

Abstract
Transposition of the gallbladder to the left side without situs inversus viscerum is rare. These gallbladders are situated under the left lobe of the liver between Segment III and IV or on Segment III to the left of the falciform ligament. Because routine preoperative studies may not detect the anomaly, it may provide the surgeons with an unusual surprise during laparoscopy. Awareness of the unpredictable confluence of the cystic duct into the common bile duct and selective use of intraoperative cholangiography aid in the safe laparoscopic management of this unusual problem.
Keywords: Laparoscopy, Sinistroposition of the gall-bladder, Left-sided gallbladder, situs inversus
CASE REPORT
The patient is a 60-year-old male who is a known diabetic. He was admitted to the hospital with a history of jaundice. Liver function tests revealed an elevated serum bilirubin of 9.8 mg/dL (direct bilirubin, 7.1 mg/dL; indirect, 2.7 mg/ dL); alkaline phosphatase, 1040 IU/L; serum glutamic pyruvic transaminase, 85 IU/L; gamma glutamyl transpeptidase, 370 IU/L. An abdominal ultrasound showed a grossly distended gallbladder with diffuse wall thickening with calculus at the neck of the gallbladder and mild dilatation of intrahepatic biliary radicles. Magnetic resonance cholangiopancreatography performed because of the patient's high bilirubin and alkaline phosphatase showed cholelithiasis with gallbladder wall thickening and mild intrahepatic biliary radical dilatation. The patient was managed conservatively with parenteral antibiotics. Repeat liver function tests performed 4 days later showed a decrease in serum bilirubin, alkaline phosphatase, and enzymes. The patient was discharged and periodically followed up. He was readmitted after 6 weeks for elective cholecystectomy. His liver function tests were normal. Diagnostic laparoscopy was performed with the patient in the supine position. The gallbladder was severely diseased and lying to the left of the falciform ligament (Figure 1). The cardiac pulsation was on the left side, and the rest of the abdominal viscera were normally positioned. The patient was placed in the lithotomy position. Accessory ports were placed in the left subcostal region. Calot's triangle was frozen. With difficulty, the anterior and posterior branches of the cystic artery were isolated, clipped, and divided (Figure 2). The cystic duct area was wide and firmly adherent to the common hepatic duct (Mirrizzi's syndrome –Type I). Retrograde dissection of the gallbladder was performed. The cystic duct was separated from the common hepatic duct. It entered the common hepatic duct on the right side. The cystic duct was clipped and divided. The gallbladder was put in an endobag and extracted through the epigastric port. The patient recovered well and was discharged on the second postoperative day. Pathological examination revealed a gallbladder with subepithelial round cell infiltrates associated with fibrosis.
Figure 1.

Gallbladder lying to the left of the falciform ligament in relation to Segment III.
Figure 2.
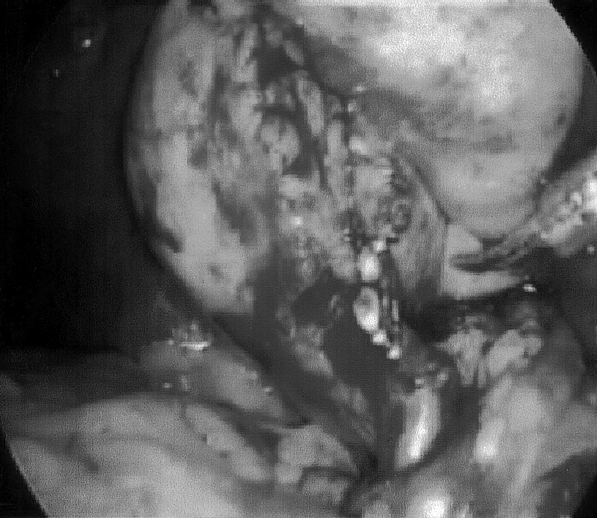
Anterior and posterior branches of cystic artery– clipped and divided.
DISCUSSION
A left-sided gallbladder can occur as a component of situs inversus viscerum. Malposition of gallbladder occurring in the absence of situs inversus is a very rare anomaly.1
Two types of malposition are known: (1) medioposition (2) sinistroposition (transposition, true left-sided gallbladder)
In medioposition, the gallbladder is displaced medially to lie on the undersurface of the quadrate lobe (Segment IV) but is still on the right side of the round ligament. In sinistroposition, the gallbladder lies under the left lobe (Segment III) to the left of the round ligament.1 In a multicenter series1 of laparoscopic cholecystectomies, the prevalence of sinistroposition was 0.3%. In our series of 10,235 laparoscopic cholecystectomies over the last 12 years (1992 to 2004), we had 8 left-sided gallbladders of which this was the only true left-sided gallbladder.
In sinistroposition, the cystic artery always crosses in front of the common bile duct from right to left. The cystic duct may open on the left or right side of the common hepatic duct or on to the left hepatic duct directly.
It is important to emphasize that it is difficult to obtain the diagnosis of this malformation preoperatively as the clinical picture usually is one of pain on the right side. Hence, it may provide the surgeons with an unusual surprise during laparoscopy. The anomaly does not preclude a safe laparoscopic cholecystectomy but demands exercising surgical prudence, limiting the use of diathermy, and avoiding the division of structures until a clear picture of the bile duct and blood vessels is obtained.
Although in our case retrograde dissection was necessitated in view of the associated Mirrizzi syndrome, antegrade dissection of the gallbladder starting as close as possible to the gallbladder margin is advocated because it provides better visualization of the anatomical structures.2,3 Adopting the French position, modification of the port sites and the use of falciform ligament lift facilitates the procedure in these cases.4
If necessary, intraoperative cholangiography helps to further define the biliary system.2,4 However, if the anatomy remains unclear, open surgery should be considered before undesirable complications occur.
CONCLUSION
Left-sided gallbladders without situs inversus viscerum are rare entities that can provide an unusual surprise during laparoscopy. Awareness of the unpredictable biliary anatomy, modification of the technique and the selective use of intraoperative cholangiography aid in the safe laparoscopic management of this unusual entity.
References:
- 1. Rozsos I, Ferenczy J, Vincze K, Rainer S. Left sided gallbladder [in Hungarian]. Magy Seb. 2002;55(5):329–330 [PubMed] [Google Scholar]
- 2. Corbajo MA, Martin del Omo JC, Blanco JI, et al. Congenital malformation of the gallbladder and cystic duct diagnosed by laparoscopy: high surgical risk. JSLS. 1999;3:319–321 [PMC free article] [PubMed] [Google Scholar]
- 3. Gui D, Magalini S, Prete F, Sermoneta D. What's right when the gallbladder's left? A case report. Surg Endosc. 2002;16(11): 1637. [DOI] [PubMed] [Google Scholar]
- 4. Donthi R, Thomas DJ, Sanders D, Schmidt SP. Report of laparoscopic cholecystectomy in two patients with left-sided gallbladders. JSLS. 2001;5:53–56 [PMC free article] [PubMed] [Google Scholar]