

Abstract
A 50-year-old woman with Beçhet's disease presented with episodic diarrhoea and generalised abdominal pain. She was on regular mycophenolate maintenance therapy, being intolerant of both ciclosporin and azathioprine. Previous rectal biopsy was consistent with colitis, probably associated with Beçhet's disease. During this admission, she began passing faecal matter per vaginam. Digital rectal examination confirmed the presence of a large rectovaginal fistula. She underwent urgent laparotomy for a subtotal colectomy with end ileostomy. Although there were no signs of septicaemia preoperatively, small perforations were identified in the caecum and at the splenic flexure on laparotomy. Histopathology confirmed the presence of multiple shallow ulcers throughout the colon with features suggestive of Beçhet's colitis.
Background
Although originally described by Hippocrates,1 2 Beçhet's disease was first identified as a syndrome by a Turkish physician, Hulusi Beçhet,3 in 1937. It is a systemic vasculitis characterised by recurrent oral aphthous ulceration associated with urogenital ulceration, skin lesions and eye inflammation.2 4
Our patient has had an undulating pattern of disease progression since her diagnosis in 2001 and has been hospitalised multiple times for relapses. Each time she presented with characteristic systemic features of Beçhet's disease such as oral apthae, skin lesions and genital ulceration. Her medical notes suggest she previously had a positive pathergy response inducible by venepuncture. However, on this admission she presented without systemic Beçhet's disease symptoms and the pathergy phenomenon could not be elicited. She was neither septic nor peritonitic, even though her bowel was later found to be perforated.
Rectovaginal fistula in the absence of other characteristic symptoms is an important but uncommon presentation of Beçhet's disease.
Case presentation
A 50-year-old Caucasian woman with a known history of Beçhet's disease was admitted with episodic diarrhoea and generalised abdominal pain. A diagnosis of Beçhet's disease was made in 2001 but she had experienced symptoms consistent with Beçhet's disease for 20 years. These included recurrent oral and vaginal ulceration along with polyarthropathy, vasculitic papular rash and a positive pathergy test. She did not report gastrointestinal symptoms until September 2008 when she experienced weight loss and recurrent episodes of severe vomiting and diarrhoea. Colonoscopy identified significant bowel ulceration, although the biopsy was unable to confirm Beçhet's intestinal disease. The patient was commenced on 60 mg prednisolone which elicited a satisfactory response. In January 2009, she became refractory to steroid treatment and an 8-weekly course of infliximab was initiated.
During this admission, she complained of profuse diarrhoea and faeculent discharge about eight times daily. She denied appreciable weight loss, anorexia or fever. Her drug history included mycophenolate 1 g twice daily, infliximab once every 8-week therapy, lansoprazole, ilandronate, calcium, vitamin and prednisolone 20 mg once a day. On examination her abdomen was soft and only tender to deep palpation. Pelvic and digital rectal examination confirmed a 2×3 cm rectovaginal fistula (RVF).
Differential diagnosis
RVF are common postpartum complications especially following episiotomy.5 6 Crohn's disease is the second commonest cause of RVF6 and may occur concurrently with Beçhet's disease.7 However, in this case, the history of Beçhet's disease was sufficient to explain the fistula as a result of intestinal Beçhet's colitis.
Treatment
The patient was started on high dose steroid treatment (prednisolone 60 mg once a day), metronidazole and mycophenolate. However, she did not respond to this 7-day treatment and surgical input was therefore indicated. She underwent emergency laparotomy with an end ileostomy. Her bowel was found to be perforated at the caecum and splenic flexure, the latter associated with an abscess.
Outcome and follow-up
Although the patient's large bowel was perforated in two places, she did not exhibit signs of peritonitis or sepsis preoperatively. This may be explained by symptom masking as a result of steroid administration.8
She made an initial recovery but subsequently developed a fluid collection 10 days later (figure 1). Two pigtail drains were inserted to drain the collection but failed to control her symptoms. She underwent a further laparotomy 2 weeks later to facilitate abdominal drainage and washout with 10 l of fluid. A Hickman line was inserted to enable total parenteral nutrition.
Figure 1.
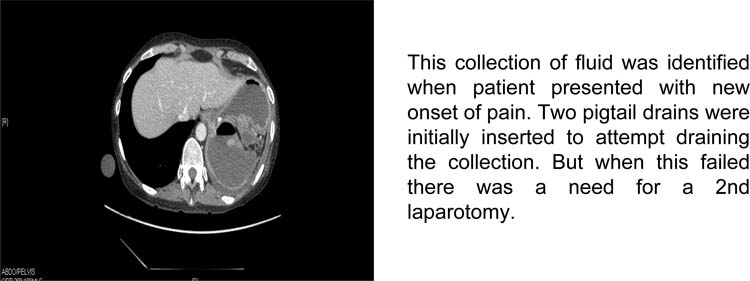
CT- Abdomen. Image showing collection of fluid identified when the patient presented with new onset of pain.
The patient showed signs of improvement but later developed central line sepsis (Klebsiella sp. was cultured). She was transferred to the intensive care unit for escalated monitoring and aggressive treatment. While in the intensive therapy unit she developed an enterocutaneous fistula which was conservatively managed. These complications delayed her recovery but she was finally discharged 62 days after her emergency admission.
Discussion
Gastrointestinal symptoms in Beçhet's disease include vomiting, abdominal pain, flatulence, diarrhoea and constipation.4 9 It is more common in patients from the far East than from Europe.2 The ethnic and geographical variation in the distribution of symptoms associated with Beçhet's disease could provide clues to the genetic basis of this condition. No single causative gene for Beçhet's disease has yet emerged, although it exhibits a marked association with human leukocyte antigen-B51.2
The progression of mild abdominal symptoms to fistula formation within a year demonstrates the unpredictability of Beçhet's intestinal disease progression. Our patient had a long history of Beçhet's disease before rapidly developing gastrointestinal symptoms years later. Only one case of fistula formation 2 months after initial presentation has been described to date.10 It is widely accepted that gastrointestinal symptoms do not develop before the major criteria of the syndrome (as defined by an international study group in 1990) are satisfied.4 In general, gastrointestinal symptoms develop around 6 years after first presentation.11 The diagnosis of Beçhet's disease is often delayed as initial symptoms may not be immediately recognised as part of the constellation making up the syndrome. Patients often have Beçhet's disease long before diagnosis and so the development of RVF 2 months after diagnosis (as in the case mentioned above10) could be an artefact of delayed diagnosis.
A case of RVF in a Beçhet's disease patient after episiotomy has been previously described.12 In this case, surgical management using diversion colostomy and two advancement flap procedures failed to resolve the fistula. Infliximab was subsequently used until the fistula resolved and a mucosal flap was created.12 However, in our patient, the fistula developed in the setting of treatment with infliximab. Continuation of this drug was therefore abandoned in favour of surgical management.
The gastrointestinal and systemic features of Beçhet's disease and inflammatory bowel diseases (especially Crohn's disease) overlap considerably, thus posing a diagnostic challenge.13 14 There are reported cases of Beçhet's intestinal colitis mimicking Crohn's disease but without the typical granulomatous inflammation.14 There are other reports that support the possibility of co-existent Beçhet's colitis and Crohn's disease in one patient.7 Systemic manifestations of both conditions are remarkably similar. Uveitis, oral aphtous ulcers, erythema nodusum and arthritis are features of both diseases. However, urogenital ulcers tend to occur frequently in Beçhet's but rarely, if ever, in Crohn's disease. Colonoscopic appearance can sometimes be inconclusive as longitudinal ulcers and the cobblestone mucosa appearance previously associated with Crohn's have also been noted in Beçhet's disease.13 14 The only way to reliably distinguish between these conditions is histopathology (figure 2). Transmural inflammation is a hallmark of both conditions but granuloma formation, lymphoid aggregates and submucosal fibrosis are rarely found in Beçhet's disease.
Figure 2.
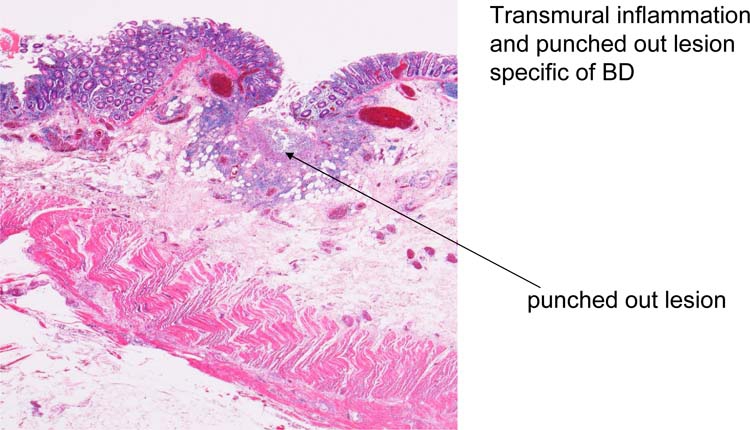
Histopathology slide of resected colon. The transmural inflammation and punched out lesion specific of Beçhet's disease is shown.
Learning points.
-
▶
Beçhet's intestinal disease is an unusual cause of rectovaginal fistula, so other possibilities must be excluded.
-
▶
Surgical treatment should not be delayed in cases where medical therapy does not yield anticipated results.
-
▶
The possibility of concurrent Crohn's disease and Beçhet's disease in the same patient means histopathology remains the definitive mode for establishing diagnosis.
Footnotes
Competing interests None.
Patient consent Obtained.
References
- 1.Feigenbaumn A. Description of Behçet's syndrome in the Hippocratic Third Book of Endemic Diseases. Br J Ophthalmol 1956; 40:355–357 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Verity DH, Wallace GR, Vaughan RW, et al. Behçet's disease: from Hippocrates to the third millennium. Br J Ophthalmol 2003;87:1175–83 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.UStün C. A famous Turkish dermatologist, Dr. Hulusi Behçet. Eur J Dermatol 2002;12:469–70 [PubMed] [Google Scholar]
- 4.International Study Group for Behçet's Disease. Criteria for diagnosis of Behçet's disease. Lancet. 1990; 335:1078–80 [PubMed] [Google Scholar]
- 5.Venkatesh KS, Ramanujam PS, Larson DM, et al. Anorectal complications of vaginal delivery. Dis Colon Rectum 1989;32:1039–41 [DOI] [PubMed] [Google Scholar]
- 6.Rivadeneira DE, Ruffo B, Amrani S, et al. Rectovaginal fistulas: current surgical management. Clin Colon Rectal Surg 2007;20:96–101 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Houman H, Dahmen FB, Ghorbel IB, et al. Behcet's disease associated with Crohn's disease. Annales de Medecine Interne. 2001;152:480–2 [PubMed] [Google Scholar]
- 8.Klygis LM, Jutabha R, McCrohan MB, et al. Esophageal perforations masked by steroids. Abdom Imaging 1993;18:10–2 [DOI] [PubMed] [Google Scholar]
- 9.Kobayashi K, Ueno F, Bito S, et al. Development of consensus statements for the diagnosis and management of intestinal Behçet's disease using a modified Delphi approach. J Gastroenterol 2007;42:737–45 [DOI] [PubMed] [Google Scholar]
- 10.Teh LS, Green KA, O'Sullivan MM, et al. Behçet's syndrome: severe proctitis with rectovaginal fistula formation. Ann Rheum Dis 1989;48:779–80 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Smith GE, Kime LR, Pitcher JL. The colitis of Behcet's disease: a separate entity? Colonoscopic findings and literature review. Am J Dig Dis 1973;18:987–1000 [DOI] [PubMed] [Google Scholar]
- 12.Chawla S, Smart CJ, Moots RJ. Recto-vaginal fistula: a refractory complication of Behcet's disease. Colorectal Dis 2007;9:667–8 [DOI] [PubMed] [Google Scholar]
- 13.Levent F, Ibrahim B. Differentiation of Behcet's disease from inflammatory bowel diseases: Anti-saccharomyces cerevisiae antibody and anti-neutrophilic cytoplasmic antibody. World J Gastroenterol 2008. ;14:7271. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Kim ES, Chung WC, Lee KM, et al. A case of intestinal Behcet's disease similar to Crohn's colitis. J Korean Med Sci 2007;22:918–22 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Lee SK, Kim BK, Kim TI, et al. Differential diagnosis of intestinal Behçet's disease and Crohn's disease by colonoscopic findings. Endoscopy 2009;41:9–16 [DOI] [PubMed] [Google Scholar]