

Abstract
A young mountaineer suffered from sudden cardiac arrest at high altitude. Cardiopulmonary resuscitation was initiated immediately. After 30 min a rescue team arrived and successfully defibrillated ventricular fibrillation upon which spontaneous circulation returned. The subsequent ECG was suggestive of extensive anterior myocardial infarction. Therefore, the patient was thrombolysed and transferred for primary percutaneous coronary intervention. Echocardiography revealed severely reduced left ventricular function with antero-septo-apical akinesia. However, angiography showed unobstructed coronary arteries. The patient fully recovered and left ventricular function normalised within 2 weeks. It may be speculated that exposure to high altitude resulted in acute coronary thrombosis which dissolved by rapid thrombolysis.
Background
Sudden cardiac arrest in young athletes is a rare condition. The most common causes are hypertrophic cardiomyopathy, arrhythmogenic right ventricular dysplasia and coronary anomalies.1 In this regard, acute myocardial infarction combined with normal coronary angiography is a rather surprising finding, as some form of abnormality is usually found in the majority of the cases, that is, luminal narrowings, thrombosis, dissections, spasms or muscle bridges. In acute myocardial infarction, the time to reperfusion determines myocardial salvage and mortality.2 3 The present case underlines that rapid thrombolysis within the golden hour may result in excellent outcome, given that the individual was young and previously healthy.
Case presentation
A 23-year-old mountaineer, used to high altitude, climbed one of the highest summits in the Alps (4556 m). Back in the bivouac (approx. 3200 m) he realised the loss of his gas bottle and, therefore, further descended to a mountain hut (2795 m), where he collapsed 10 min after arrival while sitting in a chair. Two anaesthesiologists, fellow mountaineers, diagnosed pulse-less cardiac arrest and initiated cardiopulmonary resuscitation. After 30 min, a mountain rescue team arrived by helicopter and obtained a 12-lead ECG showing ventricular fibrillation, which was successfully defibrillated into sinus rhythm whereupon spontaneous circulation returned. Extensive anterior myocardial infarction was suspected due to ST-segment elevation in V1-5 (figure 1). Therefore, the patient was thrombolysed (reteplase) and flown to our hospital centre for primary angioplasty. Echocardiogram showed severely reduced left ventricular ejection fraction (EF 25–30%) with akinesia of the anterior and septal wall without significant valvulopathy. And 2.5 h after onset of cardiac arrest, coronary angiography revealed normal coronary arteries without narrowings or dissection.
Figure 1.
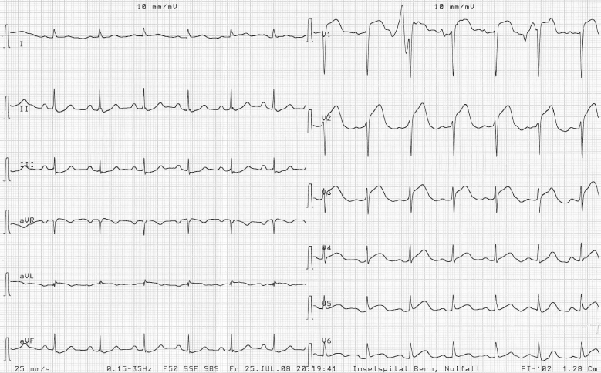
ECG at presentation to the emergency room. Significant ST-segment elevation in V1-5 and ST-segment depression in II, III, aVF.
Cardiac serum markers suggested extensive myocardial necrosis with maximal creatine kinase of 15 674 U/l (myocardial fraction 737 μg/l) and maximal troponin T of 7.87 μg/l. Ten days after cardiac arrest, an ECG (figure 2) showed regredient but still significant ST-segment elevation in V1-3 and negative T waves in V1-6, suggesting the sequel of extensive anterior myocardial infarction with subsequent aneurysm formation. However, left ventricular function gradually increased and was 35% and 65% after 1 and 2 weeks, respectively, without regional wall-motion abnormalities. Cardiac magnetic resonance was performed after 3 weeks to rule out cardiomyopathy. The scan was found to be normal and remarkably without scar.
Figure 2.
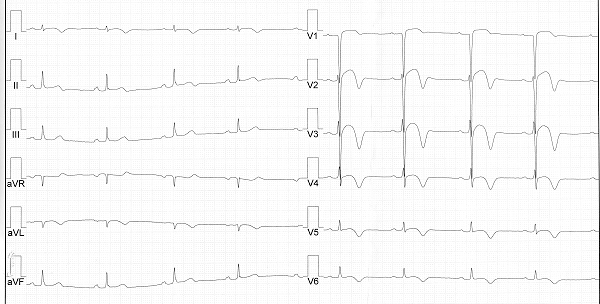
ECG 10 days after cardiac arrest. Regredient ST-segment elevation remaining significant in V1-3 and discordant, negative T waves in V1-6, I, II.
Ventricular biopsy was performed to rule out inflammatory, infiltrative or degenerative causes. The former causes and in particular peri- and myo-carditis were further ruled out with a normal cardiac magnetic resonance scan.
Electrophysiological causes, for example, abnormal conduction system or repolarisation, could not be substantiated by ECG findings. In order to rule out cardiac or paradoxical embolism a trans-oesophageal echocardiogram was performed which was normal.
A cardioverter-defibrillator was implanted for secondary prevention because an arrhythmogenetic cause could not be excluded entirely. One month after the cardiac arrest, the young mountaineer was discharged in good condition. Ironically, a lost gas bottle and the subsequent descent to a mountain hut saved his life.
Discussion
The presented case of a previously healthy young mountaineer who suffered acute myocardial infarction complicated by sudden cardiac arrest is special mainly for two reasons.
First, acute myocardial infarction in the setting of normal coronary arteries is exceedingly rare.2 It is well known that heavy physical exercise may trigger acute myocardial infarction.4 In the first hour after the onset of vigorous exercise, the risk of acute myocardial infarction was found to be particularly high. However, this risks decreases in individuals engaged in regular exercise. The risk of coronary thrombosis is increased in individuals exposed to high altitude for a prolonged time due to the induction of a hypercoagulable state:5 hypobaric hypoxia leads to erythrocytosis, increased platelet count and platelet activation, raised fibrinogen and decreased fibrinolytic activity due to increased plasminogen activator inhibitor-1. In our patient, coronary thrombosis was dissolved by thrombolysis and probably by cardiopulmonary reanimation (CPR). In fact, the cause of this catastrophic event in this young and fit mountaineer remains unclear.
Second, the clinical outcome is remarkable in our patient with normalisation of left ventricular function within 2 weeks. In most patients with acute myocardial infarction undergoing reperfusion therapy, either thrombolysis or catheter-based therapy, left ventricular function increases steadily over months and normalisation was only rarely found.6 7 The excellent outcome in our case may be explained by immediate professional CPR, successful defibrillation and rapid thrombolysis aided by the fact that the patient was young and previously healthy.
We found only two cases describing acute myocardial infarction in athletes with normal coronary arteries. Hutchison et al8 described a case of 29-year-old mountaineer who suffered acute inferior myocardial infarction in the Himalayas. However, the patient may have suffered from premature coronary artery disease as he had an episode of similar chest pain before. He was conservatively managed due to the lack of reperfusion therapy and did not fully recover.
In this journal, Whyte et al9 reported a case of 46-year-old recreational athlete who suffered acute myocardial infarction in the presence of normal coronary arteries and without any risk factors. Coronary angiogram was performed more than 3 h after onset of chest pain and revealed a thrombus in the mid-right coronary artery. Systolic left ventricular function was assessed after reperfusion and was found to be normal.
Learning points.
Immediate CPR, followed by rapid reperfusion, determines the outcome in patients with acute myocardial infarction. However, full recovery after 30 min of CPR and subsequent successful defibrillation is unusual.
Exposure to high altitude may induce a hypercoagulable state triggering arteriolar thrombosis.
Footnotes
Competing interests None.
Patient consent Obtained.
References
- 1.Maron BJ, Doerer JJ, Haas TS, et al. Sudden deaths in young competitive athletes: analysis of 1866 deaths in the United States, 1980-2006. Circulation 2009;119:1085–92 [DOI] [PubMed] [Google Scholar]
- 2.Widimsky P, Stellova B, Groch L, et al. ; PRAGUE Study Group Investigators Prevalence of normal coronary angiography in the acute phase of suspected ST-elevation myocardial infarction: experience from the PRAGUE studies. Can J Cardiol 2006;22:1147–52 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Da Costa A, Isaaz K, Faure E, et al. Clinical characteristics, aetiological factors and long-term prognosis of myocardial infarction with an absolutely normal coronary angiogram; a 3-year follow-up study of 91 patients. Eur Heart J 2001;22:1459–65 [DOI] [PubMed] [Google Scholar]
- 4.Mittleman MA, Maclure M, Tofler GH, et al. Triggering of acute myocardial infarction by heavy physical exertion. Protection against triggering by regular exertion. Determinants of Myocardial Infarction Onset Study Investigators. N Engl J Med 1993;329:1677–83 [DOI] [PubMed] [Google Scholar]
- 5.Kotwal J, Apte CV, Kotwal A, et al. High altitude: a hypercoagulable state: results of a prospective cohort study. Thromb Res 2007;120:391–7 [DOI] [PubMed] [Google Scholar]
- 6.Sheehan FH, Doerr R, Schmidt WG, et al. Early recovery of left ventricular function after thrombolytic therapy for acute myocardial infarction: an important determinant of survival. J Am Coll Cardiol 1988;12:289–300 [DOI] [PubMed] [Google Scholar]
- 7.Ottervanger JP, van ‘t Hof AW, Reiffers S, et al. Long-term recovery of left ventricular function after primary angioplasty for acute myocardial infarction. Eur Heart J 2001;22:785–90 [DOI] [PubMed] [Google Scholar]
- 8.Hutchison SJ, Litch JA. Acute myocardial infarction at high altitude. JAMA 1997;278:1661–2 [DOI] [PubMed] [Google Scholar]
- 9.Whyte G, Godfrey R, O'Hanlon R, et al. Acute myocardial infarction in the presence of normal coronaries and the absence of risk factors in a young, lifelong regular exerciser. BMJ Case Reports 2009 [DOI] [PMC free article] [PubMed] [Google Scholar]