

Abstract
Context: In a recent article in this journal, Sam Harper and his colleagues (2010) call for increased awareness and open dialogue of moral judgments underlying health inequality measures. They recommend that analysts use relative inequality measures when concerned only about health inequality but use absolute inequality measures when also concerned about other issues, such as the overall level of population health and the level of health for each group in the population.
Methods: Using a simple, hypothetical example, this commentary shows that the relationships among inequality, the absolute level for each group, and the overall level in the population are more complex than suggested by the analysis by Harper and his colleagues.
Findings: First, analysts must make the choice of absolute or relative inequality measures, separately, for single- and multiple-population cases. Second, in the single-population cases, analysts can use both relative and absolute inequality measures when concerned only about health inequality independent of other considerations. Third, in almost all real-world multiple-population cases, when using either the absolute or relative inequality measure, the assessment of health inequality is influenced by the absolute level of health for each group.
Conclusions: The choice between absolute and relative inequality measures is not about the independent normative significance of inequality, as Harper and his colleagues suggest. In choosing between absolute and relative measures, future work needs to integrate an empirical examination of values, a moral assessment of values, and a technical understanding of inequality measures.
Keywords: Health inequalities, measurement, ethics, health policy
In a recent article in this journal, Sam Harper and his colleagues (2010) call for increased awareness and an open dialogue about the moral judgments underlying health inequality measures. Before this article was written, the issue of value judgments regarding health inequality measures rarely enjoyed the systematic treatment it deserves (Asada 2007). Using real-world examples, the Harper article reviews five issues that require value judgments in the measurement of health inequalities: (1) choosing absolute or relative inequality measures, (2) determining the boundaries of the population within which health inequalities can most meaningfully be measured, (3) being sensitive to the shape of health distributions in the assessment of health inequalities, (4) giving extra weight to the health of the disadvantaged when measuring inequalities, and (5) identifying the standard against which inequality is assessed.
My commentary focuses on the first issue, the recommendation by Harper and his colleagues that analysts use relative inequality measures when concerned only about health inequality (i.e., endorsing “the very strict egalitarian position that what matters is equality in itself, independent of other considerations”[Harper et al. 2010, 9]) but use absolute inequality measures when concerned also about other issues, such as the population's overall level of health and each group's level of health (i.e., supporting the view that “inequality matters but it is not all that matters”[10]). The authors’ effort to explore the “best metric for assessing trends in inequality” (9) is commendable, and paying attention to both the normative and the technical aspects of inequality measures is important. But choosing between absolute and relative inequality measures is not about the independent normative significance of inequality, as the authors suggest.
The relationships among inequality, the absolute level for each group, and the overall level in the population are more complex than suggested by the analysis in the Harper article. Here, using a simple, hypothetical example, I show, first, that analysts must make the choice of absolute or relative inequality measures, separately, for single- and multiple-population cases. In single-population cases analysts measure inequality in one population, and in multiple-population cases analysts compare inequalities across populations, either cross-sectionally or longitudinally. Second, I demonstrate that in the single-population cases, analysts can use both relative and absolute inequality measures when concerned only about health inequality independent of other considerations. Third, I show that in almost all real-world multiple-population cases, when using either the absolute or the relative inequality measure, the assessment of health inequality is influenced by each group's absolute level of health. I end by sketching out future work that will help analysts choose between absolute and relative measures.
Single-Population Cases
Suppose that we are concerned about inequality in life expectancy by sex in a society in which the population is divided evenly between men and women. This society is very sick: the life expectancy for men is twenty years and for women is thirty years; thus the average life expectancy is twenty-five years. We can measure the degree of inequality in life expectancy by sex in this society by either the absolute inequality measure (life expectancy for women—life expectancy for men) or the relative inequality measure (life expectancy for women/life expectancy for men). The absolute inequality measure indicates that women are expected to live ten years longer than men, whereas the relative inequality measure suggests that women live 50 percent longer than men.
Notice that neither the absolute nor the relative inequality measure says anything about the population's overall level of health or each group's absolute level of health. The same ten-year difference could come from a sicker population (10, 20), and the same 50 percent difference could come from a healthier population (60, 90). Thus, in the single-population cases, for which we are interested in the degree of health inequality in one population, we can use both relative and absolute inequality measures to assess only inequality.
Multiple-Population Cases
Imagine that scientists discover two types of pills to improve the life expectancy of both men and women (figure 1). Both pills improve the life expectancy of the population by twenty-five to fifty years, but the pills distribute the improvements differently between men and women. If all the persons in this society take one red pill each, the life expectancy of both men and women will increase by twenty-five years, thereby increasing it to forty-five years and fifty-five years, respectively. But if all persons take one blue pill each, the life expectancy of both men and women will double, thereby increasing it to forty years and sixty years, respectively.
Figure 1.
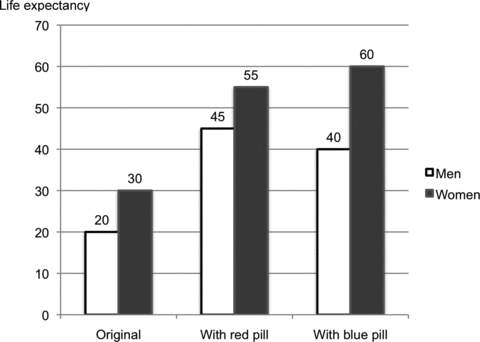
A Hypothetical Example of Comparing Health Inequalities across Populations.
Does each pill reduce inequality in life expectancy by sex? This is a question for multiple-population cases, for which we measure health inequality in each population (i.e., the original, the red pill, and the blue pill) and compare health inequalities across populations (i.e., the original versus the red pill, and the original versus the blue pill). In the multiple-population cases, the information about the absolute level of health for each group (i.e., men and women) and how it differs across populations is important to the measurement of health inequalities. In addition, properties of absolute and relative measures that are not obvious in the single-population cases become apparent. The absolute inequality measure estimates the degree of inequality invariant across populations with equal absolute difference for the comparative groups (e.g., the original versus the red pill), and the relative inequality measure assesses the degree of inequality invariant across populations with equal relative difference for the comparative groups (e.g., the original versus the blue pill). In the inequality measurement literature, these properties are referred to as mean-sensitivity. It is obvious from the hypothetical example, however, that the mean is not the driving force of these properties. Rather, the driving force is the absolute level of health for each group, whose differences across populations result in a difference in the mean across populations. For example, although both the red pill population and the blue pill population have the same mean, their absolute and relative inequality measures differ.
Even though these properties—insensitivity to the equal absolute change or translation invariance and insensitivity to the equal proportional change or scale invariance—are well known, their implications in empirical application are rarely articulated. Apart from a hypothetical scenario like that in figure 1, we rarely observe health distributions that are different either equiproportionally or equiabsolutely. For example, none of the real-world examples that Harper and his colleagues use in their article fits equiproportional or equiabsolute differences. Analysts still can apply absolute and relative measures to any distributions, but in real-world applications, the assessment of health inequality is influenced by each group's absolute level of health. Both measures suggest that the inequality is smaller when the sicker group improves more than the healthier group but that the inequality is greater when the healthier group improves more than the sicker group. The difference between these measures is that the absolute inequality measure always considers improvement in terms of the absolute difference, whereas the relative inequality measure considers it in terms of the relative difference.
Thus, in the obesity example presented by Harper and his colleagues, in which the prevalence of obesity was 13.8 percent among the low-education group and 8.6 percent among the high-education group from 1976 to 1980 and was 24.1 percent and 17.1 percent, respectively, from 1988 to 1994, it is correct to state: “If we consider the rate difference … we would conclude that inequality is worsening in this case because the absolute increase in the rate of obesity has been greater for the disadvantaged” (Harper et al. 2010, 10). But the reason why the rate ratio (relative inequality) indicates that “educational inequalities in obesity are decreasing” (10) is not because the rate ratio is “implicitly endorsing the position that equality matters most” (10) but because the relative increase in the rate of obesity has been greater for the advantaged.
Future Work
We should investigate our conception of health inequality recognizing the complex relationships among inequality, the level of each group or individual, and the overall level. To do so, we need to integrate an empirical examination of values, a moral assessment of our values, and technical understanding of inequality measures.
It will be useful to know empirically just how people compare inequalities across different distributions and overall levels (e.g., do people think that health inequality is reduced, increased, or unchanged after taking the red or the blue pill, and what aspects of distributions affect their judgment?). Such an empirical examination would be largely an uncharted area, except for the work by Gakidou, Murray, and Frenk (2000) in developing the inequality measure for The World Health Report 2000 by the World Health Organization (WHO 2000). Their survey respondents indicated that an equal proportional increase (e.g., the blue pill) increases the inequality and that an equal absolute addition (e.g., the red pill) reduces the inequality. This finding implies that neither absolute nor relative inequality measures alone properly reflect our conception of inequality.
Even though such an empirical examination can uncover potential disagreements between available inequality measures and our conception of inequality, it should not be our only guide for choosing or developing inequality measures. People's perceptions may not always offer the right answer, so a careful moral investigation of our values is necessary as well. Philosopher Larry Temkin's Inequality(1993), a major landmark in this literature, was a resource for the WHO team's development of the inequality measure. Temkin asked whether “inequality matter[s] more in a poor society than in a rich one” (1993, 157), and interestingly, his answer appears to support the WHO survey respondents’ assessments (Asada 2007, 115–16). Should the moral investigation indeed corroborate the empirical assessment, the question of choosing either the absolute or the relative inequality measures would be irrelevant. But the development or application of alternative inequality measures would be necessary, such as intermediate inequality measures assessing that an equal absolute increase makes the inequality smaller but an equal proportional increase makes the inequality greater (according to such measures, compared with the original population the inequality is smaller in the red pill population and greater in the blue pill population).
After empirically and morally investigating our conceptions of inequality, we then must express them in the quantitative language of inequality measures. Not long ago, Erreygers (2009) called attention to another issue: the choice of absolute or relative health inequality measures may depend not only on the relationship among inequality, the absolute level of each group or individual, and the population's overall health but also on the scale type (i.e., ordinal, interval, or ratio) of the measurement of health. Erreygers was suggesting that the measurement of health inequalities must extend beyond learning from the measurement of income inequalities and must be responsive to additional complications caused by the measurement of health.
Acknowledgments
I am grateful for comments from Dan Hausman, Jeremiah Hurley, George Kephart, Adrian Levy, André Maddison, Thomas Muir, John Mullahy, Ole Frithjof Norheim, Trygve Ottersen, Alyce Whipp, Dan Wikler, and Yoko Yoshida. The views presented in this article and the remaining errors are mine. I thank the Canadian Institutes of Health Research New Investigator Award and the Dalhousie Faculty of Medicine Clinical Research Scholar Award for their support.
References
- Asada Y. Health Inequality: Morality and Measurement. Toronto: University of Toronto Press; 2007. [Google Scholar]
- Erreygers G. Can a Single Indicator Measure Both Attainment and Shortfall Inequality? Journal of Health Economics. 2009;28:885–93. doi: 10.1016/j.jhealeco.2009.03.005. [DOI] [PubMed] [Google Scholar]
- Gakidou E, Murray CJL, Frenk J. Measuring Preferences on Health System Performance Assessment. 2000. Global Programme on Evidence for Health Policy Discussion Paper 20. Available at http://www.who.int/healthinfo/paper20.pdf (accessed September 9, 2010) [Google Scholar]
- Harper S, King NB, Meersman SC, Reichman ME, Breen N, Lynch J. Implicit Value Judgments in the Measurement of Health Inequalities. The Milbank Quarterly. 2010;88(1):4–29. doi: 10.1111/j.1468-0009.2010.00587.x. Available at http://www.milbank.org/quarterly/8801feat.html (accessed November 4, 2010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Temkin L. Inequality. New York: Oxford University Press; 1993. [Google Scholar]
- WHO (World Health Organization) The World Health Report 2000—Health Systems: Improving Performance. Geneva: 2000. Available at http://www.who.int/whr/2000/en/index.html (accessed November 5, 2010. [Google Scholar]