

Abstract
OBJECTIVES
The use of continuous infusion medications with individualized concentrations may increase the risk for errors in pediatric patients. The objective of this study was to evaluate the effect of computerized prescriber order entry (CPOE) for continuous infusions with standardized concentrations on frequency of pharmacy processing errors. In addition, time to process handwritten versus computerized infusion orders was evaluated and user satisfaction with CPOE as compared to handwritten orders was measured.
METHODS
Using a crossover design, 10 pharmacists in the pediatric satellite within a university teaching hospital were given test scenarios of handwritten and CPOE order sheets and asked to process infusion orders using the pharmacy system in order to generate infusion labels. Participants were given three groups of orders: five correct handwritten orders, four handwritten orders written with deliberate errors, and five correct CPOE orders. Label errors were analyzed and time to complete the task was recorded.
RESULTS
Using CPOE orders, participants required less processing time per infusion order (2 min, 5 sec ± 58 sec) compared with time per infusion order in the first handwritten order sheet group (3 min, 7 sec ± 1 min, 20 sec) and the second handwritten order sheet group (3 min, 26 sec ± 1 min, 8 sec), (p<0.01). CPOE eliminated all error types except wrong concentration. With CPOE, 4% of infusions processed contained errors, compared with 26% of the first group of handwritten orders and 45% of the second group of handwritten orders (p<0.03). Pharmacists were more satisfied with CPOE orders when compared with the handwritten method (p=0.0001).
CONCLUSIONS
CPOE orders saved pharmacists' time and greatly improved the safety of processing continuous infusions, although not all errors were eliminated. pharmacists were overwhelmingly satisfied with the CPOE orders
Keywords: continuous infusions, CPOE, medication errors, pediatric critical care, standardized concentrations
INTRODUCTION
Children and neonates are vulnerable populations at risk for medication errors, especially in intensive care units where continuous infusion medications are vital treatment components.1 Errors associated with intravenous medications in pediatric settings are very common2 and often result in serious adverse events.3,4 The Institute for Safe Medication Practices5 recommends careful prescribing, compounding and administration of continuous infusion medications (e.g., insulin, dopamine) and categorizes these medications as “high-alert” because of their narrow safety margins. Despite the high risk for errors associated with continuous infusions, few studies are available regarding the incidence and severity of such errors.6
Pediatric continuous infusion medications have been historically dosed and compounded using the “rule-of-six,” a weight-based method to calculate a standardized infusion rate by varying the infusion concentration. Using the rule-of-six, the amount of drug in milligrams that should be added to 100 mL of a diluent equals six times the patient weight in kilograms, and the infusion rate per hour (mL/hr) equals the ordered dose in mcg/kg/min.7 This results in a unique concentration for each patient weight. The rule-of-six technique was originally developed to dose and compound infusions in emergency situations; however, it became a common practice even in non-emergency situations because of its convenience in calculating continuous infusions where a frequent dose titration is needed.
Weight-based dosing using equations in pediatrics was responsible for 70% of calculation errors at a large teaching hospital.8 In addition, the use of individualized concentrations was distinguished as an error-prone and time-consuming process for pharmacists9 and nurses.10 As a consequence, per the National Patient Safety Goals for 2003, The Joint Commission regarded the rule-of-six as an error-prone activity and mandated all pediatric institutions to transition to a limited number of standardized concentrations.11
In response to The Joint Commission mandate of using standardized concentrations and to improve safety and standardize the process of ordering, compounding, and administering continuous infusion medications, we developed and implemented a computerized prescriber order entry (CPOE) system in a pediatric intensive care unit (PICU) at a large university teaching hospital.12 The system generates two to four standardized concentrations (low, intermediate, high and maximum concentrations) that can meet diverse weight ranges of PICU patients for each continuous infusion drug. In addition, the system recommends the “optimal concentration” that would result in a clinically acceptable fluid load for a patient's weight. Decision support capabilities were incorporated into the CPOE system to prevent inadvertent drug overdose when continuous infusion medications are prescribed. In addition, the CPOE system generates order sheets that include detailed instructions for pharmacists and nurses to safely process, compound and administer infusion orders.
We have conducted several different studies at our institution to evaluate the effect of this CPOE on patient safety during the entire continuous infusion medication management process (ordering, dispensing and administering stages) by comparing the system with the previously used handwritten (HW) system based on the rule-of-six. 13 This study focuses on the system effect on the medication dispensing process.
Pharmacists' practices are known for their high level of accuracy in compounding medications. Dispensing accuracy measured in 50 different pharmacies in six cities in the United States revealed an accuracy rate of 98.3 per 100 prescriptions. 14 In addition, the United States Pharmacopeia4 recommended limiting the preparation of all intravenous medications to pharmacists, and in 2003, The Joint Commission15 mandated the removal of dangerous medications (such as concentrated potassium chloride) from floor stocks and recommended the limiting of opiate and narcotic floor stocks. Furthermore, dispensing errors were found to be the least common type of errors when compared with medication prescribing and administration errors,16–19 although in some of these studies, the self-report of errors, which is inherently biased, was a major error-detection methodology. As a result, some studies recommended increasing the clinical responsibilities of pharmacists and involving pharmacists in physician rounds to decrease medication errors and enhance safety.20 On the other hand, using a direct observation technique, other studies found that dispensing errors were the second most common type of errors and accounted for 34% of the total potential adverse drug events in an ICU,21 and other studies classified 26% of the total reported dispensing errors (out of 82 errors) as significant errors.22 Methodological differences accounted for the difference in the detected dispensing error rate. Therefore, medication errors can result from any stage of the medication management process, and strategies should be implemented to decrease such errors.
The CPOE was found to be an effective strategy to decrease medication prescribing errors,23 although it is not a panacea.24 The introduction of a CPOE system requires a change at the institutional level that also involves restructuring the process of dispensing and administering medications. Therefore, examining the system effect on the medication dispensing process and capturing pharmacists' opinions about the system should be an integral part of CPOE evaluation. In general, there is limited evidence about the effect of CPOE systems on incidence of medication dispensing errors. In one study, the use of CPOE resulted in a 19% reduction in prescribing errors and a 68% reduction in medication dispensing errors.25 In addition, no previous studies have examined the effect of a CPOE system with standardized concentrations on decreasing errors of continuous infusion medications in a PICU. Furthermore, there is limited evidence about the safety of using standardized concentrations when compared with the rule-of-six method in delivering continuous infusion medications.9,26,27
Larsen et al. provided the highest error reduction data, showing a 73% decrease in errors upon the implementation of multiple interventions including standard concentrations, user-friendly medication labels and smart pump technology. However, handwritten or preprinted orders were used and not CPOE.9 Apkon et al. performed a failure mode effects analysis to compare rule-of-six ordering with standardized concentrations; results revealed lower risk priority numbers with the use of standardized concentrations.26 Lehmann et al. evaluated the effect of a calculator and a decision-support system to assist prescribers in ordering rule-of-six pediatric continuous intravenous infusions.27 Although this study did not look at the safety of standardized infusions, the authors claimed that since they found an initial 27% error rate in the handwritten rule-of-six infusion orders, this supports the use of standardized concentrations.
The purpose of the current study was to determine if CPOE-generated order sheets with standardized concentrations are better than rule-of-six HW orders with regard to pharmacy processing errors, processing time, and pharmacist satisfaction with CPOE-generated orders.
Materials and Methods
Design
Approval from the study hospital Institutional Review Board was obtained and participants were consented. The study was conducted in a quiet room in a tertiary care teaching hospital with a 24-bed PICU. All pharmacists in the pediatric satellite (n=12) were eligible to participate. Using a crossover design, participants were given test scenarios of HW and CPOE-generated order sheets and asked to process infusion orders using the computerized pharmacy system and generate infusion labels. Errors in the generated infusion labels were examined, as well as time to complete the task and pharmacist satisfaction with CPOE orders.
Dispensing Process of Continuous Infusion Medications
The dispensing process of continuous infusion orders at the study hospital has two steps: 1) order processing, which includes entering/selecting order parameters by the pharmacist using the computerized pharmacy system to generate an infusion label; and 2) order creation (compounding). The focus of this study was on order processing. The study was conducted six months after the implementation of CPOE in the PICU and the use of CPOE-generated order sheets by pharmacists. Prior to implementation, pharmacists used HW infusion orders that were processed using weight-based (rule-of-six) dosing and non-standardized concentrations.
The steps of the infusion dispensing process, using the CPOE and HW methods at the study hospital, are described in Appendix 1. As shown, integration of CPOE mnemonics for standardized concentrations into the computerized pharmacy system shortened order processing by decreasing the number of manual steps that required “typing in” order information and eliminating the need for calculation.
CPOE Order Sheets
The CPOE-generated order sheet with standardized concentrations has safety features for pharmacists to process and compound infusion orders (Appendix 2). These include legible and complete orders, a dosing-infusion rate reference table that helps quickly identify the correct dose-infusion rate relationship without the need for calculation, and a mnemonic for each drug that helps the pharmacist process the order (also without the need for calculation) using the computerized pharmacy system. Each continuous infusion drug was assigned a unique mnemonic, and these mnemonics were incorporated into the computerized pharmacy system. Each mnemonic consists of four components. For example, the mnemonic shown in Appendix 2 “std2000dobu2” is interpreted as follows: “std” refers to a standardized concentration; “2000” is the amount of drug that should be added to the ordered volume of the diluent; “dobu” refers to the drug dobutamine; and “2” refers to volume of the infusion, in this example, 2 refers to 250 mL.
Simulated Test Environment
In this study, participants were given infusion orders and were asked to generate infusion labels (process the order using the computerized pharmacy system). Each participant was required to process five computerized infusion orders, five error-free HW orders and four inaccurate HW orders. Since errors in ordering continuous infusions are common, and it is the pharmacist's responsibility to detect and correct these errors, the HW order sheet with four inaccurate infusion orders was used to check pharmacists' ability to identify and correct errors in order to mimic real-life practice. In this HW order sheet, two drugs were deliberately ordered with the wrong infusion rate (calculation errors), and the other two drugs were deliberately ordered with concentrations that exceeded the maximum recommended.
The selection of the drugs in the three order sheets was based on the most commonly used infusions in the PICU. Scenarios were based on realistic patient cases and constructed by two PICU physicians, two PICU nurses and two pediatric pharmacists.
Prior to the actual study, the entire testing procedure was pilot-tested using a senior and a junior pharmacist. Test subjects were able to complete the task accurately and indicated they received clear instructions. These subjects did not participate in the study.
Standardized instructions for participation were given to pharmacists at the beginning of the study, and testing sessions were conducted in a quiet room. The initial method (CPOE or HW orders) presented to participants to process the orders and generate infusion labels was randomly assigned to each pharmacist. Pharmacists were asked to check orders for accuracy, identify and correct the wrong order (by keeping the same dose ordered and without exceeding the maximum recommended concentration), process all infusion orders using the computerized pharmacy system, and print labels for all orders. In addition, each participant was required to identify his/her inability to process any order. Time required to process infusion orders for each order sheet was recorded. Finally, the pharmacist completed a user satisfaction questionnaire on the web. Help resources were available in the study room to participants while processing orders and included a list of the recommended maximum concentrations for each drug based on the pharmacy policy, a calculator, and the most commonly used drug information handbooks.
Main Outcome Measures
Medication Errors
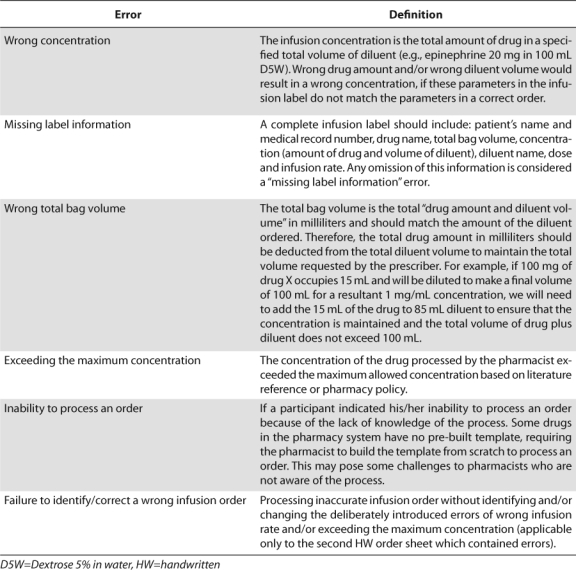
All infusion labels generated by participants were analyzed for errors using predetermined classifications (Table 1) that were based on the National Coordinating Council28 definition of medication errors. Errors that would result in a 100% deviation or more between dose specified in the order sheet and dose processed by pharmacists were classified as “high-risk” errors; all others were categorized as “low-risk” errors. This cutoff value was based on consensus of two PICU physicians and two pediatric pharmacists. Infusion labels were tested for errors by two independent researchers: a nurse and a pharmacist.
Table 1.
Targeted Errors in Infusion Labels
Time to Completion
Time to completion was measured as the total time required to process all infusion orders and to generate labels for all drugs in each order sheet.
User Satisfaction
User satisfaction was measured by a web-administered questionnaire consisting of four validated items selected from the literature29–31 based on a 5-point Likert response scale. Pharmacists were asked to indicate their agreement on each of four items about CPOE orders “as compared to HW orders.” Demographic data including age, sex, and computer skills, as well as information about pharmacist confidence in processing the orders, were collected via the questionnaire.
Data Analysis
Statistical tests included a paired sample t-test to compare time using the two methods, Wilcoxon test for paired data to compare percentages of medication errors using the two methods, one-sample t-test to compare user satisfaction between the two methods, and Pearson's correlation coefficient to examine relationships between variables. Data were analyzed using SPSS (version 12.5, SPSS Inc., Chicago, IL) with a significance level of 0.05. Since we already have a small number of available pharmacists (N=10), a priori power analysis to decide on the sample size was not conducted, and instead a convenience sampling approach of all willing pharmacists was utilized. However, a power analysis was conducted in order to decide on the number of infusions that should be processed by all pharmacists. Using t-test, results showed that we needed 51 infusions in each group (processing method) using an alpha level of 0.05 and a medium effect size of 0.5 to reach a power of 80% for a one-tailed directional hypothesis. This means that each of the 10 available pharmacists (see results section) had to process 5 infusions using each processing method.
RESULTS
Pharmacist Characteristics
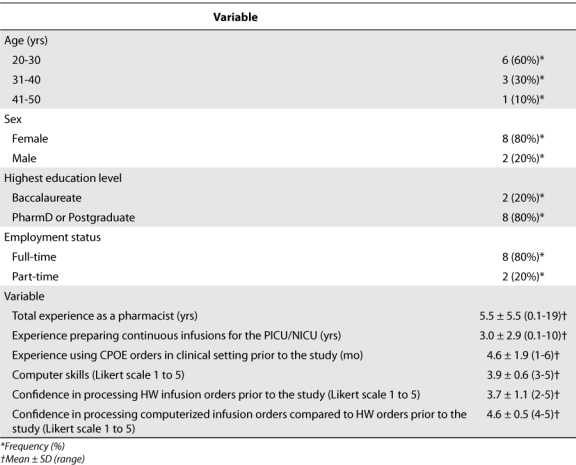
Out of the 12 pharmacists in the pediatric satellite, 10 participated in the study. The other 2 pharmacists were excluded form the study as they participated in the testing procedure of the scenarios. Participant characteristics are described in Table 2. Participants varied widely in years of experience as a pharmacist, years of experience in processing continuous infusion orders for the pediatric/neonatal ICU, and average number of months using the computerized orders in the pharmacy. Only 2 of 10 pharmacists reported less than one year of experience in the profession or in processing continuous infusions. The majority of pharmacists (6 of 10) had used the computerized orders for six months at the time of the study, and the others reported one to three months of use. Mean self-reported computer skills were “above average” using a 5-point Likert type scale (3.9 ± 0.6). Pharmacists varied in their confidence “before this study” to process HW infusion orders based on a 5-point Likert type scale (3.7 ± 1.1), although half were “moderately confident.” In contrast, there was a little variability in confidence to process computerized orders “before this study” when compared with HW orders (4.6 ± 0.5).
Table 2.
Pharmacist Demographics (n=10)
Time to Process Continuous Infusion Orders
With the CPOE method, the average processing time per one infusion order was 2 min, 5 sec (± 58 sec) as compared to 3 min, 7 sec (± 1 min, 20 sec) in the first HW order sheet (p=0.01), and 3 min and 26 seconds (1 min, 8 sec) in the second HW order sheet (p=0.001) (Figure 1).
Figure 1.
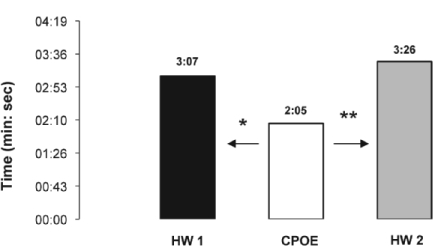
Average processing time per one infusion order using computerized prescriber order entry (CPOE) and handwritten (HW) order sheets. *p=0.01, **p= 0.001.
There was no relationship between total time spent processing infusion orders using each of the HW order sheets and duration of using the CPOE orders in real clinical practice in the pharmacy (p>0.05).
Medication Errors in Processing Continuous Infusion Orders
There was a 100% agreement between the nurse and the pharmacist who analyzed the errors in infusion labels.
Incidence of Errors
Each of the 10 participants processed five correct infusion orders generated by the CPOE method (total 50 orders), five correct orders for the first HW order sheet (total 50 orders), and four inaccurate infusion orders for the second HW order sheet (total 40 orders). With the CPOE method, there were two infusions (4%) with processing errors, compared with 13 infusions (26%) for the first HW order sheet (p=0.03) and 18 infusions (45%) for the second HW order sheet (p=0.007) (Figure 2). Some of the infusion labels had more than one error type (e.g., exceeded maximum concentration and had missing label information). Errors in the CPOE method were committed by two of the 10 participants, while errors in the first and second groups of HW orders were committed by seven and nine of the 10 participants, respectively.
Figure 2.
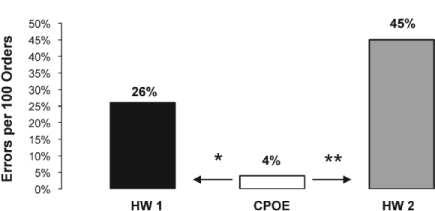
Percentage of errors using computerized prescriber order entry (CPOE) and handwritten (HW) orders. *p= 0.03; **p=0.007.
Although the difference in errors between the two HW order sheets (processing correct infusion orders vs. orders with deliberate errors placed within them) was not part of the study purpose, interestingly, there was no difference in the percentage of infusions with processing errors (p>.05). Typically, one would expect fewer errors when correct infusion orders are being processed.
Types of Errors
There was a total of two error elements while processing the computerized orders, 15 error elements for the first group of HW orders and 21 error elements for the second group of HW orders. No relationship was found between the total number of errors in each of the HW order sheets and duration of using CPOE orders in clinical practice (p>0.05).
With CPOE orders, the only error type found was wrong concentration (Table 3). One error was a result of selecting twice the concentration ordered from the computerized pharmacy system (500 mcg of epinephrine in 250 mL diluent instead of 200 mcg in 100 mL diluent). Although this type of error would not result in a dosing error, it would result in waste. The other error resulted from selecting a wrong drug amount (Table 4), which would result in a wrong dose. In addition to these two errors, two participants processed two different infusion orders without using the mnemonics.
Table 3.
. Error Type Using CPOE and Handwritten Orders
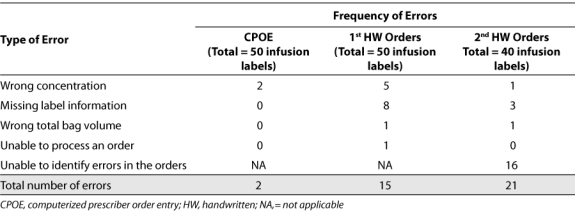
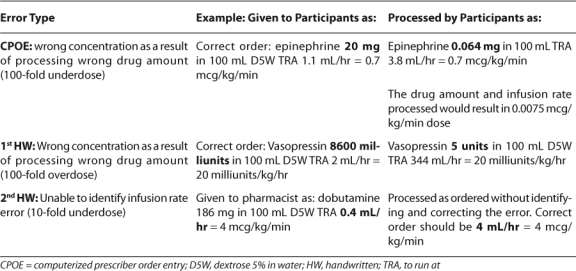
Table 4.
Examples of High-Risk Errors Processed By the Participants
For the first HW order sheet, wrong concentration was also common (5 errors), although missing label information was the most common type of error (8 errors). This included omitting the dose and infusion rate information. In addition, one of the participants indicated his/her inability to process a vasopressin order due to confusion about how to appropriately process the medication order.
With the second HW order sheet, the most common type of error was failure to identify and to correct the deliberate errors (two infusion rate errors and 14 exceeding maximum concentration), which resulted in orders being processed incorrectly.
High Risk Errors
With the CPOE method, there was one infusion (2%) processed with high-risk errors, not statistically different from the 5 infusions with high risk errors (10%) in the first group of HW orders, or the 4 infusions (10%) in the second HW order sheet (p>0.05). The majority of high-risk errors in both methods resulted from processing the wrong drug amount. High-risk errors in the CPOE method and in the first HW orders would result in 100-fold over- or underdose. Table 4 illustrates some actual orders processed by pharmacists as examples of high-risk errors.
Pharmacist Satisfaction with CPOE Orders
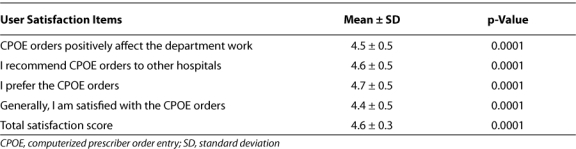
The reliability of the pharmacist satisfaction questionnaire was high (Cronbach's alpha= 0.70). Pharmacists were more satisfied with CPOE when compared with the HW method at each individual item and at the scale level (p=0.0001) (Table 5).
Table 5.
. User Satisfaction with CPOE vs. Handwritten Orders (n=10)
DISCUSSION
Continuous infusion medications are vital in the treatment of critically ill children. However, intravenous medication delivery is associated with a high level of errors and adverse drug events.2,3 Although a few studies are available about errors associated with continuous infusion medications, to our knowledge, no study addresses errors associated with infusion labels generated by pharmacists processing continuous infusion orders comparing computerized orders with standardized concentrations and HW orders. Infusion labels are used to prepare and compound medications; therefore, errors in the labels may result in preparing and delivering the wrong medication to patient units. In addition, infusion labels are a main reference for nurses to program infusion pumps. This study focused on processing continuous infusions for pediatric patients by comparing CPOE-generated orders using standardized concentrations with HW orders using rule-of-six method. Major findings of this study showed that CPOE-generated orders with standardized concentrations significantly decreased errors in this process, shortened time required by pharmacists to process orders and resulted in satisfied users.
The use of CPOE orders with standardized concentrations resulted in 33% to 39% reduction in the time spent processing each infusion order. This anticipated finding reflects the positive changes in processing infusion orders as a result of integrating CPOE mnemonics for standardized concentrations into the pharmacy system, which, in turn, results in reducing unnecessary activities and eliminating the need for calculation. In the pediatric pharmacy, there is an average of three infusion orders processed every hour, which results in a total of 72 orders per day. This study showed that the time saved per infusion order ranged from 1 min to 1 min, 20 sec. Accordingly, this would result in a total time savings of 72 min to 93 min a day.
Errors in the HW method were very common and committed by almost all participants. More surprisingly, almost all participants were unable to identify erroneous orders in the second HW order sheet, and there was no difference between the number of errors in processing correct and incorrect HW infusion orders. This suggests that processing rule-of-six orders is a high-risk process for errors, even when orders are written correctly with no errors. Of particular importance to note is that 10% of the orders processed in each HW order sheet contained high-risk errors that would result, in some cases, in a 100-fold overdose. Although the 2% error rate in CPOE orders was not statistically different from the handwritten orders, it may be clinically significant. In addition, some of the rule-of-six orders were too challenging for some pharmacists to process. These errors occurred even though the selection of drugs in our study was based on the most commonly used drugs in the PICU. Data also showed that the high error rate found in the HW method was not associated with the period of using CPOE orders in real clinical practice; therefore, it is less likely that the time lapsed of not processing HW orders (since pharmacists stopped using these orders 6 months before conducting the study) would affect the accuracy of processing these orders in this study.
Use of CPOE orders resulted in an 81% reduction of infusion processing errors, but it did not eliminate the wrong concentration errors. One of these errors resulted from mistakenly identifying a drug concentration as one that exceeded the maximum recommended by one of the participants following the concentration limits used in the old HW system, which resulted in changing the drug amount by the pharmacist to generate a label. This can be attributed to ineffective communication about the updates in drug concentrations after using CPOE orders. Studies showed that although a simple CPOE system had the potential to decrease medication errors by 66%, effective communication between healthcare team members had the potential to decrease errors by 76%.32 Although CPOE orders eliminated the missing information in infusion labels, which is a critical benefit that will enhance communication between healthcare team members as nurses depend on this information to program infusion pumps, effective communication about changes resulting from implementing the technology is critical for patient safety.
Another error that resulted from using CPOE orders was related to possible selection of the wrong drug concentration from the computerized pharmacy system. This critical finding suggests that integrating decision support systems into the pharmacy system and a double-check policy are important to prevent such an error from occurring.
Despite the benefits of CPOE orders, the possibility of processing infusion orders without using the mnemonics was an unexpected finding and has considerable implications. Implementing the correct technology is not sufficient to deliver a safe practice. Noncompliance in using mnemonics may increase the likelihood of committing other types of errors found in the HW system and suggests the need for forced use of mnemonics for order processing. This approach would provide a standardized process for the appropriate use of the computerized orders.
Pharmacists felt more confident in processing the computerized orders and were significantly more satisfied with CPOE orders, indicating that the system was carefully designed to meet user needs.
Consistent with other findings, this study found that HW medication systems in pediatric settings are error-prone,2 errors of continuous infusions are very frequent,6,10 many are important errors that may result in adverse events,33 and that CPOE did not eliminate all types of errors.23
We responded to The Joint Commission mandate of the transition to standardized concentrations using a comprehensive, computerized, and easily customizable solution that can be used by different pediatric institutions. Our CPOE system was found to be a very effective strategy in decreasing errors of processing orders and in saving clinicians' time. This CPOE was a stand-alone system designed with the possibility of easy future integration into a larger CPOE system. Our system is relatively easy to implement and had immediate benefits at the point of care; thus, offering a practical solution for institutions who face the challenge of implementing a large CPOE system. Widespread use of the CPOE system in this study by different healthcare institutions may encourage pharmaceutical manufacturers to produce two to four standardized concentrations for each continuous infusion medication, which may have great potential for decreasing medication manipulation, perhaps further reducing medication errors and waste.
The current study has some limitations. First, the study examined the use of CPOE-generated infusion orders for children; therefore, the results may not be applicable to other CPOE systems. Second, we examined errors using a simulation methodology that may be different than the error rate which occurred in real clinical practice; however, our simulation mimicked the exact steps of order processing in real-life practice. In addition, the use of simulation identified new limitations of the HW ordering systems and explored types of errors that have never been investigated in previous studies, such as the inability of the pharmacist to identify erroneous orders or process infusion orders. It also facilitated examining different variables, such as errors and time, in a manageable way. Finally, although the sample included all pharmacists in the pediatric satellite, it consisted of only 10 participants, which hindered conducting extra analyses to investigate the relationships between pharmacist characteristics and main study outcomes.
In conclusion, errors of processing continuous infusions are very common in the pediatric population. The implementation of effective system-based error prevention strategies should be a priority in pediatric hospitals. The rule-of-six HW medication management system has inherent weaknesses that can be managed by using CPOE with standardized concentrations; however, CPOE is not a panacea. CPOE orders with standardized concentrations resulted in faster medication processing and more satisfied users, and they greatly decreased errors associated with processing infusion orders. More attention is warranted regarding the integration of CPOE into the pharmacy system and pharmacists' compliance with the appropriate use of CPOE orders. Effective communication about the changes introduced by CPOE into different work processes is vital to improving patient safety. Future studies should evaluate the effect of the additional enhancements of CPOE on eliminating errors.
ABBREVIATIONS
- CPOE
computerized prescriber order entry
- HW
handwritten
- ICU
Intensive Care Unit
- PICU
Pediatric Intensive Care Unit
Appendix 1.
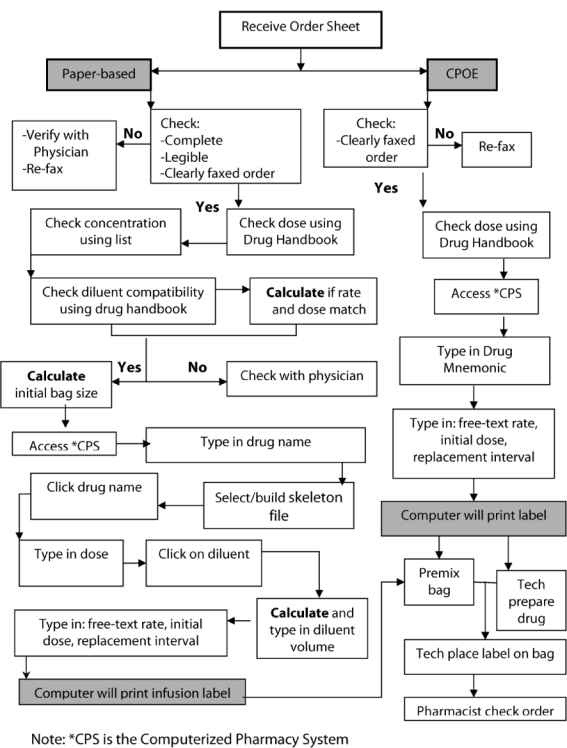
Description of the Medication Dispensing Process Using HW vs. CPOE Orders.
Appendix 2.
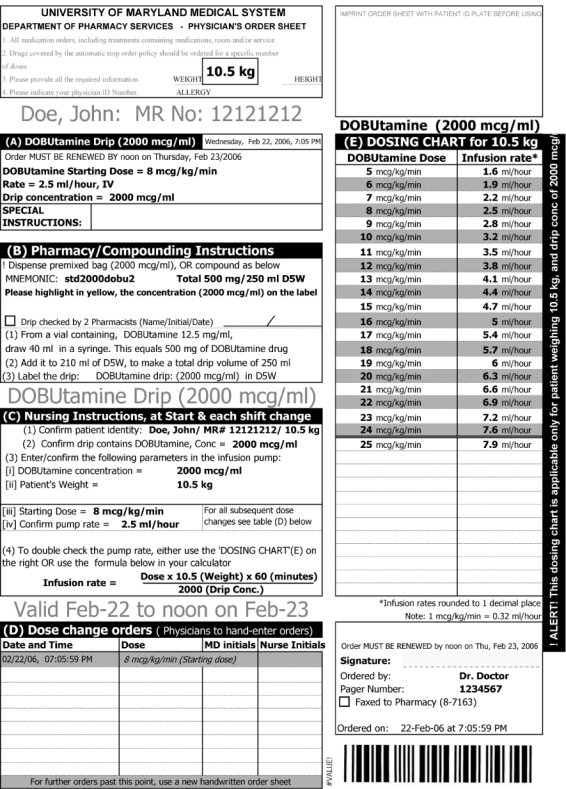
CPOE Medication Order Sheet.
Footnotes
DISCLOSURE Drs. Sowan and Soeken declare no conflicts or financial interests in any product or service mentioned in the manuscript, including grants, equipment, medications, employment, and gifts. Drs. Hilmas and Vaidya receive royalties from Accupedia.
REFERENCES
- 1.Wilson D, McArtney R, Newcombe R, et al. Medication errors in pediatric practice: insights from a continuous quality improvement approach. Eur J Pediatr. 1998;157:769–774. doi: 10.1007/s004310050932. [DOI] [PubMed] [Google Scholar]
- 2.Kaushal R, Bates D, Landrigan C, et al. Medication errors and adverse drug events in pediatric inpatients. JAMA. 2001;285:2114–2120. doi: 10.1001/jama.285.16.2114. [DOI] [PubMed] [Google Scholar]
- 3.Ross L, Wallace J, Paton Y. Medication errors in a pediatric teaching hospital in the UK: five years' operational experience. Arch Dis Child. 2000;83:492–497. doi: 10.1136/adc.83.6.492. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.United States Pharmacopeia. Seniors are at risk for medical errors in hospitals. Available at: http://www.uspharmacist.com/index.asp?show=article&page=8_1198.htm. Accessed March 25, 2008.
- 5.Institute for Safe Medication Practice. ISMP's list of high-alert medications. Available at: http://www.ismp.org/Tools/highalertmedications.pdf. Accessed February 25, 2008.
- 6.Taxis K, Barber N. Ethnography study of incidence and severity of intravenous drug errors. Br Med J. 2003;326:684. doi: 10.1136/bmj.326.7391.684. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.McLeroy P. The rule of six: calculating intravenous infusions in a pediatric crisis situation. Hosp Pharm. 1994;29:939–943. [PubMed] [Google Scholar]
- 8.Lesar T. Errors in the use of medication dose equations. Arch Pediatr Adolesc Med. 1998;152:340–344. doi: 10.1001/archpedi.152.4.340. [DOI] [PubMed] [Google Scholar]
- 9.Larsen G, Parker H, Cash J, et al. Standard drug concentrations and smart-pump technology reduce continuous-medication-infusion errors in pediatric patients. Pediatrics. 2005;116:21–25. doi: 10.1542/peds.2004-2452. [DOI] [PubMed] [Google Scholar]
- 10.Herout P, Erstad B. Medication errors involving continuously infused medications in a surgical intensive care unit. Crit Care Med. 2004;32:428–432. doi: 10.1097/01.CCM.0000108876.12846.B7. [DOI] [PubMed] [Google Scholar]
- 11.Rich D. Ask the Joint Commission: more on the requirements of the medication-related National Patient Safety Goals for 2003–2004. Hosp Pharm. 2003;38:977–989. [Google Scholar]
- 12.Vaidya V, Gaffoor M, Hilmas E, et al. New York, NY: 2004 Sep. 30. A computerized program for changing from rule-of-six to standardized drips. Poster presented at: Pediatric Critical Care Colloquium. [Google Scholar]
- 13.Hilmas E, Sowan A, Gaffoor M, et al. Implementation and evaluation of a comprehensive system to deliver pediatric continuous infusion medications with standardized concentrations. Am J Health-Syst Pharm. 2010;67:58–69. doi: 10.2146/ajhp080598. [DOI] [PubMed] [Google Scholar]
- 14.Flynn E, Barker K, Carnahan B. National observational study of prescription dispensing accuracy and safety in 50 pharmacies. J Am Pharm Assoc. 2003;43:191–200. doi: 10.1331/108658003321480731. [DOI] [PubMed] [Google Scholar]
- 15.The Joint Commission for Accreditation of Healthcare Organizations. JCAHO Patient Safety Goals 2003. Available at: http://www.va.gov/ncps/TIPS/Docs/TIPSDec02.doc. Accessed February 28, 2008. [PubMed]
- 16.Bates D, Cullen D, Laird N, et al. Incidence of adverse drug events and potential adverse drug events: implications for prevention. JAMA. 1995;274:29–34. [PubMed] [Google Scholar]
- 17.Gurwitz J, Field T, Harrold L, et al. Incidence and preventability of adverse drug events among older persons in the ambulatory setting. JAMA. 2003;289:1107–16. doi: 10.1001/jama.289.9.1107. [DOI] [PubMed] [Google Scholar]
- 18.Leape L, Bates D, Cullen D, et al. Systems analysis of adverse drug events. JAMA. 1995;274:35–43. [PubMed] [Google Scholar]
- 19.Nebeker J, Hoffman J, Weir C, et al. High rates of adverse drug events in a highly computerized hospital. Arch Intern Med. 2005;165:1111–1116. doi: 10.1001/archinte.165.10.1111. [DOI] [PubMed] [Google Scholar]
- 20.Brown G. Assessing the clinical impact of pharmacists' interventions. Am J Hosp Pharm. 1991;8:2644–2647. [PubMed] [Google Scholar]
- 21.Kopp B, Erstad B, Allen M, et al. Medication errors and adverse drug events in an intensive care unit: direct observation approach for detection. Crit Care Med. 2006;34:415–425. doi: 10.1097/01.ccm.0000198106.54306.d7. [DOI] [PubMed] [Google Scholar]
- 22.Rolland P. Occurrence of dispensing errors and efforts to reduce medication errors at the Central Arkansas Veteran's healthcare system. Drug Safety. 2004;27:271–282. doi: 10.2165/00002018-200427040-00004. [DOI] [PubMed] [Google Scholar]
- 23.Bates D, Teich J, Lee J, et al. The impact of computerized physicians order entry on medication error prevention. JAMA. 1999;6:313–321. doi: 10.1136/jamia.1999.00660313. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Koppel R, Metlay J, Cohen A, et al. Role of computerized physician order entry systems in facilitating medication errors. JAMA. 2005;293:1179–1203. doi: 10.1001/jama.293.10.1197. [DOI] [PubMed] [Google Scholar]
- 25.Bates D, Leape L, Cullen D, et al. Effect of computerized physician order entry and a team intervention on prevention of serious medication errors. JAMA. 1998;280:1311–1316. doi: 10.1001/jama.280.15.1311. [DOI] [PubMed] [Google Scholar]
- 26.Apkon M, Leonard J, Probst L, et al. Design of a safer approach to intravenous drug infusions: failure mode effects analysis. Qual Saf Health Care. 2004;13:265–71. doi: 10.1136/qshc.2003.007443. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Lehmann CU, Kim GR, Gujral R, et al. Decreasing errors in pediatric continuous intravenous infusions. Pediatr Crit Care. 2006;7:225–230. doi: 10.1097/01.PCC.0000216415.12120.FF. [DOI] [PubMed] [Google Scholar]
- 28.National Coordinating Council. The National Coordinating Council for Medication Error Reporting and Prevention. Available at: http://www.nccmerp.org/pdf/report-Final2005-11-29.pdf. Accessed February 25, 2008.
- 29.Lee F, Teich J, Spurr C, Bates D. Implementation of physician order entry: user satisfaction and self-reported usage patterns. J Am Med Inform Assoc. 1996;3:42–55. doi: 10.1136/jamia.1996.96342648. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.O'Connell R, Cho C, Shah N, et al. Take note(s): differential EHR satisfaction with two implementations under one roof. J Am Med Inform Assoc. 2004;11:43–49. doi: 10.1197/jamia.M1409. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Rosenbloom T, Talbertc D, Aronsky D. Clinicians' perceptions of clinical decision support integrated into computerized provider order entry. Int J Med Inform. 2004;73:433–441. doi: 10.1016/j.ijmedinf.2004.04.001. [DOI] [PubMed] [Google Scholar]
- 32.Fortescue E, Kaushal R, Ladrigan C, et al. Prioritizing strategies for preventing medication errors and adverse drug events in pediatric inpatients. Pediatrics. 2003;111:722–729. doi: 10.1542/peds.111.4.722. [DOI] [PubMed] [Google Scholar]
- 33.Rothschild J, Keohane C, Cook E, et al. A controlled trial of smart infusion pumps to improve medication safety in critically ill patients. Crit Care Med. 2005;33:533–540. doi: 10.1097/01.ccm.0000155912.73313.cd. [DOI] [PubMed] [Google Scholar]