

Abstract
Background
The optimal strategy for resectable synchronous colorectal liver metastases remains controversial. Although some authors advocate a staged treatment, an increasing number of studies have reported that combined colorectal and liver resection is safe. Laparoscopic combined resection in primary colorectal cancer with synchronous liver metastases has been reported but there are no specific data for major liver resections. In the present study, we evaluated the feasibility of a simultaneous entirely laparoscopic procedure, in the light of the benefits of laparoscopy in both colon and liver surgery, and discussed the benefits of this strategy.
Methods
Two cases are presented of totally laparoscopic major liver resections associated with laparoscopic colorectal resections for synchronous liver metastases with the emphasis on the technical aspects. Duration of surgery, blood loss and post-operative outcome were evaluated.
Results
Laparoscopic right hepatectomy or left hepatectomy with simultaneous colon resection for liver metastasis was feasible and safe with only one suprapubic 5-mm trocar added to the usual trocar sites. The mean duration of surgery was 327 min with a mean estimated blood loss of 200 ml. The post-operative course was uneventful.
Discussion
In selected patients, laparoscopic major hepatectomies for unilobular synchronous metastases can be safely performed simultaneously with colorectal surgery.
Keywords: hepatectomy, laparoscopy, synchronous metastasis, major liver resection, colorectal surgery
Introduction
Laparoscopic colon resection for cancer has been shown to be safe and oncologically equivalent to conventional surgery.1–3 Moreover, it reduces hospital stay, shortens recovery times and reduces post-operative complications.4–7 Among patients newly diagnosed with colorectal cancer, approximately 20% are found to have synchronous metastases.8,9 The optimal strategy for resectable synchronous colorectal liver metastases remains controversial. Although some authors advocate a staged treatment,10–12 an increasing number of studies have reported that combined colorectal and liver resection is feasible and safe.13–22 However, there is currently little information available on colorectal resection associated with major liver resection.13
Laparoscopic liver surgery is now recognized as safe, with surgical and post-operative outcomes showing some improvement in minor liver resections. Successful laparoscopic major resections have been reported recently by expert teams in hepatic surgery and laparoscopy.23 Laparoscopic combined colon and liver resection in primary colorectal cancer with synchronous liver metastases has been reported24–27 but there are no data specific to major liver resections.
The feasibility of a simultaneous entirely laparoscopic procedure is evaluated, in the light of the benefits of laparoscopy in both colon surgery and liver resection, and the benefits of this combined strategy are discussed.
Patients and results
Case 1
A 36-year-old woman presented with intermittent pain in the right upper quadrant. A computed tomography (CT) revealed a 25-mm lesion centrally located in the right liver (Fig. 1). Colonoscopy revealed an ileo-colic mass measuring 4 cm and two polyps of 15 and 8 mm in the right colon. Biopsy of the ileo-colic tumour showed a well-differentiated endocrine carcinoma. OctreoScan scintigraphy was negative. Serum levels of chromogranin A and serotonin were normal.
Figure 1.
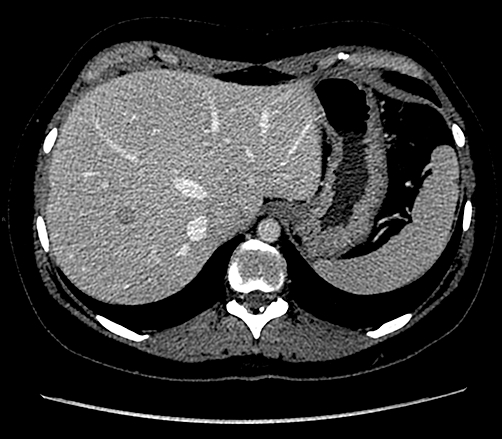
Computed tomography showing the lesion in the right liver of patient 1
Given that both lesions were on the right side a simultaneous laparoscopic resection was attempted by the same surgical team. The patient was placed supine, legs apart and the placement of trocars is shown in Fig. 2. Only one suprapubic 5-mm trocar was added to the usual trocar sites for right hepatectomy. The operating surgeon took a position between the legs for hepatectomy and on the left side for colon resection. A laparoscopic right hepatectomy was performed after an initial extraparenchymal control of vascular inflow and outflow as well as a complete mobilization of the right liver as previously described.28,29 A short suprapubic incision was made for specimen extraction and to perform a hand-sewn ileo-colic anastomosis. The estimated blood loss was 200 ml and the duration of surgery was 310 min. The post-operative course was uneventful and the patient was discharged on day four.
Figure 2.
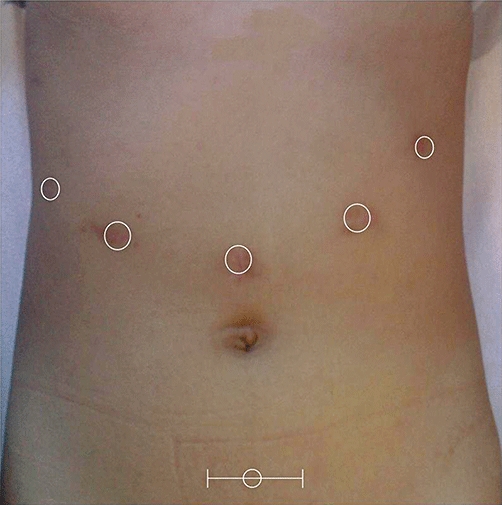
Trocars placement for laparoscopic right or left hepatectomy combined with a colonic resection
Case 2
A 78-year-old man presented with symptoms of rectal bleeding and colonoscopy showed a sigmoid adenocarcinoma of the colon located 18 cm from the anal verge and a CT revealed a 45-mm lesion of the left liver (Fig. 3). The patient demonstrated partial response to neoadjuvant chemotherapy and a simultaneous colonic and hepatic resection was planned.
Figure 3.
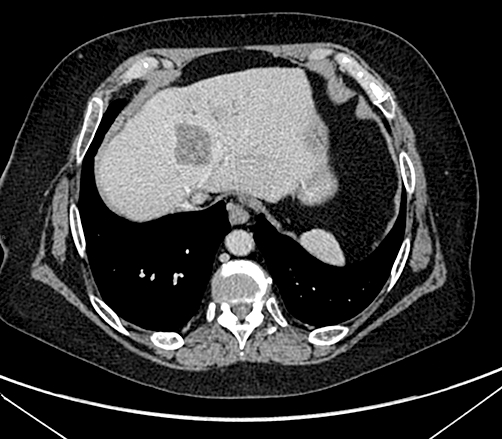
Computed tomography showing the tumour in left liver of patient 2
Both resections were performed in a similar manner to the previous case. The operating surgeon took up a position between the legs of the patient with an assistant on the left for the left hepatectomy. The surgical procedure for left hepatectomy with prior vascular control of the portal pedicle and the left hepatic vein has been described elsewhere30,31 (Fig. 4). The operating surgeon changed his position to the right side for colon resection. A circular stapler was used to perform a colorectal anastomosis. The procedure was well tolerated, with an estimated blood loss of 200 ml and a total operative time of 345 min. The post-operative course was uneventful and the hospital stay lasted 6 days.
Figure 4.
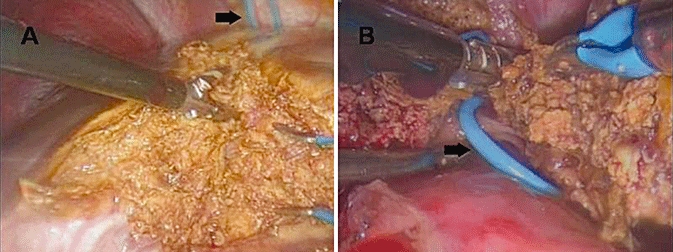
(a) Parenchymal transection during a left hepatectomy, performed with a thermofusion device. (b) The hepatic vein previously controlled with a vessel loop (black arrow) is sectioned at the end of liver division
Discussion
The surgical strategy remains controversial for patients diagnosed with liver metastases at the same time as a primary tumour. A staged treatment was advocated because synchronous resection gave poorer post-operative results.10–12 The high morbidity and mortality rates were attributed to the association of a clean surgical procedure with one likely to cause contamination. Moreover, impaired liver protein function after liver resection may result in the patient becoming vulnerable to infection and anastomotic leakage.32,33 Furthermore, liver pedicle clamping causes transient portal hypertension. This may impair colonic anastomosis as a result of intestinal oedema which increases the risk of anastomotic leakage.12,34,35 Authors reluctant to perform synchronous resections argue that incisions for simultaneous surgery preclude adequate liver exploration and safe vascular control of the inferior vena cava and the hepatic veins.12
However, an increasing number of studies have reported that combined colorectal and liver resection is feasible and safe14–22 but the majority of these report wedge or minor resections. Capussotti et al.13 were the first to focus on major liver resections and demonstrate similar mortality rates to those for patients undergoing staged resections. Post-operative complication rates were higher and post-operative hospital stay longer for staged procedures than those for the simultaneous resection group.
Compared with conventional laparotomy, the laparoscopic approach has several advantages. Laparoscopy is increasingly used in the treatment of colorectal liver metastases.36,37 Studies of both colorectal1–3 and liver surgery38–40 concluded that laparoscopy was associated with lower morbidity, less pain, a faster recovery and a shorter hospital stay than open surgery, without compromising oncological clearance. Life expectancy for patients with colorectal cancer has increased, thus considerable numbers of patients with metastatic disease survive for long periods with an acceptable and improved quality of life.41 Repeated surgery is often required, making laparoscopy particularly beneficial for these patients. Bretagnol et al.24 reported 10 colorectal laparoscopic resections accompanied by open liver resection, which included one patient who underwent an open right hepatectomy. Studies on this topic devoted entirely to laparoscopy involve minor resections and left lateral sectionectomies.24,25 To the best of our knowledge, this is the first study reporting simultaneous, entirely laparoscopic major liver resection associated with a laparoscopic colorectal resection.
We showed that laparoscopic colon resection with synchronous right hepatectomy or left hepatectomy for liver metastasis was feasible and safe with the addition of only one extra trocar. The selective control of vascular inflow and outflow performed in our technique for anatomical liver resections allowed a bloodless parenchymal transection with no need for additional clamping. Blood loss was low in the two cases reported and the lack of need for clamping enabled the anastomosis to be performed without portal hypertension or intestinal oedema.
Laparoscopic major hepatectomies can be performed safely for unilobular synchronous metastasis at the same time as colorectal surgery in selected patients. Larger series and prospective studies are still needed to confirm the advantages of this combined strategy.
Conflicts of interest
None declared.
References
- 1.Lacy AM, Delgado S, Castells A, Prins HA, Arroyo V, Ibarzabal A, et al. The long-term results of a randomized clinical trial of laparoscopy-assisted versus open surgery for colon cancer. Ann Surg. 2008;248:1–7. doi: 10.1097/SLA.0b013e31816a9d65. [DOI] [PubMed] [Google Scholar]
- 2.Fleshman J, Sargent DJ, Green E, Anvari M, Stryker SJ, Beart RW, et al. Laparoscopic colectomy for cancer is not inferior to open surgery based on 5-year data from the COST Study Group trial. Ann Surg. 2007;246:655–662. doi: 10.1097/SLA.0b013e318155a762. [DOI] [PubMed] [Google Scholar]
- 3.Jayne DG, Guillou PJ, Thorpe H, Quirke P, Copeland J, Smith AM, et al. Randomized trial of laparoscopic-assisted resection of colorectal carcinoma: 3-year results of the UK MRC CLASICC Trial Group. J Clin Oncol. 2007;25:3061–3068. doi: 10.1200/JCO.2006.09.7758. [DOI] [PubMed] [Google Scholar]
- 4.Veldkamp R, Kuhry E, Hop WC, Jeekel J, Kazemier G, Bonjer HJ, et al. Laparoscopic surgery versus open surgery for colon cancer: short-term outcomes of a randomised trial. Lancet Oncol. 2005;6:477–484. doi: 10.1016/S1470-2045(05)70221-7. [DOI] [PubMed] [Google Scholar]
- 5.Lacy AM, Garcia-Valdecasas JC, Delgado S, Castells A, Taura P, Pique JM, et al. Laparoscopy-assisted colectomy versus open colectomy for treatment of non-metastatic colon cancer: a randomised trial. Lancet. 2002;359:2224–2229. doi: 10.1016/S0140-6736(02)09290-5. [DOI] [PubMed] [Google Scholar]
- 6.Guillou PJ, Quirke P, Thorpe H, Walker J, Jayne DG, Smith AM, et al. Short-term endpoints of conventional versus laparoscopic-assisted surgery in patients with colorectal cancer (MRC CLASICC trial): multicentre, randomised controlled trial. Lancet. 2005;365:1718–1726. doi: 10.1016/S0140-6736(05)66545-2. [DOI] [PubMed] [Google Scholar]
- 7.Clinical Outcomes of Surgical Therapy Study Group. A comparison of laparoscopically assisted and open colectomy for colon cancer. N Engl J Med. 2004;350:2050–2059. doi: 10.1056/NEJMoa032651. [DOI] [PubMed] [Google Scholar]
- 8.Leporrier J, Maurel J, Chiche L, Bara S, Segol P, Launoy G. A population-based study of the incidence, management and prognosis of hepatic metastases from colorectal cancer. Br J Surg. 2006;93:465–474. doi: 10.1002/bjs.5278. [DOI] [PubMed] [Google Scholar]
- 9.Manfredi S, Lepage C, Hatem C, Coatmeur O, Faivre J, Bouvier AM. Epidemiology and management of liver metastases from colorectal cancer. Ann Surg. 2006;244:254–259. doi: 10.1097/01.sla.0000217629.94941.cf. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Bolton JS, Fuhrman GM. Survival after resection of multiple bilobar hepatic metastases from colorectal carcinoma. Ann Surg. 2000;231:743–751. doi: 10.1097/00000658-200005000-00015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Nordlinger B, Guiguet M, Vaillant JC, Balladur P, Boudjema K, Bachellier P, et al. Surgical resection of colorectal carcinoma metastases to the liver. A prognostic scoring system to improve case selection, based on 1568 patients. Association Francaise de Chirurgie. Cancer. 1996;77:1254–1262. [PubMed] [Google Scholar]
- 12.Belghiti J. [Synchronous and resectable hepatic metastases of colorectal cancer: should there be a minimum delay before hepatic resection?] Ann Chir. 1990;44:427–429. [PubMed] [Google Scholar]
- 13.Capussotti L, Ferrero A, Vigano L, Ribero D, Lo Tesoriere R, Polastri R. Major liver resections synchronous with colorectal surgery. Ann Surg Oncol. 2007;14:195–201. doi: 10.1245/s10434-006-9055-3. [DOI] [PubMed] [Google Scholar]
- 14.Weber JC, Bachellier P, Oussoultzoglou E, Jaeck D. Simultaneous resection of colorectal primary tumour and synchronous liver metastases. Br J Surg. 2003;90:956–962. doi: 10.1002/bjs.4132. [DOI] [PubMed] [Google Scholar]
- 15.Martin R, Paty P, Fong Y, Grace A, Cohen A, DeMatteo R, et al. Simultaneous liver and colorectal resections are safe for synchronous colorectal liver metastasis. J Am Coll Surg. 2003;197:233–241. doi: 10.1016/S1072-7515(03)00390-9. [DOI] [PubMed] [Google Scholar]
- 16.Elias D, Detroz B, Lasser P, Plaud B, Jerbi G. Is simultaneous hepatectomy and intestinal anastomosis safe? Am J Surg. 1995;169:254–260. doi: 10.1016/S0002-9610(99)80146-9. [DOI] [PubMed] [Google Scholar]
- 17.Schlag P, Hohenberger P, Herfarth C. Resection of liver metastases in colorectal cancer – competitive analysis of treatment results in synchronous versus metachronous metastases. Eur J Surg Oncol. 1990;16:360–365. [PubMed] [Google Scholar]
- 18.Vogt P, Raab R, Ringe B, Pichlmayr R. Resection of synchronous liver metastases from colorectal cancer. World J Surg. 1991;15:62–67. doi: 10.1007/BF01658964. [DOI] [PubMed] [Google Scholar]
- 19.Lyass S, Zamir G, Matot I, Goitein D, Eid A, Jurim O. Combined colon and hepatic resection for synchronous colorectal liver metastases. J Surg Oncol. 2001;78:17–21. doi: 10.1002/jso.1117. [DOI] [PubMed] [Google Scholar]
- 20.de Santibanes E, Lassalle FB, McCormack L, Pekolj J, Quintana GO, Vaccaro C, et al. Simultaneous colorectal and hepatic resections for colorectal cancer: postoperative and longterm outcomes. J Am Coll Surg. 2002;195:196–202. doi: 10.1016/s1072-7515(02)01235-8. [DOI] [PubMed] [Google Scholar]
- 21.Chua HK, Sondenaa K, Tsiotos GG, Larson DR, Wolff BG, Nagorney DM. Concurrent vs. staged colectomy and hepatectomy for primary colorectal cancer with synchronous hepatic metastases. Dis Colon Rectum. 2004;47:1310–1316. doi: 10.1007/s10350-004-0586-z. [DOI] [PubMed] [Google Scholar]
- 22.Tanaka K, Shimada H, Matsuo K, Nagano Y, Endo I, Sekido H, et al. Outcome after simultaneous colorectal and hepatic resection for colorectal cancer with synchronous metastases. Surgery. 2004;136:650–659. doi: 10.1016/j.surg.2004.02.012. [DOI] [PubMed] [Google Scholar]
- 23.Dagher I, O'Rourke N, Geller DA, Cherqui D, Belli G, Gamblin TC, et al. Laparoscopic major hepatectomy: an evolution in standard of care. Ann Surg. 2009;250:856–860. doi: 10.1097/SLA.0b013e3181bcaf46. [DOI] [PubMed] [Google Scholar]
- 24.Bretagnol F, Hatwell C, Farges O, Alves A, Belghiti J, Panis Y. Benefit of laparoscopy for rectal resection in patients operated simultaneously for synchronous liver metastases: preliminary experience. Surgery. 2008;144:436–441. doi: 10.1016/j.surg.2008.04.014. [DOI] [PubMed] [Google Scholar]
- 25.Geiger TM, Tebb ZD, Sato E, Miedema BW, Awad ZT. Laparoscopic resection of colon cancer and synchronous liver metastasis. J Laparoendosc Adv Surg Tech A. 2006;16:51–53. doi: 10.1089/lap.2006.16.51. [DOI] [PubMed] [Google Scholar]
- 26.Kim SH, Lim SB, Ha YH, Han SS, Park SJ, Choi HS, et al. Laparoscopic-assisted combined colon and liver resection for primary colorectal cancer with synchronous liver metastases: initial experience. World J Surg. 2008;32:2701–2706. doi: 10.1007/s00268-008-9761-z. [DOI] [PubMed] [Google Scholar]
- 27.Patriti A, Ceccarelli G, Bartoli A, Spaziani A, Lapalorcia LM, Casciola L. Laparoscopic and robot-assisted one-stage resection of colorectal cancer with synchronous liver metastases: a pilot study. J Hepatobiliary Pancreat Surg. 2009;16:450–457. doi: 10.1007/s00534-009-0073-y. [DOI] [PubMed] [Google Scholar]
- 28.Dagher I, Caillard C, Proske JM, Carloni A, Lainas P, Franco D. Laparoscopic right hepatectomy: original technique and results. J Am Coll Surg. 2008;206:756–760. doi: 10.1016/j.jamcollsurg.2007.09.012. [DOI] [PubMed] [Google Scholar]
- 29.Dagher I, Franco D. [Right hepatectomy by laparoscopic approach] J Chir (Paris) 2007;144:47–51. doi: 10.1016/s0021-7697(07)89456-7. [DOI] [PubMed] [Google Scholar]
- 30.Dagher I, Franco D. [Left hepatectomy: laparoscopic technique] J Chir (Paris) 2007;144:432–433. doi: 10.1016/s0021-7697(07)74001-2. [DOI] [PubMed] [Google Scholar]
- 31.Di Giuro G, Lainas P, Franco D, Dagher I. Laparoscopic left hepatectomy with prior vascular control. Surg Endosc. 2010;24:697–699. doi: 10.1007/s00464-009-0613-1. [DOI] [PubMed] [Google Scholar]
- 32.Miyazaki M, Kohda S, Itoh H, Kaiho T, Kimura F, Ambiru S, et al. Inhibition of hepatic regeneration after 70% partial hepatectomy by simultaneous resection of the bowel in rats. Eur Surg Res. 1995;27:396–405. doi: 10.1159/000129426. [DOI] [PubMed] [Google Scholar]
- 33.Kimura F, Miyazaki M, Suwa T, Kakizaki S, Itoh H, Kaiho T, et al. Reduced hepatic acute-phase response after simultaneous resection for gastrointestinal cancer with synchronous liver metastases. Br J Surg. 1996;83:1002–1006. doi: 10.1002/bjs.1800830738. [DOI] [PubMed] [Google Scholar]
- 34.Jaeck D, Bachellier P, Weber JC, Boudjema K, Mustun A, Paris F, et al. [Surgical strategy in the treatment of synchronous hepatic metastases of colorectal cancers. Analysis of a series of 59 operated on patients] Chirurgie. 1999;124:258–263. doi: 10.1016/s0001-4001(99)80091-9. [DOI] [PubMed] [Google Scholar]
- 35.Figueras J, Llado L, Ruiz D, Ramos E, Busquets J, Rafecas A, et al. Complete versus selective portal triad clamping for minor liver resections: a prospective randomized trial. Ann Surg. 2005;241:582–590. doi: 10.1097/01.sla.0000157168.26021.b8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Nguyen KT, Laurent A, Dagher I, Geller DA, Steel J, Thomas MT, et al. Minimally invasive liver resection for metastatic colorectal cancer: a multi-institutional, international report of safety, feasibility, and early outcomes. Ann Surg. 2009;250:842–848. doi: 10.1097/SLA.0b013e3181bc789c. [DOI] [PubMed] [Google Scholar]
- 37.Kazaryan AM, Pavlik Marangos I, Rosseland AR, Rosok BI, Mala T, Villanger O, et al. Laparoscopic liver resection for malignant and benign lesions: ten-year Norwegian single-center experience. Arch Surg. 2010;145:34–40. doi: 10.1001/archsurg.2009.229. [DOI] [PubMed] [Google Scholar]
- 38.Mala T, Edwin B, Gladhaug I, Fosse E, Soreide O, Bergan A, et al. A comparative study of the short-term outcome following open and laparoscopic liver resection of colorectal metastases. Surg Endosc. 2002;16:1059–1063. doi: 10.1007/s00464-001-9176-5. [DOI] [PubMed] [Google Scholar]
- 39.Castaing D, Vibert E, Ricca L, Azoulay D, Adam R, Gayet B. Oncologic results of laparoscopic versus open hepatectomy for colorectal liver metastases in two specialized centers. Ann Surg. 2009;250:849–855. doi: 10.1097/SLA.0b013e3181bcaf63. [DOI] [PubMed] [Google Scholar]
- 40.Topal B, Fieuws S, Aerts R, Vandeweyer H, Penninckx F. Laparoscopic versus open liver resection of hepatic neoplasms: comparative analysis of short-term results. Surg Endosc. 2008;22:2208–2213. doi: 10.1007/s00464-008-0023-9. [DOI] [PubMed] [Google Scholar]
- 41.Champagne BJ, Delaney CP. Laparoscopy for metastatic colorectal cancer. Surg Oncol. 2007;16:15–24. doi: 10.1016/j.suronc.2007.04.002. [DOI] [PubMed] [Google Scholar]