

Abstract
The goal of the current study was to determine if failure to develop/utilize alcohol-specific strategies to manage drinking behavior might serve as a mechanism through which early alcohol exposure leads to higher levels of later alcohol use and alcohol-related negative consequences, while taking into account impulsivity as an underlying risk factor for both of these outcomes. Data were collected between September and December of 2005 from a random sample of college students via an online survey. A total of 309 students provided complete data on all measure of interest. Separate regression analyses predicting typical weekly alcohol consumption and alcohol-related problems indicated that use of alcohol-specific protective strategies partially mediated the effect of age of first use on these outcomes. An earlier age of onset was associated with less frequent use of alcohol-specific protective strategies, which in turn was associated with drinking- and alcohol-related problems. Implications for tailoring alcohol prevention and intervention programs targeting adolescents are discussed.
Keywords: Alcohol, Age of first use, Protective behavioral strategies, College students
Alcohol use and misuse by adolescents and young adults is a major public health issue. Findings from Monitoring the Future (MTF) indicate that 14% of 8th graders, 35% of 10th graders, and 48% of 12th graders report having been drunk in the past year (Johnston et al., 2006a). Although rates of alcohol consumption in high school are alarming, peak rates do not occur until early adulthood when many young people begin college. Data from MTF show that rates of any drinking and heavy drinking (five or more drinks on one occasion) are higher among college students than among any other group in the population (Johnston et al., 2006b). In response to high rates of consumption among adolescents and young adults, the Surgeon General issued a “Call to Action to Prevent and Reduce Underage Drinking” in 2007. The report highlighted the problem and emphasized the need for research identifying both risk and protective factors (U.S. Department of Health and Human Services, 2007). In addition to identifying risk and protective factors for alcohol consumption, it is critical to identify factors influencing the development of alcohol-related problems because negative consequences may occur at relatively moderate levels of consumption for some individuals.
One known risk factor that is particularly relevant for underage drinking is age of first alcohol use. Research has consistently shown that an earlier age of first alcohol use is associated with increased potential for the subsequent development of a maladaptive pattern of alcohol use and alcohol dependence (DeWit et al., 2000; Grant and Dawson, 1997; Hawkins et al., 1997; Warner and White, 2003). For example, among a normative sample of adolescents, Pedersen and Skrondal (1998) found alcohol use prior to age 13 was predictive of increased drinking- and alcohol-related problems by age 19. Although age of first use is reliably associated with risk for alcohol-related problems, the mechanism of risk associated with an early age of first is not yet clear. Some have argued that early exposure to alcohol interferes with cognitive and social developments due to neurotoxic effects of alcohol occurring during a critical stage of brain development (cite). Others have argued that an early age of drinking onset is simply a marker for other known risk factors like impulsivity (McGue et al., 2001). To determine if an early age of first use is a cause or simply a correlate of alcohol-related problems, it is critical to conduct research that examines both underlying trait factors like impulsivity, and potential intermediate behaviors that may serve as mechanisms of risk.
Thus, the goal of the current study was to examine alcohol-specific protective strategies (e.g. strategies used to control levels of consumption) as one mechanism through which early alcohol exposure might contribute to later risk, while taking into account impulsivity as an underlying risk factor. We hypothesized that early exposure to alcohol would be associated with impaired cognitive function leading to a failure to develop effective strategies for managing and moderating alcohol consumption, and that the failure to develop these strategies would increase risk for the experience of alcohol-related problems.
Consistent with our hypothesis, alcohol use in adolescence has been found to have a significant negative impact on brain development, which may impact cognitive functions including memory, learning, and decision-making. For example, Tapert et al. (2002) found that, among both alcohol abusing and non-abusing adolescents, greater alcohol involvement was directly related to poorer cognitive performance that continued to worsen with ongoing alcohol consumption into adulthood. Individuals who are cognitively impaired by alcohol may fail to develop adequate strategies to regulate their behavior, including alcohol consumption. In support of this model, Brown and Tapert (2004) found that adolescents who were lower in cognitive functioning and who used fewer coping skills reported greater alcohol and drug use after treatment. Failure to develop adequate self-regulation skills in adolescence may set the stage for later problems with alcohol, particularly during college when alcohol is widely available and drinking is normative.
Consistent with this possibility, studies with college students suggest that failure to use alcohol-specific skills to manage drinking behavior may serve as a risk factor for the development of problems. For example, Martens et al. (2004) found increased negative consequences among students who failed to use alcohol-specific protective strategies, even when controlling for gender and alcohol consumption. Another study found that students who used protective behaviors such as “using a designated driver, limiting number of drinks, making one’s own drinks” (p. 115) reported fewer negative consequences (Benton et al., 2004). It is important to note that, even among students whose drinking was considered ‘above the norm’ (i.e., 6 or more drinks when they party), the use of protective behavioral strategies was related to experiencing fewer harmful consequences. In addition, women (who typically drink less) generally use more alcohol-specific protective behavioral strategies than men, presumably to limit intoxication and consequences (Delva et al., 2004; Haines et al., 2006; Walters et al., 2007).
Although there is considerable evidence for the importance of alcohol-specific protective strategies as a predictor of drinking behavior, no study to date has examined use of these strategies in relation to age of onset of alcohol use. Thus, the goal of the current study was to assess alcohol-specific protective strategies as a potential mechanism through which early alcohol exposure might contribute to later risk. In addition, we controlled for the influence of impulsivity on drinking behavior given considerable evidence that impulsivity is related to both age of first alcohol use and alcohol-related negative consequences (Patock-Peckham and Morgan-Lopez, 2006; Simmons et al., 2004).
1. Method
1.1. Participants and procedures
A total of 1440 randomly sampled undergraduate students from a small, private university in the northeastern United States were invited via e-mail to participate in an online survey retrospectively assessing health behaviors during the fall semester of 2005. The survey was administered online via a research-based web server with secure 128 bit data encryption, and took approximately 30–50 min to complete. Participants were entered into a drawing for one of five $20 Visa Gift Cards that would be awarded to participants from each of twelve residential units. Participants who responded to the invitation were required to complete an electronic consent form and all participants who provided consent were eligible for the prize drawing, even if they did not complete the survey. Individuals who did not respond to the original invitation were sent subsequent e-mail invitations once every 5 days for 3 weeks, at which point the survey was closed. The overall response rate was modest (29.4%, N=423), but consistent with other studies using this approach (McCabe et al., 2006). All study procedures were approved by the institutional review board for human subjects.
Of the 423 students who initiated the survey, 65 were excluded from all analyses as they reported no drinking during the assessment window (i.e., 39 reported that they were lifetime abstainers and 26 reported no alcohol consumption in the past 3 months and thus were not asked to answer questions related to negative consequences of drinking or use of protective drinking strategies). An additional 41 cases were excluded from analyses due to incomplete data (i.e., they discontinued the survey prior to completing all measures or selectively refused to answer questions used to calculate variables in the analyses), and another 8 cases were excluded due to reported values that represented statistical outliers (see Data management section for further details). Thus, the final sample comprised 309 drinkers (Mage =19.84 years; SD=1.33). Consistent with national norms, approximately half of the sample (56.6%) identified as female (Snyder et al., 2008). The distributions of race endorsed by participants were: 75.1% Caucasian, 11.7% Asian American, 2.9% African American, and 10.3% of mixed or other racial identity. In addition to the racial categories above, 6.1% of the sample reported Hispanic/Latino as their ethnicity. Relative to the racial/ethnic distribution of undergraduate students enrolled in the fall of 2005 (the last year reported by the National Center for Education Statistics), Caucasian and Asian-American students were slightly over-represented (66.7% and 6.5%, respectively), and African--American students were under-represented (13.1%; Snyder et al., 2008). Although the sample of 309 was largely representative of the larger sample of 423 who initiated the survey, participants in the final sample were slightly older than those who were not included in analyses (M=19.85, SD=1.34 versus M=19.34, SD=1.37). In addition, Caucasian participants were over-represented (75.4% versus 57.5%) and Asian American (12.1% versus 18.3%) and African American (3.0% versus 13.3%) participants were under-represented in the final sample relative to those who were not included.
1.2. Measures
Participants were asked to provide basic demographic information including their current age, ethnic and racial identity (separate questions), and biological sex. Age of first drink was assessed via a single continuous item adapted from the Core Alcohol and Drug Survey, Long Form (Core Institute, 2005): “At what age did you first use alcohol without the permission of your parents?”
Impulsivity was assessed via the 30-item Barratt Impulsiveness Scale-11 (BIS-11; Patton, Stanford, & Barratt, 1995). The BIS-11 assesses three different facets of impulsivity: motor impulsiveness (i.e., physical action without thought), attentional impulsiveness (i.e., lack of concentration), and non-planning impulsiveness (i.e., spontaneity and present-focused orientation). Participants were asked to respond to items such as “I do things without thinking,” “I have racing thoughts,” and “I make up my mind quickly” on a 4-point Likert-type scale with anchors of rarely/never, occasionally, often, and almost always. The BIS-11 total scale (summing all of the items on the full scale) demonstrated acceptable internal consistency within this sample (Cronbach’s alpha=.82).
Typical weekly drinking during the past 3 months was assessed via a revised version of the Daily Drinking Questionnaire (DDQ; Collins, Parks, & Marlatt, 1985). The Daily Drinking Questionnaire-Revised (DDQ-R) disaggregates typical frequency and quantity information by assessing how many days each week individuals consumed alcohol on average, and only for those days that they drank, how many drinks they typically consumed. Typical weekly consumption was calculated by summing the quantity estimates for each drinking day, dividing by seven, and multiplying this average by the frequency estimate.
Alcohol-related negative consequences experienced during the past 3 months were assessed via the 23-item version of the Rutgers Alcohol Problems Index (RAPI; White and Labouvie, 1989). Items include “Not able to work or study for a test” and “Was told by a friend or neighbor to stop or cut down on drinking.” As responses to the individual items on the RAPI and the overall composite scores were non-normally distributed, each item was made dichotomous (0=consequence not experienced in the past 3 months, 1=consequence experienced one or more times in the past 3 months). Individual items were then summed to assess the total number of different consequences that were experienced during the assessment window. Thus, the possible range of scores for the measure was 0 to 23. The dichotomized RAPI demonstrated reasonable internal consistency in this sample (Kuder–Richardson=0.81).
The frequency with which participants engaged in controlled-drinking strategies (i.e., specific behaviors to moderate their level of intoxication before or during drinking episodes) was assessed via the 16-item Protective Strategies Questionnaire (PSQ; Palmer, 2004) using a Likert-type scale (1=never, 7=always). Items on the PSQ are prefaced by “When I am drinking, I…” and followed by various behaviors such as “count the number of drinks I have over the course of the night” and “alternate alcoholic drinks with non-alcoholic beverages.” The PSQ demonstrated good internal consistency in this sample (Cronbach’s alpha=0.85).
1.3. Data management
Prior to creating the weekly drinking composite score, data were examined for univariate and multivariate outliers. Values greater than three standard deviations from the mean were identified as potential outliers and were examined relative to the overall distribution. Two values outside the distribution were identified for drinks per drinking day (values of 20.43 and 15.3 relative to the next highest value of 12.14) and one value was identified for alcohol-related problems (value of 21 relative to the next highest value of 16). These three cases were removed from the data set and the distributions of the remaining scores were examined for assumptions of normality. The typical weekly drinking measure was significantly non-normal even after the removal of univariate outliers and was therefore log-transformed. Next, the data were examined for multivariate outliers using Mahalanobis distance and leverage z values greater than 3.29 (p<.001). Five cases were identified as multivariate outliers and removed from the data set. Because removal of multivariate outliers can lead to the identification of new outliers that were hidden by the ones excluded, Mahalanobis distance and leverage were recalculated after removing the five cases. No additional multivariate outliers were identified. Means and standard deviations for drinking behavior/problems, age of first use, and protective strategies are provided in Table 1 (note that raw score values are presented for weekly drinking for ease of interpretation though the log-transformed data were used in the regression models).
Table 1.
Means (SD) for alcohol use, problems, age of first use and protective strategies.
| Variable | Mean | (SD) | Range |
|---|---|---|---|
| Drinking days per week | 1.71 | 1.19 | 0.00–7.00 |
| Drinks per drinking day | 1.69 | 1.69 | 0.14–12.14 |
| Total weekly drinking | 3.99 | 5.90 | 0.00–36.43 |
| Age of first use | 16.30 | 2.05 | 9.00–26.00 |
| Alcohol-related problems | 3.52 | 3.46 | 0.00–16.00 |
| Protective strategies | 3.55 | 0.94 | 1.15–6.00 |
1.4. Data analytic approach
Initially, correlations among age of first use, typical weekly consumption, alcohol-related problems, and BIS-11 scores were examined to see if impulsivity was significantly associated with age of first use and drinking behavior/problems. Such evidence would provide support for including BIS-11 scores in the regression analyses assessing protective strategies as a potential mediating variable. Next, standard procedures for testing mediation (Baron & Kenny, 1986) were used to evaluate the hypothesis that use of protective strategies mediates the relation between age of first use of alcohol and current drinking behavior/problems. Separate models were tested with typical weekly consumption and alcohol-related problems as outcomes. In all analyses, demographic variables of age and sex were included in the models.
In the first linear regression model for alcohol use, the direct effect of age of first use on typical weekly consumption was assessed. Next, age of first use was examined as a predictor of protective strategies. Protective strategies were then assessed as a predictor of typical weekly drinking. Finally, a full model was evaluated with both the independent variable (age of first use) and the proposed mediator (protective strategies) included as predictors of typical weekly consumption. All predictors within each model were entered simultaneously. A reduction in the size of the direct effect from age of first use to typical weekly consumption in the full model would suggest that protective strategies serve as a mediator. Full mediation would be demonstrated if the direct effect was no longer statistically significant. The Sobel z test was used to determine if the indirect effect of age of first use on typical weekly consumption (through protective strategies) was statistically significant. With the exception of the outcome measure, the approach used to test mediation with alcohol-related problems was identical.
2. Results
Correlations among age of first use, typical weekly consumption, alcohol-related problems, and BIS-11 scores are presented in Table 2. The correlation between BIS-11 scores and age of first use was significant and inverse (r=−.26) and correlations between BIS-11 scores and both alcohol use and problems were significant and positive (r=.35 and r=.34, respectively). Thus, impulsivity as assessed by the BIS-11 might well account for shared variability in the relation between age of first use and drinking behavior/problems, and BIS-11 scores were included in all regression models used to test the primary study hypotheses. Multiple regression analyses were used to test the study hypotheses first for typical weekly drinking and then for alcohol-related problems.
Table 2.
Intercorrelations for alcohol use, problems, age of first use and impulsivity.
| Variable | 1 | 2 | 3 | 4 |
|---|---|---|---|---|
| 1. DDQ-R weekly drinking (log) | - | |||
| 2. Age of first use | −0.43** | - | ||
| 3. RAPI alcohol problems | 0.61** | −0.30** | - | |
| 4. BIS-11 | 0.35** | −0.26** | 0.34** | - |
Note. DDQ-R = Revised Daily Drinking Questionnaire Log Transformed Value; RAPI = Rutgers Alcohol Problem Index; BIS-11 = Barratt Impulsiveness Scale.
p<.01.
In the first linear regression model for typical weekly consumption, age, sex, BIS-11 scores, and age of first use were entered as simultaneous predictors, accounting for significant variability (28.1%) in typical weekly consumption, F (4,252)=26.01, p <.001. Sex, β=−.15, p=.005, age, β=.11, p=.034, BIS-11 scores, β=.22, p<.001, and age of first use, β=−.379, p<.001 were each significant predictors of typical weekly consumption with men, older participants, those with higher levels of impulsivity, and those who began drinking at an earlier age reporting greater consumption. The same variables were examined as predictors of protective-strategy use, and again accounted for significant variability (22.7%), F (4,249)=19.53, p<.001. BIS-11 scores, β=−.32, p<.001, and age of first use, β=.26, p<.001 were both significant predictors of protective-strategy use with more frequent use of these strategies among those with lower BIS-11 scores and a later age of first alcohol use. In the next analysis, protective strategies (but not age of first use) were included in the model predicting typical weekly consumption. The model was significant, accounting for 27.9% of the variance in the outcome, F (4,253)=25.86, p<.001. BIS-11 scores, β=.17, p=.005, and protective strategies, β=−.42, p<.001 were both significant predictors of typical weekly consumption with higher BIS-11 scores and less use of protective strategies associated with heavier alcohol use.
Having met the prerequisite criteria for assessing mediation, the full mediation model was tested, accounting for 36.6% of the variance in typical weekly consumption, F (5,248)=30.21, p<.001. Regression coefficients for the full mediation model are presented in Table 3. Significant effects were found for age, sex, BIS-11 scores, age of first use, and protective strategies with the same direction of effects reported in previous models. Although age of first use remained a significant predictor of drinking behavior, the standardized beta coefficient was reduced from −.38 to −.29. In addition, the indirect influence of age of first use on typical weekly consumption through protective strategies was statistically significant, Sobel’s z=3.86, p<.001. Fig. 1 provides a graphic representation of the mediation model with standardized beta values.
Table 3.
Regression analyses for typical weekly drinking- and alcohol-related problems.
| Predictor | DDQ-R weekly drinking (log) |
RAPI problems |
||||||
|---|---|---|---|---|---|---|---|---|
|
n=254 |
n=236 |
|||||||
| ΔR2 | B | SE | β | ΔR2 | B | SE | β | |
| .37** | .26** | |||||||
| Age | .04 | .02 | .10* | −.33 | .21 | −.09 | ||
| Sex | −.09 | .04 | −.11* | .22 | .40 | .03 | ||
| BIS-11 | .05 | .02 | .12* | .65 | .21 | .19** | ||
| Age of first use | −.12 | .02 | −.29** | −.64 | .23 | −.17** | ||
| Protective strategies | −.13 | .02 | −.34** | −1.17 | .22 | −.34** | ||
Note. DDQ-R = Revised Daily Drinking Questionnaire Log Transformed Value; RAPI = Rutgers Alcohol Problem Index; BIS-11 = Barratt Impulsiveness Scale.
p<.05;
p<.01.
Fig. 1.

Mediation model for typing weekly drinking.
The same sequence of regression analyses was conducted with alcohol-related problems as the outcome measure. In the first model (including age of first use but not protective strategies), the variables in the model accounted for 17.3% of the variance in alcohol-related problems, F (4,231)=13.31, p<.001. BIS-11 scores, β=.29, p<.001, and age of first use, β=−.26, p<.001, were both strong predictors of alcohol-related problems, with higher levels of impulsivity and an earlier age of first use associated with more problems. With the same predictors and protective strategies as the outcome, significant effects were again identified for both BIS-11 scores, β=−.32, p<.001, and age of first alcohol use, β=.26, p<.001, and the predictor variables collectively accounted for 22.7% of the variance, F (4,249)=19.53, p<.001. Participants with higher BIS scores and an earlier age of first use were less likely to use protective strategies. The model including protective strategies (but not age of first use) as a predictor of alcohol-related problems, accounted for 23.9% of the variance, F (4,235)=19.82, p<.001. BIS-11 scores, β=.20, p =.001, and protective strategies, β=−.40, p<.001, were both significant predictors, with more problems among those with high BIS-11 scores and low use of protective strategies. As was the case for typical weekly consumption, all prerequisite criteria for assessing mediation were met. In the full mediation model, F (5,230)=17.58, p<.001, BIS-11 scores, age of first use, and protective strategies each significantly predicted alcohol-related problems with direction of effects consistent with earlier models (see Table 3 for the regression coefficients in the full mediation model). Although the effect of age of first use remained significant, the standardized beta was reduced from −.26 to −.17 and the test of the indirect effects was significant, Sobel’s z=−3.74, p<.001. Fig. 2 provides a graphic representation of the mediation model for alcohol-related problems.
Fig. 2.
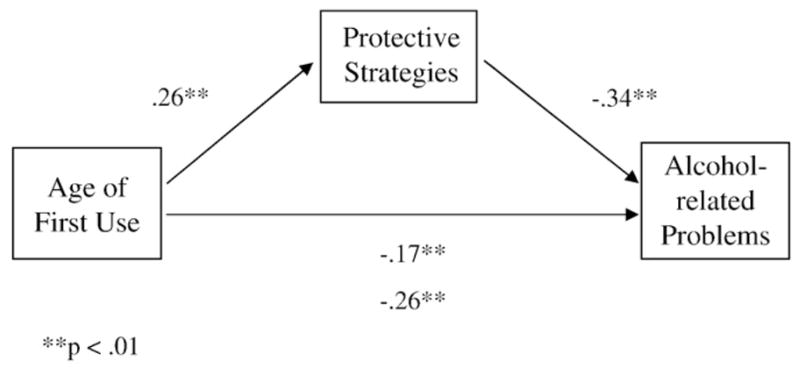
Mediation model for alcohol-related problems.
3. Discussion
Consistent with study hypotheses, an earlier age of first alcohol use was reliably associated with heavier drinking and more negative consequences of drinking, even when controlling for the influence of impulsivity. Thus, the underlying trait of impulsivity does not fully account for the relation between age of first use and later drinking behavior or problems. Although alcohol-specific protective-strategy use did not fully account for the relation, statistically significant indirect effects were observed for both drinking behavior and negative consequences. That is, an earlier age of onset was associated with less frequent use of alcohol-specific protective strategies, which in turn predicted heavier drinking and more alcohol-related problems. Despite the significant indirect effects through alcohol-specific protective-strategy use, age of first use continued to account for significant variability in alcohol-related outcomes, suggesting that research on other possible mediators is warranted.
Although no specific hypotheses were made regarding the relation between impulsivity and alcohol-specific protective strategies, the pattern of results was consistent with the proposed theoretical model. Participants who were highly impulsive engaged in fewer alcohol-specific protective strategies, suggesting that they have impaired behavioral regulation skills, and are not able to effectively plan and make decisions before drinking. Although the study design does not allow one to draw causal inferences about the effects of alcohol on the ability to plan and manage behavior, the results are consistent with alcohol-related impairment in the ability to regulate behavior.
The best way to prevent harm, particularly among adolescents, is to abstain from alcohol consumption. However, the neurotoxic effects of alcohol are dose dependent, and there is no question that heavier drinking is more damaging to the developing brain than is a lower level of consumption. A number of the alcohol-specific strategies addressed involve ways to limit levels of intoxication; if students do consume alcohol the goal would be to avoid excess. For example, certain strategies such as spacing drinks out, turning down a drink, and using protection in sexual situations would still be helpful even if alcohol has been consumed. Thus, reducing levels of alcohol use, although imperfect, may be the best way to reduce alcohol-related neurotoxicity among adolescents who have already begun to use alcohol.
The knowledge gained from the current study has potentially important implications for prevention and intervention programs targeting adolescents. Those with an early age of first use may fail to develop adequate skills to manage behavior, suggesting that interventions designed for use with this group may need to focus on the development of such skills. In contrast, those with a later onset and higher cognitive functioning may already have adequate skills to manage their drinking behavior. If this is the case, skills-based approaches may not be successful, as problems with alcohol for this group may be related to other risk factors (e.g. parental or peer influence, comorbid psychopathology) that might be appropriate targets of intervention. Consistent with this hypothesis, Brown and Tapert (2004) found that development of coping skills was associated with better treatment outcomes for individuals low in cognitive functioning, but not for those high in cognitive functioning. In summary, although considerably more research is needed on this topic, age of first use and related sequalae might eventually be used as a basis upon which to make decisions about the focus of prevention or intervention efforts.
It is important to note that skills-based interventions with underage early-onset drinkers would have to take more of a harm-reduction approach than has been traditionally used. In order to teach skills to moderate behavior, one must acknowledge that the behavior is occurring. Thus, abstinence-based approaches that have predominated in the past would not be well suited to teaching these kinds of skills. Although such an approach with adolescents might be complex and controversial, it is important to consider the possibility if skills deficits are developing during adolescence among these early-onset users. Although such skills might be taught later (e.g. in college), behavioral patterns may be more entrenched, and the adolescent may already have experienced considerable harm that might alter their long-term developmental trajectory. Such an approach does not preclude abstinence-based interventions among those who have not yet begun drinking, but does suggest the need to consider multiple options to meet the needs of the entire population.
Although the current study provides important evidence for a mechanism of risk associated with age of drinking onset, the results should be considered in the context of limitations to the study methodology, including the cross-sectional design, single-campus sample, and lack of collateral reports. The cross-sectional nature of the data makes it impossible to draw any causal inferences about the relations among the study variables. Thus, although the results were consistent with the proposed theoretical model, it is possible that the direction of effects differ in reality from the theoretically proposed direction of effects. Although the sample was reasonably representative of the campus from which it was drawn, and is roughly consistent with national demographic norms for undergraduate students, most participants were relatively light drinkers, so it will be important to replicate the results with heavier drinking samples. Although the self-report nature of the data could lead to inaccuracy due to poor recall or intentional efforts to misrepresent one’s true level of alcohol consumption, there is considerable evidence that self-reports of substance use are accurate when confidentiality is assured, and there is little evidence that collateral reports significantly improve the validity of such data (Babor et al., 2000; LaForge et al., 2005).
Another limitation relates to the low overall response rate and failure of many participants to complete all of the study measures. Although the response rate was relatively low, prior research has shown similar response rates to web-based surveys (McCabe et al., 2006). The low response rate in the current study was likely due, at least in part, to the lottery-based incentives (no guaranteed payment) and the fact that participants were eligible for incentives regardless of whether or not they completed the survey (per human subjects committee recommendations and to avoid coercion). In addition, a response of “I choose not to respond” was provided for each question, resulting in a number of missing cases for specific questions. Although the response rates were less than ideal, participants in the current study are still likely to be more representative of the general college student population than the convenience samples (e.g. undergrad psychology majors) used in many studies of college student behavior. Nonetheless, replication of the results in additional samples will be important.
Despite the aforementioned limitations, the results provide valuable insight with potential implications for prevention and intervention by providing evidence that protective behavioral strategies serve as a mechanism through which age of first use contributes to drinking behavior and alcohol-related negative consequences. Replication of these results in other samples, including adolescents, would further strengthen the argument for tailoring interventions based on age of drinking onset. In particular, it is important to consider the best way to intervene with individuals at heightened risk due to early age of drinking onset. Teaching basic skills for managing behavior (including alcohol use) may have particular utility for this group.
Acknowledgments
Role of Funding Sources
Funding for this study was provided by NIDA Grant # P50-DA 009241 and NIDA Grant # T32-DA07238. NIDA had no role in the study design, collection, analysis or interpretation of the data, writing the manuscript, or the decision to submit the paper for publication.
This research was supported by NIDA Grant # P50-DA 009241 and Grant # T32-DA07238.
Footnotes
Contributors
Rebekka Palmer, William Corbin and Jessica Cronce designed the study and wrote the protocol as a team. Rebekka Palmer conducted literature searches and provided summaries of previous research studies. William Corbin conducted the statistical analysis. Rebekka Palmer and Jessica Cronce wrote the first draft of the manuscript and all authors contributed to and have approved the final manuscript.
Conflict of Interest
There are no conflicts of interest by any of the authors of the submitted manuscript.
Contributor Information
William R. Corbin, Email: William.Corbin@Yale.edu.
Jessica M. Cronce, Email: jcronce@u.washington.edu.
References
- Babor TF, Steinberg K, Anton R, Del Boca F. Talk is cheap: Measuring drinking outcomes in clinical trials. Journal of Studies on Alcohol. 2000;61:55–63. doi: 10.15288/jsa.2000.61.55. [DOI] [PubMed] [Google Scholar]
- Baron RM, Kenny DA. The moderator–mediator variable distinction in social psychological research: Conceptual, strategic and statistical considerations. Journal of Personality and Social Psychology. 1986;51:1173–1182. doi: 10.1037//0022-3514.51.6.1173. [DOI] [PubMed] [Google Scholar]
- Benton SL, Schmidt JL, Newton FB, Shin K, Benton SA, Newton DW. College student protective strategies and drinking consequences. Journal of Studies on Alcohol. 2004;65:115–121. doi: 10.15288/jsa.2004.65.115. [DOI] [PubMed] [Google Scholar]
- Brown SA, Tapert SF. Adolescence and the trajectory of alcohol use: Basic to clinical studies. Annals of the New York Academy of Sciences. 2004;1021:234–244. doi: 10.1196/annals.1308.028. [DOI] [PubMed] [Google Scholar]
- Collins RL, Parks GA, Marlatt GA. Social determinants of alcohol consumption: The effects of social interaction and model status on the self-administration of alcohol. Journal of Consulting and Clinical Psychology. 1985;53:189–200. doi: 10.1037//0022-006x.53.2.189. [DOI] [PubMed] [Google Scholar]
- Core Institute. Validity and reliability Core Alcohol and Drug Survey Long Form. 2005 Retrieved from http://www.core.siuc.edu/files/documents/LongFormReliability2005.doc.
- Delva J, Smith MP, Howell RL, Harrison DF, Wilke D, Jackson SL. A study of the relationship between protective behaviors and drinking consequences among undergraduate college students. Journal of American College Health. 2004;53:19–26. doi: 10.3200/JACH.53.1.19-27. [DOI] [PubMed] [Google Scholar]
- DeWit DJ, Adlaf EM, Offord DR, Ogborne AC. Age at first alcohol use: A risk factor for the development of alcohol disorders. American Journal of Psychiatry. 2000;157:745–750. doi: 10.1176/appi.ajp.157.5.745. [DOI] [PubMed] [Google Scholar]
- Grant BF, Dawson DA. Age at onset of alcohol use and its association with DSb-IV alcohol abuse and dependence: Results from the National Longitudinal Alcohol Epidemiological Survey. Journal of Substance Abuse. 1997;9:103–110. doi: 10.1016/s0899-3289(97)90009-2. [DOI] [PubMed] [Google Scholar]
- Haines MP, Barker G, Rice RM. The personal protective behaviors of college student drinkers: Evidence of indigenous protective norms. Journal of American College Health. 2006;55:69–75. doi: 10.3200/JACH.55.2.69-76. [DOI] [PubMed] [Google Scholar]
- Hawkins JD, Graham JW, Maguin E, Abbot R, Hill KG, Catalano RF. Exploring the effects of age of alcohol use initiation and psychosocial risk factors on subsequent alcohol misuse. Journal of Studies on Alcohol. 1997;58:280–290. doi: 10.15288/jsa.1997.58.280. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Johnston LD, O’Malley PM, Bachman JG, Schulenberg JE. Teen drug use continues down in 2006, particularly among older teens; but use of prescription-type drugs remains high. Ann Arbor, MI: University of Michigan News and Information Services; 2006. Dec 21, Retrieved July 10, 2007, from www.monitoringthefuture.org. [Google Scholar]
- Johnston LD, O’Malley PM, Bachman JG, Schulenberg JE. NIH Publication No. 06-5882. Bethesda, MD: National Institute on Drug Abuse; 2006. Monitoring the Future national results on adolescent drug use: Overview of key findings, 2005. [Google Scholar]
- LaForge RG, Borsari B, Baer JS. The utility of collateral informant assessment in college alcohol research: Results from a longitudinal prevention trial. Journal of Studies on Alcohol. 2005;66:479–487. doi: 10.15288/jsa.2005.66.479. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Martens MP, Taylor KK, Damann KM, Page JC, Mowry ES, Cimini MD. Protective behavioral strategies when drinking alcohol and their relationship to negative alcohol-related consequences in college students. Psychology of Addictive Behaviors. 2004;18:390–393. doi: 10.1037/0893-164X.18.4.390. [DOI] [PubMed] [Google Scholar]
- McCabe SE, Diez A, Boyd CJ, Nelson TF, Weitzman ER. Comparing web and mail responses in a mixed mode survey in college alcohol use research. Addictive Behaviors. 2006;31:1619–1627. doi: 10.1016/j.addbeh.2005.12.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McGue M, Iacono WG, Legrand LN, Malone S, Elkins I. Origins and consequences of age at first drink. I. Associations with substance-use disorders, disinhibitory behavior and psychopathology and P3 amplitude. Alcoholism: Clinical and Experimental Research. 2001;25:1156–1165. [PubMed] [Google Scholar]
- Palmer RS. Unpublished doctoral dissertation. University of Washington; Seattle: 2004. Efficacy of the Alcohol Skills Training Program in mandated and nonmandated heavy drinking college students. [Google Scholar]
- Patock-Peckham JA, Morgan-Lopez AA. College drinking behaviors: Mediational links between parenting styles, impulse control, and alcohol-related outcomes. Psychology of Addictive Behaviors. 2006;20:117–125. doi: 10.1037/0893-164X.20.2.117. [DOI] [PubMed] [Google Scholar]
- Patton JH, Stanford MS, Barratt ES. Factor structure of the Barratt Impulsiveness Scale. Journal of Clinical Psychology. 1995;51:768–774. doi: 10.1002/1097-4679(199511)51:6<768::aid-jclp2270510607>3.0.co;2-1. [DOI] [PubMed] [Google Scholar]
- Pedersen W, Skrondal A. Alcohol consumption debut: Predictors and consequences. Journal of Studies on Alcohol. 1998;59:32–42. doi: 10.15288/jsa.1998.59.32. [DOI] [PubMed] [Google Scholar]
- Simmons JS, Carey KB, Gaher RM. Lability and impulsivity synergistically increase risk for alcohol-related problems. The American Journal of Drug and Alcohol Abuse. 2004;30:685–694. doi: 10.1081/ada-200032338. [DOI] [PubMed] [Google Scholar]
- Snyder TD, Dillow SA, Hoffman CM. Digest of Education Statistics 2007 (NCES 2008-022) Washington, DC: National Center for Education Statistics, Institute of Education Sciences, U.S. Department of Education; 2008. [Google Scholar]
- Tapert SF, Granholm E, Leedy N, Brown SA. Substance use and withdrawal: Neuropsychological functioning over 8 years in youth. Journal of the International Neuropsychological Society. 2002;8:873–883. doi: 10.1017/s1355617702870011. [DOI] [PubMed] [Google Scholar]
- U.S. Department of Health and Human Services. The surgeon general’s call to action to prevent and reduce underage drinking. 2007 Retrieved September 26, 2007, from http://www.surgeongeneral.gov/topics/underagedrinking/ [PubMed]
- Walters ST, Roudsari BS, Vader AM, Harris TR. Correlates of protective behavior utilization among heavy-drinking college students. Addictive Behaviors. 2007;32:2633–2644. doi: 10.1016/j.addbeh.2007.06.022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Warner LA, White HR. Longitudinal effects of age at onset and first drinking situations on problem drinking. Substance Use & Misuse. 2003;38:1983–2016. doi: 10.1081/ja-120025123. [DOI] [PubMed] [Google Scholar]
- White HR, Labouvie EW. Towards the assessment of adolescent problem drinking. Journal of Studies on Alcohol. 1989;50:30–37. doi: 10.15288/jsa.1989.50.30. [DOI] [PubMed] [Google Scholar]