

Abstract
A 57-year-old man presented at our institution with central chest pain. Serial ECGs showed dynamic T-wave changes, suggesting the possibility of unstable angina. Urgent coronary angiography revealed an unexpected finding of a radio-opaque lesion seen in the xiphisternal region during screening. Oesophogastroduodenoscopy confirmed this to be a 10p coin. The coin passed through the gastrointestinal tract without complications and the patient's symptoms and ECG changes resolved. This unusual case is a reminder that many diseases may electrocardiographically imitate an acute coronary syndrome.
Background
This case is an important reminder that oesophageal disorders are well recognised non-cardiac causes of chest pain and demonstrates that oesophageal stimulation (in this case by a foreign body) can mimic acute coronary syndrome (ACS) clinically as well as electrocardiographically. The cardio-oesophageal reflex, which is not well known, is also discussed. The other interesting feature and learning point from this case is the missed radio-opaque lesion on the admission chest radiograph, which is more apparent on alteration of the exposure electronically.
Case presentation
A 57-year-old man was admitted with chest pain which he described as though something was ”stuck” in his “gullet”. Serial ECGs demonstrated dynamic infero-lateral T-wave changes, more prominent with pain (figure 1). The admission chest radiograph was reported as normal. He was given aspirin, clopidogrel, clexane and tirofiban and transferred to the coronary care unit.
Figure 1.
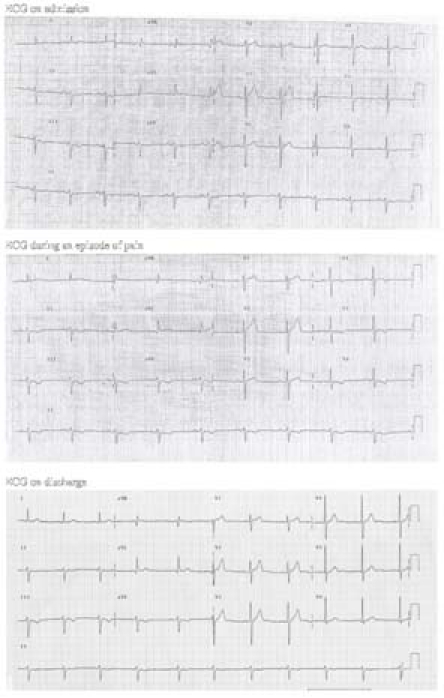
Electrocardiographic changes with pain.
Troponin levels were normal. Following further episodes of chest pain, coronary angiography was undertaken. A radio-opaque lesion was seen in the xiphisternal region during screening. The coronary arteries were normal. The patient therefore had an oesophogastroduodenoscopy, which revealed a 10p coin in the gastric fundus (figure 2).
Figure 2.
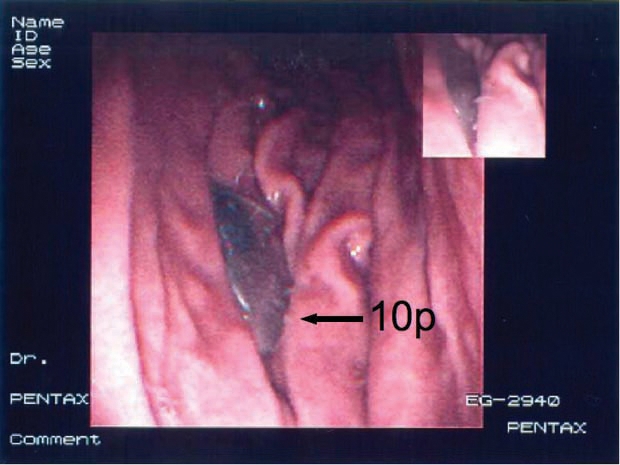
Oesophogastroduodenoscopy revealed a 10p coin.
Outcome and follow-up
The coin progressed through the gastrointestinal tract and the patient was discharged 2 days later. His symptoms and electrocardiographic changes resolved. A retrospective review of his chest radiograph (with the exposure altered electronically) revealed the 10p coin (figure 3). The patient had no recollection of swallowing a coin.
Figure 3.
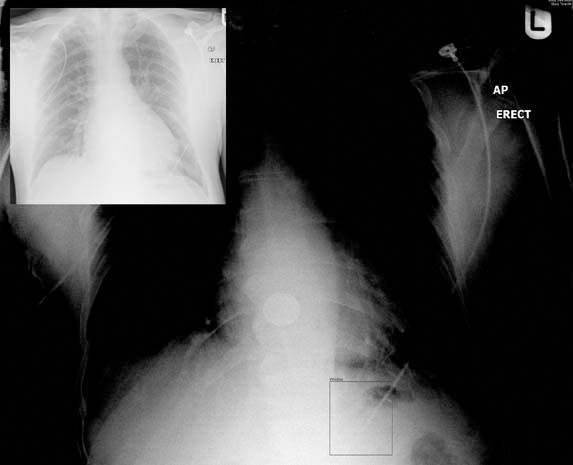
Inset: chest radiograph on admission. Main: radiograph with altered exposure revealing an opacity.
Discussion
Oesophageal disorders are well recognised non-cardiac causes of chest pain. As in this case, they may be associated with electrocardiographic changes. This phenomenon could be caused by a neurally mediated process, direct physical stimulation or a combination of both. Oesophageal acid stimulation has been shown to reduce coronary artery blood flow, producing angina-like symptoms and ECG changes.1 This is called the cardio-oesophageal reflex. Direct cardiac compression from external structures, such as a gastric tube following oesophageal reconstruction, has also been shown to induce reversible ST-T abnormalities.2 There are also a few isolated case reports in the literature of ischaemic ECG changes in patients with acute pancreatitis, acute cholecystitis and pneumonia.3 4 5
This unusual case is a reminder that many diseases may electrocardiographically imitate an ACS.
Learning points.
-
▶
Oesophageal disorders are well recognised non-cardiac causes of chest pain and can mimic an acute coronary syndrome clinically, with electrocardiographic changes, and should be considered as part of the differential diagnosis.
-
▶
The cardio-oesophageal reflex is the name for this phenomenon where a neurally mediated process or direct oesophageal stimulation produces angina-like symptoms and electrocardiographic changes.
-
▶
Altering the exposure of electronically available chest radiographs may reveal an unexpected lesion behind the heart.
Footnotes
Competing interests None.
Patient consent Obtained.
References
- 1.Chauhan A, Petch MC, Schofield PM. Cardio-oesophageal reflex in humans as a mechanism for ‘linked-angina’. Eur Heart J 1996;17:407–13 [DOI] [PubMed] [Google Scholar]
- 2.Takato T, Ashida T, Sugiyama T, et al. Marked reversible ST-T abnormalities induced by cardiac compression from a retrosternal gastric tube used to reconstruct the oesophagus after tumour resection. A case of a diabetic patient and mini-review of 7 reported patients. Int Heart J 2006;47:475–82 [DOI] [PubMed] [Google Scholar]
- 3.Patel J, Movahed A, Reeves WC. Electrocardiographic and segmental wall motion abnormalities in pancreatitis mimicking myocardial infarction. Clin Cardiol 1995;18:58. [DOI] [PubMed] [Google Scholar]
- 4.Krasna MJ, Flancbaum L. Electrocardiographic changes in cardiac patients with acute gallbladder disease. Am Surg 1986;52:541–3 [PubMed] [Google Scholar]
- 5.Dickerman JL. Electrocardiographic changes in acute cholecystitis. J Am Osteopath Assoc 1989;89:630–5 [PubMed] [Google Scholar]