

Abstract
Management of large calculi in ectopic pelvic kidneys poses a challenge to the urologist. Risk of injury to surrounding abdominal viscera and vasculature makes open surgery as well as percutaneous nephrostolithotomy in an ectopic kidney a challenging procedure. Laparoscopic management avoids open surgery and associated morbidity and offers added safety. We report the management of symptomatic stones in a pelvic ectopic kidney lying anterior to the L5 vertebra and sacrum by transmesocolic laparoscopic pyelolithotomy in an 11-year-old child. Complete stone clearance was achieved with no complications and an uneventful postoperative recovery. The patient was discharged 72 hours after the surgery.
Keywords: Ectopic kidney, Laparoscopy, Pyelolithotomy, Renal calculus
INTRODUCTION
Management of stones in an ectopic kidney poses a challenge to the urologist. The exact location of the kidney, variation of pelvicaliceal anatomy, stone size, and location are important factors for deciding the approach in these patients. Apart from open stone surgery, percutaneous nephrolithotomy (with laparoscopic or ultrasonography guided needle punctures) and laparoscopic pyelolithotomy are the treatment modalities described in the literature.1–4 We present a case of stones in a pelvic ectopic kidney managed by transmesocolic laparoscopic pyelolithotomy.
CASE REPORT
An 11-year-old boy presented with bilateral stone disease, ie, a right upper ureteric stone and 2 radiopaque stones (2.3cm × 2.0cm and 2.0cm × 0.9cm) in a left ectopic pelvic kidney (Figure 1 and 2). The left ureteric stone was treated with antegrade percutaneous nephroureterolithotomy (Figure 3). Subsequently, in the second session, the patient underwent laparoscopic pyelolithotomy. The patient was placed in a supine position after prior retrograde pyelography and placement of a double ‘J’ stent. A Veress needle was inserted through a 1.5-cm umbilical incision, pneumoperitoneum was created, and a 12-mm visualizing laparoscopic trocar (Ethicon) was inserted into the abdominal cavity. Secondary ports, 10mm and 5mm, were inserted in the right and left iliac fossae, respectively, and the table was tilted to a 30° Trendelenburg position. One additional 5-mm port was inserted in the midline one handbreadth below the umbilicus. The mesocolon of the large bowel was draped over the ectopic kidney in the pelvis overlying the sacral promontory. Because the patient was quite slim, little fat was present in the mesocolon, and the pulsations and course of the vessels could be seen clearly. We proceeded with a transmesocolic approach without mobilizing the bowel off the anterior surface of the kidney and renal pelvis. Stones were located in the renal pelvis and middle posterior calyx. Both the stones were extracted under vision after pyelotomy, using a 10-mm right angle forceps (Figure 4). The pelvis was primarily closed using interrupted Vicryl sutures and re-retroperitonealization of the kidney by suturing the overlying peritoneum. A 14F drain was placed in the peritoneal cavity close to the kidney through the left 5-mm laparoscopic port. Hemostasis was confirmed, and the laparoscopic ports were removed. Complete clearance was documented with plain x-ray KUB.
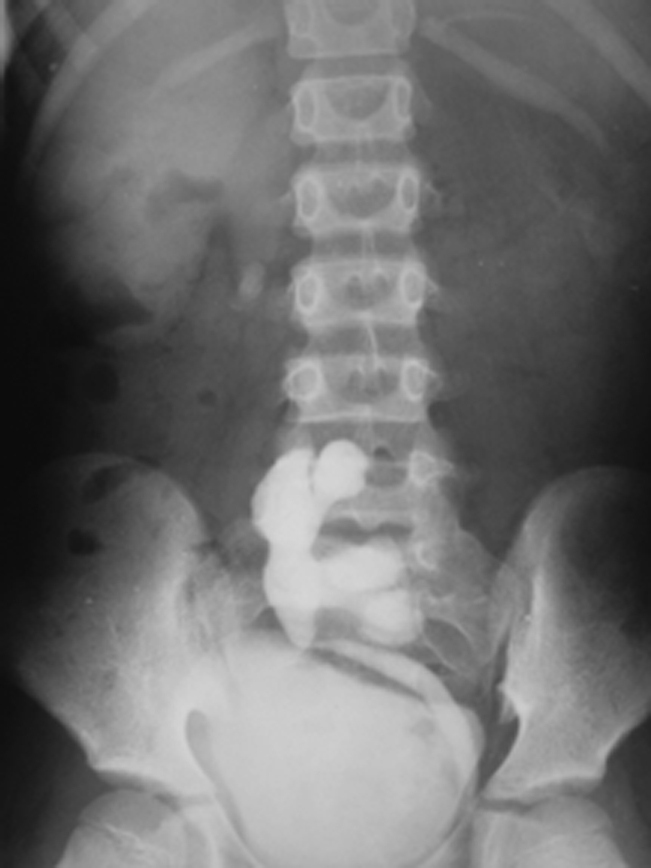
Figure 1.

Plain x-ray KUB showing a single stone on the right side (white arrow) at the level of the third lumber vertebra and 2 stones overlying the sacrum (black arrow).
Figure 2.

X-ray KUB showing 2 calculi overlying the sacrum in the left ectopic pelvic kidney. Nephrostomy tube and double “J” in situ seen on the right side.
Figure 3.
Intravenous urography showing an ectopic left pelvic kidney with the stone lying in the pelvis and the calyx.
Figure 4.

Intraoperative photograph after pyelotomy. Stone being removed using laparoscopic right angle forceps.
RESULTS
Complete stone clearance was achieved. Operative time was 94 minutes. Estimated blood loss was <50 mL. No notable complications were encountered. The intraperitoneal drain was removed on day 2, and the patient was discharged 72 hours after surgery. All 3 stones were calcium-oxalated dihydrate. The double J stent was removed 4 weeks after surgery as an office procedure with the patient under local anesthesia. Follow-up ultrasonography at 6 months revealed a normal kidney without any hydronephrosis or stones.
DISCUSSION
Small stone burden in an ectopic kidney can be dealt with by shock wave lithotripsy or flexible ureteroscopy.5 However, larger stone sizes require more invasive procedures. Percutaneous access through a standard flank approach may not be suitable in pelvic ectopic kidneys and frequently requires modification of the technique including laparoscopic assistance to avoid inadvertent injury to the surrounding visceras.3,6 Some authors have also suggested the use of ultrasound-guided punctures to achieve percutaneous access in ectopic kidneys prior to percutaneous nephrolithotomy (PNL). Desai et al4 utilized ultrasound-guided punctures for PNL in 9 patients for the treatment of stones in the ectopic pelvic kidneys. Three patients required 2-stage procedures, while others were treated in a single stage. Seven patients needed one tract, and 2 required 2 tracts. Notable technical factors were use of a mature tract or an Amplatz sheath, routine postoperative double-J stenting, and a nephrostogram before nephrostomy tube removal.
Laparoscopic guidance for achieving access to the pelvicaliceal system (PCS) has been used to add safety to the transperitoneal route of percutaneous nephrolithotomy. Various authors have reported successful outcomes and complete stone clearance with no intraoperative or postoperative morbidity.7,8 This method also provides the opportunity for safe access to the pelvicaliceal system and stone clearance in a single session.
Because the location and configuration of the renal pelvicaliceal system of an ectopic kidney can vary, each case requires a unique approach for surgical management of stones. In the situation of an ectopic kidney with a laterally or anteriorly directed pelvis, a skilled laparoscopic surgeon can easily perform laparoscopic pyelolithotomy. Thus, not only complete clearance can be achieved in a single operative session, but also postoperative morbidity can be minimized by primarily closing the opening in the pelvicaliceal system. In a similar situation, Kamat et al9 have found laparoscopic pyelolithotomy to be an effective procedure with low morbidity. In addition, a transmesocolic approach in our case avoided the additional procedure of mobilization of the bowel without any associated risk of bowel or major vascular injury and should be a viable option in select thin-built patients with ectopic kidneys.
CONCLUSIONS
Laparoscopic pyelolithotomy can be safely and effectively performed in a pelvic kidney with a laterally or anteriorly directed pelvis without the need for ancillary modalities.
References:
- 1. Gupta N, Mandhani A, Sharma D, Kapoor R, Dubey D, Kumar A. Is laparoscopic approach safe for ectopic pelvic kidneys? Urol Int. 2006;77(2):118–121 [DOI] [PubMed] [Google Scholar]
- 2. Modi P, Goel R, Dodia S. Case report: laparoscopic pyeloplasty with pyelolithotomy in crossed fused ectopia. J Endourol. 2006;20(3):191–193 [DOI] [PubMed] [Google Scholar]
- 3. Maheshwari PN, Bhandarkar DS, Andankar MG, Shah RS. Laparoscopically guided transperitoneal percutaneous nephrolithotomy for calculi in pelvic ectopic kidneys. Surg Endosc. 2004;18(7):1151, [DOI] [PubMed] [Google Scholar]
- 4. Desai MR, Jasani A. Percutaneous nephrolithotripsy in ectopic kidneys. J Endourol. 2000;14(3):289–292 [DOI] [PubMed] [Google Scholar]
- 5. Tunc L, Tokgoz H, Tan MO, Kupeli B, Karaglan U, Bozkirli I. Stones in anomalous kidneys: results of treatment by shock wave lithotripsy in 150 patients. Int J Urol. 2004;11:831–836 [DOI] [PubMed] [Google Scholar]
- 6. Matlaga BR, Kim SC, Watkins SL, Kuo RL, Munch LC, Lingeman JE. Percutaneous nephrolithotomy for ectopic kidneys: over, around, or through. Urology. 2006;67:513–517 [DOI] [PubMed] [Google Scholar]
- 7. Holman E, Toth C. Laparoscopically assisted percutaneous transperitoneal nephrolithotomy in pelvic dystopic kidneys: experience in 15 successful cases. J Laparoendosc Adv Surg Tech. 1998;A8:431–435 [DOI] [PubMed] [Google Scholar]
- 8. Troxel SA, Low RK, Das S. Extraperitoneal laparoscopy assisted percutaneous nephrolithotomy in a left pelvic kidney. J Endourol. 2002;16:655–657 [DOI] [PubMed] [Google Scholar]
- 9. Kamat N, Khandelwal P. Laparoscopic pyelolithotomya technique for the management of stones in the ectopic pelvic kidney. Int J Urol. 11(7):581–584, 2004 l [DOI] [PubMed] [Google Scholar]