

Abstract
Objective
To examine 3-dimensional lower-extremity joint kinematics and muscle activity during cycling with and without a shank guide for a single subject with spastic diplegic cerebral palsy (CP).
Design
Single case.
Setting
Pediatric referral hospital.
Participant
A 13-year-old adolescent with spastic diplegic CP and limited ambulation abilities.
Interventions
Not applicable.
Main Outcome Measures
Kinematic data were collected for 6 joint motions and electromyographic data for 7 muscles during 10- to 15-second trials. Average variability in the kinematic curves was calculated, and kinematic and electromyographic data were analyzed descriptively.
Results
With the guide, the subject cycled at 40.1±2.0rpm compared with 13.7±4.0rpm without it. In addition, there was less variability in the kinematic curves (P=.03) and muscles tended to turn on sooner and off later. These results indicate that this subject could cycle faster with the guide, which is desirable for cardiovascular health, and that there was a possible increase in motor control due to reduced needs to control excessive joint motions.
Conclusions
Based on these findings, a shank guide may allow some people with CP to cycle faster and provide improved joint kinematics.
Keywords: Biomechanics, Cerebral palsy, Disabled children, Exercise, Rehabilitation
Stationary cycling is frequently used in a rehabilitation setting as an active warm-up or to improve range of motion, strength, and cardiovascular conditioning. For people with neurologic dysfunction, adaptations to the cycle are often needed in order to allow effective cycling and may include alterations to the seat and pedals as well as adding a restraint system with straps.1 For children with CP, specific adaptations may be needed due to additional impairments, such as lower-extremity deformities. These adaptations may also limit the degrees of freedom of the task, potentially allowing them to cycle vigorously enough to have an impact on the cardiorespiratory system.
A recent study by Williams and Pountney2 examined the outcomes of a 6-week cycling intervention with an adapted cycle for children with CP classified as levels IV and V using the GMFCS. This adapted cycle had anterior and lateral trunk supports, wrist supports, specialized footplates, and ankle straps, but no guide to support the lower extremity in the frontal or transverse planes. After the intervention, the children showed increases in their Gross Motor Function Measure scores and cycling duration, as well as in the cycling cadences and resistances used. It is unknown if cycling biomechanics changed as a result of participation, which may be important to understand because children and adolescents with CP have altered cycling biomechanics, compared with their typically developing peers. These alterations include increased muscle cocontraction,3,4 decreased smoothness of the cycling pattern as indicated by an uneven amount of time spent in each quadrant,3 altered joint kinematics,4 and decreased cycling efficiency.4
Our previous work5 showed that the use of a shank guide designed to limit motion in the frontal and transverse planes during cycling in adolescents with CP led to improvements in joint kinematics during cycling but had minimal impact on the onset and offset of muscle activity and no impact on muscle cocontraction for subjects classified as GMFCS levels III and IV. The purpose of this case report is to describe the biomechanical findings of cycling with and without a shank guide for a subject classified as GMFCS level IV, who had difficulty with the cycling task, and who appeared to benefit more from the shank guide than indicated by our previously reported group data.
METHODS
Participant
The subject in this report was a 13-year-old girl with spastic diplegia, classified as level IV using the GMFCS. She ambulated with bilateral Lofstrand crutches for short distances but used a manual wheelchair for longer distances and all community mobility. She reported that she had cycled with assistance as a young child during physical therapy but had not cycled in many years. She weighed 58.8kg and was 158cm tall. After receiving information about the study, the subject and her mother signed institutional review board–approved assent and consent forms, respectively.
Cycle and Shank Guide
A free-standing recumbent stationary cyclea was used in this study (fig 1). The cycle pedals had a full footplate, and the pedal spindle was located approximately at the height of the lateral malleolus, and the resistance set at 3.8Nm.4 The cycle has no seat, so the subject sat on a therapy benchb attached to the cycle through an adjustable bar and held handgrips attached to the bench. The distance of the seat and seat back from the cycle and the crank arm length were set based on anthropometrics.4 The second metatarsal head was aligned with the pedal spindle to maximize ankle power,6 which was set by manipulating the footplate fastened with self-adhesive (Velcro) to the pedal. In addition, the footplate was positioned to allow her feet to be externally rotated in relation to her shank to accommodate for tibial torsion and foot deformities. This change in foot position aligned her knee with the direction of movement of the pedals (knee facing forward).
Fig 1.
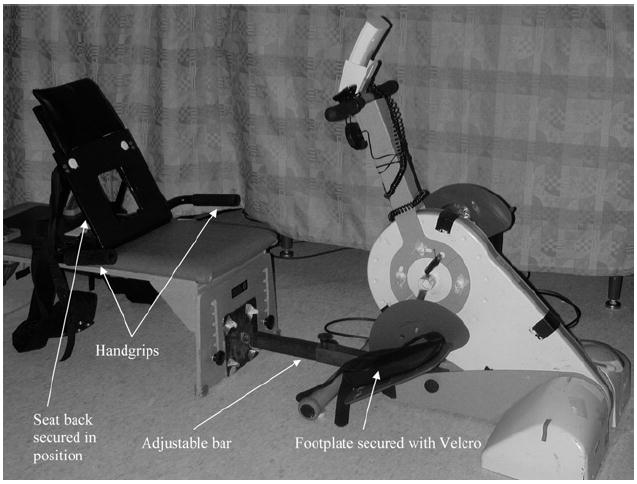
Cycle design.
The cycle provided the ability to use a shank guide (fig 2) on the lateral shank to limit the motion of the lower extremity. The guide was attached to the pedal surface with a ball and socket joint, thus providing movement in any direction. The subject’s shank was secured to the guide with a self-adhesive strap and once the desired position of the lower extremity was achieved, the screws on the ball and socket joint were tightened to prevent any movement of the guide on the pedal. In this study, the guide was primarily used to limit the excursion of the lower extremity in the frontal and transverse planes. In the sagittal plane, the guide was positioned to attempt to maintain the ankle in approximately 15° of plantarflexion when held in a static position (without the pedals moving).5
Fig 2.
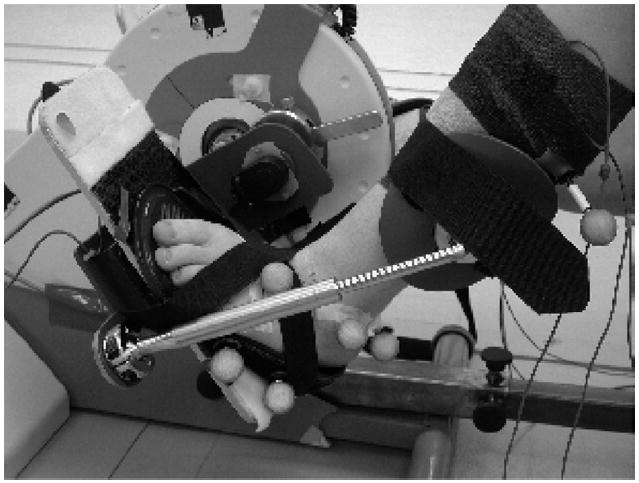
Placement of the shank guide during testing.
Training
The subject received 2 practice sessions of approximately 20 minutes each, with 1 session conducted in the morning and the second in the afternoon of the same day. She was instructed to pedal as fast as she was able in these sessions and was permitted to rest as needed. During the first practice session, she cycled without the shank support. During the second session, she practiced cycling with the shank guide. All cycling was done with the subject barefoot.
Data Collection
Data collection occurred the next day and included left lower-extremity kinematics and muscle activity using electromyography, which were collected in a motion analysis laboratory. Six trials of 10 to 15 seconds in duration were performed, 3 with the shank guide and 3 without the guide. The 0° position of the crank revolution was defined as the crank arm being horizontal and farthest from the subject.4
Kinematic Evaluation
Three-dimensional kinematics of the hip, knee, and ankle were collected using a 7-camera Vicon 370 motion analysis systemc using a standard marker set.7 Data were collected at 60Hz and digitally filtered (6-Hz low-pass filter). To detect crank arm position, the voltage change of a rotary encoderd on the crank axis was measured in 0.3° increments. Data were synchronized and processed using customized software using Vicon Plug-in-Gait, Version 1.9, Build 051.c Kinematic data were normalized to 1° increments of the crank position.
Electromyography
Surface electromyographic data were collected from 7 muscles6 (rectus femoris, vastus lateralis, medial hamstrings, biceps femoris, anterior tibialis, lateral gastrocnemius, soleus)8-10 at 1200Hz using a Motion Lab Systems MA-300 surface electromyography recording system and MA-310 electrodes.e Noise was eliminated by subtracting quiet baseline values. Electromyographic data were digitally filtered using a band-pass filter of 20 to 350Hz, and onset and offset of muscle activity were determined as previously described using the rule of the muscle being active when the electromyographic activity was 3 SDs above the quiet baseline.4 Crank positions for the onset and offset of muscle activity were determined in 0.3° increments.
Data Analysis
For the kinematic data, average variability of 2 kinematic curves was determined for each of 6 joint motion pairs studied (hip flexion and extension, hip adduction and abduction, hip internal and external rotation, knee flexion and extension, knee varus and valgus, ankle dorsiflexion and plantarflexion) by taking the square root of the average variance within each of the 2 revolutions. The average variance provides information as to how the values differ during a revolution. The variability data were combined across the joint motions due to the small number of revolutions and were then compared between conditions using a paired t test. For the electromyographic and kinematic data, a descriptive analysis of differences between conditions was performed, and previously collected cycling biomechanics data for adolescents with typical development were used as the reference for typical cycling biomechanics.4
RESULTS
The subject had difficulty cycling without the guide, as indicated by a nonsmooth cycling pattern with starts and stops during the revolution. Four cycling revolutions with complete data were obtained for each condition (with and without the shank guide). Data from more revolutions were collected; however, only 4 revolutions were usable due to problems with the cameras visualizing the ankle and foot markers during the remaining revolutions. The average cadence for these 4 revolutions was 40.1±2.0rpm with the guide and 13.7±4.0rpm without it. From the 4 revolutions, 2 representative revolutions were selected for each condition for comparison.
When cycling with the guide, joint motion changed direction less frequently (fig 3), and there was less variability (P=.03) within the kinematic curves (table 1). The guide also helped maintain the hip in abduction as opposed to the adduction that was seen without the guide. Overall, the joint angles obtained during cycling were more similar in magnitude to those of adolescents with typical development for hip abduction and adduction, knee flexion and extension, and ankle dorsiflexion and plantarflexion, but not for hip flexion and extension, hip internal and external rotation or knee varus and valgus. Joint excursions appeared to decrease for hip abduction and adduction, knee flexion and extension, knee varus and valgus, and ankle dorsiflexion and plantarflexion, but not the other motions, when cycling with the guide.
Fig 3.
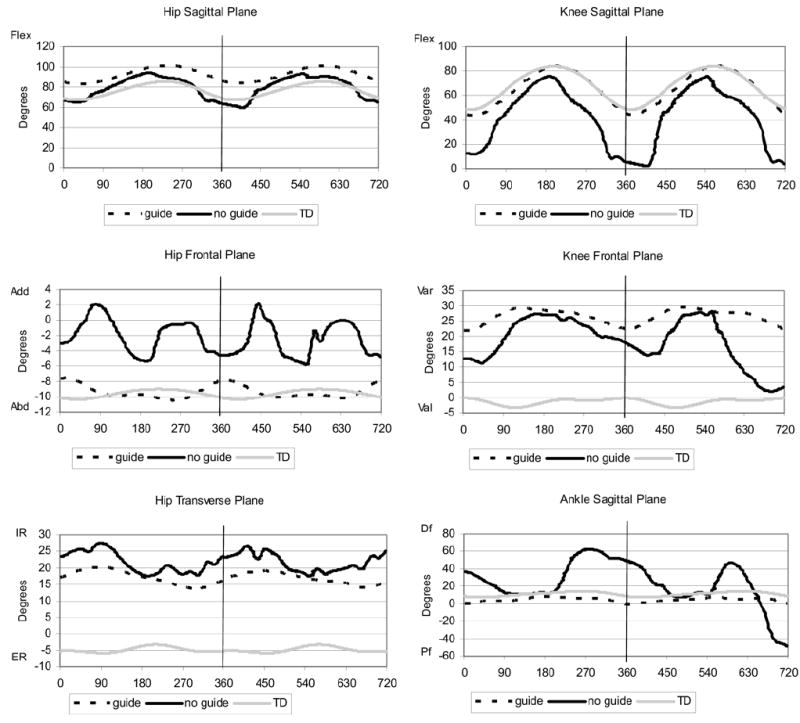
Kinematic plots with and without the guide. The x axis indicates the position of the crank arm and the y axis indicates the degrees of motion. Abbreviations: Abd, abduction; Add, adduction; Df, dorsiflexion; ER, external rotation; Flex, flexion; IR, internal rotation; Pf, plantarflexion; TD, typically developing; Val, valgus; Var, varus.
Table 1.
Variability (square root of the average variance) of the Kinematic Curves
| Curve | No Guide | Guide |
|---|---|---|
| Hip sagittal plane | 10.87 | 6.36 |
| Hip frontal plane | 2.18 | 0.85 |
| Hip transverse plane | 3.02 | 1.90 |
| Knee sagittal plane | 24.17 | 14.27 |
| Knee frontal plane | 6.89 | 2.37 |
| Ankle sagittal plane | 21.93 | 2.49 |
NOTE. Using a paired t test, there was a difference in variability when cycling with versus without the guide (P=.03) when examining all joint motions as a group.
The electromyographic data (fig 4) showed that muscles tended to turn on sooner and off later when cycling with the guide. In looking at the electromyographic plots, it appears that more phasic muscle activity was seen when cycling without the guide, primarily for the vastus lateralis and the anterior tibialis muscles. The pattern of activity of the biceps femoris also differed when cycling with versus without the guide. In addition, amplitude differences appeared to be present for the vastus lateralis, medial hamstrings, and gastrocnemius muscles with greater amplitudes when cycling with the guide.
Fig 4.
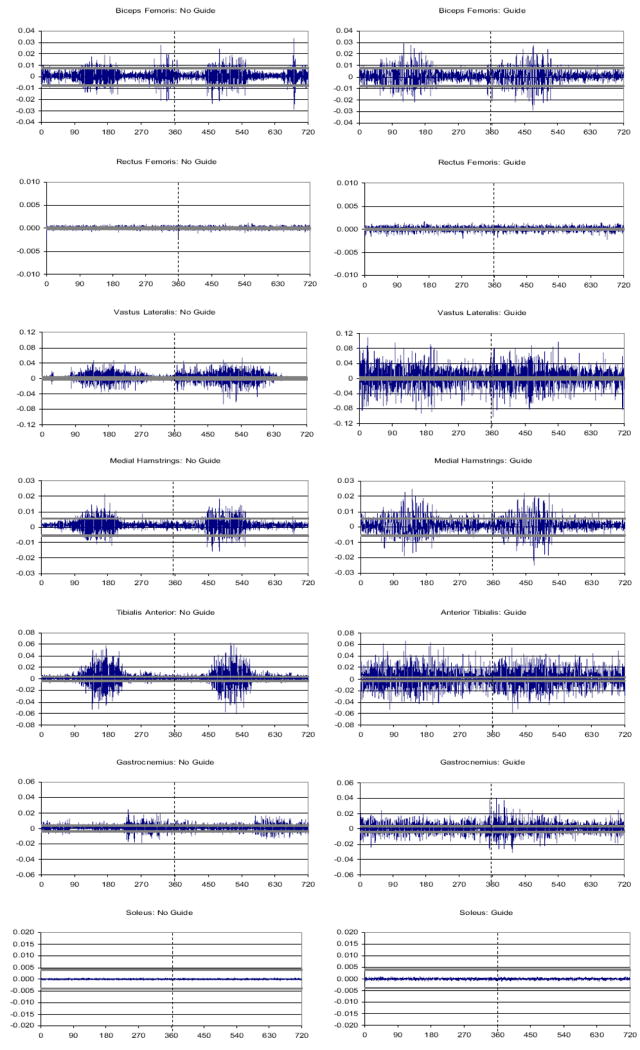
Electromyographic plots with and without the guide. The x axis indicates the position of the crank arm and the y axis indicates the electromyographic voltage. The solid gray bars represent 3 SDs above and below the quiet baseline activity. A muscle was determined to be active when activity occurred that was greater than 3 SDs from the mean.
DISCUSSION
For this subject, cycling with the guide allowed her to achieve a faster cycling cadence, which differs from what was seen with our previously reported group data5 in that all of the other children could achieve similar cadences with and without the guide. Higher cadences can lead to higher peak heart rates, which in turn place greater stress on the cardiovascular system. Because some children with CP have difficulty obtaining sufficient exercise, the guide may be useful for these children to increase their exercise intensity to improve their overall cardiorespiratory fitness.11
Cycling with the guide led to joint angles that better approximated the angles obtained by adolescents with typical development for some joint motions. The guide did not appear to have an impact on hip internal and external rotation or knee varus and valgus. Although they were not measured in this study, it is possible that anatomical differences such as ante-version or a varus deformity may have contributed to the lack of effect. In this study, the subject was able to achieve a smoother cycling pattern with less variability of joint motion when cycling with the guide. Variability can be seen as a measure of stability of the sensorimotor system,12 thus potentially indicating greater motor control. The increase in motor control may be due to the reduction in the need to control excessive joint motions that are counterproductive to cycling, thus decreasing the degrees of freedom of the task. In this subject, the excessive joint motions were likely due to decreased strength and to spasticity, which are common impairments in people with CP. In addition, children with CP have difficulty activating muscles in the proper sequence during functional activities and often lack the ability to produce postural compensations for these abnormal patterns.13 The guide may have assisted this subject with the cycling motion by decreasing the need for postural compensations that would be required to maintain the lower extremities in a more desirable position for cycling.
With the guide, this subject showed longer periods of muscle activity, and less phasic activity was visible for some muscles. Differences in activity of the anterior tibialis may be related to differences in plantarflexion angle achieved with and without the guide, because children show prolonged activity of muscles around the ankle when walking faster.14 However, many of the differences seen may be due to the differences in cycling cadence achieved with and without the guide, because our earlier work showed increases in the duration of muscle activity for children with CP when cycling at higher cadences.4 This finding is consistent with other work that found increased muscle cocontraction during faster movements of the shoulder and elbow.15 In adults without disability, higher cycling cadences lead to increased hip moments, which are attributed to increased acceleration and deceleration of the hip.16 Because children with CP have difficulty with acceleration during fast movements, muscle activity for our subject may have needed to increase to meet this demand when cycling at the faster cadence with the guide. Our earlier work with a larger sample size showed minimal and not clinically significant differences in electromyographic activity when cycling with and without a guide5; therefore cadence may be more likely to be the reason for the electromyographic differences seen in this subject.
Muscle activity may also have been impacted by the novelty of the task for this subject. Novice cyclists without disability, but not highly trained cyclists, have been shown to increase the amplitude and duration of muscle activity when cycling at higher speeds, thus suggesting less developed control of muscle recruitment.17 Therefore, the prolonged muscle activity seen in our subject may have been related to decreased motor control when trying to move more quickly during this novel task. Another study examined differences in cocontraction between low-skilled and high-skilled children during the preparatory phase of a drop jump and found that the low-skilled children displayed greater cocontraction, which may be due to immature feed-forward control strategies. It was suggested that with repetition, these strategies may improve.18 In our subject, similar immaturity may have impacted the results. Future work should examine the effect of cycling practice on muscle activity for children with CP.
Study Limitations
As a case report, this study has inherent limitations; thus its findings may not be applicable to a larger population. Another limitation of this study is the setting of the ankle position when using the guide. Although the ankle was positioned statically at 15°, the subject did not maintain this position while cycling. However, setting the ankle statically at this joint angle allowed her to obtain ankle joint angles during cycling that were similar to what was seen in adolescents with typical development when cycling without a guide. In addition, this study was a biomechanical study; therefore the impact of the guide on a cycling intervention for children with CP can only be surmised at this time. Future work should examine the cardiorespiratory and musculoskeletal effects of cycling with the guide.
CONCLUSIONS
A shank guide that was designed to better align the legs for cycling allowed this subject with CP to cycle faster and show joint kinematics closer to those seen in adolescents with typical development. Muscles turned on sooner and off later with the guide for this subject, which may have been due to the faster cycling cadence that was achieved. Based on these findings, a shank guide may be useful for some adolescents with CP in order to allow faster cycling cadences and improved joint kinematics. Faster cycling may lead to greater cardiorespiratory benefits.
Acknowledgments
Supported by Shriners Hospitals for Children (grant no. 8530), the Pediatric Section of the American Physical Therapy Association (clinical research grant), and the National Institutes of Health (grant no. HD043859).
List of Abbreviations
- CP
cerebral palsy
- GMFCS
Gross Motor Function Classification System
Footnotes
Restorative Therapies Inc, 907 Lakewood Ave, Baltimore, MD 21224.
Kaye Products, 535 Dimmocks Mill Rd, Hillsborough, NC 27278.
Vicon Motion Systems, 9 Spectrum Pointe Dr, Lake Forest, CA 92630.
US Digital Corp, 1400 NE 136th Ave, Vancouver, WA 98684.
Motion Lab Systems, 15045 Old Hammond Hwy, Baton Rouge, LA 70816.
No commercial party having a direct financial interest in the results of the research supporting this article has or will confer a benefit on the authors or on any organization with which the authors are associated.
References
- 1.Fujiwara T, Liu M, Chino N. Effect of pedaling exercise on the hemiplegic lower limb. Am J Phys Med Rehabil. 2003;82:357–63. doi: 10.1097/01.PHM.0000064722.01940.E4. [DOI] [PubMed] [Google Scholar]
- 2.Williams H, Pountney T. Effects of a static bicycling programme on the functional ability of young people with cerebral palsy who are non-ambulant. Dev Med Child Neurol. 2007;49:522–7. doi: 10.1111/j.1469-8749.2007.00522.x. [DOI] [PubMed] [Google Scholar]
- 3.Kaplan SL. Cycling patterns in children with and without cerebral palsy. Dev Med Child Neurol. 1995;37:620–30. doi: 10.1111/j.1469-8749.1995.tb12050.x. [DOI] [PubMed] [Google Scholar]
- 4.Johnston TE, Barr AE, Lee SC. Biomechanics of submaximal recumbent cycling in adolescents with and without cerebral palsy. Phys Ther. 2007;78:572–85. doi: 10.2522/ptj.20060261. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Johnston TE, Barr AE, Lee SC. Biomechanics of recumbent cycling in adolescents with cerebral palsy with and without the use of a fixed shank guide. Gait Posture. 2008;27:539–46. doi: 10.1016/j.gaitpost.2007.07.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Ericson MO, Nisell R, Arborelius UP, Ekholm J. Muscular activity during ergometer cycling. Scand J Rehabil Med. 1985;17:53–61. [PubMed] [Google Scholar]
- 7.Davis RB, Ounpuu S, Tyisurski D, Gage JR. A gait analysis data collection and reduction technique. Hum Mov Sci. 1991;20:575–87. [Google Scholar]
- 8.Jorge M, Hull ML. Analysis of EMG measurements during bicycle pedalling. J Biomech. 1986;19:683–94. doi: 10.1016/0021-9290(86)90192-2. [DOI] [PubMed] [Google Scholar]
- 9.Raasch CC, Zajac FE. Locomotor strategy for pedaling: muscle groups and biomechanical functions. J Neurophysiol. 1999;82:515–25. doi: 10.1152/jn.1999.82.2.515. [DOI] [PubMed] [Google Scholar]
- 10.Ericson MO. Muscular function during ergometer cycling. Scand J Rehabil Med. 1988;20:35–41. [PubMed] [Google Scholar]
- 11.Centers for Disease Control and Prevention and President’s Council on Physical Fitness and Sports. Healthy People 2010. Physical activity and fitness. [Aug 24, 2006]; Available at: http://www.healthypeople.gov/Document/pdf/Volume2/22Physical.pdf.
- 12.Newell KM, Corcos DM. Issues in variability and motor control. In: Newell KM, Corcos DM, editors. Issues in variability and motor control. Champaign: Human Kinetics; 2003. pp. 1–12. [Google Scholar]
- 13.Giuliani CA. Dorsal rhizotomy for children with cerebral palsy: support for concepts of motor control. Phys Ther. 1991;71:248–59. doi: 10.1093/ptj/71.3.248. [DOI] [PubMed] [Google Scholar]
- 14.Detrembleur C, Willems P, Plaghki L. Does walking speed influ-ence the time pattern of muscle activation in normal children? Dev Med Child Neurol. 1997;39:803–7. doi: 10.1111/j.1469-8749.1997.tb07546.x. [DOI] [PubMed] [Google Scholar]
- 15.Suzuki M, Shiller DM, Gribble PL, Ostry DJ. Relationship between cocontraction, movement kinematics and phasic muscle activity in single-joint arm movement. Exp Brain Res. 2001;140:171–81. doi: 10.1007/s002210100797. [DOI] [PubMed] [Google Scholar]
- 16.Redfield R, Hull ML. On the relation between joint moments and pedalling rates at constant power in bicycling. J Biomech. 1986;19:317–29. doi: 10.1016/0021-9290(86)90008-4. [DOI] [PubMed] [Google Scholar]
- 17.Chapman AR, Vicenzino B, Blanch P, Hodges PW. Leg muscle recruitment during cycling is less developed in triathletes than cyclists despite matched cycling training loads. Exp Brain Res. 2007;181:503–18. doi: 10.1007/s00221-007-0949-5. [DOI] [PubMed] [Google Scholar]
- 18.Hamstra-Wright KL, Swanik CB, Sitler MR, et al. Gender comparisons of dynamic restraint and motor skill in children. Clin J Sport Med. 2006;16:56–62. doi: 10.1097/01.jsm.0000179232.10261.65. [DOI] [PubMed] [Google Scholar]