

Abstract
Background
Previous studies estimating the fraction of transmissions from persons with primary HIV have not focused on the effects of switching sex role in male homosexual populations. Such behavioral fluctuations can increase the contribution of primary HIV in the overall population.
Methods
We modeled HIV transmission with 8 compartments defined by 4 behavioral groups, with different anal-insertive and anal-receptive combinations, and 2 stages of infection. We explored the effects of fluctuating behavioral categories on endemic prevalence and the fraction of transmissions from primary HIV. We varied transition rates to develop the theory on how behavioral fluctuation affects infection patterns, and we used the transition rates in a Netherlands cohort to assess overall effects in a real setting.
Results
The dynamics of change in behavior-group status over time observed in the Netherlands cohort amplifies the prevalence of infection and the fraction of transmissions from primary HIV, resulting in the highest proportions of transmissions being from people with primary HIV. Fluctuation between dual- or receptive-role periods and no-anal-sex periods mainly determines this amplification. In terms of the total transmissions, the dual-role risk group is dominant. Fluctuation between insertive and receptive roles decreases the fraction of transmissions from primary HIV, but such fluctuation is infrequently observed.
Conclusion
The fraction of transmissions from primary HIV is considerably raised by fluctuations in insertive and receptive anal sex behaviors. This increase occurs even when primary HIV or later infection status does not influence risk behavior. Thus, it is not simply biology but also behavior patterns and social contexts that determine the fraction of transmissions from primary HIV. Moreover, each primary HIV transmission has a larger population effect than each later infection transmission because the men to whom one transmits from primary HIV carry on more chains of transmissions than the men to whom one transmits later in infection. Reducing transmissions from primary HIV should be a primary focus of HIV control efforts.
HIV transmission among men who have sex with men is an increasing problem in both relative and absolute terms.1 Neither public nor grassroots organizations have come up with sufficiently effective control strategies for this problem. In addition to condom use and testing for HIV status with counseling, new opportunities for control are emerging. However, as options increase for pre- and postexposure prophylaxis or early treatment to stop transmission, new challenges arise in finding control efforts that achieve a favorable balance between their potential risks and benefits. To face these challenges, we need better theory regarding the transmission dynamics that disseminate HIV through populations. It is particularly important to understand the role of transmission from primary HIV infection—the brief period after infection before the strong immune response characterized by high viral titer. This is a critical period because early treatment options are less likely to reduce primary HIV transmissions than postprimary HIV transmissions. Also, we need to decide which populations and which individuals to target for pre-exposure prophylaxis programs.
We build here, on a recent theoretical advance and an older observational study of risk behavior, dynamics to construct a theory for HIV transmission in populations of men who have sex with men. The theoretical advance elucidates the differences in transmission dynamics between homosexual and heterosexual populations that generate considerably more transmissions in homosexual populations even though the contact rates and transmission probabilities in the 2 groups may be the same.2 Considering that men who have sex with men are able to reciprocate insertive and receptive sexual practices, it takes far fewer new sexual partnerships to sustain HIV transmission.
The observational data on the dynamic fluctuations between insertive and receptive behaviors in men who have sex with men came from one of the early cohort studies. This analysis of a Netherlands cohort by Blower et al3 demonstrates that anal sex fluctuates across 6-month observation periods in a manner that jointly affects the dynamics underlying both of the theoretical advances outlined earlier. The observed changes in sexual behavior over time appeared to be approximately independent of past sexual roles.
Risk-behavior fluctuation is influenced by partnership dynamics as well as by psychologic, social, and economic factors in both homosexual and heterosexual populations. In periods of high risk, a person is likely to encounter sexual partners who also accept higher risk behaviors. One is, therefore, more likely to become infected and to spread infection during these periods of high risk (and the persons to whom one transmits are in turn more likely to carry on chains of transmission) compared with periods of lower risk behavior.4 Additionally, as high-risk populations turn over, the population of susceptible individuals needed to sustain high levels of transmission is replenished. These phenomena enhance the role of transmissions from primary HIV in sustaining chains of transmission.
We combine the observed behavior dynamics in the Netherlands cohort data with a staged HIV infection and transmission model. This allows us to analyze the effects of the behavior dynamics on the role of primary HIV transmissions. The observed behavior dynamics are consistent with a considerable amplification of the role of primary HIV transmissions during the endemic equilibrium phase of an epidemic. Fluctuations between abstinence and sexual activity account for these effects. We also demonstrate that switching between insertive and receptive behaviors lowers the fraction of transmissions coming from primary HIV transmissions. In the population observed by Blower et al,3 however, such fluctuations were rare, and this effect is overwhelmed by the effects of behavioral fluctuation in and out of the group having anal sex.
We have shown that the rates of role fluctuation reported by Blower et al3 result in a considerable increase in both prevalence and the fraction of transmissions from primary HIV, in contrast to what would be expected in the absence of sex-role fluctuation. We identify countervailing effects of fluctuation that generate this result. Our analysis indicates that it would be unusual to find population compositions and role-fluctuation rates that lower the fraction of transmissions from primary HIV among men who have sex with men. Fluctuation would have to mainly involve a reversal of exclusive roles, which rarely happened in the population studied by Blower et al.3 Thus, role fluctuation in the real world will typically raise the fraction of transmissions from primary HIV.
METHODS
We develop a deterministic compartmental model to analyze the effect of directional sex behavior for different risk groups in a population of men who have sex with men. We integrate risk-behavior dynamics into a model of staged HIV infection and transmission to analyze the effects of those risk dynamics on primary HIV transmissions. We use data on insertive and receptive behavior changes reported by Blower et al.3 In this section, we give an overview of the deterministic compartmental model. A fuller specification of the model and its assumptions are presented in eAppendix 1 (http://links.lww.com/EDE/A412).
The model incorporates 4 behavior groups as identified by Blower et al3: dual-role or reciprocal sex (ie, both insertive and receptive), receptive-only, insertive-only, and no anal sex (“abstinence”). Partnerships refer to either unidirectional or reciprocal anal sex acts. In this paper, we do not model oral sex or other modes of transmission. Our model classifies men as exclusively insertive, exclusively receptive, or dual role. Rather than modeling the causal process of partnering, we model directional contact rates in a phenomenologic manner by having the receptive contact rates drive the insertive partnering rates. For encounters between 2 men in the dual-role risk group, we model both unidirectional and reciprocal anal-sex acts.
The natural history of HIV infection is modeled with 2 stages of infection: primary HIV infection and postprimary HIV infection. We see little possibility that our inferences would change if we divided the second stage of infection further to account for increasing transmissibility very late during infection. Moreover, treatment now largely eliminates the late transmissibility peak. For primary HIV, we assume a short period (5 weeks) of high transmissibility, followed by the long postprimary HIV period (12 years) during which transmissibility is low. Transmission probabilities by stage of infection are estimated from the data used by Wawer et al.5 In eAppendix 2 (http://links.lww.com/EDE/A412), we describe the method used for this analysis. The risk of transmission is higher for the receptive anal-sex partner than the insertive anal-sex partner. For reciprocal sex, we assume that the transmission risk is the sum of the risks for insertive and receptive sex. Transmission risks are presented in eAppendix 2. We assume that, on average, men are sexually active for 40 years. Transmission risks are per partnership; however, due to the nature of deterministic compartmental models, risk is modeled as a single point in time. We handle this by using continuous time rates that give the observed 6-month transition probabilities from Blower et al,3 as shown in Figure 1. Additionally, we have developed an individual-based version of the deterministic compartmental model to understand the effects of relaxing assumptions regarding the natural history of infection. The individual-based version is described in eAppendix 3 (http://links.lww.com/EDE/A412).
FIGURE 1.
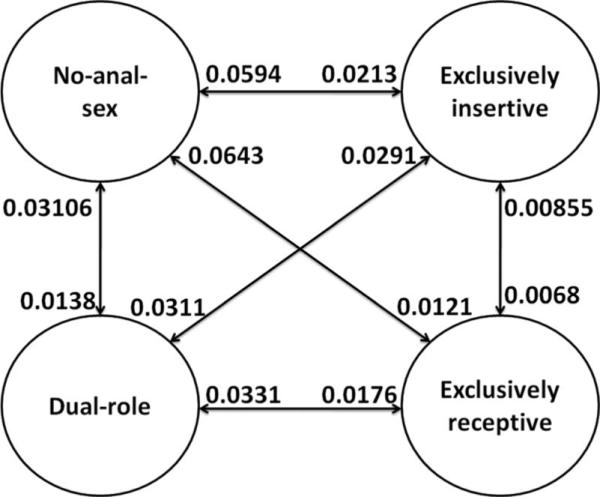
Instantaneous transition rates per month for the 4 risk groups used in the deterministic compartmental model that is adapted from Blower et al.3
RESULTS
Dynamic Analysis Given Observed Risk Behavior Flows
In a steady state without infection transmission, the Blower et al3 data suggest that 51% of the population is having no anal sex, 10% is exclusively receptive, 18% is exclusively insertive, and 21% is both. The average time spent in these 4 behavior groups is 20 months, 9 months, 10 months, and 12 months, respectively. The analysis by Blower et al,3 however, does not give information on the partnership rates in the 4 risk groups for anal sex. Moreover, they provide no data on the extent of mixing between purely unidirectional and dual-role men, or the fraction of dual-role encounters that are reciprocal, ie, when both partners assume each role. In this section, we examine outcomes across a range of parameters that are consistent with the Blower et al data.3
In the model, we set the parameters for receptive contact rates for the receptive-only and dual-role groups. Receptive sex acts are distributed according to the parameters that determine how many of the insertive partners will come from the dual-role group and how many from the insertive-only risk group. Within the partnerships where both the insertive and receptive partners are dual-role men, we set a model parameter that determines what fraction of the dual-role men will assume reciprocal sex roles, ie, when a single encounter will involve 2 acts with reversed sex roles. For our first analysis, we assume this fraction to be one-half; ie, half of all partnerships in which both partners are from the dual-role group are reciprocal.
Figure 2A shows the prevalence and fraction of transmissions from primary HIV over a period of 60 years. We can see a quick rise of the epidemic that peaks after 20 years and finally reaches an endemic equilibrium level of 42% prevalence. The fraction of transmissions from primary HIV rises quickly to a high value and eventually reaches equilibrium at 52%. The reasons for the quick rise to a high level in the fraction of transmission from primary HIV during the early stage of the epidemic are well understood.6 It is the latter value at equilibrium on which we concentrate in this paper. We can compare the 52% from primary HIV to the 42% transmission potential,7 which can be calculated by taking the duration of each stage of infection × its transmission probability. This 42% level is observed if we set the entire population to be dual-role men all the time, or if we set the entire population to be either exclusively insertive or receptive with no change of sex role.
FIGURE 2.

Dynamic analysis given observed risk behavior flows from Blower et al3 when half of the dual-role individuals are responsible for the reciprocal sex acts. A, HIV Prevalence and fraction of transmissions from primary HIV in the overall population. B, HIV Prevalence with respect to the no-anal-sex, insertive-only, receptive-only and dual-role risk groups. C, Fraction of total transmissions from the insertive-only, receptive-only and dual-role risk groups. D, Fraction of transmission from primary HIV from the insertive-only, receptive-only and dual-role risk groups.
In Figure 2B, we see that in the early stages of the epidemic, transmission is high in the dual-role group and eventually disseminates to other risk groups. In our model, dissemination to the no-anal-sex group is strictly due to change in risk behaviors, ie, when infected men choose to abstain from sex. The impact of dual-role men is further illustrated in Figure 2C, which presents the fraction of all transmissions from the various behavior groups. The fraction for the dual-role group dominates over the insertive-only and receptive-only groups. At equilibrium, 75% of all transmissions arise from the dual-role men. Only 3% of infections arise from the receptive-only men and 22% arise from the insertive-only men. At equilibrium, 90% of all transmissions and 91% of the dual-role transmissions are from insertive to receptive partners.
The rapid rise seen in Figure 2C is due to the fact that dual-role men can assume both unidirectional and reciprocal sex roles. This results in a high risk of new infection as well as a high risk of transmission during the primary HIV period, thus sustaining more chains of transmission from primary HIV. In Figure 2D, we see the fraction of transmissions from each group from primary HIV. The dual-role and receptive-only men have high fractions of their transmissions from primary HIV. The receptive-only men transmit rarely, however, so that they account for only 4% of primary HIV transmissions. In contrast, the dual-role group accounts for 87%. The insertive-only men are at a low risk of getting infected during their exclusively-insertive behavior phase. That is, most of the infected men in this phase were infected while in either a dual-role or receptive-only phase. When they moved into this phase they were already beyond their primary HIV stage of infection.
The low rate of primary HIV transmissions from insertive-only men generates a countervailing force to risk-behavior fluctuation effects. At these settings, risk fluctuation causes a higher fraction of transmissions from primary HIV (52%) than would be expected given homogeneous behaviors (42%). It also amplifies the effect on the endemic prevalence by a separate mechanism that goes beyond the fraction of transmissions from primary HIV. Men infected by a source case with primary HIV will transmit to others about 1.2 times as frequently as a man whose source case was in the postprimary HIV stage of infection (calculated from an average of 10 simulation runs from the individual-based version of the model). Thus, preventing one primary HIV transmission has a greater population effect than preventing one postprimary HIV transmission.
Equilibrium Analysis Given Observed Behavior Flows
We now examine the endemic prevalence in the population by exploring a fuller range of parameters that could be consistent with the Blower et al data.3 In our conformation of who mixes with whom, a certain fraction of the receptive acts of dual-role men are reserved for other dual-role men who play the insertive role. The remaining sex acts of the dual-role men are distributed randomly between those who are dual-role and those who are exclusively insertive. We examine settings where none, half, or all of the receptive acts by dual-role men are reserved for other dual-role men. In Figure 3A, we see that concentrating dual-role sex acts with other dual-role men considerably drops the transmission threshold and raises the prevalence. In Figure 3B, we see that this also raises the fraction of transmissions from primary HIV. As we can observe, concentrating sex acts of dual-role men with other dual-role men amplifies transmission, especially from primary HIV. This is because the men to whom transmission occurs are more likely to carry on transmission.
FIGURE 3.

Equilibrium analysis given observed risk behavior flows from Blower et al.3 Panels (A and B) give the prevalence and fraction of transmission from primary HIV respectively for the average receptive contact rate per month for unidirectional sex for dual role contacts that are 0%, 50% and 100% reciprocal. Panels (C and D) gives the prevalence and fraction of transmission from primary HIV respectively for the average receptive contact rate per month for unidirectional sex for 80%, 67%, and 51% as the initial proportion of the population in the no anal sex group.
Another factor affecting the overall prevalence and the number of secondary infections from PHI is the fraction of the population that is in the no-anal-sex group. The way the cohort was enrolled in the Netherlands study,3 men who were in a low-risk mode and had a lower chance of engaging in high-risk sex were likely to be undersampled. To assess the effect of this undersampling on our inferences, we keep the transition rates into and out of the 3 active sex groups the same, but cut the rates out of the no-anal-sex group to one-half or one-quarter. Figure 3C shows the prevalence and Figure 3D shows the fractions of transmission from primary HIV for 3 situations in which the average receptive contact rate was varied. The 3 cases in Figure 3C and D correspond to one-quarter, one-half, and the original value of the transition rates out of the no-anal-sex group. The fraction of the dual-role men having reciprocal sex was set at 0.5. This results in the initial fraction of the population in the no-anal-sex group to be 80%, 67%, and 51% for the 3 cases, respectively. We see that a high initial population of the no-anal-sex group has an effect on lowering the threshold and raising the fraction of transmissions from primary HIV.
Due to higher turnover in the no-anal-sex group, a newly infected man who becomes inactive is more likely to go back to being active and contribute to the basic reproductive ratio (R0). For higher initial populations of the no-anal-sex group (ie, 80% and 67% of the total population), we find an increase in the fraction of transmissions from primary HIV to 63% and 69%, respectively. This is in contrast to the 56% contribution from primary HIV when the initial fraction of the no-anal-sex group is 51%. The reason is that a greater inflow of susceptible men who become sexually active causes more sustained chains of primary HIV transmission in the high-risk dual-role sex groups. By contrast, the prevalence is lowered because the denominator includes more sexually-inactive men.
From the aforementioned analysis for the observed behavior-change patterns reported by Blower et al,3 we find that the expected fraction of transmissions from primary HIV is considerably above what would have been expected under random homogenous mixing. This suggests that the fraction of transmissions from primary HIV is not merely a function of the transmissibility of infection during different stages of infection; it also depends on the risk-behavior dynamics. An important effect is the switching behavior from being dual-role to having no anal sex, which makes a large contribution to increasing the transmission potential from primary HIV and sustaining HIV transmission in the system.
Equilibrium Analysis Under Theoretical Conditions to Clarify Causes in Dynamics
In the full set of flows documented by Blower et al,3 there are many dynamic events happening at once. For instance, a shift from high-fluctuation to no-fluctuation between the risk groups increases the proportion of secondary cases generated from primary HIV. By contrast, fluctuation between insertive and receptive risk behavior decreases the proportion of transmissions from primary HIV. To help clarify our inferences about these dynamic effects, we now pursue theoretical analyses.
First, we consider a situation in which there is no one in the no-anal-sex group. This eliminates a major source of risk fluctuation, although switching from a dual-role to a unidirectional role still generates risk fluctuation. We vary the size of the dual-role risk group from zero to the sum of both the insertive-only and receptive-only risk groups. We then run the model until the size of the dual-role risk group reaches 50%, at which point the fraction of transmissions from primary HIV reaches equilibrium. The average time spent in the 3 groups is set to 12 months with equal transition rates.
In Figure 4A, we observe that when the entire population is either in the insertive-only or the receptive-only group, the fraction of transmissions from primary HIV is considerably below its potential of 42%. In contrast, as the size of the dual-role population increases, this fraction rises as well. At the extreme left (ie, without the dual-role population), we find the fraction of primary HIV transmissions to be considerably low. This is because the receptive-only men, who are more likely to become infected, transmit more readily when they switch to the insertive-only sex role. However, the low levels of transmissions are due to the fact that the infected men who are receptive-only are likely to have passed through the primary infection stage by the time they switch their sex role. On the contrary, the fraction of transmissions from primary HIV increases as the proportion of the population in the dual-role risk group is increased. It reaches just below the transmission potential when half of the population is in the dual-role risk group. This eventual rise is due to the fluctuations between the insertive behavior (and to a lesser extent receptive behavior) and the dual-role behavior.
FIGURE 4.

Equilibrium analysis under theoretical conditions to clarify causes in dynamics. Panel (A) shows the prevalence and fraction of transmission from primary HIV, varied over the dual-role population from zero to the sum of the insertive-only and receptive-only populations. Panel (B) shows the prevalence and fraction of transmission from primary HIV without persons having no anal sex for the dual-role population varied over the fluctuation rate between the insertive-only and receptive-only groups.
To examine what happens at the extreme left in Figure 4A, we consider a situation with just the insertive-only and receptive-only groups. We vary the rate of fluctuation between the 2 risk groups, as shown in Figure 4B. At the left side of Figure 4B, when there is no fluctuation, we find that the infection level is lowest and the fraction of transmissions from primary HIV is precisely at its calculated baseline-transmission potential. As fluctuation increases, the fraction of transmissions decreases for the reasons discussed earlier with regard to the setting in Figure 4A. With an ever-increasing fluctuation, however, the fraction of primary HIV transmissions rises again. When switching is extremely fast (such that the population is essentially a dual-role population), it once again reaches its baseline transmission potential.
In eAppendix 1 (http://links.lww.com/EDE/A412), we look into the fluctuation between the dual-role and no-anal-sex risk groups only. We find that the fraction of transmission from primary HIV is highest when the time spent in the dual-role group is closer to the duration of primary HIV. It remains above the baseline transmission potential except in the extreme cases of fast and no switching, where it is equal to the baseline 42%. Furthermore, we investigate the effect of fluctuation of insertive and receptive sex roles in the absence of the dual-role and no-anal-sex groups for the observed and the theoretical settings. For the risk group transitions based on the study by Blower et al,3 the fraction of transmissions from primary HIV remained considerably high throughout. For the theoretical setting, increasing fluctuation between the insertive-only and receptive-only risk groups increases the prevalence even when the transmission fraction is low.
The aforementioned theoretical analysis shows that switching between exclusively unidirectional sex roles (insertive or receptive) decreases the transmissions from the primary HIV stage of high transmissibility. In contrast, switching between the dual-role and no anal sex increases the fraction of transmissions from primary HIV. Transitions from unidirectional to reciprocal sex also had this increasing effect. Overall, in the presence of all risk groups and with equal transitions rates, this fraction is slightly below the baseline 42%.
DISCUSSION
We examined how changes in sex roles in a population of men who have sex with men determine HIV prevalence, and the role of primary HIV infection stage in sustaining transmission. We focused on the effects of varying temporal patterns of insertive and receptive anal sex. Under the observed sex behavior patterns reported by Blower et al,3 the expected fraction of transmissions from primary HIV is considerably above what would be expected under random mixing given fixed behavioral status. In theoretical models, we observed that transitions back and forth between exclusively-insertive and exclusively-receptive sex roles can decrease the fraction of transmissions from primary HIV. Transitions back and forth from abstinence (or no anal sex) to the versatile dual role greatly increase the transmissions from PHI. Transitions from unidirectional to reciprocal sex also have an increasing effect. The net effect of the fluctuations observed by Blower et al3 is a balance of these positive and negative effects. More broadly, the fraction of transmissions from primary HIV is not just a function of transmissibility by stage, but of risk-behavior transition patterns as well.
Our results have important implications for how HIV control should be pursued. HIV counseling and testing alone has not had a big effect on reducing HIV transmission in gay male populations because it does not reduce transmissions from primary HIV.8–10 To integrate multiple prevention modalities into an effective and coherent prevention program, it is therefore important to determine the fraction of transmissions generated from primary HIV and to understand the role of such transmission in sustaining population infection levels. Previous modeling studies that have estimated the fraction of transmissions from primary HIV did not take into account the fluctuation of sex role among men who have sex with men.11–15 Our results indicate that these studies have underestimated the role of primary HIV. Our results suggest that populations sustaining primary HIV transmissions chains will be important targets for treatments such as pre-exposure prophylaxis. Whether men with or without currently infected partners or partners of unknown HIV status should be targeted is also likely to be influenced by primary HIV transmission risks.
Our model has ignored some important determinants of HIV transmission dynamics that should be included in subsequent studies. These include risk from oral sex.16 It is possible that dissemination of infection during oral sex in the no-anal-sex group could amplify the effects we have presented here. Likewise, periods of high and low sex-act rates within any of the 4 behavioral categories in our model are likely to further amplify the effects of primary HIV transmission. In contrast, some aspects of reality could lower the fraction of primary HIV transmissions. A recent study has shown that incorporating contact duration and concurrency in a homosexual population greatly affects the prevalence and the fractions from primary HIV.17 We suspect that integrating these factors will result in attributing even greater importance to primary HIV.
Our paper adds to the discussion of sex-role dynamics among men having sex with men as one of the key determinants that affect the fractions of transmissions from primary HIV infection at the population level. We have shown that theory-based models can help in understanding the dynamics in observed data. Nevertheless, the ability of our analysis to explain and predict the observed levels of infection and to estimate key parameters is limited by the scope of the available data and how those data are incorporated in our models. To explain the dynamics of risk associated with HIV among the population of men who have sex with men, we need to build a theory explaining the changes in the environment that may affect sexual behavior, as well as to accommodate data sources such as detailed ethnographic observations, carefully sampled prospective cohorts, and cross-sectional studies.
Supplementary Material
Acknowledgments
Supported by a subcontract to the University of Michigan from NIH grant R01 DA 03574 (to S.J.A., J.S.K., E.O.R.S., J.H.K., G.E.); supported by fellowships from the University of Michigan Rackham Graduate School (to J. Kim); by NIH T32 AI049816 (to E.O.R.S.); by NIH grant R01AI078752 (to J.S.K., E.O.R.S., J.H.K., G.E.).
Footnotes
Supplemental digital content is available through direct URL citations in the HTML and PDF versions of this article (www.epidem.com).
REFERENCES
- 1.Jaffe HW, Valdiserri RO, De Cock KM. The reemerging HIV/AIDS epidemic in men who have sex with men. JAMA. 2007;298:2412–2414. doi: 10.1001/jama.298.20.2412. [DOI] [PubMed] [Google Scholar]
- 2.Goodreau SM, Golden MR. Biological and demographic causes of high HIV and STD prevalence in men who have sex with men. Sex Transm Infect. 2007;83:458–462. doi: 10.1136/sti.2007.025627. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Blower SM, Vangriensven GJ, Kaplan EH. An analysis of the process of human immunodeficiency virus sexual risk behavior change. Epidemiology. 1995;6:238–242. doi: 10.1097/00001648-199505000-00008. [DOI] [PubMed] [Google Scholar]
- 4.Abu-Raddad LJ, Longini IM., Jr No HIV stage is dominant in driving the HIV epidemic in Sub-Saharan Africa. AIDS. 2008;22:1055. doi: 10.1097/QAD.0b013e3282f8af84. [DOI] [PubMed] [Google Scholar]
- 5.Wawer MJ, Gray RH, Sewankambo NK, et al. Rates of HIV-1 transmission per coital act, by stage of HIV-1 infection, in Rakai, Uganda. J Infect Dis. 2005;191:1403–1409. doi: 10.1086/429411. [DOI] [PubMed] [Google Scholar]
- 6.Jacquez JA, Koopman JS, Simon CP, Longini IM., Jr Role of the primary infection in epidemics of HIV infection in gay cohorts. J Acquir Immune Defic Syndr. 1994;7:1169. [PubMed] [Google Scholar]
- 7.Fraser C, Hollingsworth TD, Chapman R, de Wolf F, Hanage WP. Variation in HIV-1 set-point viral load: Epidemiological analysis and an evolutionary hypothesis. Proc Natl Acad Sci USA. 2007;104:17441–17446. doi: 10.1073/pnas.0708559104. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Higgins DL, Galavotti C, O'Reilly KR, et al. Evidence for the effects of HIV antibody counseling and testing on risk behaviors. JAMA. 1991;266:2419–2429. [PubMed] [Google Scholar]
- 9.Matovu JK, Gray RH, Makumbi F, Wawer MJ, Serwadda D, Kigozi G. Voluntary HIV counseling and testing acceptance, sexual risk behavior and HIV incidence in Rakai, Uganda. AIDS. 2005;19:503–511. doi: 10.1097/01.aids.0000162339.43310.33. [DOI] [PubMed] [Google Scholar]
- 10.Weinhardt LS, Carey MP, Johnson BT, Bickham NL. Effects of HIV counseling and testing on sexual risk behavior: a meta-analytic review of published research, 1985–1997. Am J Public Health. 1999;89:1397–1405. doi: 10.2105/ajph.89.9.1397. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Hollingsworth TD, Anderson RM, Fraser C. HIV-1 transmission, by stage of infection. J Infect Dis. 2008;198:687–693. doi: 10.1086/590501. [DOI] [PubMed] [Google Scholar]
- 12.Gelgor L, Kaldor J. Epidemiology of primary HIV-1 infection. Curr Opin HIV AIDS. 3:4–9. doi: 10.1097/COH.0b013e3282f310c5. [DOI] [PubMed] [Google Scholar]
- 13.Pilcher CD, Tien HC, Eron JJ, Jr, et al. Brief but efficient: acute HIV infection and the sexual transmission of HIV. J Infect Dis. 2004;189:1785–1792. doi: 10.1086/386333. [DOI] [PubMed] [Google Scholar]
- 14.Pinkerton SD. How many sexually-acquired HIV infections in the USA are due to acute-phase HIV transmission. AIDS. 2007;21:1625–1629. doi: 10.1097/QAD.0b013e32826fb6a6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Rapatski BL, Suppe F, Yorke JA. HIV epidemics driven by late disease stage transmission. J Acquir Immune Defic Syndr. 2005;38:241–253. [PubMed] [Google Scholar]
- 16.Vittinghoff E, Douglas J, Judon F, McKiman D, MacQueen K, Buchinder SP. Per-contact risk of human immunodeficiency virus transmission between male sexual partners. Am J Epidemiol. 1999;150:306–311. doi: 10.1093/oxfordjournals.aje.a010003. [DOI] [PubMed] [Google Scholar]
- 17.Kim JH. Dynamic Partnerships and HIV Transmissions by Stage [PhD Dissertation] University of Michigan; Ann Arbor, MI: 2009. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.