

Introduction
Dengue virus infection has emerged as a notable public health problem in recent decades in terms of the mortality and morbidity associated with it.(1) Dengue is endemic in many parts of India and epidemics are frequently reported from various parts of India(2–4) and abroad.(5,6) The case fatality rate in patients with dengue hemorrhagic fever (DHF) and dengue shock syndrome (DSS) can be as high as 44%.(7) Hence early and rapid laboratory diagnosis of dengue is crucial. Appropriate clinical management can save the lives of DHF and DSS patients and mortality can be reduced to less than 1%.(8) It is also worthwhile for planning appropriate control strategies. The present communication reports the seroprevalence of dengue infections occurred in Central India.
Materials and Methods
Study design
This was a cross-sectional study.
Setting
Central India's referral institute, i.e., Government Medical College and Hospital, Nagpur, was selected.
Participants
Indoor patients suspected of dengue or DHF or DSS were selected.
Methods
Blood samples from 131 suspected cases from medicine and pediatric wards were collected during a period from September 2005 to December 2006. Sera were separated and subjected for antidengue IgM and IgG antibody testing by the solid phase immunochromatographic assay, a commercial dengue virus rapid test kit manufactured by Standard Diagnostics, Inc., Korea, in the Department of Microbiology, GMCH, Nagpur, Maharashtra.
Results
Out of 131 cases, 41 (31.3%) were found to be positive for IgM or IgG or for both the antibodies. In 2005, the highest number of suspected dengue patients admitted was in the month of November, i.e., 41 with 15 (36.59%) positive followed by in October, i.e., 28 with 7 (25%) positive. However, in 2006, the highest number of dengue patients admitted was in the month of September, i.e., 24 with 14 (58.33%) positive followed by November, i.e., 5 with 2 (40%) positive. From January 2006 to August 2006, out of 16 suspected sera, no sample was found positive for dengue antibodies.
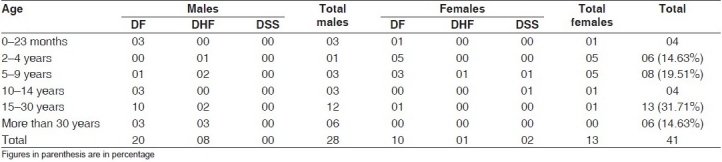
The most affected age group was 15 to 30 year, with 13 (31.71%), followed by the 5 to 9 year age group, with 08 (19.51%). The male-to female ratio was found to be 2.15:1 [Table 1].
Table 1.
Age- and sexwise distribution of dengue positive cases
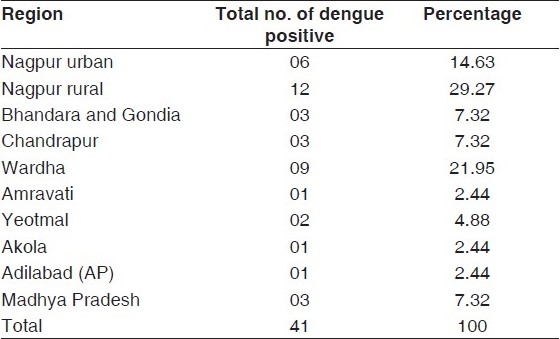
Majority of seropositive patients, i.e., 12 (29.27%), were from Nagpur district followed by 09 (21.95%) from Wardha district. A total of 06 (14.63%) positive patients were from Nagpur city only. Dengue was found prevalent not only in Vidarbha but also in Madhya Pradesh and Andhra Pradesh states [Table 2].
Table 2.
Frequencies of dengue positive cases by region of their residence
Discussion
In the present study, 31.3% patients were serologically positive for dengue infection. The dengue infection from Nagpur was reported earlier in 1965.(9) In Maharashtra, the dengue outbreak was reported from Parbhani(10) and Dhule.(11) In India, the outbreak of dengue was reported from Bangalore,(2) Punjab,(3) and Delhi.(4) The present dengue cases occurred during the postmonsoon season, i.e., from September to November only, which is similar to most of the previous outbreaks in India.(3,4) It may be because this season is very favorable for high breeding of the vector, i.e., Aedes aegypti. This seasonal outbreak of disease transmission is very important at local level for effective control measures.
The age group of 15-30 years was highly affected with dengue which is consistent with the outbreak in Delhi in 2003.(4) In some parts of the world, it is mainly a pediatric public health problem.(12) It is attributed to the changes in locations where disease transmission takes place. The higher prevalence of dengue infection was noted among male patients than female patients unlike other reports in which both the sexes were equally affected.(10) The male-to-female ratio was 2.15:1 which is comparable with the study in Delhi.(4) Male preponderance and the age group of 15-30 years indicate more transmission of dengue infections at work sites.
In this study, majority of the dengue-positive patients were from the rural areas of Vidarbha (Maharashtra), although 14.63% were from Nagpur city alone. The study also reveals that dengue infection is also prevalent in adjacent areas of Maharashtra like Chhindwada and Balaghat districts of Madhya Pradesh as well as Adilabad district of Andrapradesh. This suggests that dengue infection is no more an urban area infection but it is extending its arms to rural areas also, which may become a cause for concern to health authorities. This study calls for a careful vigil to prevent the possible transportation of the vector between different areas.
Conclusions
Dengue cases were more during September to November in the postmonsoon season which is useful to plan special preventive strategies. The study draws attention toward the male, young adult age group. Dengue infection is no more an urban area infection but it has penetrated in rural areas also.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
References
- 1.World Health Organization: Dengue haemorrhagic fever: Diagnosis, Treatment, Prevention and Control. 2nd ed. Geneva: World Health Organization; 1997. pp. 12–23. [Google Scholar]
- 2.George S, Soman RS. Studies on Dengue in Bangalore City: Isolation of virus from Man and Mosquitoes. Indian J Med Res. 1975;63:396–401. [PubMed] [Google Scholar]
- 3.Kaur H, Prabhakar H, Mathew P, Marshalla R, Arya M. Dengue haemorrhagic fever outbreak in October-November 1996 in Ludhiana, Panjab, India. Indian J Med Res. 1997;106:1–3. [PubMed] [Google Scholar]
- 4.Gupta E, Dar L, Narang P, Srivastava VK, Broor S. Serodiagnosis of dengue during an outbreak at a tertiary care hospital in Delhi. Indian J Med Res. 2005;121:36–8. [PubMed] [Google Scholar]
- 5.Fakeeh M, Zaki AM. Dengue in Jeddah, Saudi Arabia, 1994-2002. Dengue Bull. 2003;27:13–8. [Google Scholar]
- 6.Chalupa P, Kolarova M, Sojkova N, Januska J. Diagnosis of imported Dengue fever in the Czech Republic. Dengue Bull. 2003;27:34–8. [Google Scholar]
- 7.Perez JG, Clark GG, Gubler DJ, Reiter P, Sanders EJ, Vorndam AV. Dengue and Dengue haemorrhagic fever. Lancet. 1998;352:971–6. doi: 10.1016/s0140-6736(97)12483-7. [DOI] [PubMed] [Google Scholar]
- 8.Chaturvedi UC, Shrivastava R. Dengue haemorrhagic fever: A global challenge. Indian J Med Microbiol. 2004;22:5–10. [PubMed] [Google Scholar]
- 9.Rodrigues FM, Patankar MR, Banerjee K, Bhatt PN, Goverdhan MK, Pavri KM, et al. Etiology of the 1965 epidemic of febrile illness in Nagpur City, Maharashtra state, India. Bull WHO. 1972;46:173–9. [PMC free article] [PubMed] [Google Scholar]
- 10.Mehendale SM, Risbud AR, Rao JA, Banerjee K. Outbreak of Dengue fever in rural areas of Parbhani district of Maharashtra, India. Indian J Med Res. 1991;93:6–11. [PubMed] [Google Scholar]
- 11.Padbidri VS, Mahadev PV, Thakre JP, Pant U, Illkal MA, Varghese GG, et al. Virological and entomological investigations of an outbreak of Dengue fever in Dhule district, Maharashtra. Indian J Med Microbiol. 1996;14:25–32. [Google Scholar]
- 12.Gubler DJ. Dengue and Dengue haemorrhagic fever. Clin Microbiol Rev. 1998;11:480–96. doi: 10.1128/cmr.11.3.480. [DOI] [PMC free article] [PubMed] [Google Scholar]