

Abstract
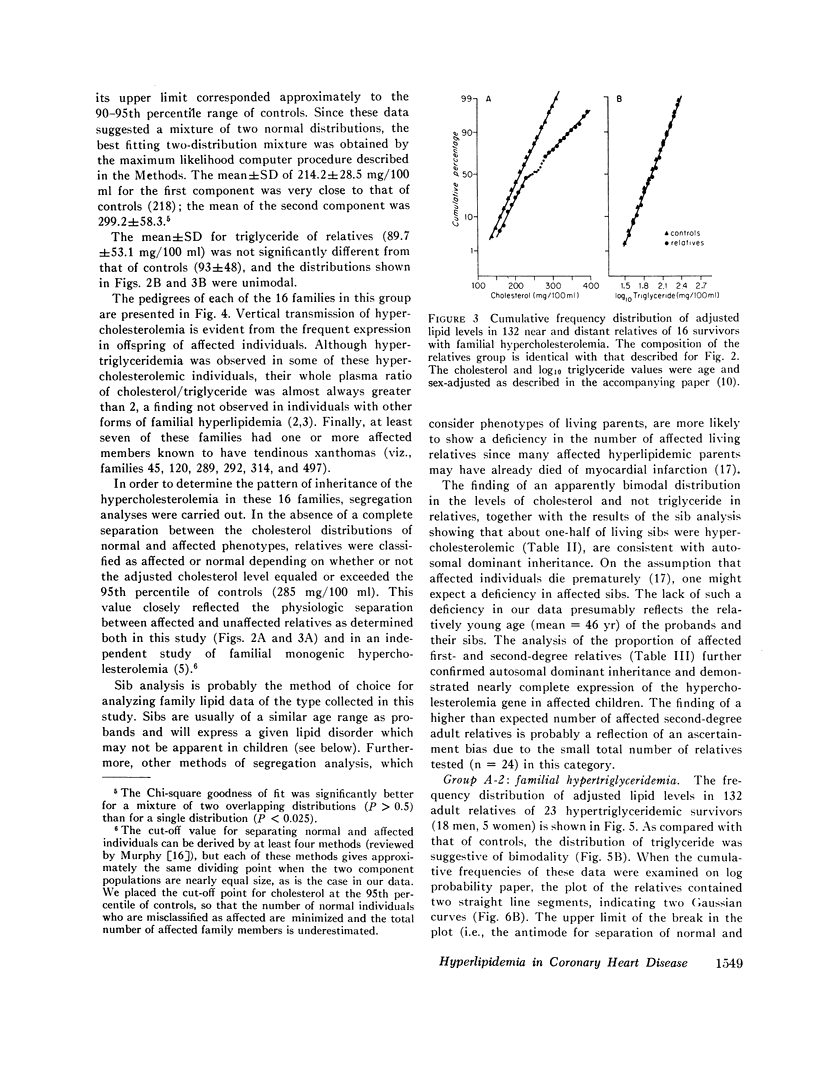
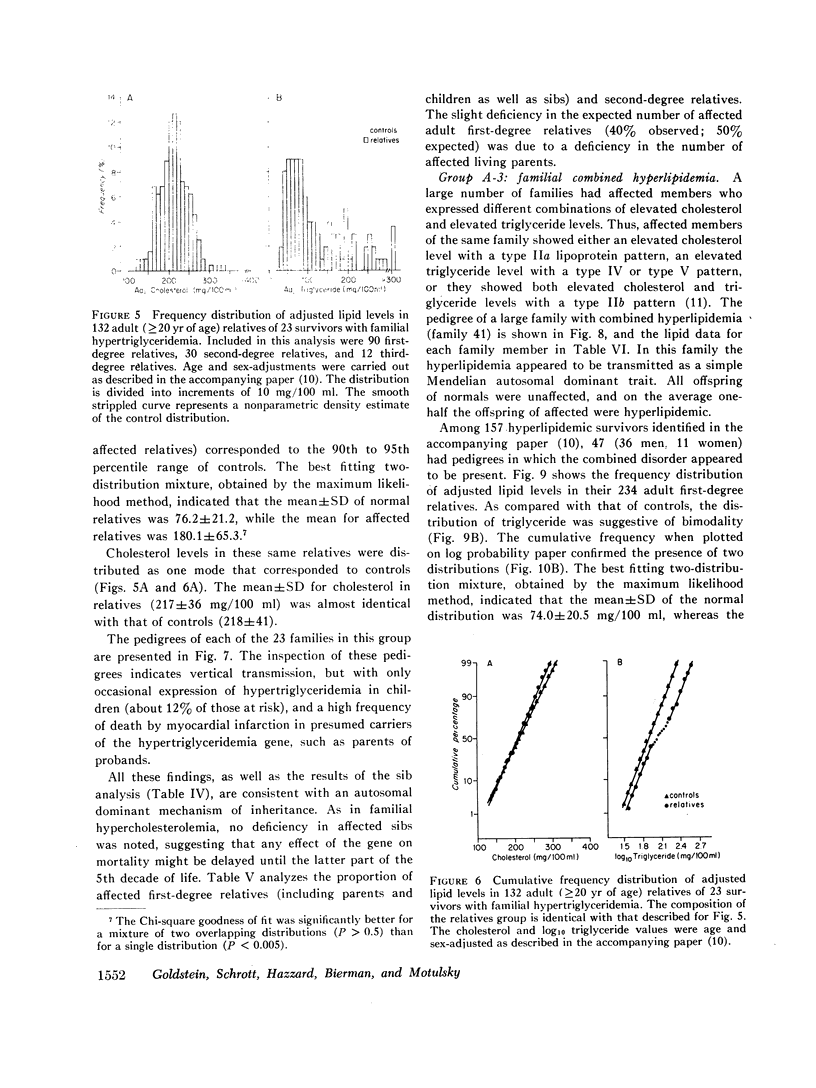
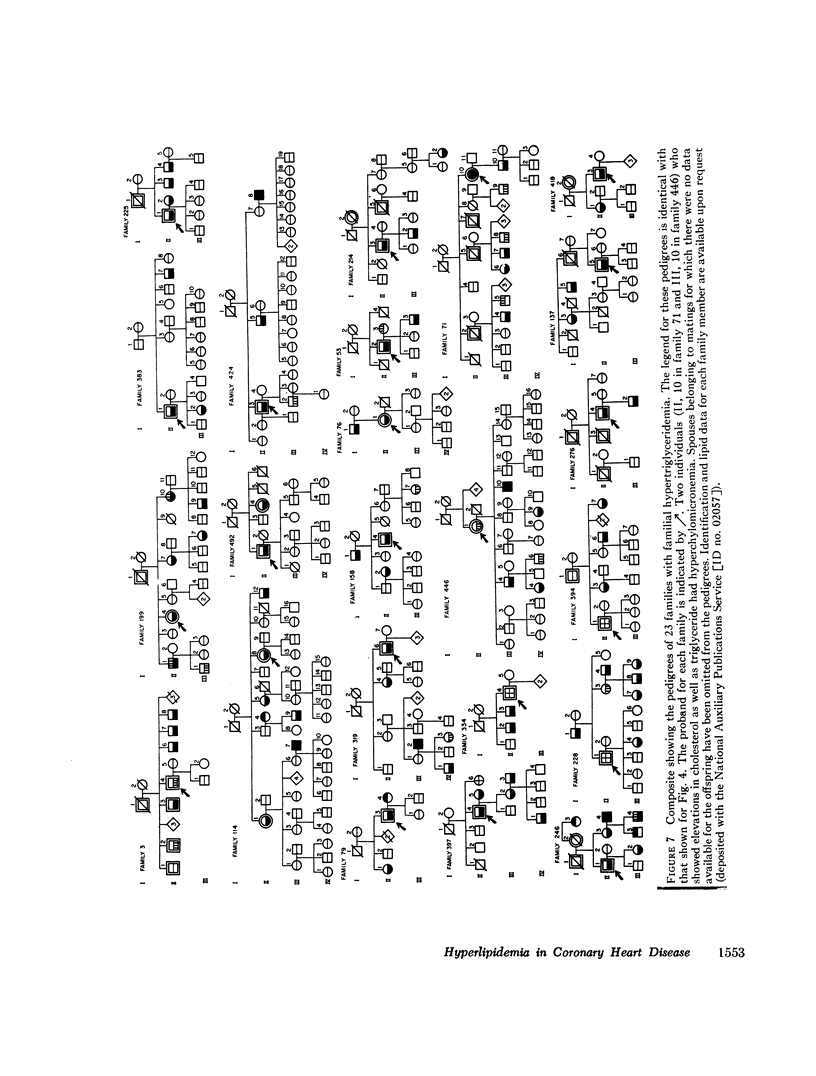
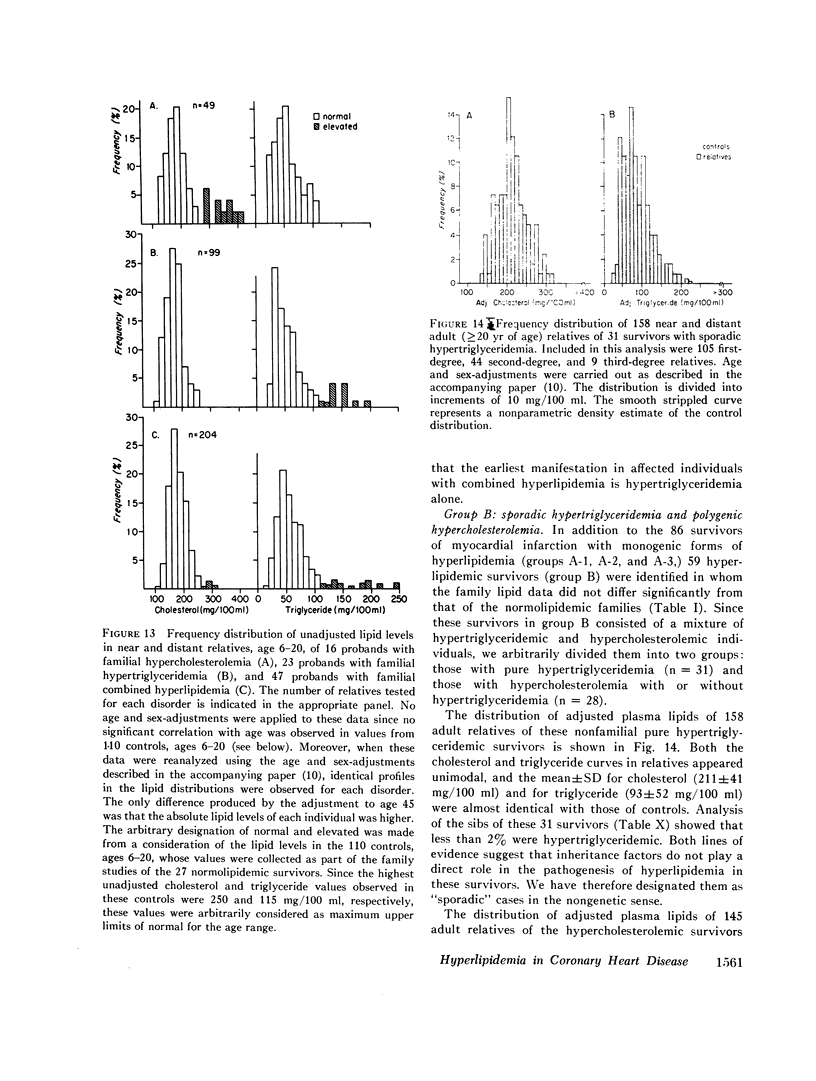
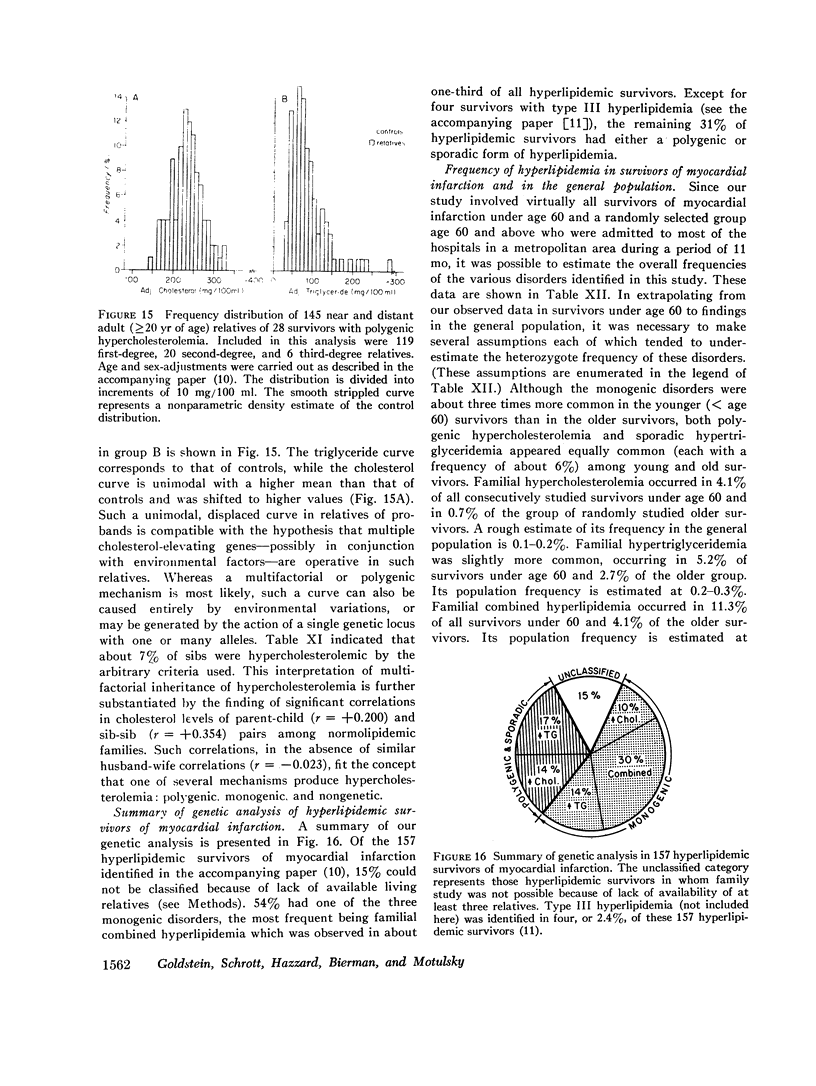
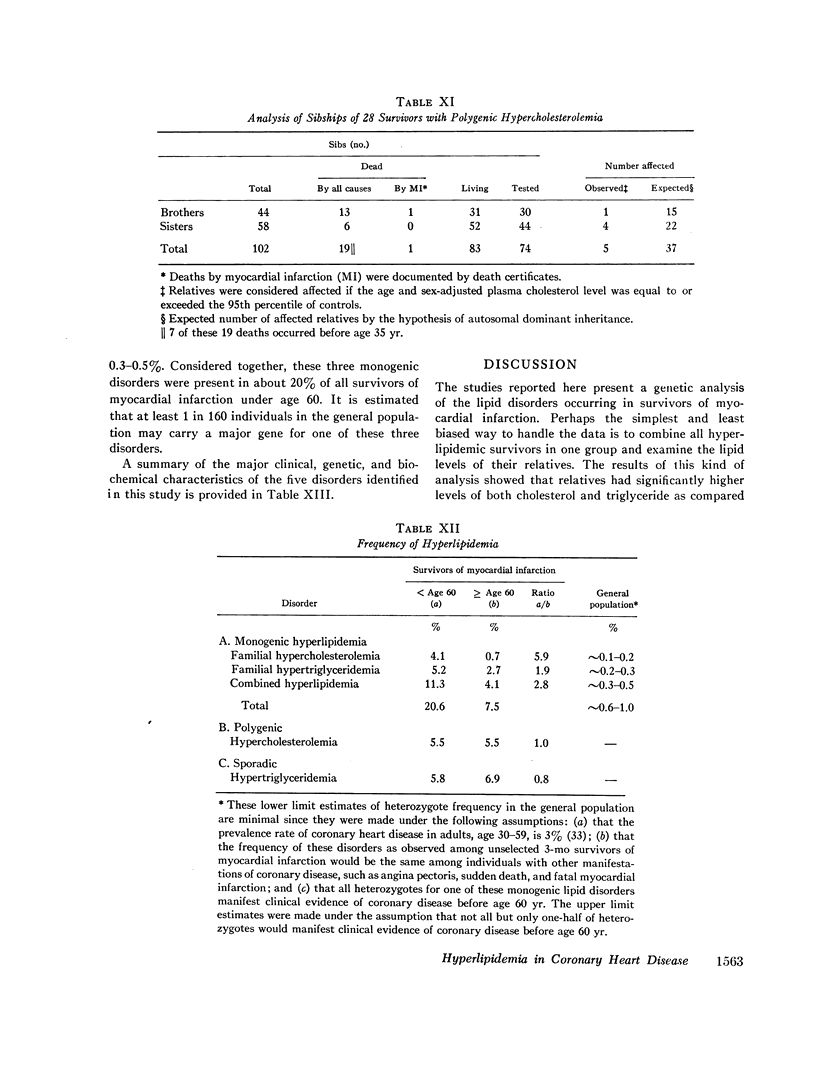
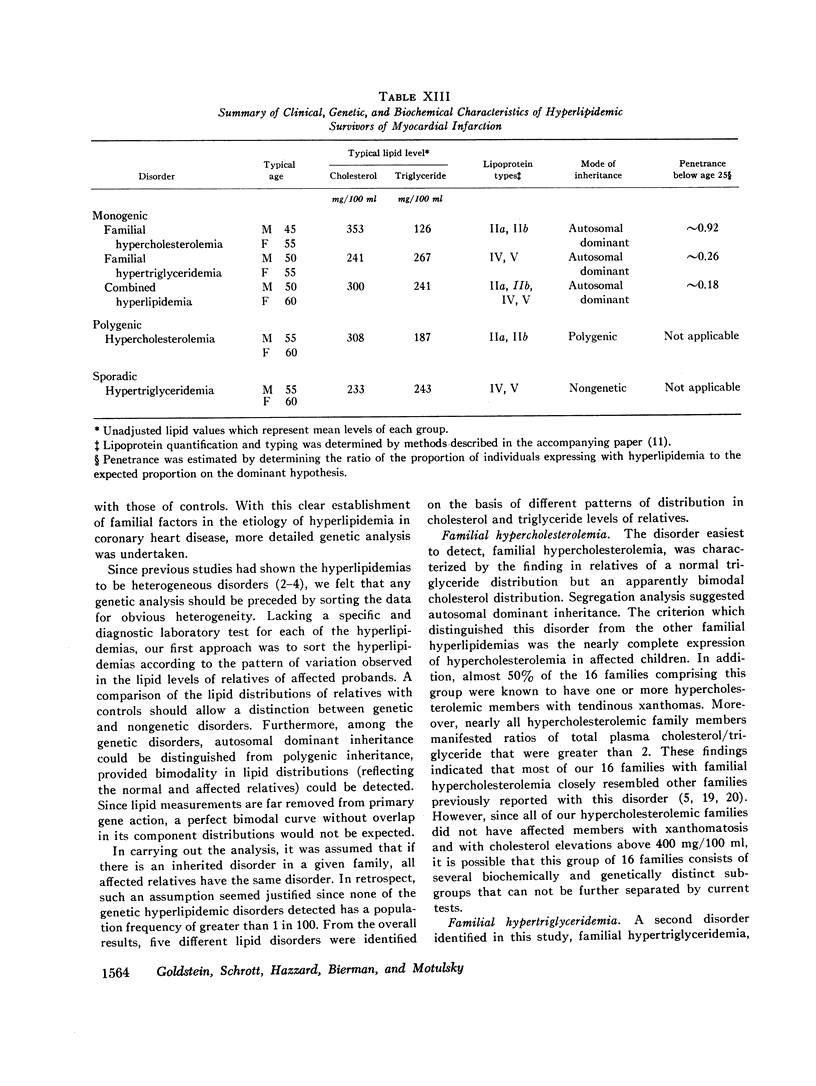
To assess the genetics of hyperlipidemia in coronary heart disease, family studies were carried out in 2520 relatives and spouses of 176 survivors of myocardial infarction, including 149 hyperlipidemic and 27 normolipidemic individuals. The distribution of fasting plasma cholesterol and triglyceride values in relatives, together with segregation analyses, suggested the presence of five distinct lipid disorders. Three of these—familial hypercholesterolemia, familial hypertriglyceridemia, and familial combined hyperlipidemia—appeared to represent dominant expression of three different autosomal genes, occurring in about 20% of survivors below 60 yr of age and 7% of all older survivors. Two other disorders—polygenic hypercholesterolemia and sporadic hypertriglyceridemia—each affected about 6% of survivors in both age groups.
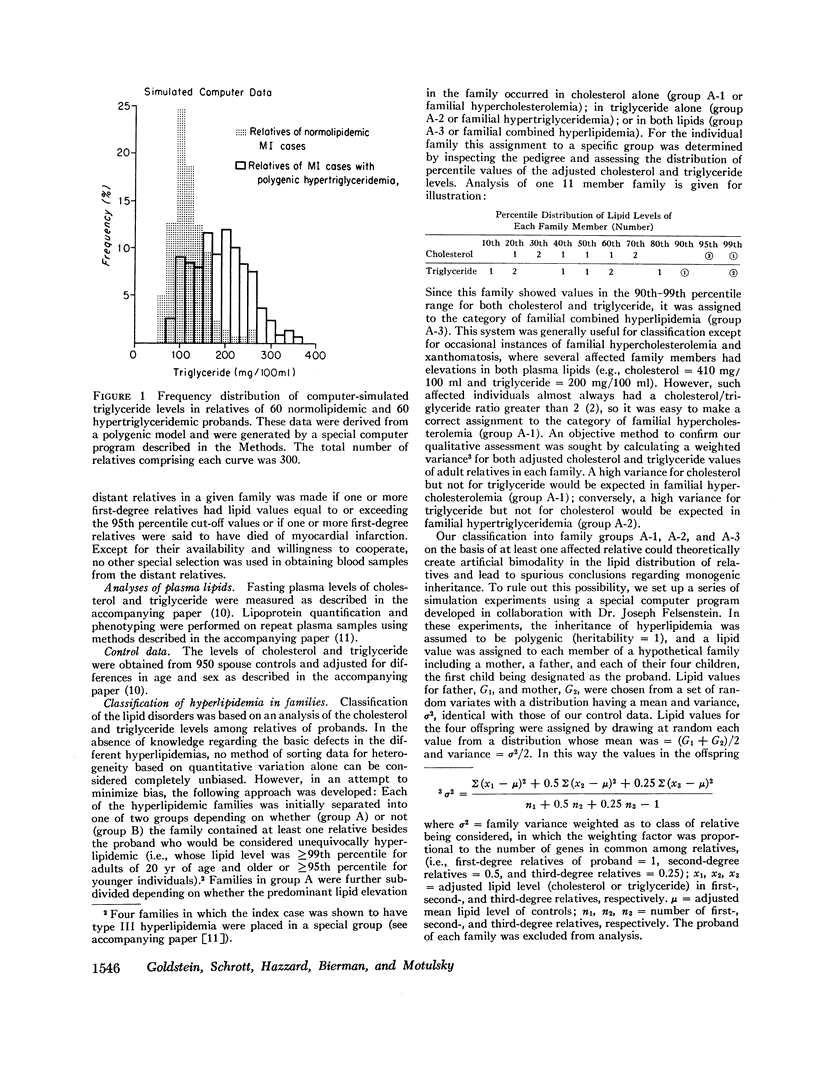
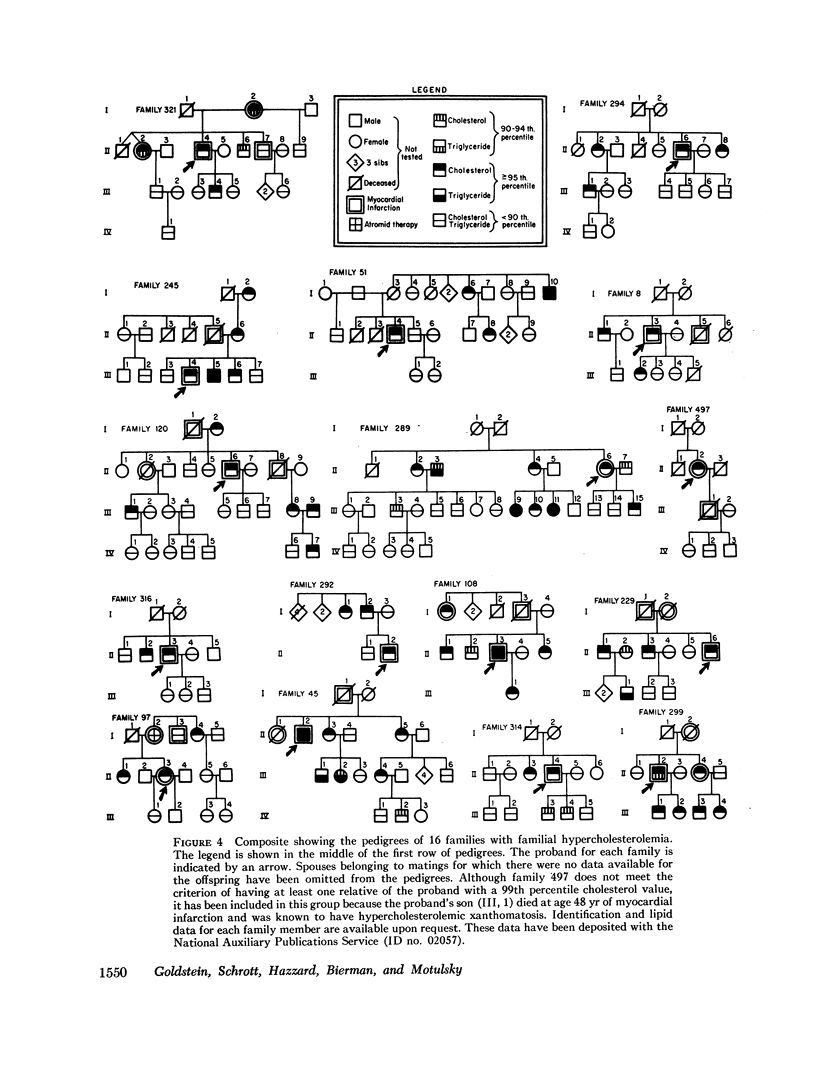
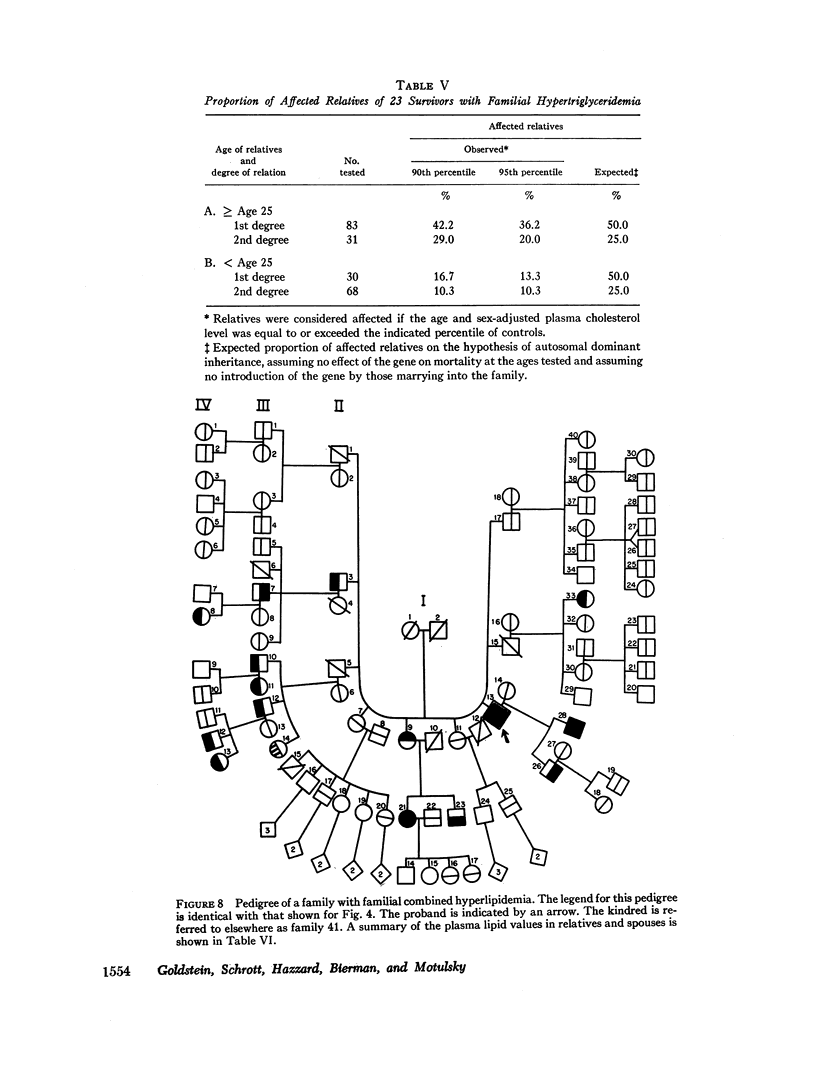
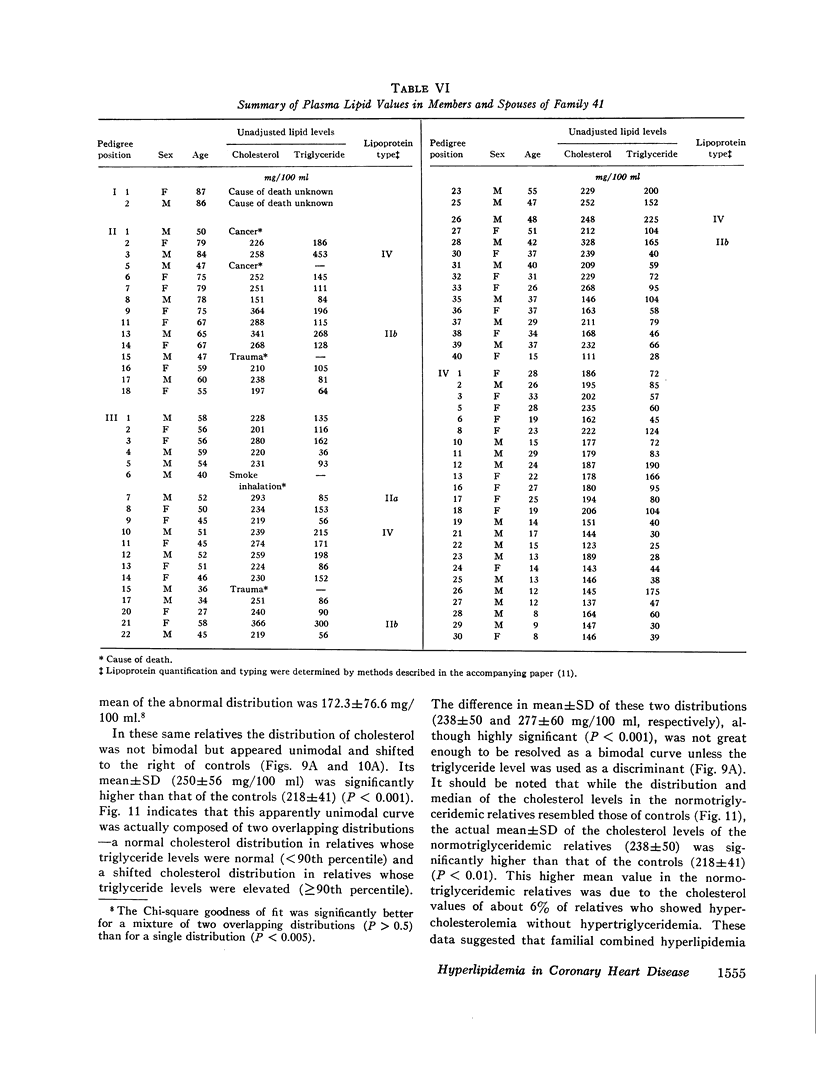
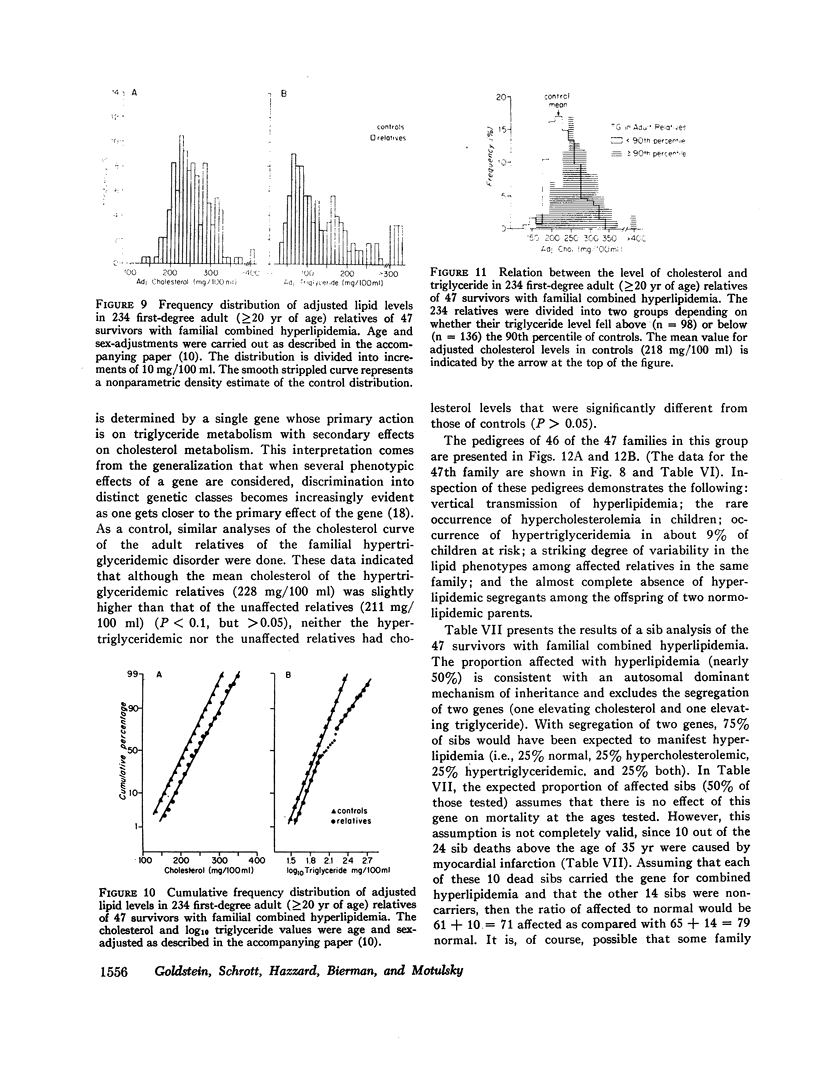
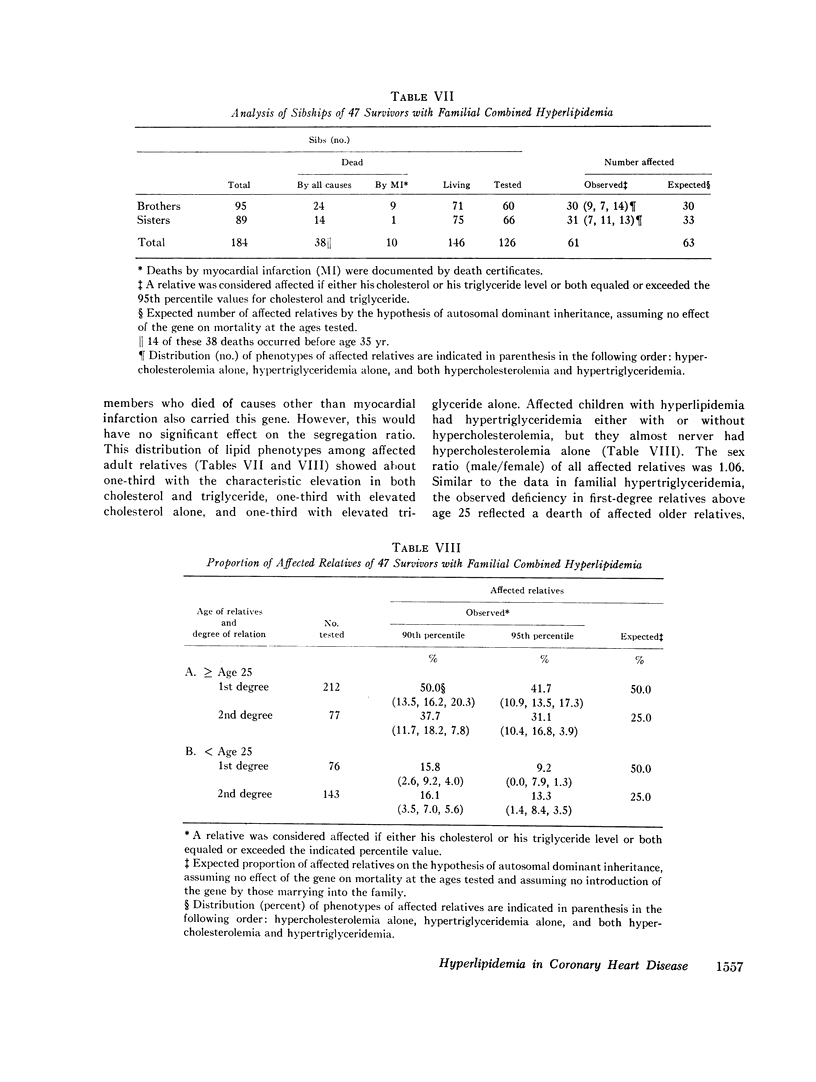
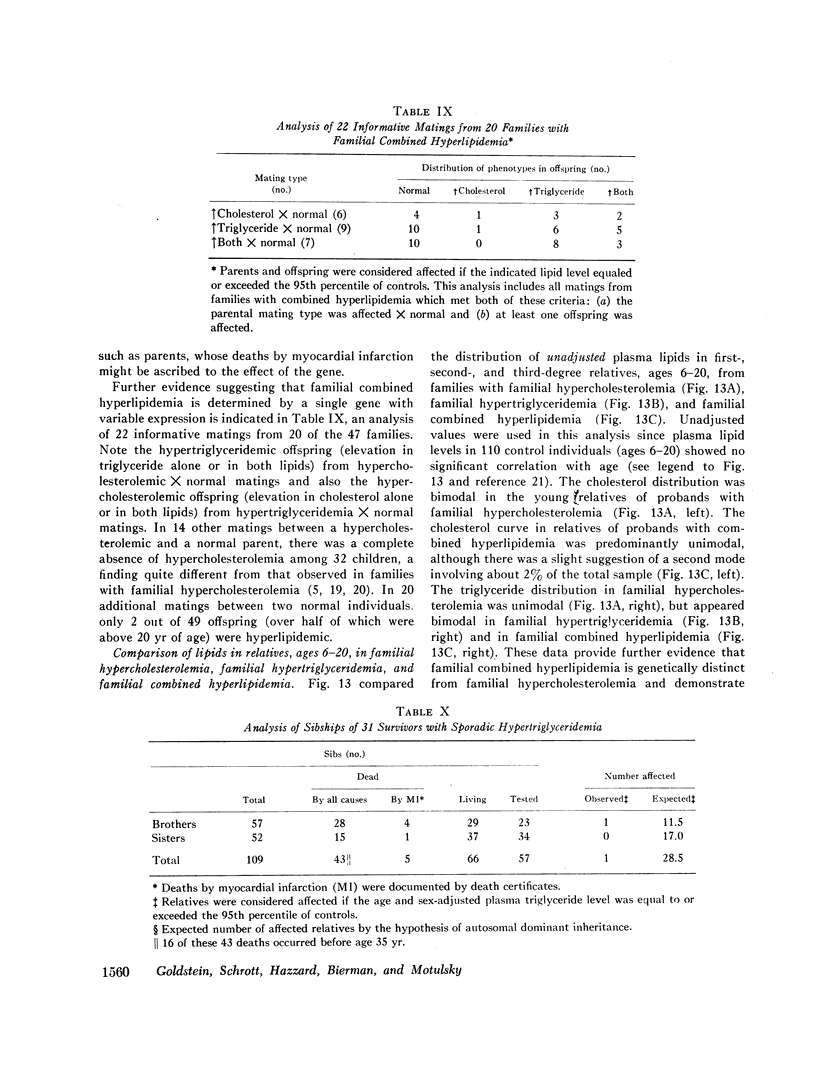
The most common genetic form of hyperlipidemia identified in this study has hitherto been poorly defined and has been designated as familial combined hyperlipidemia. Affected family members characteristically had elevated levels of both cholesterol and triglyceride. However, increased cholesterol or increased triglyceride levels alone were also frequently observed. The combined disorder was shown to be genetically distinct from familial hypercholesterolemia and familial hypertriglyceridemia for the following reasons: (a) the distribution pattern of cholesterol and triglyceride levels in relatives of probands was unique; (b) children of individuals with combined hyperlipidemia did not express hypercholesterolemia in contrast to the finding of hypercholesterolemic children from families with familial hypercholesterolemia; and (c) analysis of informative matings suggested that the different lipid phenotypes owed their origin to variable expression of a single autosomal dominant gene and not to segregation of two separate genes, such as one elevating the level of cholesterol and the other elevating the level of triglyceride.
Heterozygosity for one of the three lipid-elevating genes identified in this study may have a frequency in the general population of about 1%, constituting a major problem in early diagnosis and preventive therapy.
Full text
PDF


Images in this article
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Beaumont J. L., Carlson L. A., Cooper G. R., Fejfar Z., Fredrickson D. S., Strasser T. Classification of hyperlipidaemias and hyperlipoproteinaemias. Bull World Health Organ. 1970;43(6):891–915. [PMC free article] [PubMed] [Google Scholar]
- Bilheimer D. W., Eisenberg S., Levy R. I. The metabolism of very low density lipoprotein proteins. I. Preliminary in vitro and in vivo observations. Biochim Biophys Acta. 1972 Feb 21;260(2):212–221. doi: 10.1016/0005-2760(72)90034-3. [DOI] [PubMed] [Google Scholar]
- Carter C. O. Genetics of common disorders. Br Med Bull. 1969 Jan;25(1):52–57. doi: 10.1093/oxfordjournals.bmb.a070671. [DOI] [PubMed] [Google Scholar]
- Edwards J. H. Familial predisposition in man. Br Med Bull. 1969 Jan;25(1):58–64. doi: 10.1093/oxfordjournals.bmb.a070672. [DOI] [PubMed] [Google Scholar]
- Fredrickson D. S., Levy R. I., Lees R. S. Fat transport in lipoproteins--an integrated approach to mechanisms and disorders. N Engl J Med. 1967 Jan 19;276(3):148–contd. doi: 10.1056/NEJM196701192760305. [DOI] [PubMed] [Google Scholar]
- Goldstein J. L., Hazzard W. R., Schrott H. G., Bierman E. L., Motulsky A. G. Genetics of hyperlipidemia in coronary heart disease. Trans Assoc Am Physicians. 1972;85:120–138. [PubMed] [Google Scholar]
- Goldstein J. L., Hazzard W. R., Schrott H. G., Bierman E. L., Motulsky A. G. Hyperlipidemia in coronary heart disease. I. Lipid levels in 500 survivors of myocardial infarction. J Clin Invest. 1973 Jul;52(7):1533–1543. doi: 10.1172/JCI107331. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Havel R. J. Pathogenesis, differentiation and management of hypertriglyceridemia. Adv Intern Med. 1969;15:117–154. [PubMed] [Google Scholar]
- Hazzard W. R., Goldstein J. L., Schrott M. G., Motulsky A. G., Bierman E. L. Hyperlipidemia in coronary heart disease. 3. Evaluation of lipoprotein phenotypes of 156 genetically defined survivors of myocardial infarction. J Clin Invest. 1973 Jul;52(7):1569–1577. doi: 10.1172/JCI107333. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jensen J., Blankenhorn D. H. The inheritance of familial hypercholesterolemia. Am J Med. 1972 Apr;52(4):499–516. doi: 10.1016/0002-9343(72)90041-1. [DOI] [PubMed] [Google Scholar]
- Kannel W. B., Castelli W. P., Gordon T., McNamara P. M. Serum cholesterol, lipoproteins, and the risk of coronary heart disease. The Framingham study. Ann Intern Med. 1971 Jan;74(1):1–12. doi: 10.7326/0003-4819-74-1-1. [DOI] [PubMed] [Google Scholar]
- MURPHY E. A. ONE CAUSE?MANY CAUSES?THE ARGUMENT FROM THE BIMODAL DISTRIBUTION. J Chronic Dis. 1964 Apr;17:301–324. doi: 10.1016/0021-9681(64)90073-6. [DOI] [PubMed] [Google Scholar]
- Matthews R. J. Type 3 and IV familial hyperlipoproteinemia. Evidence that these two syndromes are different phenotypic expressions of the same mutant gene(s). Am J Med. 1968 Feb;44(2):188–199. doi: 10.1016/0002-9343(68)90150-2. [DOI] [PubMed] [Google Scholar]
- Murphy E. A., Bolling D. R. Testing of single locus hypotheses where there is incomplete separation of the phenotypes. Am J Hum Genet. 1967 May;19(3 Pt 1):322–334. [PMC free article] [PubMed] [Google Scholar]
- Murphy E. A. Some difficulties in the investigation of genetic factors in coronary artery disease. Can Med Assoc J. 1967 Nov 11;97(20):1181–1192. [PMC free article] [PubMed] [Google Scholar]
- Nevin N. C., Slack J. Hyperlipidaemic xanthomatosis. II. Mode of inheritance in 55 families with essential hyperlipidaemia and xanthomatosis. J Med Genet. 1968 Mar;5(1):9–28. doi: 10.1136/jmg.5.1.9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- PENROSE L. S. Measurement of pleiotropic effects in phenylketonuria. Ann Eugen. 1951 Sep;16(2):134–141. doi: 10.1111/j.1469-1809.1951.tb02467.x. [DOI] [PubMed] [Google Scholar]
- Patterson D., Slack J. Lipid abnormalities in male and female survivors of myocardial infarction and their first-degree relatives. Lancet. 1972 Feb 19;1(7747):393–399. doi: 10.1016/s0140-6736(72)90853-7. [DOI] [PubMed] [Google Scholar]
- Rose H. G., Kranz P., Weinstock M., Juliano J., Haft J. I. Inheritance of combined hyperlipoproteinemia: evidence for a new lipoprotein phenotype. Am J Med. 1973 Feb;54(2):148–160. doi: 10.1016/0002-9343(73)90218-0. [DOI] [PubMed] [Google Scholar]
- Schreibman P. H., Wilson D. E., Arky R. A. Familial type IV hyperlipoproteinemia. N Engl J Med. 1969 Oct 30;281(18):981–985. doi: 10.1056/NEJM196910302811803. [DOI] [PubMed] [Google Scholar]
- Schrott H. G., Goldstein J. L., Hazzard W. R., McGoodwin M. M., Motulsky A. G. Familial hypercholesterolemia in a large indred. Evidence for a monogenic mechanism. Ann Intern Med. 1972 May;76(5):711–720. doi: 10.7326/0003-4819-76-5-711. [DOI] [PubMed] [Google Scholar]
- Slack J. Risks of ischaemic heart-disease in familial hyperlipoproteinaemic states. Lancet. 1969 Dec 27;2(7635):1380–1382. doi: 10.1016/s0140-6736(69)90930-1. [DOI] [PubMed] [Google Scholar]