

Abstract
Although analysis of lipoprotein phenotypes is widely used to diagnose and classify the familial hyperlipidemias, an evaluation of this system as a method for genetic classification has hitherto not been published. The present study of 156 genetically defined survivors of myocardial infarction was therefore designed to examine the relationship between lipoprotein phenotypes and genetic lipid disorders. The lipoprotein phenotypes of each survivor was determined primarily by measurement of his plasma triglyceride and low density lipoprotein (LDL)-cholesterol concentrations; his genetic disorder was identified by analysis of whole plasma cholesterol and triglyceride levels in relatives.
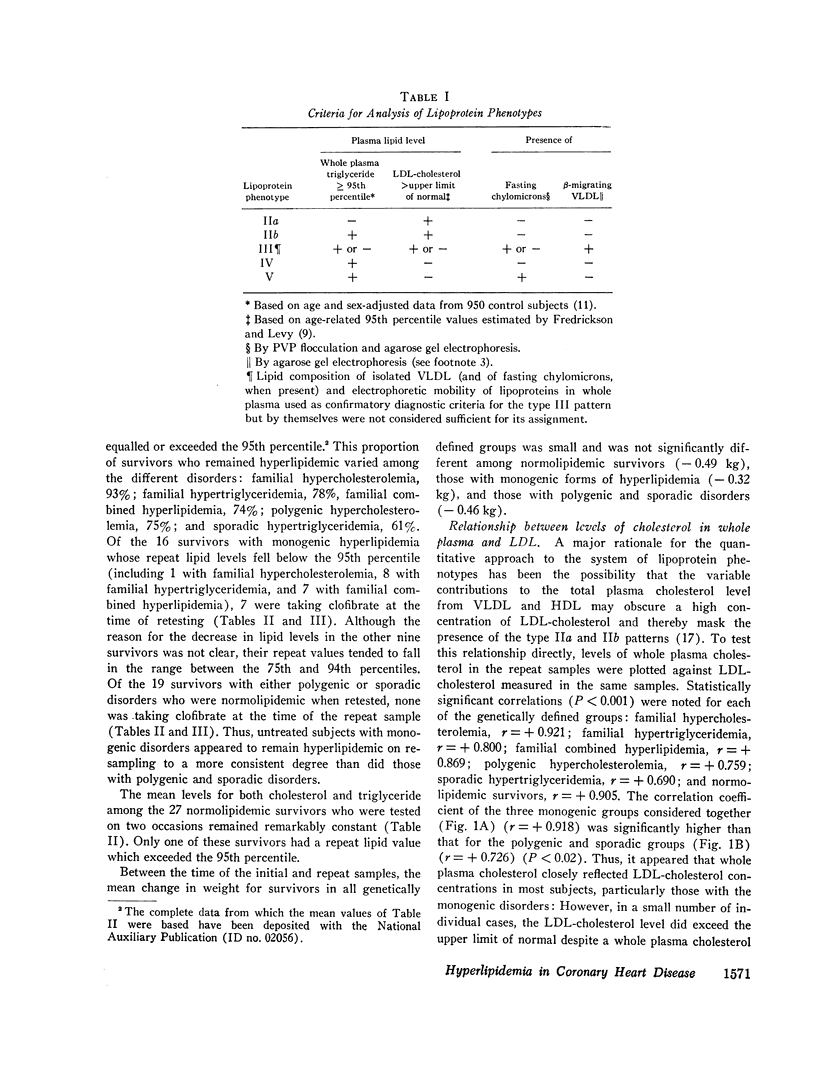
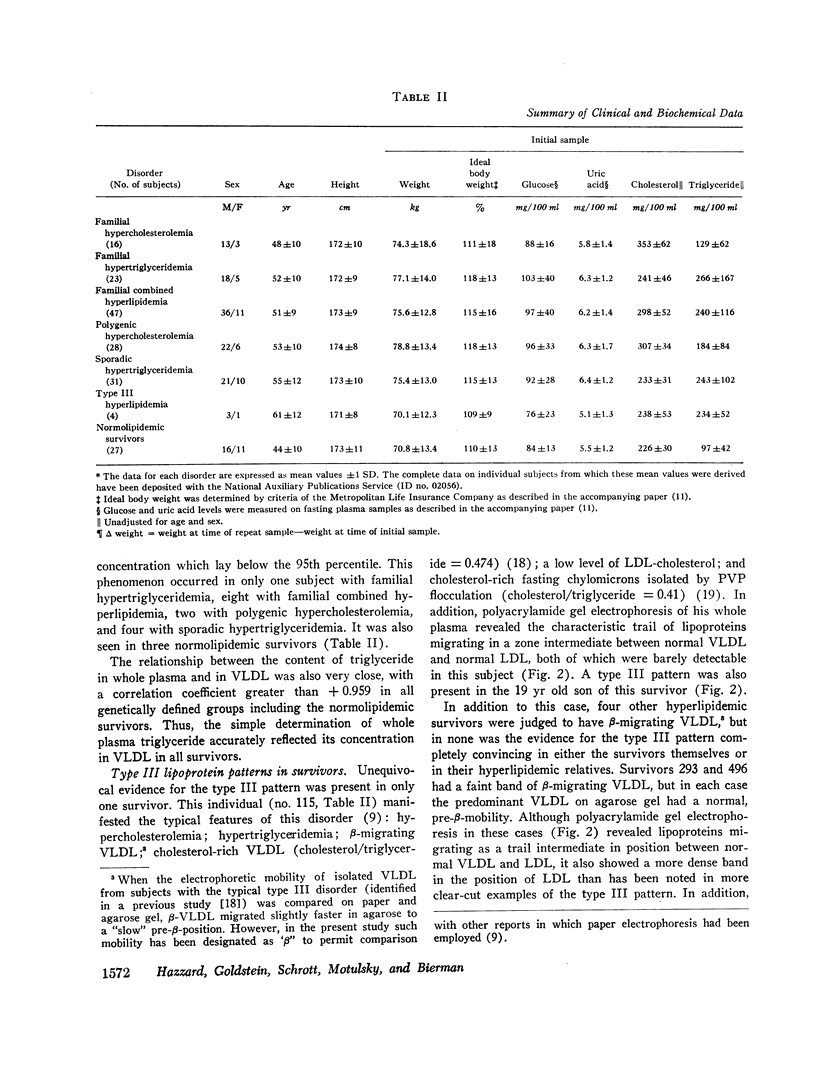
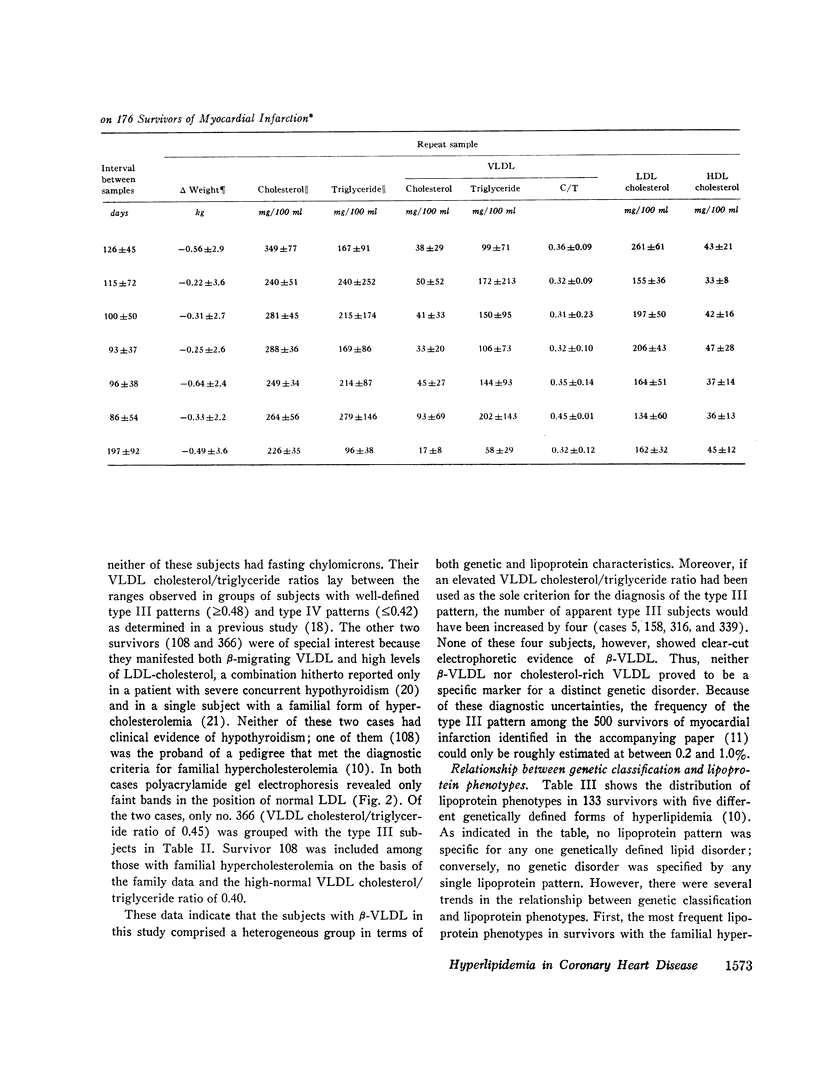
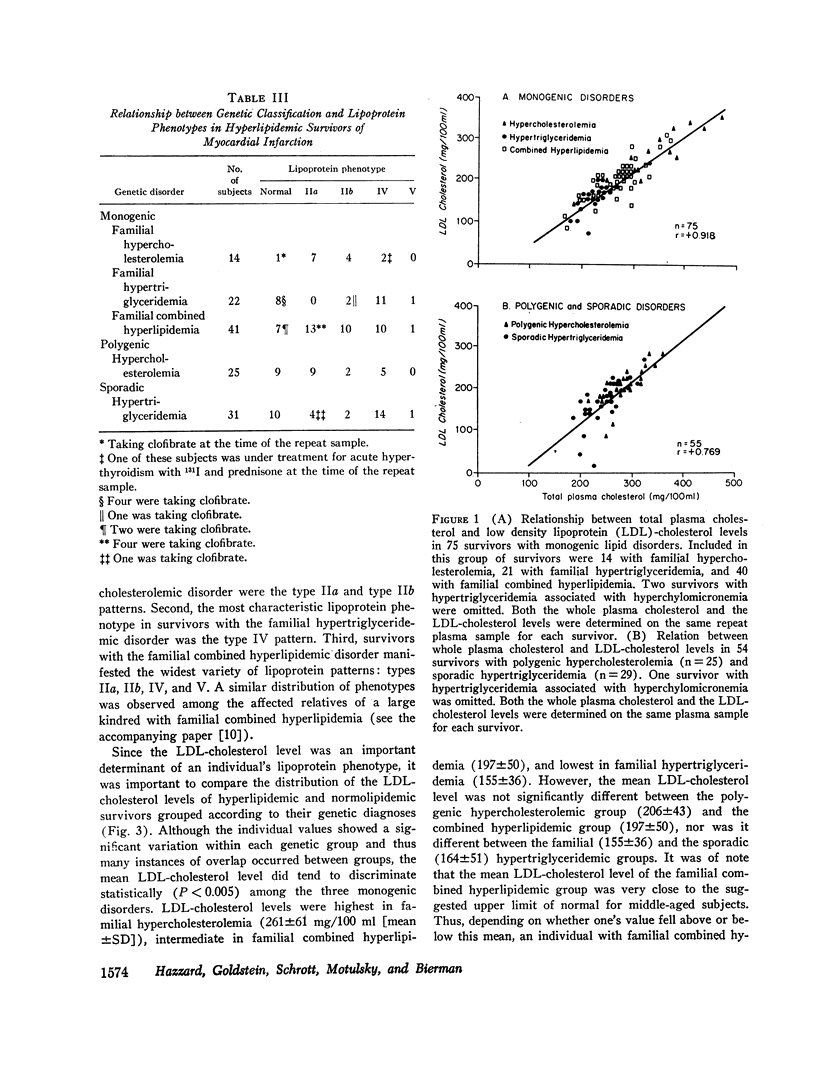
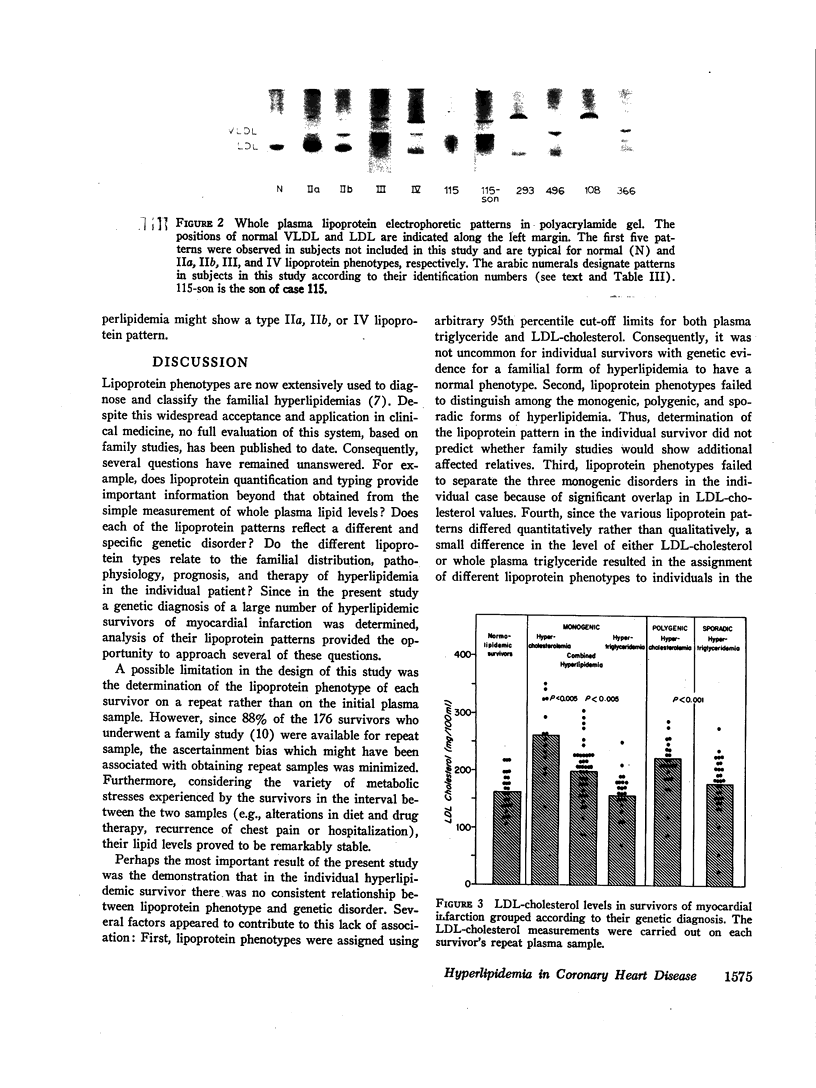
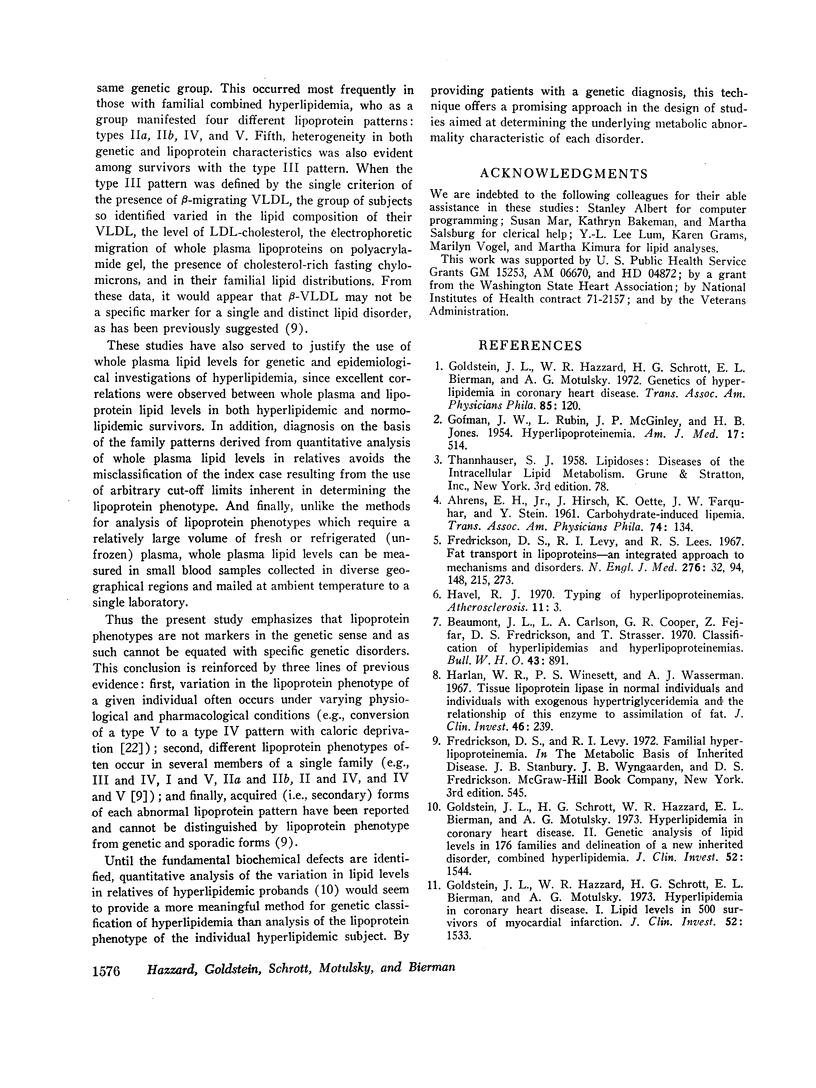
The mean levels of LDL-cholesterol discriminated statistically among the three monogenic lipid disorders; it was highest in survivors with familial hypercholesterolemia (261±61 mg/100 ml [mean ±SD]); intermediate in those with familial combined hyperlipidemia (197±50); and lowest in those with familial hypertriglyceridemia (155±36) (P < 0.005 among the three groups). However, on an individual basis no lipoprotein pattern proved to be specific for any particular genetic lipid disorder; conversely, no genetic disorder was specified by a single lipoprotein pattern. This lack of correlation occurred for the following reasons: (a) individual LDL-cholesterol levels frequently overlapped between disorders; (b) in many instances a small quantitative change in the level of either LDL-cholesterol or whole plasma triglyceride caused qualitative differences in lipoprotein phenotypes, especially in individuals with familial combined hyperlipidemia, who showed variable expression (types IIa, IIb, IV, or V); (c) lipoprotein phenotypes failed to distinguish among monogenic, polygenic, and sporadic forms of hyperlipidemia; (d) clofibrate treatment of some survivors with genetic forms of hyperlipidemia caused their levels of triglyceride and LDL-cholesterol to fall below the 95th percentile, thus resulting in a normal phenotype; and (e) β-migrating very low density lipoproteins (β-VLDL), previously considered a specific marker for the type III hyperlipidemic disorder, was identified in several survivors with different lipoprotein characteristics and familial lipid distributions.
These studies indicate that lipoprotein phenotypes are not qualitative markers in the genetic sense but instead are quantitative parameters which may vary among different individuals with the same genetic lipid disorder. It would therefore seem likely that a genetic classification of the individual hyperlipidemic patient with coronary heart disease made from a quantitative analysis of lipid levels in his relatives may provide a more meaningful approach than determination of lipoprotein phenotypes.
Full text
PDF

Images in this article

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- AHRENS E. H., Jr, HIRSCH J., OETTE K., FARQUHAR J. W., STEIN Y. Carbohydrate-induced and fat-induced lipemia. Trans Assoc Am Physicians. 1961;74:134–146. [PubMed] [Google Scholar]
- BURSTEIN M., SAMAILLE J. [On a rapid determination of the cholesterol bound to the serum alpha- and beta-lipoproteins]. Clin Chim Acta. 1960 Jul;5:609–609. doi: 10.1016/0009-8981(60)90075-9. [DOI] [PubMed] [Google Scholar]
- Beaumont J. L., Carlson L. A., Cooper G. R., Fejfar Z., Fredrickson D. S., Strasser T. Classification of hyperlipidaemias and hyperlipoproteinaemias. Bull World Health Organ. 1970;43(6):891–915. [PMC free article] [PubMed] [Google Scholar]
- DAVIS B. J. DISC ELECTROPHORESIS. II. METHOD AND APPLICATION TO HUMAN SERUM PROTEINS. Ann N Y Acad Sci. 1964 Dec 28;121:404–427. doi: 10.1111/j.1749-6632.1964.tb14213.x. [DOI] [PubMed] [Google Scholar]
- Fredrickson D. S., Levy R. I., Lees R. S. Fat transport in lipoproteins--an integrated approach to mechanisms and disorders. N Engl J Med. 1967 Jan 19;276(3):148–contd. doi: 10.1056/NEJM196701192760305. [DOI] [PubMed] [Google Scholar]
- GOFMAN J. W., RUBIN L., McGINLEY J. P., JONES H. B. Hyperlipoproteinemia. Am J Med. 1954 Oct;17(4):514–520. doi: 10.1016/0002-9343(54)90126-6. [DOI] [PubMed] [Google Scholar]
- Goldstein J. L., Hazzard W. R., Schrott H. G., Bierman E. L., Motulsky A. G. Genetics of hyperlipidemia in coronary heart disease. Trans Assoc Am Physicians. 1972;85:120–138. [PubMed] [Google Scholar]
- Goldstein J. L., Hazzard W. R., Schrott H. G., Bierman E. L., Motulsky A. G. Hyperlipidemia in coronary heart disease. I. Lipid levels in 500 survivors of myocardial infarction. J Clin Invest. 1973 Jul;52(7):1533–1543. doi: 10.1172/JCI107331. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Goldstein J. L., Schrott H. G., Hazzard W. R., Bierman E. L., Motulsky A. G. Hyperlipidemia in coronary heart disease. II. Genetic analysis of lipid levels in 176 families and delineation of a new inherited disorder, combined hyperlipidemia. J Clin Invest. 1973 Jul;52(7):1544–1568. doi: 10.1172/JCI107332. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Harlan W. R., Jr, Winesett P. S., Wasserman A. J. Tissue lipoprotein lipase in normal individuals and in individuals with exogenous hypertriglyceridemia and the relationship of this enzyme to assimilation of fat. J Clin Invest. 1967 Feb;46(2):239–247. doi: 10.1172/JCI105526. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Havel R. J. Typing of hyperlipoproteinemias. Atherosclerosis. 1970 Jan-Feb;11(1):3–6. doi: 10.1016/0021-9150(70)90003-1. [DOI] [PubMed] [Google Scholar]
- Hazzard W. R., Bierman E. L. Aggravation of broad- disease (type 3 hyperlipoproteinemia) by hypothyroidism. Arch Intern Med. 1972 Dec;130(6):822–828. [PubMed] [Google Scholar]
- Hazzard W. R., Porte D., Jr, Bierman E. L. Abnormal lipid composition of chylomicrons in broad-beta disease (type 3hyperlipoproteinemia). J Clin Invest. 1970 Oct;49(10):1853–1858. doi: 10.1172/JCI106403. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hazzard W. R., Porte D., Jr, Bierman E. L. Abnormal lipid composition of very low density lipoproteins in diagnosis of broad-beta disease (type 3 hyperlipoproteinemia). Metabolism. 1972 Nov;21(11):1009–1019. doi: 10.1016/0026-0495(72)90031-5. [DOI] [PubMed] [Google Scholar]
- Noble R. P. Electrophoretic separation of plasma lipoproteins in agarose gel. J Lipid Res. 1968 Nov;9(6):693–700. [PubMed] [Google Scholar]
- O'Hara D. D., Porte D., Jr, Williams R. H. Use of constant composition polyvinylpyrrolidone columns to study the interaction of fat particles with plasma. J Lipid Res. 1966 Mar;7(2):264–269. [PubMed] [Google Scholar]
- Quarfordt S. H., Boston F., Hilderman H. Transfer of triglyceride between isolated human lipoproteins. Biochim Biophys Acta. 1971 Mar 16;231(2):290–294. doi: 10.1016/0005-2760(71)90141-x. [DOI] [PubMed] [Google Scholar]
- Rifkind B. Typing of hyperlipoproteinaemias. Atherosclerosis. 1970 May-Jun;11(3):545–546. doi: 10.1016/0021-9150(70)90032-8. [DOI] [PubMed] [Google Scholar]