

Abstract
A 20-year-old woman who was fit and well presented with a history of left nasal blockage for 2 years. She was noted on anterior rhinoscopy to have nasal septal deviation towards the left. She was listed for septoplasty with the aim of relieving nasal obstruction. At operation she was found to have a mildly deviated septum to the left. There was also a rhinolith in the left nostril posterior to the deviated septum (figure 1). Following removal of the rhinolith, her nasal airway appeared adequate; hence, septoplasty was not performed. Postoperatively, the patient was pleased with the outcome. When the patient was shown the foreign body she recalled inserting a pen cover into her nose about 10 years previously (figure 2). When she presented to the Accident and Emergency department at that time she was told that there was no foreign body in her nose.
Figure 1.

Endoscopic view of rhinolith.
Figure 2.
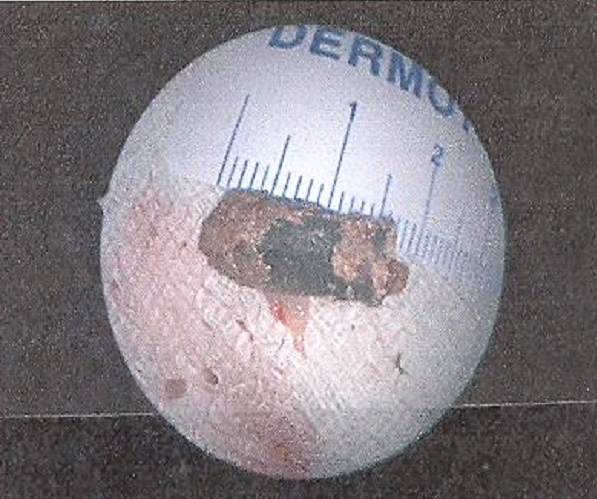
Rhinolith.
Background
This case demonstrates that performing endoscopy in clinic may have identified the foreign body. This would then have changed the management plan from surgery to correct nasal septal deviation to removal of foreign body, which can be performed under local anaesthesia.
Case presentation
A 20-year-old woman who was fit and well presented with a history of left nasal blockage for 2 years. She also complained of nasal discharge from the same side with occasional bleeding. She had been given a variety of steroid nasal sprays, which had minimal effect.
There was no history of any significant drug allergies, eczema, hay fever or asthma.
When she presented she was noted on anterior rhinoscopy that the nasal septum was deviated to the left with the presence of clear nasal discharge on the floor of the nose. There were no polyps seen. Endoscopic examination of the nose was not undertaken.
Differential diagnosis
Deviated nasal septum; nasal polyps; rhinitis; foreign body (in retrospect); hypertrophic turbinate bones; large adenoids; sarcoidosis; overuse of nose sprays (rhinitis medicamentosa); contraceptive pills.
Treatment
The planned treatment was septoplasty. When the nose was inspected under general anaesthesia in the operating theatre it became clear that there was a foreign body mass in the left nasal cavity posterior to the septal deviation. The nasal obstruction was relieved by removal of the foreign body. The adjacent mucosa was noted to be polypoid and a biopsy of this was taken. After removal of the mass her nasal airway was assessed to be adequate and septoplasty was not performed.
Outcome and follow-up
After removal of the mass it was identified as a rhinolith. On sectioning there was a black plastic object in the centre of the rhinolith and on closer inspection this resembled the cover of a disposable pen. Histology of the nasal mucosa showed benign inflammatory changes only.
Postoperatively, when the patient was shown the foreign body she remembered inserting a pen cover into her nose about 10 years previously. When she presented to the Accident and Emergency department at that time she was told that there was no foreign body in her nose.
Following the removal of the rhinolith the patient was pleased with the outcome and was discharged from ear, nose and throat care.
Discussion
A rhinolith is an object that has become lodged in the nose and has slowly calcified.1
Bartholin first identified rhinoliths in 1654. Since then, over 600 cases have been reported in literature. Their incidence is 1 in every 10 000 otolaryngology outpatients.2
Rhinoliths are rare and can have various clinical presentations. A high index of suspicion is required for the diagnosis of such a forgotten entity.3
Rhinolithiasis should be suspected in every case with unilateral, foul-smelling rhinorrhoea and nasal obstruction.4 Sometimes they may cause complications, such as unilateral nasal obstruction, fetid rhinorrhoea or epistaxis.5 Chronic nasal discharge without a history of rhinologic disease requires an endonasal examination under good conditions after retraction.6
This case illustrates that it is appropriate to perform endoscopy of the nasal cavities to investigate nasal obstruction before proceeding to surgery. The nasal bleeding and obstruction of 2 years’ duration experienced by this patient did not correlate with the extent of nasal septal deviation. Symptoms were severe enough for her to request referral to a specialist. If endoscopy had been performed, a general anaesthesia may have been avoided. However, based on previous experience, this may not always be the case as a rhinolith can be difficult to remove in clinic due to pain and possibly bleeding especially if it is posterior to a septal deviation.
All patients presenting for a specialist opinion for nasal obstruction should be seen by clinicians with access to flexible and rigid endoscopes in the out-patient department. This case illustrates the need to consider causes for nasal symptoms throughout the nasal cavity despite the presence of abnormalities anteriorly. Literature search did not show any other similar publications.
Learning points.
If the presenting nasal symptoms do not completely correlate with the clinical findings nasal endoscopy should be performed to ensure that another abnormality is not missed.
Full examination of the nose is likely to ensure that unusual pathology is not missed and allow appropriate treatment planning and patient counselling.
Although rhinolith is a rare condition, it should not be forgotten as a cause for nasal obstruction.
Footnotes
Competing interests None.
Patient consent Obtained.
References
- 1.Appleton SS, Kimbrough RE, Engstrom HI. Rhinolithiasis: a review. Oral Oral Med Oral Pathol 1988;65:693–8 [DOI] [PubMed] [Google Scholar]
- 2.Pitt SK, Rout PG. Rhinoliths presenting during routine radiography: two cases. Dent Update 2000;27:505–7 [DOI] [PubMed] [Google Scholar]
- 3.Hadi U, Ghossaini S, Zaytoun G. Rhinolithiasis: a forgotten entity. Otolaryngol Head Neck Surg 2002;126:48–51 [DOI] [PubMed] [Google Scholar]
- 4.Yasar H, Ozkul H, Verim A. Rhinolithiasis: a retrospective study and review of the literature. Ear Nose Throat J 2009;88:E24. [PubMed] [Google Scholar]
- 5.Sumbullu MA, Tozoglu U, Yoruk O, et al. Rhinolithiasis: the importance of flat panel detector-based cone beam computed tomography in diagnosis and treatment. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2009;107:e65–7 [DOI] [PubMed] [Google Scholar]
- 6.Kharoubi S. General review of rhinolithiases. Ann Otolaryngol Chir Cervicofac 2008;125:11–17 [DOI] [PubMed] [Google Scholar]