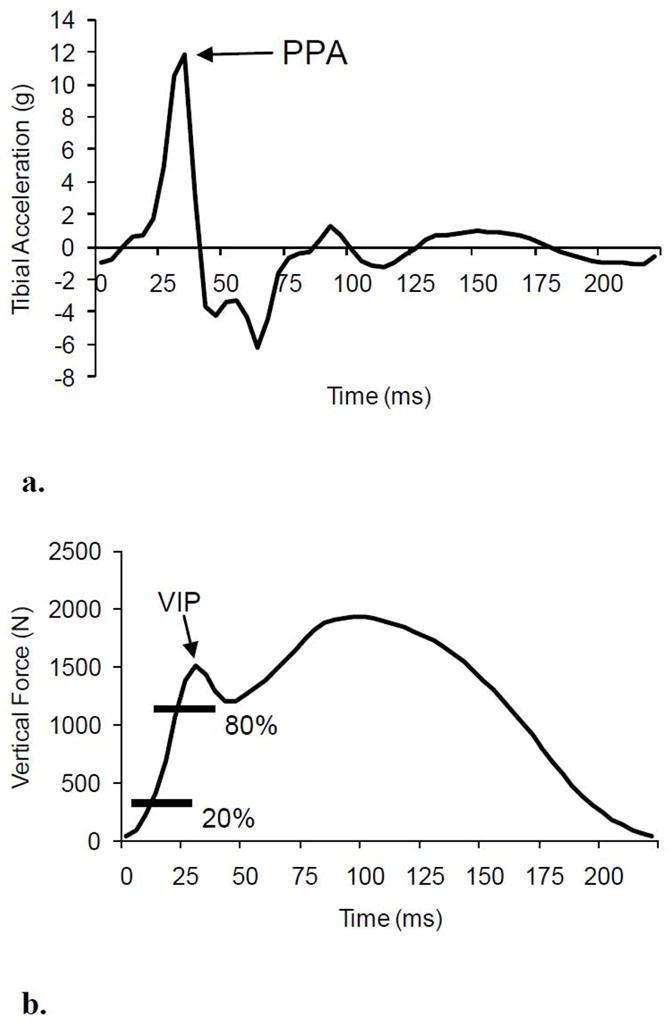
Variables of interest: PPA obtained from (a) the tibial acceleration curve and VIP, VILR, and VALR obtained from (b) the vertical ground reaction force curve. Note that both vertical loading rates (VILR and VALR) were calculated in the region between 20% and 80% of the VIP.
2.4. Gait Retraining
The subjects then began the retraining program, which included eight sessions over a two-week period. In each session, an accelerometer was taped to the anteromedial aspect of the subject’s distal tibia. Subjects wore their own shoes and ran on a treadmill at a self-selected speed. The signal from the accelerometer was displayed on a monitor in front of the treadmill. Tibial acceleration was chosen as the feedback variable because of its link to stress fractures (Davis et al., 2004; Milner et al., 2006a). In addition, tibial acceleration can be provided as feedback without the use of an instrumented treadmill, thus increasing the ease with which this training can be transitioned to a clinical environment. At the beginning of the first session, the accelerometer signal was visually inspected, and a line was placed across the display at approximately 50% of the mean peak positive acceleration. This reduction would bring the peak positive acceleration for each subject within one standard deviation of the mean peak positive acceleration measured on the group of uninjured runners. Subjects were instructed to “run softer,” make their footfalls quieter, and to keep the acceleration peaks below the line (Figure 3). Run time was gradually increased from 15 to 30 minutes over the eight sessions. Feedback was provided continuously for the first four sessions. The feedback was progressively removed in the last four sessions (Figure 4). During the last four sessions, one third of the feedback was provided at the beginning of each session, one third in the middle, and one third at the end. By the last session, runners were provided one minute of feedback in the beginning, one in the middle and one in the end of the session. The retraining sessions were scheduled with one rest day between every two sessions. During the two-week retraining period, subjects were instructed not to run outside of their training sessions in the lab. The subjects were monitored for signs of problems related to their new running gait. This was done by asking subjects how they felt after each retraining session. Then at the beginning of each subsequent session, they were asked about any pain or soreness from the previous session. The subjects’ comments were recorded and reviewed in order to identify pain or soreness that grew worse or did not subside after a few sessions.
Fig. 3.
Example of the real-time feedback from the accelerometer that was presented to subjects while they ran on the treadmill. Subjects were instructed to maintain their tibial acceleration below the horizontal line set at 50% of their peak values.
Fig. 4.

Schedule of running time and feedback time over the 8 retraining sessions. Note that the feedback was gradually removed after the fourth session.
2.5. Post-training Data Collection and Follow-up
Following completion of the last retraining session, another instrumented gait analysis was conducted. Subjects had approximately one hour to rest before the post-training data collection. Subjects were then instructed to run at least 16 km per week with their new gait pattern for the next four weeks. They then returned for a 1-month follow-up instrumented gait analysis. The post-training and 1-month follow-up data were collected and analyzed in the same manner as for the pre-training assessment.
2.6. Data Analysis
Repeated measures, one-way analysis of variance was used to analyze the PPA, VILR, VALR, and VIP data. Tukey’s pairwise comparisons were used to identify differences among the pre-training, post-training, and 1-month follow-up results. The level of significance for all statistical calculations was set at 0.05. These calculations were made using SPSS 14 for Windows® (SPSS, Inc., Chicago, IL, USA). In addition to the mean and standard deviation for each dependent variable, the effect sizes were also calculated.
3. Results
A comparison of the pre-training and post-training results revealed that there were significant reductions in PPA, VILR, and VALR at the post-training data collection (Figures 5 and 6). Also, there was a trend toward lower VIP from pre-training to post-training (P=0.06). In addition, a comparison of the pre-training results and the 1-month follow-up results showed that there were significant reductions in all of the variables (PPA, VILR, VALR, and VIP) at the 1-month follow-up (Figures 5 and 6). At the post-training and 1-month follow-up data collections, the reductions in PPA, VILR, VALR, and VIP from the pre-training values ranged between 20% and 50% (Table 1). In addition to being statistically significant, the reduction in each variable was associated with a large effect size (Cohen, 1988), ranging between 1.2 and 1.7 (Table 1). As expected, impact loading variables were not significantly different between post-training and 1-month. A slight increase was noted for PPA, VILR, and VALR and a slight decrease was seen VIP (Table 1).
Fig. 5.

Mean (SD) (a) peak positive tibial acceleration (PPA) and (b) vertical impact peak (VIP) at pre-training, post-training, and 1-month follow-up.
* Indicates significantly different from pre-training, P≤0.05.
Fig. 6.

Mean (SD) vertical instantaneous loading rate (VILR) and vertical average loading rate (VALR) at pre-training, post-training, and 1-month follow-up.
* Indicate significantly different from pre-training, P<0.05.
Table 1.
Changes (in percent difference and effect size) in variables of interest as a result of the gait retraining
| PPA | VILR | VALR | VIP | |
|---|---|---|---|---|
| Pre-training to Post-training | ||||
| Percent Difference | −48* | −34* | −32* | −19 |
| Effect Size | 1.5 | 1.7 | 1.5 | 1.2 |
| Pre-training to 1-month | ||||
| Percent Difference | −44* | −30* | −27* | −20* |
| Effect size | 1.4 | 1.7 | 1.3 | 1.3 |
| Post-training to 1-month | ||||
| Percent Difference | 6.2 | 6.4 | 7.6 | −1.3 |
| Effect size | 0.1 | 0.2 | 0.02 | 0.1 |
A negative percent difference indicates a reduction in the variable; a positive value indicates an increase.
Indicates significantly different as determined by post hoc testing, P≤0.05.
Eight of the ten subjects reported some type of soreness associated with the retraining. Six subjects experienced tibialis anterior soreness, and four of those subjects also described soreness in their calves. One subject had tight hamstrings and slight knee pain in two sessions. Another subject had soreness in the quadriceps after two of the sessions. However, none of the pain or soreness became worse or lasted for more than a few sessions. Additionally, none of the subjects reported any pain, soreness, or injury at the one-month follow-up. Interestingly, all subjects reported that the new gait pattern felt natural by the end of the sixth retraining session.
4. Discussion
The purpose of this study was to examine the efficacy of a gait retraining program designed to reduce lower extremity loading during running. The main feature of the program was multiple training sessions on a treadmill involving real-time visual feedback of tibial acceleration. In addition, it involved a gradual increase in running time and a gradual removal of the feedback. This program resulted in a reduction in all of the loading variables of interest (PPA, VILR, VALR, and VIP). Subjectively, all of the subjects reported that their new gait patterns felt natural by the end of the sixth session. More importantly, the changes brought about by the retraining persisted for at least one month.
The results of this study build on the results of the previous study by Crowell et al. (2010). In that study, a single gait retraining session using real-time visual feedback was conducted. The objectives were to determine whether subjects could reduce their lower extremity loading and maintain the reductions for a few minutes after the feedback was removed. In that study, the changes in PPA, VILR, VALR, and VIP ranged from +6% to −60%, −15% to −39%, −16% to −39%, and −6% to −30%, respectively. For the group of subjects in the current study, the reductions in PPA, VILR, VALR, and VIP fall within the ranges achieved in the previous study. Thus, gait retraining using real-time visual feedback of tibial acceleration appears to be effective in reducing lower extremity loading for up to one month.
The loading variables (PPA, VILR, VALR, and VIP) were chosen because they occur when the foot is impacting the ground during running (generally within the first 50 ms of stance). Increases in these variables have been shown to be associated with tibial stress fractures (Davis et al., 2004, Milner et al., 2006a). Following the retraining program, PPA, VILR, VALR, and VIP were within the range reported for normal subjects in other studies (Hennig et al., 1993; Mahar et al., 1997; Laughton et al., 2003; Davis et al., 2004; Milner et al., 2006a). This indirectly suggests that the risk of tibial stress fractures was reduced for subjects in this study. However, prospective studies are needed to confirm this.
Attempts by others to reduce loading during running have included the use of cushioned shoes, foot orthoses and shock attenuating insoles. In terms of tibial acceleration, researchers have found reductions in PPA of roughly 11% (Milani et al., 1997) to 20% (Butler et al, 2006) when comparing different shoes. Reductions in PPA of 16% have been reported for subjects running with cushioned insoles compared to running with standard insoles (O’Leary et al., 2008). In examinations of foot orthoses, researchers have reported reductions as high as 23% for VILR, 18% for VALR, and 10% for VIP when running with custom orthoses in running sandals (Mundermann et al., 2003) or commercially available orthoses in military boots (Dixon, 2007). However, reductions in PPA, VILR, VALR, and VIP achieved in the current study (Table 1) were at least two times greater than those achieved through the use of cushioning shoes, foot orthoses, or shock attenuating insoles. This suggests that an individual’s ability to alter their own running mechanics may be greater than that of external devices such as shoes, orthoses, or insoles.
An important indication of learning is the retention of motor skills beyond the training period (Salmoni et al., 1984). We found that the reduced loading noted after the retraining persisted at the 1-month follow-up. We postulate that this was due to the faded feedback design used in the current study. Subjects who receive intermittent or delayed feedback have been shown to perform better in the long-term than subjects who received continuous immediate feedback (Swinnen et al., 1990; Winstein and Schmidt, 1990). Removing the feedback is beneficial to motor skill learning because the subjects must rely on internal cues for performing correct motor patterns (Winstein, 1991). While insignificant, there were small increases in some of the variables between the post-training data collection and the 1-month follow-up (Table 1). A continued increase in these values post-training might indicate that subjects may need more than eight retraining sessions, or that they may need periodic refresher training. A study with longer follow-up is currently underway to determine this.
Changing a runner’s gait to reduce the risk of a stress fracture may have unintended consequences such as increasing the chance of another kind of injury. For the subjects in this study, the gait retraining did not appear to cause any injuries. The subjects appeared to accommodate to the new gait pattern quickly, and the soreness that occurred during the retraining sessions did not last for more than a few sessions. In addition, no injuries were reported at the one-month follow-up.
Runners seem to be able to modify their gait without specific instructions on how to accomplish it. In this study, subjects were given the same instructions about running softer and keeping their PPA below the line on the monitor. As a result, they all achieved reductions in their PPA, VILR, VALR, and VIP. Some of the strategies used by the subjects may be more effective than others, and these strategies are being examined as part of a larger study.
One of the strengths of this simple retraining program is its applicability to a variety of settings. The required equipment (treadmill, accelerometer, computer, and monitor) is readily available and relatively inexpensive. Therefore, it could be easily implemented into physical therapy clinics, fitness centers, and military training facilities in order to assess and retrain individuals at risk for stress fractures.
The results of this study are significant in many ways. First, the reductions in PPA, VILR, VALR, and VIP achieved through retraining are, on average, greater than the reductions achieved through the use of cushioning shoes, foot orthoses, or shock reducing insoles. Thus, impact loading may be more effectively reduced with gait retraining than footwear and orthotics, which may be more cost effective in the long run. Reducing this impact loading may reduce the risk of stress fractures in runners and allow them to remain physically active, resulting in healthier lifestyles. In terms of the military, recruits who sustain stress fractures and exhibit high impact loading could undergo the retraining during their rehabilitation. This may significantly reduce their risk for re-injury and could significantly reduce the high cost to the military when a soldier is medically discharged. Future studies will be focused on the kinematic strategies used to reduce PPA, VILR, VALR, and VIP. In addition, the gait retraining program used in this study will serve as the foundation for future experiments with other feedback methods and training schedules. The long-term goal of this work is to use gait retraining as a means for preventing stress fractures. Thus, after the feedback method and training schedule are optimized, a prospective study with a large group of runners at high risk of stress fractures can be conducted. This would show the efficacy of gait retraining for the prevention of stress fractures.
5. Conclusion
The results of this study suggest that lower extremity impact loading can be reduced with a gait retraining program that uses real-time visual feedback. In addition, these changes appear to persist at the 1-month follow-up. Longer term follow-ups are needed to evaluate the continued persistence of the gait changes. The long-term follow-ups are also needed to ensure that gait changes to reduce the risk of stress fractures are not leading to increased risk for other injuries.
Acknowledgments
The authors would like to acknowledge the research assistants and students of the Motion Analysis Laboratory at the University of Delaware for their assistance with data collections. This research was funded in part by the following grants: DOD W911NF-05-1-0097, DOD X81XWH-07-1-0395, NIH R01HD050679, and NIH 1-S10-RR022396. The organizations that funded this research encourage publication of the results.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- Anderson MW, Greenspan A. Stress fractures. Radiology. 1996;119:1–12. doi: 10.1148/radiology.199.1.8633129. [DOI] [PubMed] [Google Scholar]
- Beck BR. Tibial stress injuries: An aetiological review for the purposes of guiding management. Sports Medicine. 1998;26:265–279. doi: 10.2165/00007256-199826040-00005. [DOI] [PubMed] [Google Scholar]
- Bennell K, Brukner P. Preventing and managing stress fractures in athletes. Physical Therapy in Sport. 2005;6:171–180. [Google Scholar]
- Butler RJ, Hamill J, Davis IS. Interaction of arch type and footwear on running mechanics. The American Journal of Sports Medicine. 2006;34:1998–2005. doi: 10.1177/0363546506290401. [DOI] [PubMed] [Google Scholar]
- Cohen J. Statistical Power Analysis for the Behavioral Sciences. 2. Hillsdale (NJ): Lawrence Earlbaum Associates; 1988. [Google Scholar]
- Coyle EF, Martin WH, Sinacore DR, Joyner MJ, Hagberg JM, Holloszy JO. Time course of loss of adaptations after stopping prolonged intense endurance training. Journal of Applied Physiology: Respiratory, Environmental and Exercise Physiology. 1984;57:1857–1864. doi: 10.1152/jappl.1984.57.6.1857. [DOI] [PubMed] [Google Scholar]
- Coyle EF, Martin WH, Bloomfield SA, Lowry OH, Holloszy JO. Effects of detraining on responses to submaximal exercise. Journal of Applied Physiology. 1985;59:853–859. doi: 10.1152/jappl.1985.59.3.853. [DOI] [PubMed] [Google Scholar]
- Creaby MW, Dixon SJ. External frontal plane loads may be associated with tibial stress fracture. Medicine and Science in Sports and Exercise. 2008;40:1669–1674. doi: 10.1249/MSS.0b013e31817571ae. [DOI] [PubMed] [Google Scholar]
- Crowell HP, Milner CE, Hamill J, Davis IS. Reducing impact loading during running with the use of real-time visual feedback. Journal of Orthopaedic & Sports Physical Therapy. 2010;40:206–213. doi: 10.2519/jospt.2010.3166. [DOI] [PubMed] [Google Scholar]
- Davis I, Milner C, Hamill J. Does increased loading during running lead to tibial stress fractures? A prospective study. Medicine and Science in Sports and Exercise. 2004;35(Supplement):S58. [Google Scholar]
- Dingwell JB, Davis BL, Frazier DM. Use of an instrumented treadmill for real-time gait symmetry evaluation and feedback in normal and trans-tibial amputee subjects. Prosthetics and Orthotics International. 1996;20:101–110. doi: 10.3109/03093649609164426. [DOI] [PubMed] [Google Scholar]
- Dixon SJ. Influence of a commercially available orthotic device on rearfoot eversion and vertical ground reaction force when running in military footwear. Military Medicine. 2007;172:446–450. doi: 10.7205/milmed.172.4.446. [DOI] [PubMed] [Google Scholar]
- Doyon J, Penhune V, Ungerleider LG. Distinct contribution of the cortico-striatal and cortico-cerebellar systems to motor skill learning. Neuropsychologia. 2003;41:252–262. doi: 10.1016/s0028-3932(02)00158-6. [DOI] [PubMed] [Google Scholar]
- Faul F, Erdfelder E. GPOWER: A priori, post hoc, and compromise power analysis for MS-DOS [computer program] Bonn, FRG: Bonn University, Department of Psychology; 1992. [Google Scholar]
- Gapsis JJ, Grabois M, Borrell RM, Menken SA, Kelly M. Limb load monitor: evaluation of a sensory feedback device for controlled weight bearing. Archives of Physical Medicine and Rehabilitation. 1982;63:38–41. [PubMed] [Google Scholar]
- Hauret KG, Shippey DL, Knapik JJ. The physical training and rehabilitation program: Duration of rehabilitation and final outcome of injuries in basic combat training. Military Medicine. 2001;166:820–826. [PubMed] [Google Scholar]
- Hennig E, Milani T, Lafortune M. Use of ground reaction force parameters in predicting peak tibial accelerations in running. Journal of Applied Biomechanics. 1993;9:306–314. doi: 10.1123/jab.9.4.306. [DOI] [PubMed] [Google Scholar]
- Jones BH, Thacker SB, Gilchrist J, Kimsey CD, Sosin DM. Prevention of lower extremity stress fractures in athletes and soldiers: A systematic review. Epidemiologic Reviews. 2002;24:228–247. doi: 10.1093/epirev/mxf011. [DOI] [PubMed] [Google Scholar]
- Jones BH, Harris JM, Vinh TN, Rubin C. Exercise-induced stress fractures and stress reactions of bone: epidemiology, etiology, and classification. Exercise and Sport Sciences Reviews. 1989;17:379–422. [PubMed] [Google Scholar]
- Korman M, Raz N, Flash T, Karni A. Multiple shifts in the representation of a motor sequence during the acquisition of skilled performance. Proceedings of the National Academy of Sciences of the United States of America. 2003;100:12492–12497. doi: 10.1073/pnas.2035019100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Laughton CA, Davis IM, Hamill J. Effect of strike pattern and orthotic intervention on tibial shock during running. Journal of Applied Biomechanics. 2003;19:153–168. [Google Scholar]
- Lee TD, Schmidt RA. Motor learning and memory. In: Roediger HL, Byrne JH, editors. Learning and Memory: A Comprehensive Reference. Elsevier; Oxford: 2008. pp. 645–662. [Google Scholar]
- Mahar AT, Derrick TR, Hamill J, Caldwell GE. Impact shock and attenuation during in-line skating. Medicine and Science in Sports and Exercise. 1997;29:1069–1075. doi: 10.1097/00005768-199708000-00013. [DOI] [PubMed] [Google Scholar]
- McClay IS, Williams DS, Laughton CA. Can Gait be Retrained to Prevent Injury in Runners?. Proceedings of the American Society of Biomechanics; Pittsburgh, PA. 1999. [Google Scholar]
- Messier SP, Cirillo K. Effects of a verbal and visual feedback system on running technique, perceived exertion and running economy in female novice runners. Journal of Sports Sciences. 1989;7:113–126. doi: 10.1080/02640418908729830. [DOI] [PubMed] [Google Scholar]
- Milgrom C, Giladi M, Chisin R, Dizian R. The long-term followup of soldiers with stress fractures. The American Journal of Sports Medicine. 1985;13:398–400. doi: 10.1177/036354658501300606. [DOI] [PubMed] [Google Scholar]
- Milani TL, Hennig EM, Lafortune MA. Perceptual and biomechanical variables for running in identical shoe constructions with varying midsole hardness. Clinical Biomechanics. 1997;12:294–300. doi: 10.1016/s0268-0033(97)00008-9. [DOI] [PubMed] [Google Scholar]
- Milner CE, Ferber R, Pollard CD, Hamill J, Davis IS. Biomechanical factors associated with tibial stress fracture in female runners. Medicine and Science in Sports and Exercise. 2006a;38:323–328. doi: 10.1249/01.mss.0000183477.75808.92. [DOI] [PubMed] [Google Scholar]
- Milner CE, Davis IS, Hamill J. Free moment as a predictor of tibial stress fracture in distance runners. Journal of Biomechanics. 2006b;39:2819–2825. doi: 10.1016/j.jbiomech.2005.09.022. [DOI] [PubMed] [Google Scholar]
- Mundermann A, Nigg BM, Humble RN, Stefanyshyn DJ. Orthotic comfort is related to kinematics, kinetics, and EMG in recreational runners. Medicine and Science in Sports and Exercise. 2003;35:1710–1719. doi: 10.1249/01.MSS.0000089352.47259.CA. [DOI] [PubMed] [Google Scholar]
- O’Leary K, Vorpahl KA, Heiderscheit B. Effect of cushioned insoles on impact forces during running. Journal of the American Podiatric Medical Association. 2008;98:36–41. doi: 10.7547/0980036. [DOI] [PubMed] [Google Scholar]
- Pepper M, Akuthota V, McCarty EC. The pathophysiology of stress fractures. Clinics in Sports Medicine. 2006;25:1–16. doi: 10.1016/j.csm.2005.08.010. [DOI] [PubMed] [Google Scholar]
- Petrofsky JS. The use of electromyogram feedback to reduce Trendelenburg gait. European Journal of Applied Physiology. 2001;85:491–495. doi: 10.1007/s004210100466. [DOI] [PubMed] [Google Scholar]
- Pohl MB, Mullineaux DR, Milner CE, Hamill J, Davis IS. Biomechanical predictors of retrospective tibial stress fractures in runners. Journal of Biomechanics. 2008;41:1160–1165. doi: 10.1016/j.jbiomech.2008.02.001. [DOI] [PubMed] [Google Scholar]
- Rauh MJ, Macera CA, Trone DW, Shaffer RA, Brodine SK. Epidemiology of stress fracture and lower-extremity overuse injury in female recruits. Medicine and Science in Sports and Exercise. 2006;38:1571–1577. doi: 10.1249/01.mss.0000227543.51293.9d. [DOI] [PubMed] [Google Scholar]
- Salmoni AW, Schmidt RA, Walter CB. Knowledge of results and motor learning: a review and critical reappraisal. Psychological Bulletin. 1984;95:355–386. [PubMed] [Google Scholar]
- Seeger BR, Caudrey DJ, Scholes JR. Biofeedback therapy to achieve symmetrical gait in hemiplegic cerebral palsied children. Archives of Physical Medicine and Rehabilitation. 1981;62:364–368. [PubMed] [Google Scholar]
- Swinnen SP, Schmidt RA, Nicholson DE, Shapiro DC. Information feedback for skill acquisition: Instantaneous knowledge of results degrades learning. Journal of Experimental Psychology: Learning, Memory, and Cognition. 1990;16:706–716. [Google Scholar]
- Taunton JE, Ryan MB, Clement DB, McKenzie DC, Lloyd-Smith DR, Zumbo BD. A retrospective case-control analysis of 2002 running injuries. British Journal of Sports Medicine. 2002;36:95–101. doi: 10.1136/bjsm.36.2.95. [DOI] [PMC free article] [PubMed] [Google Scholar]
- United States General Accounting Office. Report GAO/NAIAD-93–213. Washington, DC: US General Accounting Office; 1998. Military attrition: Better data coupled with policy changes could help the services reduce separations. [Google Scholar]
- White SC, Lifeso RM. Altering asymmetric limb loading after hip arthroplasty using real-time dynamic feedback when walking. Archives of Physical Medicine and Rehabilitation. 2005;86:1958–1963. doi: 10.1016/j.apmr.2005.04.010. [DOI] [PubMed] [Google Scholar]
- Winstein CJ, Schmidt RA. Reduced frequency of knowledge of results enhances motor skill learning. Journal of Experimental Psychology: Learning, Memory, and Cognition. 1990;16:677–691. [Google Scholar]
- Winstein CJ. Knowledge of results and motor learning – implications for physical therapy. Physical Therapy. 1991;71:140–149. doi: 10.1093/ptj/71.2.140. [DOI] [PubMed] [Google Scholar]