

Abstract
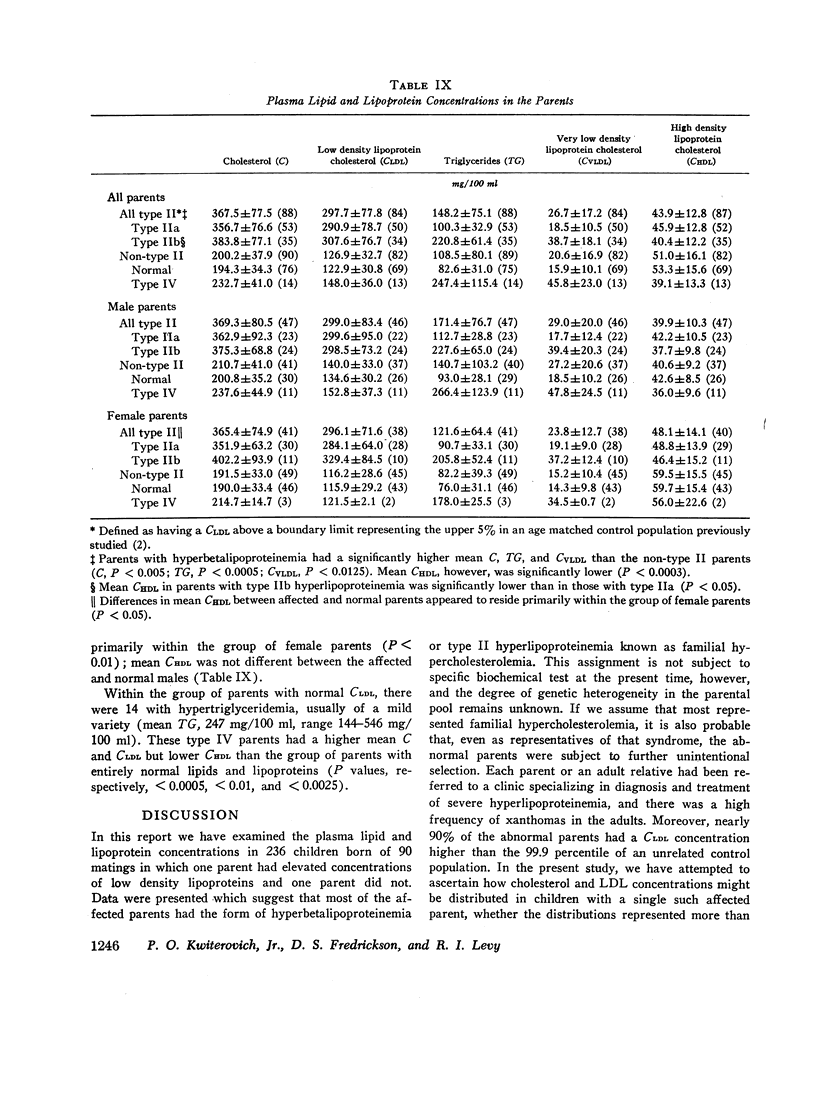
Primary hyperbetalipoproteinemia (type II hyperlipoproteinemia) is a common disorder associated with premature vascular disease. It is frequently due to genetic abnormalities, some of which are expressed in childhood. We have examined the manner in which that form of hyperbetalipoproteinemia known as familial hypercholesterolemia may be expressed in 236 children aged 1-19 born of 90 matings in which one parent had hyperbetalipoproteinemia of this variety and one parent did not.
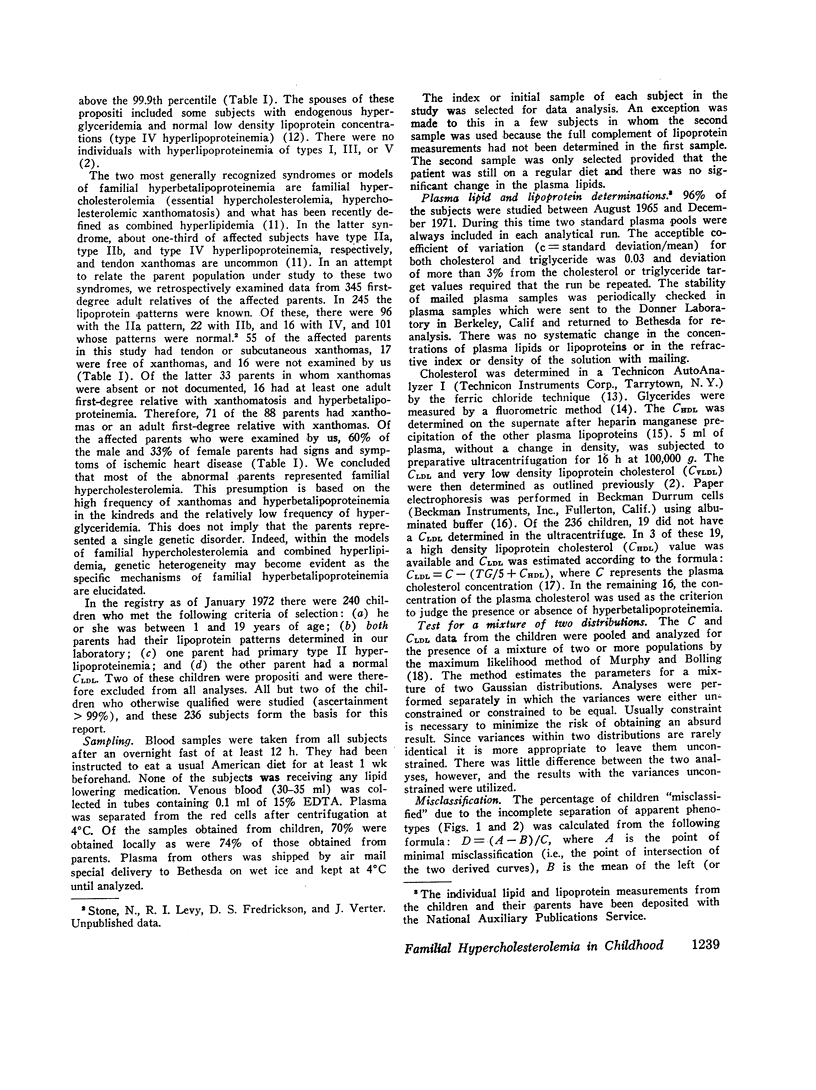
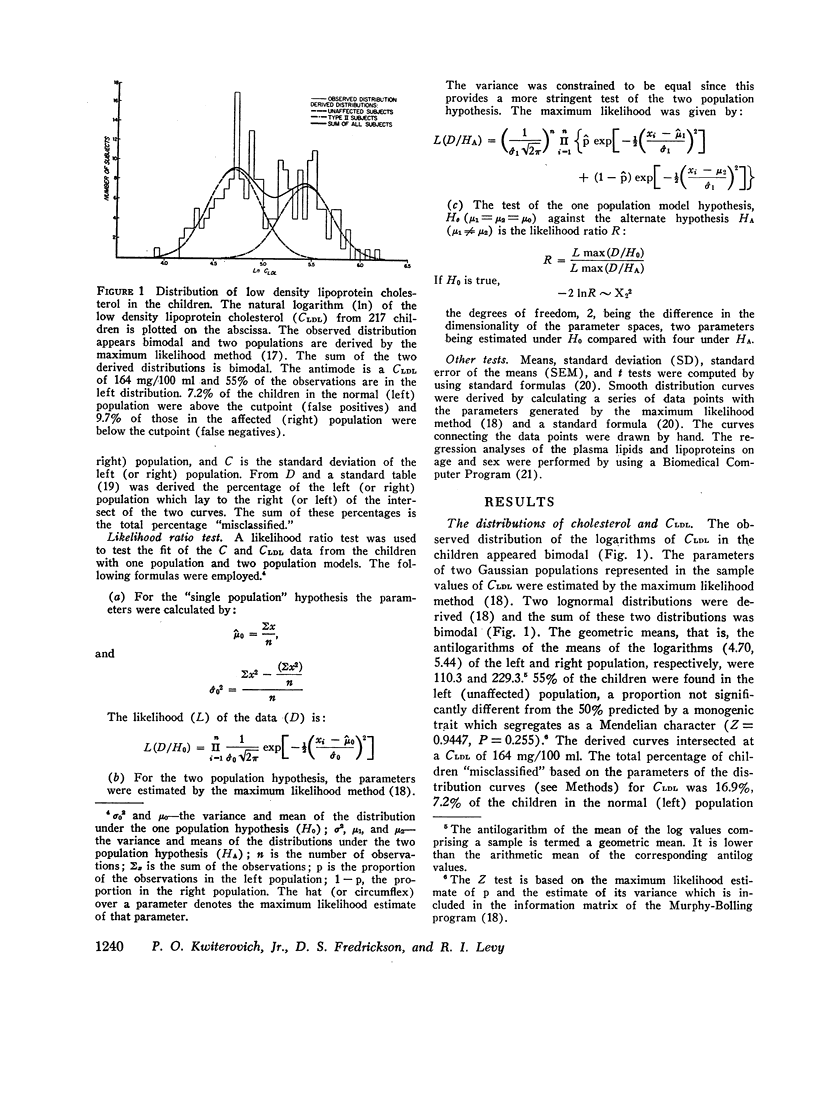
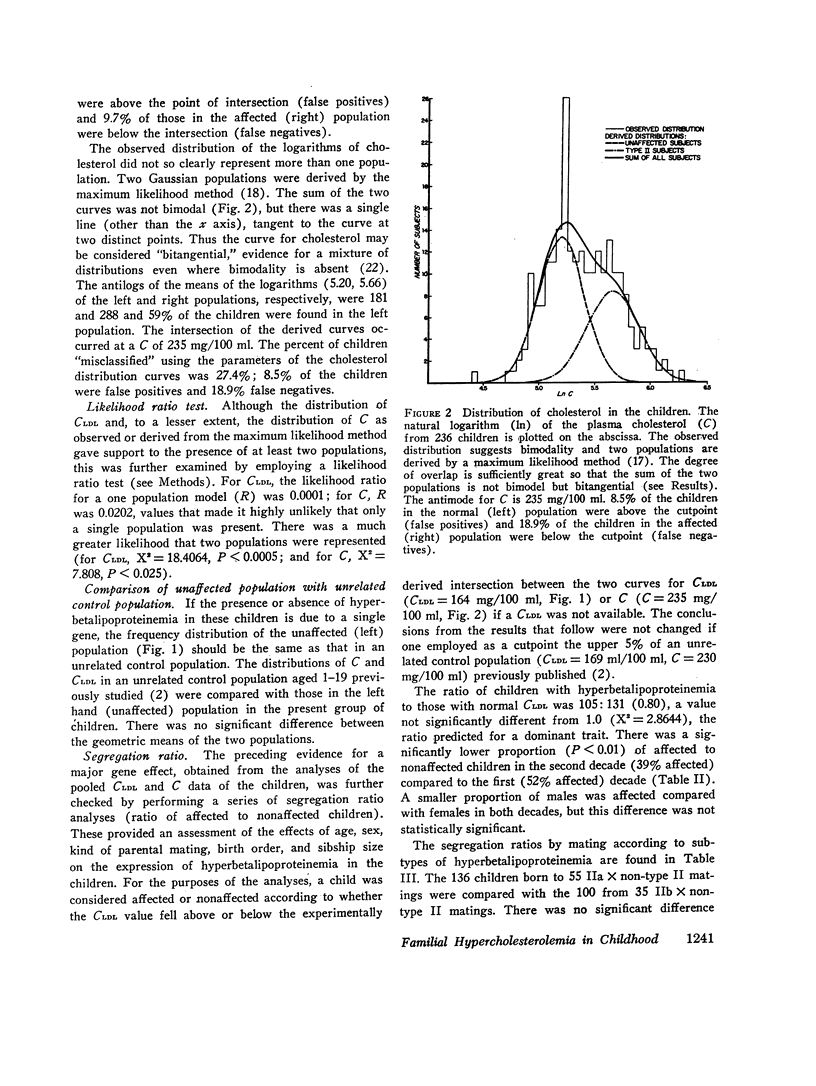
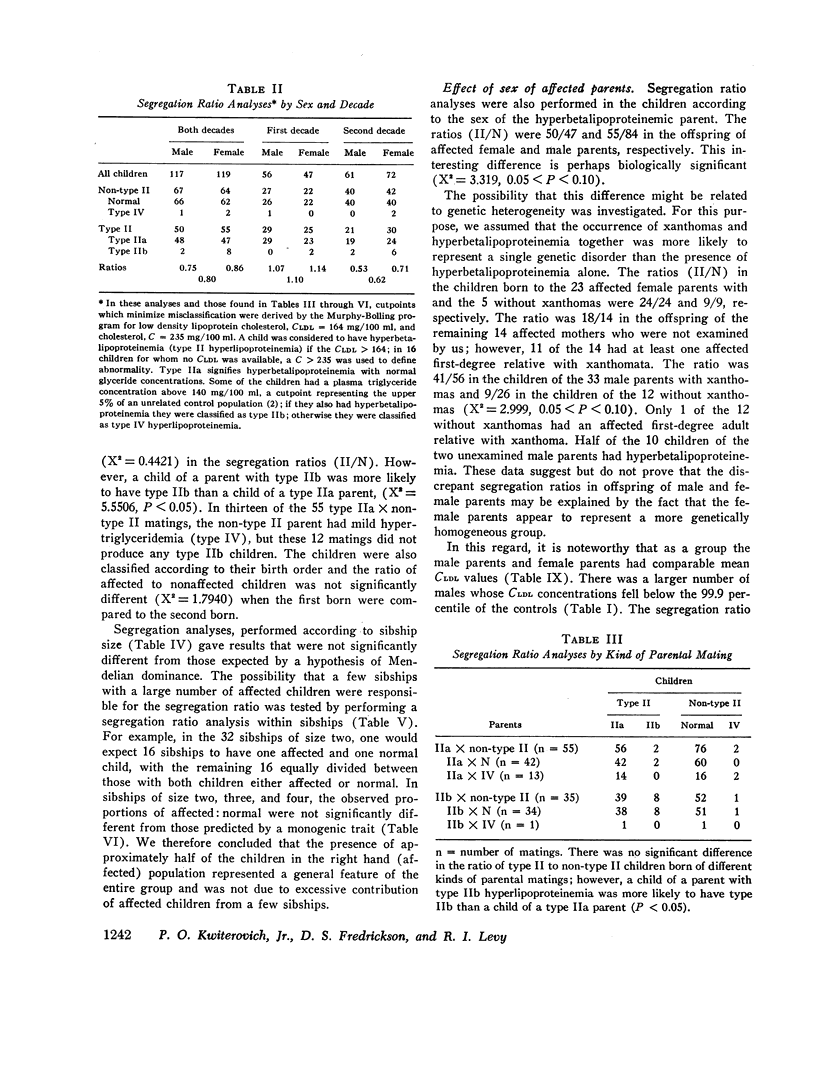
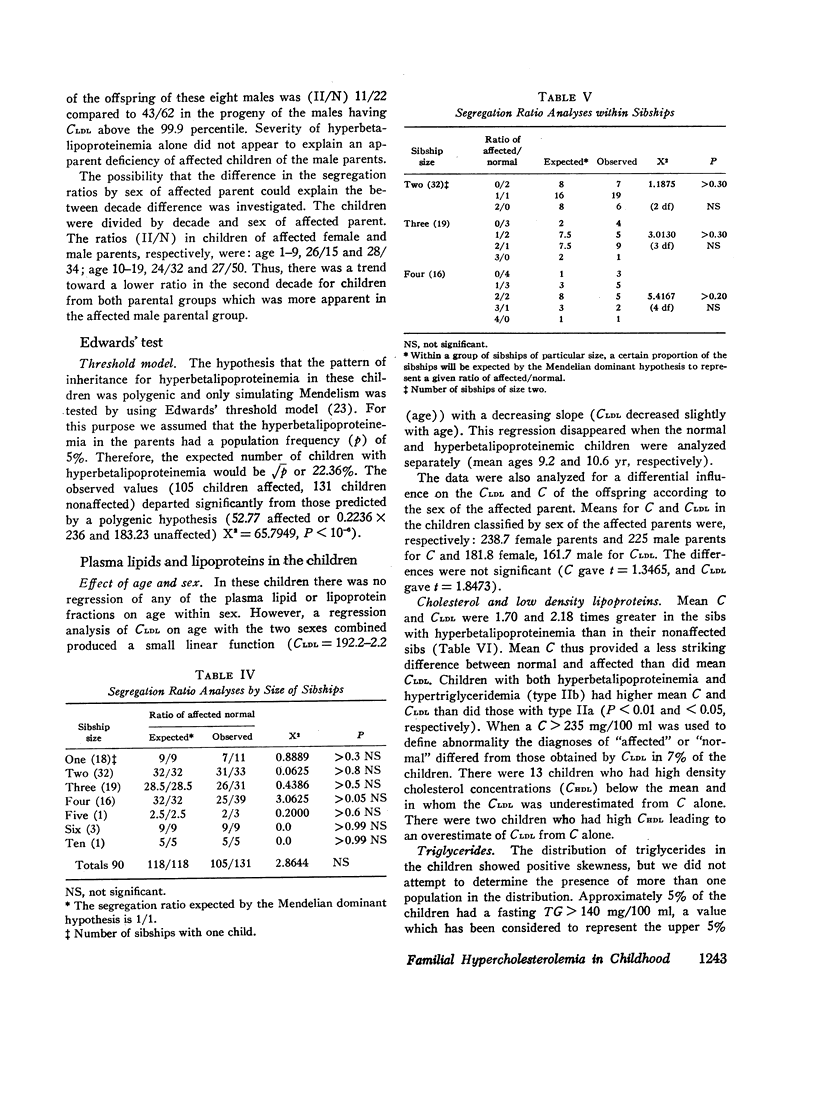
Two Gaussian populations were fitted to the distribution of both low density lipoprotein cholesterol (CLDL) and plasma cholesterol (C) in these children and a likelihood ratio test strongly favored a two over a one population model for both CLDL (X2 = 18.41, P < 0.0005) and C (X2 = 7.81, P < 0.025). 45% of the children were in the population identified as affected; their mean CLDL was 229. The remaining 55% were in the normal population with a mean CLDL of 110 which was indistinguishable from that of an unrelated control population, aged 1-19. On the basis of an assumed frequency of hyperbetalipoproteinemia in the general population of 5%, the Edwards' test indicated that a polygenic model of inheritance was highly unlikely (expected, 22%; observed, 45%).
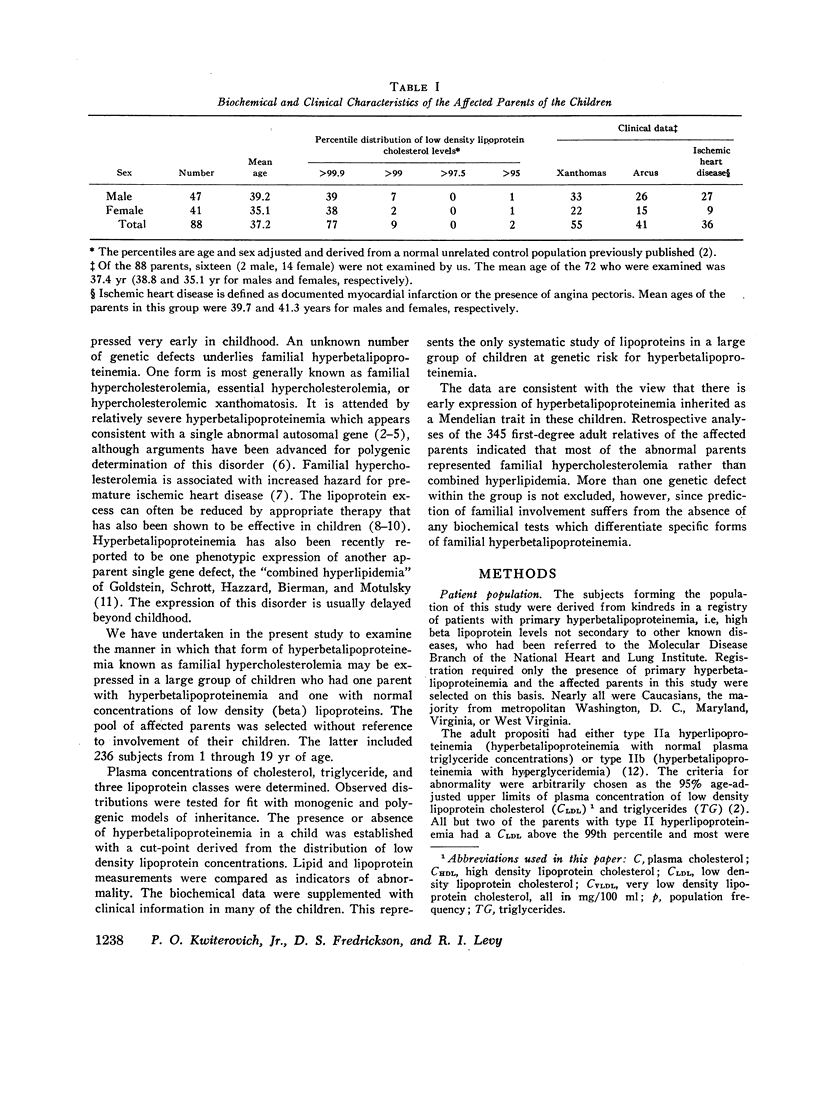
The segregation ratio obtained from the derived intersection between the two population curves (CLDL, 164 mg/100 ml; C, 235 mg/100 ml) was 45/55 (abnormal/normal). The percentage of abnormal children in the first decade (52%) significantly exceeded that in the second (39%) (P < 0.01). The ratios (II/N) were 50/47 and 55/84 in the offspring of affected female and male parents, respectively (X2 = 3.819, 0.05 < P < 0.10). Only 10% of hyperbetalipoproteinemic children were considered to have hyperglyceridemia. These children, frequently, but not invariably, had a parent with hyperglyceridemia in addition to hyperbetalipoproteinemia (P < 0.05). None of the affected children who were examined had ischemic heart disease (IHD) and 7% had tendon xanthomas. Half of the parents (mean age, 37.4 yr) who were examined had IHD and three-quarters had xanthomas.
The data agree well with the hypothesis that hyperbetalipoproteinemia is inherited as a monogenic trait with early expression in these children. More than one genetic defect within the group is not excluded, but retrospective analyses of the 345 first-degree adult relatives of the affected parents indicated that most of the abnormal parents probably represented familial hypercholesterolemia, rather than combined hyperlipidemia, the other most generally recognized form of familial hyperbetalipoproteinemia.
Full text
PDF

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- BURSTEIN M., SAMAILLE J. [On a rapid determination of the cholesterol bound to the serum alpha- and beta-lipoproteins]. Clin Chim Acta. 1960 Jul;5:609–609. doi: 10.1016/0009-8981(60)90075-9. [DOI] [PubMed] [Google Scholar]
- Beaumont J. L., Carlson L. A., Cooper G. R., Fejfar Z., Fredrickson D. S., Strasser T. Classification of hyperlipidaemias and hyperlipoproteinaemias. Bull World Health Organ. 1970;43(6):891–915. [PMC free article] [PubMed] [Google Scholar]
- Cole J. S., Wills R. E., Winterscheid L. C., Reichenbach D. D., Blackmon J. R. The Wolff-Parkinson-White syndrome: problems in evaluation and surgical therapy. Circulation. 1970 Jul;42(1):111–121. doi: 10.1161/01.cir.42.1.111. [DOI] [PubMed] [Google Scholar]
- EDWARDS J. H. The simulation of mendelism. Acta Genet Stat Med. 1960;10:63–70. doi: 10.1159/000151119. [DOI] [PubMed] [Google Scholar]
- Fredrickson D. S., Levy R. I., Lees R. S. Fat transport in lipoproteins--an integrated approach to mechanisms and disorders. N Engl J Med. 1967 Feb 2;276(5):273–concl. doi: 10.1056/NEJM196702022760507. [DOI] [PubMed] [Google Scholar]
- Friedewald W. T., Levy R. I., Fredrickson D. S. Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin Chem. 1972 Jun;18(6):499–502. [PubMed] [Google Scholar]
- Goldstein J. L., Schrott H. G., Hazzard W. R., Bierman E. L., Motulsky A. G. Hyperlipidemia in coronary heart disease. II. Genetic analysis of lipid levels in 176 families and delineation of a new inherited disorder, combined hyperlipidemia. J Clin Invest. 1973 Jul;52(7):1544–1568. doi: 10.1172/JCI107332. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jensen J., Blankenhorn D. H. The inheritance of familial hypercholesterolemia. Am J Med. 1972 Apr;52(4):499–516. doi: 10.1016/0002-9343(72)90041-1. [DOI] [PubMed] [Google Scholar]
- KHACHADURIAN A. K. THE INHERITANCE OF ESSENTIAL FAMILIAL HYPERCHOLESTEROLEMIA. Am J Med. 1964 Sep;37:402–407. doi: 10.1016/0002-9343(64)90196-2. [DOI] [PubMed] [Google Scholar]
- LEES R. S., HATCH F. T. Sharper separation of lipoprotein species by paper electrophoresis in albumin-containing buffer. J Lab Clin Med. 1963 Mar;61:518–528. [PubMed] [Google Scholar]
- Lee V. A. Individual trends in the total serum cholesterol of children and adolescents over a ten-year period. Am J Clin Nutr. 1967 Jan;20(1):5–12. doi: 10.1093/ajcn/20.1.5. [DOI] [PubMed] [Google Scholar]
- MURPHY E. A. ONE CAUSE?MANY CAUSES?THE ARGUMENT FROM THE BIMODAL DISTRIBUTION. J Chronic Dis. 1964 Apr;17:301–324. doi: 10.1016/0021-9681(64)90073-6. [DOI] [PubMed] [Google Scholar]
- Murphy E. A., Bolling D. R. Testing of single locus hypotheses where there is incomplete separation of the phenotypes. Am J Hum Genet. 1967 May;19(3 Pt 1):322–334. [PMC free article] [PubMed] [Google Scholar]
- Murphy E. A. Some difficulties in the investigation of genetic factors in coronary artery disease. Can Med Assoc J. 1967 Nov 11;97(20):1181–1192. [PMC free article] [PubMed] [Google Scholar]
- Nevin N. C., Slack J. Hyperlipidaemic xanthomatosis. II. Mode of inheritance in 55 families with essential hyperlipidaemia and xanthomatosis. J Med Genet. 1968 Mar;5(1):9–28. doi: 10.1136/jmg.5.1.9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schrott H. G., Goldstein J. L., Hazzard W. R., McGoodwin M. M., Motulsky A. G. Familial hypercholesterolemia in a large indred. Evidence for a monogenic mechanism. Ann Intern Med. 1972 May;76(5):711–720. doi: 10.7326/0003-4819-76-5-711. [DOI] [PubMed] [Google Scholar]
- Slack J. Risks of ischaemic heart-disease in familial hyperlipoproteinaemic states. Lancet. 1969 Dec 27;2(7635):1380–1382. doi: 10.1016/s0140-6736(69)90930-1. [DOI] [PubMed] [Google Scholar]
- West R. J., Lloyd J. K. Use of cholestyramine in treatment of children with familial hypercholesterolaemia. Arch Dis Child. 1973 May;48(5):370–374. doi: 10.1136/adc.48.5.370. [DOI] [PMC free article] [PubMed] [Google Scholar]