

Abstract
Activity in the prefrontal cortex may distinguish the meta-awareness experienced during lucid dreams from its absence in normal dreams. To examine a possible relationship between dream lucidity and prefrontal task performance, we carried out a prospective study in 28 high school students. Participants performed the Wisconsin Card Sort and Iowa Gambling tasks, then for one week kept dream journals and reported sleep quality and lucidity-related dream characteristics. Participants who exhibited a greater degree of lucidity performed significantly better on the task that engages the ventromedial prefrontal cortex (the Iowa Gambling Task), but degree of lucidity achieved did not distinguish performance on the task that engages the dorsolateral prefrontal cortex (the Wisconsin Card Sort Task), nor did it distinguish self-reported sleep quality or baseline characteristics. The association between performance on the Iowa Gambling Task and lucidity suggests a connection between lucid dreaming and ventromedial prefrontal function.
Keywords: prefrontal cortex, lucid dreaming, Iowa gambling task, Wisconsin card sort task, dream cognition, metacognition, ventromedial prefrontal function, dorsolateral prefrontal function, meta-awareness, self-consciousness
Introduction
Dreaming is a state of consciousness that shares some characteristics with waking consciousness. In both states, there is an awareness of objects and events, and an awareness of oneself (Cicogna and Bosinelli, 2001). This similarity of awareness may reflect similar brain activation. In particular, forebrain activation by ascending arousal systems of the brainstem, diencephalon and basal forebrain promote consciousness in both waking and dreaming, albeit by anatomically and neurochemically distinct mechanisms (Hobson, 1988, Hobson et al., 2000, Muzur et al., 2002). A key difference in the conscious experience of waking, however, is the presence of meta-awareness or self-consciousness – insight into ones mental state. For example, in waking but not in dreaming there is an awareness of being awake, and the ability conceive of and differentiate the waking state from alternate mental states such as dreaming (Rechtschaffen, 1978, Pace-Schott, 2009).
A notable exception to this generality, however, is the phenomenon of lucid dreaming -- the explicit awareness, while dreaming, that one is dreaming (LaBerge, 1990, 1992, 2000, 2007). Lucidity may also be accompanied by the ability to exert deliberate control over dream outcome (LaBerge, 2007). Although the detection and characterization of lucid dreams must rely to a great extent on the report of the dreamer, pioneering experiments by LaBerge and colleagues demonstrated that experienced lucid dreamers were able to signal that they were having a lucid dream by specific eye movements, pre-determined before sleep and detected by electro-oculogram during REM sleep (LaBerge et al., 1981) as well as by voluntary control of respiration (LaBerge, 1990).
Fully lucid dreams occur on a continuum of lucidity with typical dreams (Lequerica, 1996; Barrett, 1992). Training can increase the frequency of lucid dreams and the degree of lucidity achieved (Purcell et al., 1986, LaBerge, 1990), with proficient lucid dreamers typically achieving their results only after extensive self-training (LaBerge, 1990, 1992, 2000, 2007). Despite the rarity of spontaneous lucidity, metacognition in dreams, or a degree of self-reflection about dream thoughts, intentions and feelings, may be more common than previously thought (Kahan and LaBerge, 1994, Kahan et al., 1997). For example, a study directly comparing waking and normal dreaming found similar levels of self-reflection and about half as much voluntary choice in dreams relative to waking (LaBerge, 2000). Similarly, the ability to reflect on the contents of ones own and other dream characters' minds, (so-called “theory-of-mind”; Frith and Frith, 2006), has been shown to be ubiquitous in dreaming (Kahn and Hobson, 2005, MacNamara et al., 2007, Pace-Schott, 2001).
Both normal and lucid dreaming are most commonly reported following awakenings from REM-containing periods of sleep (Hobson et al., 2000, LaBerge, 1990, 1992, 2000, 2007, Nielsen, 2000). Whereas there is a substantial rate of reporting normal dreaming following awakenings from non-REM (NREM) sleep (Foulkes, 1962, Nielsen, 2000), lucid dreaming appears to be much more closely related to REM sleep (LaBerge, 1990, 1992, 2000, 2007). Brain activity during lucid dreams is similar to that during typical REM sleep in some respects (e.g. the absence of waking-like alpha [8-12 Hz] activity), but differs in others (e.g. brain activity over 30 Hz)(Voss et al. 1999). Hence lucid dreams may arise from periods of REM sleep (e.g. with transient elevation of brain activity during the phasic [rapid eye movement containing] periods of REM (Brylowski et al., 1989, LaBerge, 2007)), but are not REM sleep phenomena per se (Voss et al. 1999).
In typical dreams, the lack of awareness that one is dreaming has been attributed to deactivation of lateral frontal executive areas relative to waking (Muzur et al., 2002, Hobson et al., 2000). Indeed, it is these frontolateral regions, along with certain posterior multimodal association areas, that PET studies have shown remain deactivated throughout sleep, including REM (Maquet et al., 2005, Braun et al., 1997, Maquet et al., 1996, Braun et al., 1998). Such deactivation during normal dreaming may impair working memory such that the ability to retrospectively compare ongoing experience to experiences moments earlier is lost (Pace-Schott, 2005). If lack of lucidity in typical dreams reflects deactivation of frontal executive areas, it follows that lucid dreams may be characterized by relatively preserved or transiently elevated frontal activity with concomitant elevation of cognitive abilities that support executive function. Both fMRI and quantitative EEG studies have demonstrated elevation of cortical activity during phasic vs. tonic REM (Miyauchi et al., 2009, Wehrle et al., 2007, Corsi-Cabrera et al., 2008, Abe et al., 2008). Moreover a recent quantitative EEG study found similarly high gamma band (30-80 Hz) coherence in lateral frontal areas during waking and lucid dreaming that, in both of these states, was higher than in normal REM sleep (Voss et al., 2009). Therefore, as with polysomnographic studies, functional neuroimaging and quantitative EEG studies suggest that dream lucidity may be associated with transient elevation of frontal cortical activity.
Whereas the lateral frontal cortex typically remains deactivated relative to waking following the transition from NREM to REM, ventromedial prefrontal and anterior cingulate cortices reactivate as part of what has been termed the “anterior paralimbic REM activation area” (Nofzinger et al., 1997, 2004). This region can become activated in REM to levels exceeding waking (Nofzinger et al., 1997, 2004) and includes much of the subcortical limbic system (amygdala, ventral striatum, hypothalamus, basal forebrain) as well as other paralimbic cortices (e.g. parahippocampal and insular cortices; Nofzinger et al., 1997, 2004; and for review see Pace-Schott, 2009). Therefore, in addition to elevated activity in lateral frontal areas during lucid dreaming, it is possible that further elevation of REM-related activity in these ventromedial prefrontal regions also occurs during lucid dreaming. In waking, these ventromedial prefrontal areas support not only the self-related, social and emotional cognition that is ubiquitous in dream phenomenology (reviewed in Pace-Schott, 2009), but also support the affective guidance hypothesized to facilitate decision making (i.e. the Somatic Marker Hypothesis; Bechara et al., 2000a, Damasio, 2003).
In the present study our objective was to determine whether frontal cognitive and emotional, executive functions differed in persons who more readily have lucid dreams and those who do not. Answering this question relies on the observation that some individuals are more likely to have lucid dreams than others, and that this difference is stable (i.e. lucidity tends to reoccur in those who experience it; LaBerge, 1990, 1992). Hence individuals can be distinguished by their trait ability to more easily achieve degrees of lucidity. This trait may be related to neuropsychological traits with a similar degree of stability such as performance on executive function tasks. We hypothesized that performance on cognitive tasks that engage prefrontal cortical areas would differ between lucid and non-lucid dreamers. In particular, we hypothesized that lucid dreamers would show better performance on a cognitive task that engaged a brain region relevant to lucid dreaming, and hence potentially implicated in meta-awareness or other characteristics of the conscious experience.
To test this hypothesis we examined performance on two frontal cognitive tasks, the Wisconsin Card Sort Task (WCST; Berg, 1948) and the Iowa Gambling Task (IGT; Bechara et al., 1994, 1999), in high school students. The WCST and the IGT were chosen because performance of the former activates the dorsolateral prefrontal cortex (DLPFC; Monchi et al., 2001, Ko et al., 2008) and performance of the latter activates the ventromedial prefrontal cortex (VMPFC; Li et al., 2009, Lawrence et al., 2009, Lin et al., 2008). (Note however, that as event-related fMRI designs have become more temporally precise, more diverse frontal and striatal regions are seen to activate during the specific phases of both tasks; Monchi et al., 2001, Lawrence et al., 2009, Lin et al., 2008). The DLPFC is associated with executive function and working memory (Stuss et al., 2002) and the VMPFC is associated with measuring risk and reward in decision making (Kringelbach, 2005, Kringelbach and Rolls, 2004). High school students were chosen because there is anecdotal evidence that it is easier for younger persons to train themselves to have lucid dreams (Armstrong-Hickey, 1988).
Methods
Participants
28 students at a public high school in an affluent town in New York completed this study. Participants included 9th, 10th, 11th, and 12th graders with a mean age of 16 ± 1 [S.D.](range was 14-18). Participants were recruited by word of mouth and by flyers on campus. The inclusion criteria were only that the participant be an enrolled student and that they reported keeping a regular bedtime (within a 2-hour window for 6 nights out of 7) for the month prior to enrollment. Exclusion criteria were smoking 1 or more cigarettes in the past week or 5 or more in the past month, or currently taking medications that affect sleep or cognitive performance. 1 potential participant was excluded for use of a psychiatric medication. All participants gave written assent or written consent (for those 18 years of age) for their participation; written parental consent was also obtained for all participants regardless of age. During the assent/consent process, potential participants were required to restate in their own words the key features of the study and indicate their willingness to complete the study. The protocol and its assent and consent forms were approved by the Yale University Investigational Review Board. Participants were compensated with a $30 gift certificate for their participation.
Study Design
Participants in this study completed baseline assessments, performed two computer-based cognitive tasks, then completed 7 consecutive days of a lucid dream awareness protocol with daily sleep-related assessments.
Baseline assessments
Age, sex, current grade level, and handedness were taken as demographic variables. The Pittsburgh Sleep Quality Index (PSQI) was used to assess baseline sleep characteristics. The PSQI is a validated measure of self-reported sleep quantity and quality over the past month (Buysse et al., 1989). The global score on the PSQI ranges from 0 to 21, with lower numbers indicating better sleep, and values of 6 or more associated with sleep problems in adults (Buysse et al., 2008). The Baseline Lucidity Assessment (BLA) was developed for this study to assess dream awareness, control, and lucidity in dreams [see appendix C.]. Briefly, the BLA consists of 5 questions answered on a 5-point Likert scale where lower scores (range 5-25) reflect a greater degree of self-reported dream reflection, control, and lucidity.
Cognitive tasks
The IOWA gambling task
The computer-based Iowa Gambling Task (IGT; Psychological Assessment Resources, Inc.) (Bechara et al. 1994) was administered in its standard form. In the task, participants repeatedly select cards from one of four decks to win as much virtual “money” as possible. Each selection is associated with some amount of monetary gain and some amount of loss, where the gain may be greater or less than the loss. The gains and losses are determined by fixed schedules wherein two of the decks (A&B) are high-risk/high-reward and over time produce a net loss, and the other two decks (C&D) are low-risk/low-reward and over time produce a net gain. Participants select a total of 100 cards one at a time, and performance is measured as the difference between the number of cards selected from the advantageous decks (C&D) and the number of cards selected from the disadvantageous decks (from A&B). IGT net score is measured for each 20 cards selected (reported as the 1st through 5th quintiles) and for all 100 card (total). One male participant did not correctly complete the IGT so his data was not included in the analysis.
The Wisconsin Card Sort Task
Participants were administered the computer-based Wisconsin Card Sort Task (WCST; Psychological Assessment Resources, Inc.;Heaton, 1981). In the task, participants are required to sort cards by the design, number or color of the shapes on the cards, but are not instructed how to sort, only given feedback indicating whether their selection was correct or not. Once participants master the sorting rule, the rule is changed without indication other than the correct/incorrect feedback. In the full version of the task used in this study, two decks of 64 cards each are used. Participants are tested until they correctly master each of the sorting rules for both decks, or until there are no more cards to sort. Variables reported here are the total number of trials required, and the percent of all trials in which a perseverative error occurred (an error of sorting by a previously learned rule). Twenty-six of the 28 participants studied here completed the WCST in fewer than the maximum 128 trials.
Lucid Dream Awareness Protocol
Participants were instructed to follow a one-week protocol designed to maintain a high degree of dream awareness and promote lucidity (see appendix A.). Briefly, over the course of one week, participants attempted to promote dream awareness and lucidity by keeping a dream journal of all of their dreams, by focusing on the dream experience prior to falling asleep, by self-suggestion, and by maintaining basic sleep hygiene practices.
Daily Outcome Measures
On each of the 7 days of the lucid dream awareness protocol, participants completed a sleep questionnaire and a daily lucidity assessment. The sleep questionnaire has been used previously in research studies to assess qualitative sleep quality as well as other sleep-related data. Here, daily use of caffeine and cigarettes (noted at bedtime), and nightly sleep quality (noted upon awakening) is reported. No participant reported smoking cigarettes during the study and all participants reported drinking 3 caffeinated beverages or fewer per day on average during the study. Nightly sleep quality was measured on a 0-100, visual analog scale based on the well-validated St. Mary's Sleep Questionnaire (Leigh et al., 1988, Ellis et al., 1981), and was averaged over the 7 days.
The Morning Lucidity Assessment (MLA; see appendix C.) was also completed each morning upon awakening. The MLA is similar in structure and questions to the BLA but tailored to a daily assessment of the previous night's dreams. It is scored from 5-25 with lower scores indicating a higher degree of dream reflection and lucidity. In particular, questions #1 and #2 measure dream recall, question #3 measures dreaming meta-awareness (i.e., the awareness that one is dreaming), question #4 measures ability to control the direction of a dream, and question #5 measures prospective control of dream content. Because most participants had one or more nights in which they did not remember their dreams, and because the objective of the study was to assess the ability to have lucid dreams, peak lucidity on the MLA over the 7 days was used as the main lucidity outcome variable. Participants were then divided into “high” and “low” dream reflection/lucidity groups by a median split of their peak lucidity as measured on the MLA. These groups are referred to as “high lucidity” and “low lucidity” for simplicity hereafter.
Dream reports from each night were read and assessed for evidence of lucidity and control. Although reflective awareness and other metacognitive experiences may be underreported in dream reports (Kahan et al. 1997), this analysis was performed to test the validity of the results of the morning lucidity assessment. Lucidity was scored as present if any one or more of the participant's dream reports contained a reference to the realization of dreaming during the dream itself. Control was scored as present similarly if a dream report contained a reference to the dreamer making a willful choice as to the direction or outcome of the dream, or if the report indicated that the content of the dream had been successfully decided prior to sleep. Otherwise lucidity and/or control were scored as not present. Example excerpts from dream reports that were scored as lucid and/or with control are provided in appendix B.
Statistical Method
Initially, independent t-tests were used to compare difference in baseline characteristics (e.g., age, grade, PSQI), responses to individual questions on the Morning Lucidity Assessment, and performance on the WCST task between high and low lucidity groups as determined by median split of the peak Morning Lucidity Assessment score. Performance on the IGT was analyzed across trials using a linear mixed model with group ((high versus low lucidity) as a between-subjects factor and trial quintile (1-5) as a within-subjects explanatory factor. The interaction between group and trial was also modeled. In the above model, the best-fitting variance-covariance structure was determined by information criteria and subject was the clustering factor. Baseline characteristics such as age, grade, and measures of sleep quality were considered as covariates but were not significant and dropped for parsimony. . Likelihood that performance at trial quintiles 3, 4, and 5 differed from chance in each group was estimated using the cumulative binomial probability for the performance means. Potential associations between IGT and WCST task performance were assessed using correlation analysis.
To support the validity of our interpretation of the data, identical analyses were repeated using dream report assessments of lucidity and control in place of the Morning Lucidity Assessment. In three separate analyses, lucidity or control versus neither, lucidity versus no lucidity, and control versus no control were used to separate the participants into two groups just as the median split of peak Morning Lucidity Assessment was used in the original analysis.
Results
During the 7 days of the lucid dream awareness protocol, participants reported smoking no cigarettes, taking no medications or supplements, and drinking an average of less than one caffeinated beverage per day [range 0-3]. Mean and median peak lucidity as measured by the Morning Lucidity Assessment were 12.7±4.6 and 12 (range: 5-22), respectively. Division of the participants into the high (mean 9 ± 2) and low (mean 16 ± 4) lucidity groups by peak lucidity showed differences in the responses to 4 of the 5 questions of the MLA (Figure 1), with the greatest contributions coming from questions 3 and 4 (Q3: “I thought or knew that I was dreaming during my dreams”; Q4: “I was able to control some or all of what happened in my dreams”). There were no statistically significant differences between the high and low lucidity groups in age, grade, PSQI, nightly sleep quality, or the Wisconsin Card Sorting Task measures (Table 1). Females were represented non-significantly greater (85%) in the high lucidity group compared to the low lucidity group (53%) (Table 1).
Figure 1.
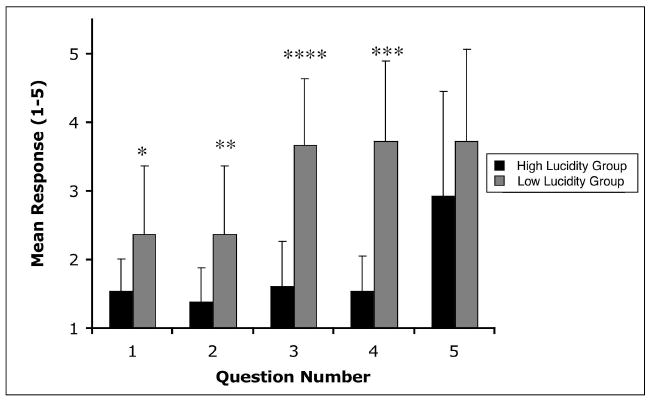
Morning Lucidity Assessment responses. The high and low lucidity groups were distinguished by 4 of the 5 questions on the morning lucidity assessment, with the greatest differences between groups seen in question 3 (“I thought or knew that I was dreaming during my dreams”) and question 4 (“I was able to control some or all of what happened in my dreams”; error bars indicate standard deviation; *, p<0.05; **, p<0.005, ***, p<10-5, ****, p<10-6).
Table 1. Demographic and Select Outcome Data.
| High Lucidity Group Peak lucidity <12 (N=13) | Low Lucidity Group Peak lucidity ≥12 (N=15)* | Statistics | ||||
|---|---|---|---|---|---|---|
| mean | s.d. | Mean | s.d. | t(26)* | P-value | |
| Age (years) | 16.1 | 1.1 | 16.2 | 0.9 | -0.32 | 0.75 |
| Grade | 10.5 | 0.8 | 10.5 | 0.9 | 0.02 | 0.99 |
| PSQI | 4.9 | 0.8 | 4.3 | 2.0 | 1.02 | 0.32 |
| BLA | 13.3 | 3.6 | 15.9 | 3.7 | -1.91 | 0.07 |
| Nightly Sleep Quality | 57 | 13 | 58 | 7 | -0.32 | 0.75 |
| WCST Raw Score | 93 | 20 | 98 | 21 | -0.58 | 0.56 |
| WCST Errors %perseverative | 10.8 | 4.4 | 14.4 | 10.5 | -1.15 | 0.26 |
| Females/Males (N) | 11/2 | 8/7 | - | 0.11** | ||
PSQI = Pittsburgh Sleep Quality Index, BLA = Baseline Lucidity Assessment, WCST = Wisconsin Card Sort Task, IGT = Iowa Gambling Task;
For the IGT, N=14 for peak lucidity ≥ 12 [see methods] with a corresponding loss of 1 degree of freedom,
Fisher's Exact test.
However, performance on the IGT was differentiated by peak lucidity. Analysis of IGT across trials revealed a significant main effect of trial quintile (F[4,100] = 5.3, P = 0.0006) and a trend effect for group (F[1,25]=3.5, P= 0.07). Importantly, the interaction between trial quintile and group was significant (F[4,100] = 2.8, P=0.03), explained by significantly greater IGT scores among high lucidity dreamers compared to their low lucidity counterparts during trial quintiles 3 (p=.03), 4 (p=.02), and 5 (p=.015)(Figure 2). Furthermore, mean performance during each of trial quintiles 3,4 and 5 was better than chance in the “high” lucidity group (0.006 < P < 0.02) but not in the “low” lucidity group (P > 0.25), and mean performance across trials 3-5 was better than chance in the “high” lucidity group (P < 0.00002) but not in the “low” lucidity group (P > 0.12)
Figure 2.
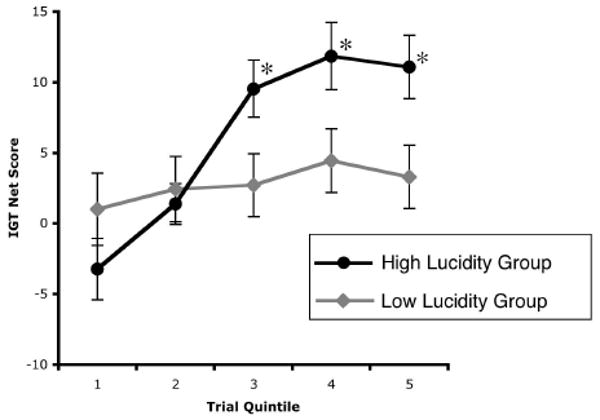
Iowa Gambling Task. Greater lucidity as measured on the Morning Lucidity Assessment was associated with IGT performance improvement as the task progressed. Statistically significant differences between groups occurred in the 3rd, 4th, and 5th quintiles of trials (error bars are ± standard error; *, p<0.05).
Total and individual trial IGT scores did not correlate with WCST performance as measured by WCST raw scores and %perseverative errors (all R2 < 0.08, p > 0.16).
Peak lucidity as measured by the MLA corresponded with the presence of lucidity or control on dream reports. 14 of 28 participants had evidence of lucidity or control in their dream reports (including 9 with lucidity, 12 with control, and 7 with both). Out of the 14 participants with evidence for lucidity or control in their dream reports, such evidence was present on 1.9 ± 0.7 (mean ± SD; range 1-3) of the 7 nights measured. Peak lucidity score on the MLA was assessed as a predictor of dream-report measured lucidity or control and was found to perform well in a range that included the group median (Figure 3).
Figure 3.
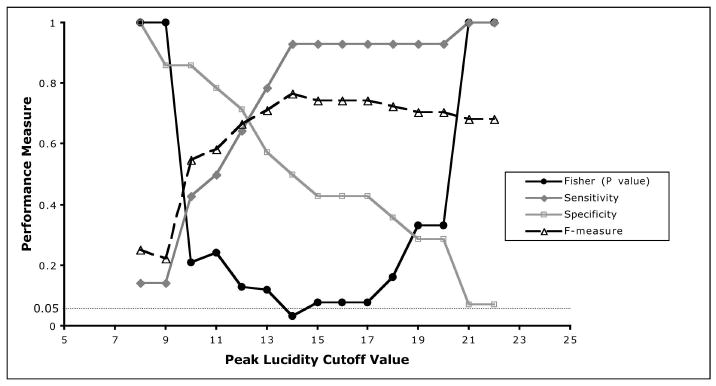
Peak lucidity as measured by the Morning Lucidity Assessment was assessed as a predictor of dream report evidence of lucidity-related phenomena. Dream report evidence of lucidity or dream control was compared to MLA-measured peak lucidity where values below a given cutoff value were considered to be evidence of lucidity. Sensitivity, specificity, F-measure (harmonic mean of positive predictive value and sensitivity), and the P-value of the Fisher Exact test are shown over a range of peak lucidity cutoff values on the Morning Lucidity Assessment. Higher values for sensitivity, specificity, and F-measure, and lower P-values indicate better prediction of dream report gauged lucidity by the MLA at a given cutoff value.
Analysis of the main outcome measures using dream report-measured lucidity or control resulted in statistical findings similar to that obtained with the MLA. In particular, there were no statistically significant differences in any of the measures reported in Table 1, except that retrospective baseline lucidity measured by the BLA was significantly different (t[26] = 2.37, P = 0.03) with the presence of lucidity or control in the dream reports associated with a greater lucidity score on the BLA. Furthermore, IGT performance was distinguished by the presence of dream report lucidity or control, with a significant interaction between trial quintile and group (F[4,100] = 4.86, P = 0.001) with statistically significant differences at trial quintiles 1 and 5 (Figure 4).
Figure 4.
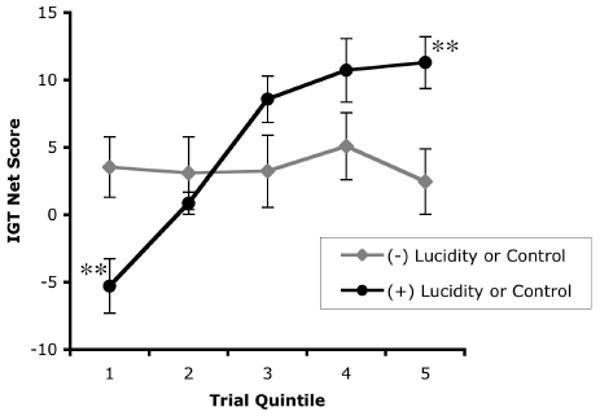
Iowa Gambling Task. The presence of lucidity-related dream phenomena including lucidity itself or control of dream outcome (+Lucidity or Control), as measured by dream report assessment, was associated with IGT performance improvement as the task progressed. Statistically significant difference between groups occurred in the 1st and 5th quintiles of trials (error bars are ± standard error; **, p< 0.01).
Separating the groups by the presence or absence of lucidity [regardless of control] or by control [regardless of lucidity] produced qualitatively similar results. However, in the case of lucidity [regardless of control], the trial quintile by group interaction was a statistical trend (F[4,100] = 2.24, P = 0.07), as were the post-hoc differences at trial quintiles 1 and 5 (P = 0.06 and P=0.05 respectively). In the case of control [regardless of lucidity], the statistically significant findings seen previously were seen with trial quintile by group interaction (F[4,100] = 5.27, P = 0.0007) and post-hoc differences at trial quintiles 1,4 and 5 (P = 0.01, 0.007, and 0.0009) respectively.
Discussion
In high school students participating in a lucid dream awareness protocol, we found that those who exhibited evidence of greater lucidity performed better on the Iowa Gambling Task. However, achieving lucidity did not distinguish performance on the Wisconsin Card Sorting Task, nor did it distinguish other potentially relevant characteristics like self-reported sleep quality prior to or during the study, age, and grade level. A relatively small difference in baseline, retrospective lucidity also was not statistically significant. The high lucidity group contained relatively more females than the low lucidity group - consistent with some prior observations (Armstrong-Hickey 1988) - but this difference was also not significant, and was not present when dream reports were used to assess lucidity. Hence, the difference in IGT performance between high and low lucidity groups was unique among the observed variables, and was in marked contrast to WCST performance. These findings have potential relevance to understanding brain function, and provide some potential insight into the relationship between meta-awareness or self-consciousness and other brain functions. Because the present work reflects only behavior measures, however, neuroanatomical interpretations must be considered speculative until confirmed with functional imaging.
The IGT was designed to assess affect-guided decision making under conditions of uncertainty (Bechara et al., 1997, Wagar and Dixon, 2006) whereas the WCST measures what is typically described as mental flexibility and set shifting ability (Lezak et al., 2004).
In adolescents, variation in performance and age-related changes in performance on the IGT appear to reflect development of the VMPFC and its connections. These variations are independent of performance on working memory and behavioral inhibition tasks thought to reflect activity of other prefrontal regions (e.g. DLPFC; Hooper et al. 2004). Notably, whereas lateral areas of the PFC remain relatively deactivated in REM sleep, VMPFC regions reactivate along with other subcortical aspects of the anterior paralimbic REM activation area (Maquet et al., 2005, Nofzinger et al., 1997, 2004). Therefore, the VMPFC physiological substrate believed to support IGT performance (Bechara et al., 1994, 1999, 2000b) is being selectively activated during REM — the presumed physiological substrate of lucid dreaming (LaBerge, 1990, 1992) — at the same time as regions that support WCST performance may remain relatively inactive. It is tempting to speculate that the developing capacity for emotion regulation and its integration with cognition, associated with prefrontal cortical development across adolescence (Yurgelun-Todd and Killgore, 2006, Whittle et al., 2008), underlies capacity for both lucid dream induction and affect-guided decision making.
Consequently, the ability to achieve lucidity during adolescence, a period of considerable brain myelination and re-organization (Tamnes et al., 2009), may be related to the degree to which frontal systems have become integrated and able to receive coherent input from a variety of sources, including emotional information. It is possible that REM sleep, a sleep stage that is both linked with normal emotional memory (Wagner et al., 2001, Hu et al., 2006) and disrupted in emotional disorders (Mellman, 2006, Peterson and Benca, 2006), may contribute to the normal development of emotionally guided decision making during adolescence. Should REM sleep influence development of the brain substrate of emotion regulation in adolescence, both IGT performance and success with lucidity training may vary with cross-sectional, individual differences in this developmental trajectory. It would be of considerable interest to compare, in adolescents, the ability to achieve lucidity with additional validated measures of emotion regulation and its interaction with decision making.
The present findings may also be interpreted in regard to meta-awareness, or self-consciousness, and its possible relationship to prefrontal cortical activity. Prior work implicates both dorsolateral and ventromedial prefrontal activity in lucid dreaming. Whereas dorsolateral prefrontal reactivation during lucid dreams may parallel activity during waking consciousness (Muzur et al. 2002, Hobson et al. 2000; Voss et al. 2009), greater intensity of activation within the anterior paralimbic REM activation area (i.e. including ventromedial prefrontal cortex; Nofzinger et al. 1997, 2004) during lucid dreams may spread within densely interconnected prefrontal areas (Petrides and Pandya, 2002) to an extent sufficient to trigger awareness of state without exceeding waking thresholds. Although the present results do not rule-out either possibility, we found that differences in performance on the ventromedial task but not the dorsolateral task were associated with ability to achieve lucidity. Although speculative, in as much as meta-awareness during dreams reflects the same phenomenon during wakefulness, and to the degree that the cognitive task performance reflects brain region functional differences, our data implicate differences in ventromedial function as potentially relevant to differences in the experience of meta-awareness.
Limitations of the present work are several. The lucid dream awareness protocol included lucid dream induction training that directly asked participants to try to have lucid dreams through self-suggestion among other techniques. This method introduced the possibility that participants would respond differently on measures of lucidity like the morning lucidity assessment based on how they reacted to the perceived experimenter demand. That is, some participants may have been more or less likely to report a greater degree of lucidity to respond positively or negatively to the perception that the experimenters wanted them to experience lucidity (i.e. the so called ‘good’ participant and ‘negative’ participant roles). Similar results from two distinct measures of lucidity decrease the likelihood that such experimenter demand influenced the results, but the possibility that IGT performance was differentiated on response to experimenter demands and not degree of lucidity cannot be ruled-out.
Polysomnographic sleep measurement was not done, so possible differences in objective sleep measures that could relate to lucidity or IGT performance are not known. Furthermore, an appropriate standard for the measurement of degree of lucidity was not available, with most extant measures of degree of lucidity designed to distinguish among very high degrees of lucidity. Hence the measure of lucidity employed in the present study was devised to have acceptable face validity to measure differences on the continuum between lucidity and non-lucidity, but was not previously validated nor meant to be an absolute measure of whether a lucid dream occurred. Nevertheless, the measure used in this study compared well to binary assessments of dream self-awareness and control present in dream reports, and analysis using dream reports as the basis for measuring lucidity or control produced similar results. The restriction of the study to high school student volunteers and in particular those from a high socio-economic class limits a broader interpretation of the findings. Nevertheless, the present findings show that a simple measure of degree of lucidity achieved during one week of a lucid dream awareness protocol can distinguish performance on a cognitive task engaging the VMPFC. Consequently, these results suggest possible connections both between the meta-awareness of lucid dreaming and VMPFC activity, and between the ability to have lucid dreams and VMPFC-related brain function, like emotion regulation.
Acknowledgments
This publication was made possible by CTSA Grant Number UL1 RR024139 from the National Center for Research Resources (NCRR), a component of the National Institutes of Health (NIH), and NIH roadmap for Medical Research. Its contents are solely the responsibility of the authors and do not necessarily represent the official view of NCRR or NIH. This work was also supported by the Yale University Department of Psychiatry, and the Connecticut Department of Mental Health and Addiction Services. Many thanks to Michael Inglis and Briarcliff High School for their support of the participation of M.N. in this work.
Appendices
A. Lucid Dreaming Awareness Protocol Instructions
Instructions
I will give you a dream journal in which to write all your dreams for the next 7 days. Keep the journal and a pen within reach of your bed, perhaps on a night table or under your pillow. Everytime you wake up from sleep, even in the middle of the night, write down everything that you dreamed as best as you can remember. Sometimes it is difficult to remember things in the beginning but it will get easier. Don't wait to write your dreams later as this does not work well.
Try to go to bed at the same time each night (within an hour). Make sure you have 8 hours to sleep each night or more. So if you have to wake up at 6:45am, make sure you are in bed by 10:45pm.
-
When you lie down to sleep (both the first time and each time after you wake up at night), spend a minute or two thinking about these things, telling them to yourself:
I am going to remember all of my dreams that I dream tonight
When I dream, I will know that I am dreaming
When I dream, I will be in control of my dreams, able to do what I want to
After I dream, I will wake up and write my dreams in my dream journal
Don't forget to write all of your dreams down as soon as you wake up and include descriptions of being aware that you were dreaming and/or being in control of dream if that happened.
B. Examples of Lucidity and/or Control from Dream Reports
Lucidity
1. “I was in an abandoned house, looked war-torn, but someone told me my dining room just collapsed in. I found 20 kids rushing in, and met [someone]. At this point I realize I'm dreaming. My house turns into a mall like area. We meet a girl named [name]…”
2. “I was at the mall with my friends and we were eating and shopping. The part where I had the lucid dream was I knew I was shopping in my dream. I knew I was in my bed and dreaming about what I was buying…”
Control
3. “I dream about playing baseball and that I was hitting the ball and could choose where the ball landed”
4. “More magazines. I controlled the ones I read. None about Jon and Kate. Magazines were all US Weekly or People”
Lucidity with Control of Direction of Dream
5. “Last night I had a dream that I was going to Cancun when all of a sudden I hit turbulence. The pilot put me in the cockpit and had me control the plane. I wasn't sure what I was doing and I was so confused as to what was going on. I knew in my dream that I was dreaming and I was able to control some aspects of my dream and I was able to land the plane successfully.”
6. “I was playing soccer with girls from school and it was the State Championship and we were tied and I knew I was dreaming. I was dribbling the ball down the field and made the decision to pass and not score. we won ☺”
Lucid Control of Content of Dream
7. “I did dream about summer which I wanted to. What I remember is dropping off my neighbor since I guess I [illegible]. I called her back and told her something which I feel I controlled. This was very obvious to be a dream”.
8. “Before going to sleep I kept telling myself that I was going to dream about roller coasters and I did. I dreamt that I was riding on Kingda Ka and I kept controlling where I wanted to sit on the ride”
C. Assessments
| Subject #______________ | Date:_________________ |
Baseline Lucidity Assessment
Instruction: Consider the past year in answering the following questions about your dreaming. Please circle your answers.
-
I can usually remember my dreams.
1 2 3 4 5 Strongly Agree Strongly Disagree -
My dreams have a lot of detail that I can often remember.
1 2 3 4 5 Strongly Agree Strongly Disagree -
Sometimes I can tell that I am dreaming during a dream.
1 2 3 4 5 Strongly Agree Strongly Disagree -
Sometimes I can control what happens in my dreams.
1 2 3 4 5 Strongly Agree Strongly Disagree -
Sometimes I can dream about things that I have decided I want to dream about.
1 2 3 4 5 Strongly Agree Strongly Disagree Subject #______________ Date:_________________
Morning Lucidity Assessment
Instruction: Consider the past night in answering the following questions about your dreaming. Please circle your answers.
-
It was easy to remember my dreams.
1 2 3 4 5 Strongly Agree Strongly Disagree -
I could recall most or all of the detail in my dreams.
1 2 3 4 5 Strongly Agree Strongly Disagree -
I thought or knew that I was dreaming during my dreams.
1 2 3 4 5 Strongly Agree Strongly Disagree -
I was able to control some or all of what happened in my dreams.
1 2 3 4 5 Strongly Agree Strongly Disagree -
I dreamed about things I had decided I wanted to dream about.
1 2 3 4 5 Strongly Agree Strongly Disagree
Footnotes
CoI: None of the authors has any conflicts of interest to disclose.
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- Abe T, Ogawa K, Nittono H, Hori T. Neural generators of brain potentials before rapid eye movements during human REM sleep: A study using sLORETA. Clin Neurophysiol. 2008;119:2044–53. doi: 10.1016/j.clinph.2008.05.008. [DOI] [PubMed] [Google Scholar]
- Armstrong-Hickey DA. Validation of Lucid Dreaming in School Age Children. Lucidity Letter. 1988;7:35–38. [Google Scholar]
- Barrett D. Just how lucid are lucid dreams? Dreaming. 1992;2:221–28. [Google Scholar]
- Bechara A, Damasio AR, Damasio H, Anderson SW. Insensitivity to future consequences following damage to human prefrontal cortex. Cognition. 1994;50:7–15. doi: 10.1016/0010-0277(94)90018-3. [DOI] [PubMed] [Google Scholar]
- Bechara A, Damasio H, Damasio AR. Emotion, decision making and the orbitofrontal cortex. Cereb Cortex. 2000;10:295–307. doi: 10.1093/cercor/10.3.295. [DOI] [PubMed] [Google Scholar]
- Bechara A, Damasio H, Damasio AR, Lee GP. Different contributions of the human amygdala and ventromedial prefrontal cortex to decision-making. J Neurosci. 1999;19:5473–81. doi: 10.1523/JNEUROSCI.19-13-05473.1999. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bechara A, Damasio H, Tranel D, Damasio AR. Deciding advantageously before knowing the advantageous strategy. Science. 1997;275:1293–5. doi: 10.1126/science.275.5304.1293. [DOI] [PubMed] [Google Scholar]
- Bechara A, Tranel D, Damasio H. Characterization of the decision-making deficit of patients with ventromedial prefrontal cortex lesions. Brain. 2000b;123(Pt 11):2189–202. doi: 10.1093/brain/123.11.2189. [DOI] [PubMed] [Google Scholar]
- Berg EA. A simple objective technique for measuring flexibility in thinking. J Gen Psychol. 1948;39:15–22. doi: 10.1080/00221309.1948.9918159. [DOI] [PubMed] [Google Scholar]
- Braun AR, Balkin TJ, Wesensten NJ, et al. Dissociated pattern of activity in visual cortices and their projections during human rapid eye movement sleep. J Clin Sleep Med Science. 1998;279:91–5. doi: 10.1126/science.279.5347.91. [DOI] [PubMed] [Google Scholar]
- Braun AR, Balkin TJ, Wesenten NJ, et al. Regional cerebral blood flow throughout the sleep-wake cycle. An H2(15)O PET study. Brain. 1997;120(Pt 7):1173–97. doi: 10.1093/brain/120.7.1173. [DOI] [PubMed] [Google Scholar]
- Brylowski A, Levitan L, Laberge S. H-reflex suppression and autonomic activation during lucid REM sleep: a case study. Sleep. 1989;12:374–8. doi: 10.1093/sleep/12.4.374. [DOI] [PubMed] [Google Scholar]
- Buysse DJ, Hall ML, Strollo PJ, et al. Relationships between the Pittsburgh Sleep Quality Index (PSQI), Epworth Sleepiness Scale (ESS), and clinical/polysomnographic measures in a community sample. 2008;4:563–71. [PMC free article] [PubMed] [Google Scholar]
- Buysse DJ, Reynolds CF, 3rd, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28:193–213. doi: 10.1016/0165-1781(89)90047-4. [DOI] [PubMed] [Google Scholar]
- Cicogna PC, Bosinelli M. Consciousness during dreams. Conscious Cogn. 2001;10:26–41. doi: 10.1006/ccog.2000.0471. [DOI] [PubMed] [Google Scholar]
- Corsi-Cabrera M, Guevara MA, Del Rio-Portilla Y. Brain activity and temporal coupling related to eye movements during REM sleep: EEG and MEG results. Brain Res. 2008 doi: 10.1016/j.brainres.2008.06.052. [DOI] [PubMed] [Google Scholar]
- Damasio A. Feelings of emotion and the self. Ann N Y Acad Sci. 2003;1001:253–61. doi: 10.1196/annals.1279.014. [DOI] [PubMed] [Google Scholar]
- Ellis BW, Johns MW, Lancaster R, Raptopoulos P, Angelopoulos N, Priest RG. The St. Mary's Hospital sleep questionnaire: a study of reliability. Sleep. 1981;4:93–7. doi: 10.1093/sleep/4.1.93. [DOI] [PubMed] [Google Scholar]
- Foulkes WD. Dream reports from different stages of sleep. Journal of abnormal and social psychology. 1962;65:14–25. doi: 10.1037/h0040431. [DOI] [PubMed] [Google Scholar]
- Frith CD, Frith U. The neural basis of mentalizing. Neuron. 2006;50:531–4. doi: 10.1016/j.neuron.2006.05.001. [DOI] [PubMed] [Google Scholar]
- Hobson JA. Basic Books. New York: 1988. The Dreaming Brain. [Google Scholar]
- Hobson JA, Pace-Schott EF, Stickgold R. Dreaming and the brain: toward a cognitive neuroscience of conscious states. Behav. Brain Sci. 2000;23:793–842. doi: 10.1017/s0140525x00003976. discussion 904-1121. [DOI] [PubMed] [Google Scholar]
- Hooper CJ, Luciana M, Conklin HM, Yarger RS. Adolescents' performance on the Iowa Gambling Task: implications for the development of decision making and ventromedial prefrontal cortex. Dev Psychol. 2004;40:1148–58. doi: 10.1037/0012-1649.40.6.1148. [DOI] [PubMed] [Google Scholar]
- Hu P, Stylos-Allan M, Walker MP. Sleep facilitates consolidation of emotional declarative memory. Psychol Sci. 2006;17:891–8. doi: 10.1111/j.1467-9280.2006.01799.x. [DOI] [PubMed] [Google Scholar]
- Kahan TL, Laberge S. Lucid dreaming as metacognition: Implications for cognitive science. Conscious Cogn. 1994;3:246–64. [Google Scholar]
- Kahan TL, Laberge S, Levitan L, Zimbardo P. Similarities and differences between dreaming and waking cognition: an exploratory study. Conscious Cogn. 1997;6:132–47. doi: 10.1006/ccog.1996.0274. [DOI] [PubMed] [Google Scholar]
- Kahn D, Hobson JA. Theory of Mind in Dreaming: Awareness of Feelings and Thoughts of Others in Dreams. Dreaming. 2005;15:48–57. [Google Scholar]
- Ko JH, Monchi O, Ptito A, Petrides M, Strafella AP. Repetitive Transcranial Magnetic Stimulation of Dorsolateral Prefrontal Cortex Affects Performance of the Wisconsin Card Sorting Task during Provision of Feedback. International journal of biomedical imaging. 2008:143–238. doi: 10.1155/2008/143238. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kringelbach ML. The human orbitofrontal cortex: linking reward to hedonic experience. Nature reviews. 2005;6:691–702. doi: 10.1038/nrn1747. [DOI] [PubMed] [Google Scholar]
- Kringelbach ML, Rolls ET. The functional neuroanatomy of the human orbitofrontal cortex: evidence from neuroimaging and neuropsychology. Prog Neurobiol. 2004;72:341–72. doi: 10.1016/j.pneurobio.2004.03.006. [DOI] [PubMed] [Google Scholar]
- Laberge S. Lucid dreaming: Psychophysiological studies of consciousness during REM sleep. In: Bootzin R, Kihlstrom J, Schacter D, editors. Sleep and cognition American Psychological Association. 1990. [Google Scholar]
- Laberge S. Physiological studies of lucid dreaming. In: Antrobus J, Bertini M, editors. The neuropsychology of dreaming sleep. Lawrence Erlbaum Associates; 1992. [Google Scholar]
- Laberge S. Lucid dreaming: Evidence and methodology. Behav Brain Sci. 2000;23:962–64. [Google Scholar]
- Laberge S. Lucid dreaming. In: Barrett D, Mcnamara P, editors. The New Science of Dreaming. Praeger, Greenwood Press; Westport, CT: 2007. [Google Scholar]
- Laberge S, Nagel L, Dement WC, Zarcone V., Jr Lucid dreaming verified by volitional communication during REM sleep. Percept Mot Skills. 1981;52:727–32. doi: 10.2466/pms.1981.52.3.727. [DOI] [PubMed] [Google Scholar]
- Lawrence NS, Jollant F, O'daly O, Zelaya F, Phillips ML. Distinct roles of prefrontal cortical subregions in the Iowa Gambling Task. Cereb Cortex. 2009;19:1134–43. doi: 10.1093/cercor/bhn154. [DOI] [PubMed] [Google Scholar]
- Leigh TJ, Bird HA, Hindmarch I, Constable PD, Wright V. Factor analysis of the St. Mary's Hospital Sleep Questionnaire. Sleep. 1988;11:448–53. doi: 10.1093/sleep/11.5.448. [DOI] [PubMed] [Google Scholar]
- Lequerica A. Lucid dreaming and the mind-body relationship: a model for the cognitive and physiological variations in rapid eye movement sleep. Percept Mot Skills. 1996;83:331–6. doi: 10.2466/pms.1996.83.1.331. [DOI] [PubMed] [Google Scholar]
- Lezak MD, Howieson DB, Loring D. Neuropsychological Assessment. Fourth Edition. Oxford University Press; New York, NY: 2004. [Google Scholar]
- Li X, Lu ZL, D'argembeau A, Ng M, Bechara A. The Iowa Gambling Task in fMRI images. Hum. Brain Mapp. 2009 doi: 10.1002/hbm.20875. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lin CH, Chiu YC, Cheng CM, Hsieh JC. Brain maps of Iowa gambling task. BMC neuroscience. 2008;9:72. doi: 10.1186/1471-2202-9-72. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Macnamara P, Mclaren A, Wowalczyk S, Pace-Schott EF. “Theory of Mind” in REM and NREM dreams. In: Barrett D, Mcnamara P, editors. The New Science of Dreaming. Praeger, Greenwood Press; Westport, CT: 2007. [Google Scholar]
- Maquet P, Peters J, Aerts J, et al. Functional neuroanatomy of human rapid-eye-movement sleep and dreaming. Nature. 1996;383:163–6. doi: 10.1038/383163a0. [DOI] [PubMed] [Google Scholar]
- Maquet P, Ruby P, Maudoux A, et al. Human cognition during REM sleep and the activity profile within frontal and parietal cortices: a reappraisal of functional neuroimaging data. Prog. Brain Res. 2005;150:219–27. doi: 10.1016/S0079-6123(05)50016-5. [DOI] [PubMed] [Google Scholar]
- Mellman TA. Sleep and anxiety disorders. Psychiatr Clin North Am. 2006;29:1047–58. doi: 10.1016/j.psc.2006.08.005. abstract x. [DOI] [PubMed] [Google Scholar]
- Miyauchi S, Misaki M, Kan S, Fukunaga T, Koike T. Human brain activity time-locked to rapid eye movements during REM sleep. Exp Brain Res. 2009;192:657–67. doi: 10.1007/s00221-008-1579-2. [DOI] [PubMed] [Google Scholar]
- Monchi O, Petrides M, Petre V, Worsley K, Dagher A. Wisconsin Card Sorting revisited: distinct neural circuits participating in different stages of the task identified by event-related functional magnetic resonance imaging. J Neurosci. 2001;21:7733–41. doi: 10.1523/JNEUROSCI.21-19-07733.2001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Muzur A, Pace-Schott EF, Hobson JA. The prefrontal cortex in sleep. Trends in cognitive sciences. 2002;6:475–81. doi: 10.1016/s1364-6613(02)01992-7. [DOI] [PubMed] [Google Scholar]
- Nielsen TA. A review of mentation in REM and NREM sleep: “covert” REM sleep as a possible reconciliation of two opposing models. Behav Brain Sci. 2000;23:851–66. doi: 10.1017/s0140525x0000399x. discussion 904-1121. [DOI] [PubMed] [Google Scholar]
- Nofzinger EA, Buysse DJ, Germain A, Carter C, Luna B, Price JC, Meltzer CC, Miewald JM, Reynolds CF, 3rd, Kupfer DJ. Increased activation of anterior paralimbic and executive cortex from waking to rapid eye movement sleep in depression. Arch Gen Psychiatry. 2004;61:695–702. doi: 10.1001/archpsyc.61.7.695. [DOI] [PubMed] [Google Scholar]
- Nofzinger EA, Mintun MA, Wiseman M, Kupfer DJ, Moore RY. Forebrain activation in REM sleep: an FDG PET study. Brain Res. 1997;770:192–201. doi: 10.1016/s0006-8993(97)00807-x. [DOI] [PubMed] [Google Scholar]
- Pace-Schott EF. “Theory of Mind,” Social Cognition and Dreaming. Sleep Research Society Bulletin. 2001;7:33–36. [Google Scholar]
- Pace-Schott EF. Complex hallucinations in waking suggest mechanisms of dream construction, Commentary on: Why people see things that are not there: A novel perception and attention deficit model for recurrent complex visual hallucinations by D. Collerton, E. Perry & I. McKeith. Behav. Brain Sci. 2005;28:771–72. doi: 10.1017/S0140525X05000130. [DOI] [PubMed] [Google Scholar]
- Pace-Schott EF. The Neurobiology of Dreaming. In: Kryger MH, Roth T, Dement WC, editors. Principles and Practice of Sleep Medicine 5th Edition. Elsevier; Philadelphia: 2009. [Google Scholar]
- Peterson MJ, Benca RM. Sleep in mood disorders. Psychiatr Clin North Am. 2006;29:1009–32. doi: 10.1016/j.psc.2006.09.003. abstract ix. [DOI] [PubMed] [Google Scholar]
- Petrides M, Pandya DN. Association pathways of the prefrontal cortex and functional observations. In: Stuss DT, Knight RT, editors. Principles of Frontal Lobe Function. Oxford University Press; New York: 2002. [Google Scholar]
- Purcell S, Mullington J, Moffitt A, Hoffmann R, Pigeau R. Dream self-reflectiveness as a learned cognitive skill. Sleep. 1986;9:423–37. doi: 10.1093/sleep/9.3.423. [DOI] [PubMed] [Google Scholar]
- Rechtschaffen A. The single-mindedness and isolation of dreams. Sleep. 1978;1:97–109. doi: 10.1093/sleep/1.1.97. [DOI] [PubMed] [Google Scholar]
- Stuss DT, Alexander MP, Floden D, et al. Fractionalization and localization of distinct frontal lobe processes: Evidence from focal lesions in humans. In: Stuss DT, Knight RT, editors. Principles of Frontal Lobe Function. Oxford University Press; New York: 2002. [Google Scholar]
- Tamnes CK, Ostby Y, Fjell AM, Westlye LT, Due-Tonnessen P, Walhovd KB. Brain Maturation in Adolescence and Young Adulthood: Regional Age-Related Changes in Cortical Thickness and White Matter Volume and Microstructure. Cereb Cortex. 2009 doi: 10.1093/cercor/bhp118. [DOI] [PubMed] [Google Scholar]
- Voss U, Holzmann R, Tuin I, Hobson JA. Lucid dreaming: a state of consciousness with features of both waking and non-lucid dreaming. Sleep. 2009;32:1191–200. doi: 10.1093/sleep/32.9.1191. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wagar BM, Dixon M. Affective guidance in the Iowa gambling task. Cognitive, affective & behavioral neuroscience. 2006;6:277–90. doi: 10.3758/cabn.6.4.277. [DOI] [PubMed] [Google Scholar]
- Wagner U, Gais S, Born J. Emotional memory formation is enhanced across sleep intervals with high amounts of rapid eye movement sleep. Learn Mem. 2001;8:112–9. doi: 10.1101/lm.36801. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wehrle R, Kaufmann C, Wetter TC, et al. Functional microstates within human REM sleep: first evidence from fMRI of a thalamocortical network specific for phasic REM periods. Eur J Neurosci. 2007;25:863–71. doi: 10.1111/j.1460-9568.2007.05314.x. [DOI] [PubMed] [Google Scholar]
- Whittle S, Yap MB, Yucel M, et al. Prefrontal and amygdala volumes are related to adolescents' affective behaviors during parent-adolescent interactions. Proc Natl Acad Sci U S A. 2008;105:3652–7. doi: 10.1073/pnas.0709815105. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yurgelun-Todd DA, Killgore WD. Fear-related activity in the prefrontal cortex increases with age during adolescence: a preliminary fMRI study. Neurosci Lett. 2006;406:194–9. doi: 10.1016/j.neulet.2006.07.046. [DOI] [PubMed] [Google Scholar]