

Abstract
Traditionally, radiology has been conceived as a support department providing patient scanning services to the other clinical departments in a hospital. However, recent advancements in networking technology and related information systems such as picture archiving and communication system (PACS) and radiology information system (RIS) provide new opportunities for inventing different types of diagnostic imaging businesses such as teleradiology. In this article, we examined the business processes of currently operating imaging centers and proposed a prototype of an information system that can facilitate their workflows in a more efficient way. The principal component of our proposed system is a report management module built on extensible markup language (XML) technologies that allows much flexibility and convenience for both imaging technicians and radiologists.
Key Words: Diagnostic imaging, XML, web technology, radiology information system, XForm
Introduction
Information technology (IT) has had a huge impact on the proliferation of various industrial sectors in the 21st century. The medical/dental industry was not an exception. Digital images of unimaginably high resolution have been made available with the help of recent technical developments in imaging devices such as computed tomography (CT), magnetic resonance imaging (MRI), and positron emission tomography (PET), and the abundance of diagnostic information in those images enables radiologists to make more accurate diagnostic decisions for patients. Moreover, the workflow of obtaining, reconstructing, manipulating, and analyzing those digital images has been growing more efficient through the use of a variety of information systems.1,2 That is, the quality of digital images and the efficiency of the workflow in handling those images are now considered to be crucial factors in achieving competitiveness in the diagnostic imaging industry.
Figure 1 illustrates a typical diagnostic imaging workflow in a radiology department of a hospital. This is one of the integration profiles, called “Scheduled Workflow,” which were developed by Integrating the Healthcare Enterprise (IHE) to define the core process of a hospital. IHE is a joint initiative formed by the Radiological Society of North America (RSNA) and the Healthcare Information and Management Systems Society (HIMSS).3,4 Workflow is usually supported by information systems such as hospital information system (HIS), picture archiving and communication system (PACS), and radiology information system (RIS). HIS, which usually consists of order communication system (OCS) and electronic medical record (EMR), registers patients and manages electronic charts to keep track of their medical treatment. HIS is also used to place imaging orders, which are conveyed to RIS.
Fig 1.
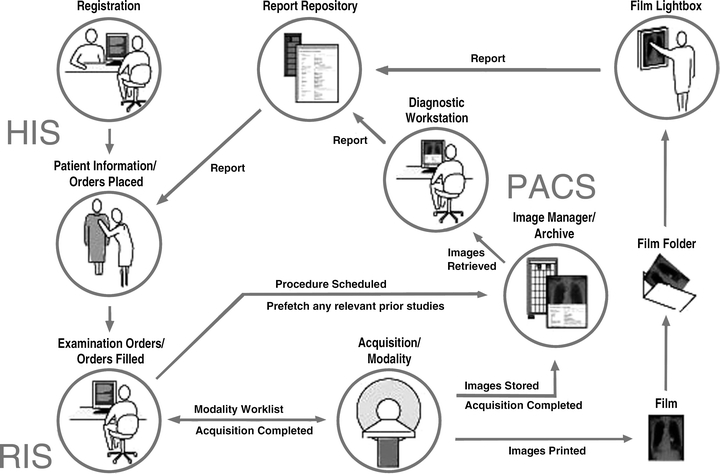
Typical imaging service in a hospital (source: http://www.ihe.net).
RIS controls the status of the imaging orders. Based on the orders placed, RIS creates work lists for each imaging technician. Subsequently, technicians check their work schedule by using RIS, and perform imaging to obtain digital images of patients as scheduled. The images are transferred to PACS, which is digital storage for archiving large volumes of images acquired by various imaging devices. As shown in the figure, PACS/RIS is a core component of digital image exchange within a hospital.
The functionalities of PACS/RIS are not restricted to operate only in a hospital. Every computer system, if it is compatible with the digital imaging and communications in medicine (DICOM) protocol, can communicate with PACS.5 Moreover, if wide-area network (WAN) communication technology is augmented to PACS, then that portion of PACS could be called teleradiology.1
Meanwhile, with regard to security and privacy, the Health Insurance Portability and Accountability Act (HIPAA) regulations came into effect in 1996, and many HIPAA-compliant software programs are now on the market.6,7 As geographical restrictions and possible security problems can be overcome, diagnostic imaging services are gradually considered as an independent business model. In the following section, we will take a closer look at the business process of imaging centers that make profits by providing diagnostic imaging service.
Web-based Imaging Service in Imaging Centers
Imaging centers for outpatients are the fastest growing segment of the global radiology market. Many imaging centers are now in business and providing their own specialized imaging service. They usually offer high-priced specialized imaging modalities for detecting particular diseases, such as mammography for breast cancer, positron emission tomography (PET) for cancer screening of seniors, dental CT scans for implant planning, and others. At present, there are more than 5,000 imaging centers and 3,000 community hospitals with stand-alone imaging departments in the United States. The number of imaging centers has increased by 12–15% annually for the past 3 years, and this strong growth is expected to continue.8
Figure 2 illustrates the typical business process of imaging centers. As shown in the figure, to streamline the business process, PACS/RIS and the related systems are playing a central role. Because the primary goal of the imaging centers is to provide their customers with high-quality diagnostic reports as quickly as possible, PACS/RIS for imaging center requires slightly different features from those of the typical systems used in a typical hospital.
Fig 2.
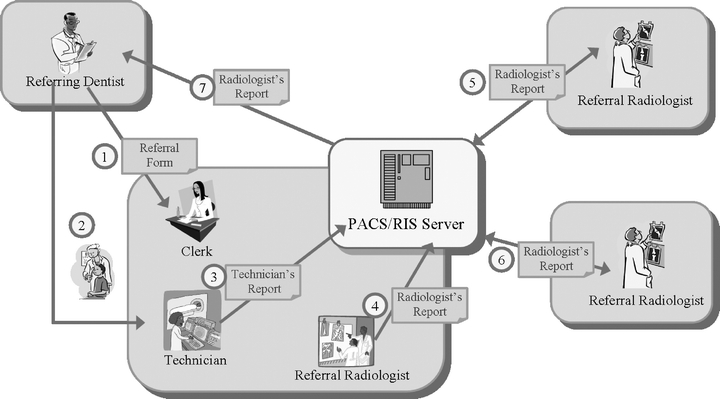
Business process in imaging center.
Support for Web-based Services
The first thing that we have considered is about providing the services through the Web. The customers of imaging centers are usually clinicians of local clinics. To make a request of an imaging service, instead of making a phone call or sending a fax, it would be more convenient for them to access an imaging center web site and to fill out a referral form. They also may need an option to choose a preferred day for imaging, and, if necessary, they may want to upload the previous treatment records of their patients. After the schedule is confirmed, the patients and the referring clinicians can be notified of the confirmed schedule by e-mail, or would like to check it by themselves through the imaging center’s web-based RIS system.
In the mean time, to improve the reliability of imaging centers diagnostic reports, external radiologists are usually consulted. In this case, the external radiologist needs to have access to related images and reports created by the imaging center. For that purpose, the diagnostic reports need to be easily published and shared, or, sometimes, edited by the external radiologists. The most efficient way to do this is providing the Web-based service.
Support for Flexible Report Management
In general, the types and number of images included in a diagnostic report vary according to the diagnostic protocol used. For example, orthodontic protocol requires a different set of images from implant protocol. In addition, imaging centers and referring clinics each have their own preferred format in which the report is to be delivered. Many different kinds of diagnostic reports need to be produced in a short time. From our experience, most imaging technicians want to complete one report in about 10 min. Therefore, to improve their job performance, it is important to provide them with effective means to edit or customize the layout and style of reports. More importantly, to make the report editing process more efficient, diagnostic work stations, which are used to generate images, need to be tightly integrated with the report editing functions.
Methodology: XML Forms as Building Blocks of RIS
We investigated the business process of imaging centers, and found that, to streamline their process, they are required to provide imaging services over the Internet. In the literature, we could find several attempts to share patient information over the internet (Jane et al, in their paper, provided a nice review of several related works), but most of them were focused on development of an underlying canonical model to provide an integrated view of patient data from the heterogeneous, distributed databases.6
Our focus is on development of an efficient and flexible working environment that can improve flexibility and efficiency in creating, storing, and exchanging diagnostic reports. To meet these needs, we considered XForms standard.
“XForms” is W3C (WWW Consortium)’s name for a specification of Web forms that can be used with a wide variety of platforms including desktop computers, handhelds, information appliances, and even paper. Traditional HTML Web forms do not separate the purpose from the presentation of a form. XForms, in contrast, are composed of separate sections that describe what the form does, and how the form looks. This allows for flexible presentation options, including classic XHTML forms, to be attached to an XML form definition.9
Report Structure Based on XForms
The design philosophy in XForms provides good features for separating the management of report contents from their presentation style.
Figure 3 shows the structure of a diagnostic report used in our system. As shown in the figure, a diagnostic report consists of three separate components: the data model, the control layout, and binding information.
Fig 3.
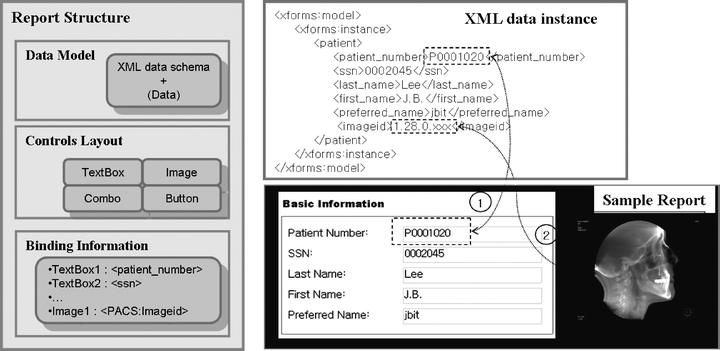
Report structure.
The data model represents the schema of the data content to be contained in the report. Data contents usually include image data and textual data such as patient information, measurements, comments, and diagnostic impressions. The data contents are organized according to that schema in XML. Data contents are displayed in graphical user interface (GUI) objects. Such GUI objects include text boxes, combo boxes, image boxes, tables, and related components. The control layout determines the kinds of GUI objects that are used and how they are arranged in a report. The reference relationship is established between GUI objects and their corresponding data contents through binding information.
For instance, suppose that a user designs a simple report that shows basic patient information and a principal image. The data contents of the report will be described in XML as shown in the figure. In the figure, arrow (1) shows the reference relationship between “Patient Number” in the XML document and the text box displaying the data element. Similarly, arrow (2) denotes the binding relationship between “image ID” and the corresponding image box.
Our report structure makes it possible to store data contents in different repositories from those of controls layout and binding information. That is, the XML data instance itself does not contain such information related to formatting a report. Moreover, with regard to images and patient information, the XML data instance has only reference for them. The reference information is used to locate the corresponding image data or patient data in the PACS database. That is, the XML data instance does not contains any actual data contents in the PACS database. This implies that the data components of a diagnostic report are physically distributed, and that the report is assembled dynamically on request. For example, when a user requests a report for browsing its data contents, RIS extracts the required data contents by using the reference information in the XML data instance, and fill out the report.
Benefits of “Separation of Concern”
This separation of concern provides many benefits in handling large volumes of data in reports.10 First of all, modification of data content has no effect on the reports that contain the data content. That is, reports are protected from unidentified variation of their contents. For example, even if a certain patient’s personal information has changed, it is not necessary to update the information in every report that contains the information. Similarly, users can design many different versions of a report, each version having a different presentation style for the same data content.
Secondly, searching reports can be performed more efficiently. Because XML is a semistructured data model, users can use the semantics incorporated into the XML elements when performing searches. XPath or XQuery, which are devised to facilitate locating and searching XML elements, can be employed to provide more convenient methods of searching reports.11,12 The use of XML-based text mining platforms not only simplifies the process of information retrieval, but also empowers researchers to explore the complex relationships that exist among diagnostic results in the report repository.7
Finally, this approach has advantage in reducing the size of storage. In many cases, one patient has many different reports. As explained earlier, by storing one piece of information at one physical location, data redundancy can be effectively avoided, and the size of storage can be considerably reduced.
Report Designer
A report template, the term we will use to describe a file that has not yet been filled with data instances, can be designed using a dedicated tool called “Report designer.” Many commercial solutions supporting the XForms have their own report template design tools. Those tools provide users with a convenient working environment, as shown in Figure 4 (in the figure we used xForm™ by Maxtron).
Fig 4.
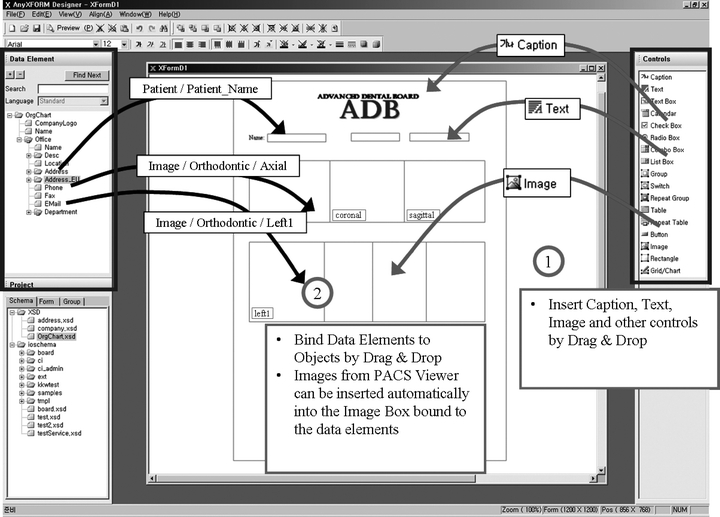
Report designer.
In the figure, the bold outlines on the left- and right-hand sides denote a data model and GUI objects, respectively. The data model is generated in conjunction with the schema of the PACS database. Initially, a user selects the GUI objects he wants to use and arranges them in the empty template (1), and then he binds the data elements in the data model to the corresponding controls by dragging and dropping the elements on the controls (2).
System Architecture and Implementation
We designed and implemented a prototype system that can support the proposed report structure. Figure 5 illustrates the architecture of the proposed system. On the client side, there are three modules: “Report designer,” a diagnostic work station, and “Report editor.” “Report editor” on the client side is implemented as a dynamic linked library (DLL) to be integrated into the diagnostic work station module. On the server side, we have PACS, RIS, and “Report editor,” which are provided as an ActiveX™ implementation to be available in a web browser.
Fig 5.
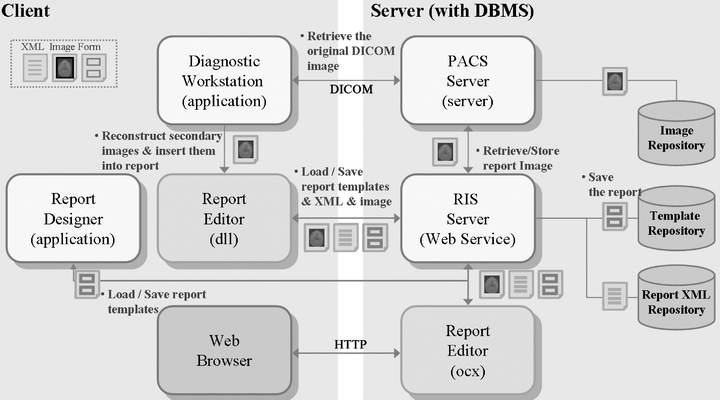
System architecture.
RIS with Report Editor
Fundamentally, RIS is a web-based system that performs order scheduling, work list management, and report management. In terms of implementation, RIS is a collection of web pages and Web services implemented on a web server. To implement the RIS Web services, we exploited functions provided by commercial DBMS. Many recent commercial DBMS provide methods to access their internal stored procedures through a Web service protocol. That is, by sending a simple object access protocol (SOAP) request, relations in DBMS can be accessed, and the results are delivered in the form of a SOAP message.13
As mentioned earlier, data contents and report templates are managed in separate repositories. Those repositories can be accessed by using the Web services implemented on RIS. For example, by using those Web services, “Report designer” downloads report templates for editing.
To make a diagnosis report visible and editable in a web browser, RIS uses “Report editor” implemented as an ActiveX control. As shown in Figure 5, when a user requests a certain report, the “Report editor” control is downloaded to the user’s web browser. In the browser, “Report editor” accesses the Web services of RIS to download the template of the report to be edited. Data instances, including image data that will be inserted into the XML data model in the template, are also retrieved from the PACS database by using those Web services. After all the data contents are obtained, “Report editor” stylizes the XML data instance by using the information contained in the template of the report. XML data instances can be easily visualized by means of the extensible stylesheet language transformation (XSLT) and the scalable vector graphics (SVG) standard employed by “Report editor.”14
Diagnostic Work station with Report Editor
Diagnostic work station is diagnostic software that uses various sophisticated image analysis tools such as 3D visualization, image reconstruction, measurements, and many others to manipulate original images in PACS. Using these tools, radiologists can finally create a diagnostic report summarizing their final diagnostic impressions and including the principal images for reference. The final reports are transferred to HIS, and managed together with the electronic chart of the corresponding patient.
Diagnostic work station is integrated with the DLL version “Report editor.” We used Accurex™ by CyberMed for the diagnostic work station. Figure 6 shows the working environment of Accurex. After creating images used for a diagnosis report, (1) a user invokes “Report editor” to download a corresponding report template. By using the drag-and-drop interface, the user is able to insert images generated by Accurex into the empty slots in the template. The user also can modify the presentation style of the GUI objects (2, 3). After all of the images and relevant information has been filled out, data in the reports are transferred to RIS and stored in the corresponding repository.
Fig 6.
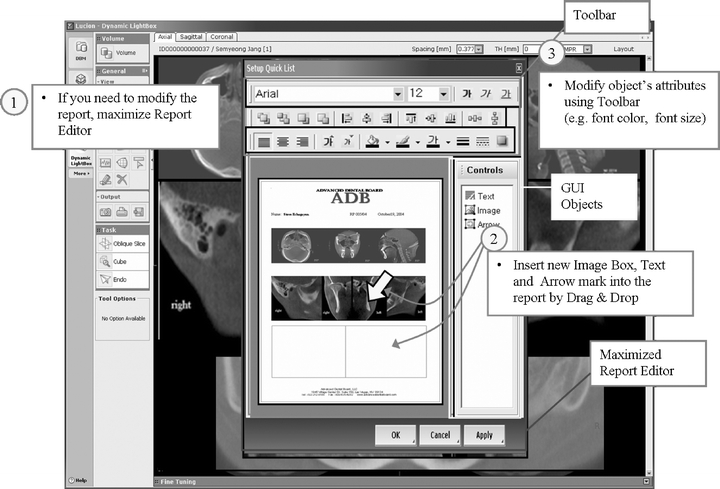
Report editing.
Conclusion
With the help of the recent development in fast network and compression techniques, a very large volume of image data can be transferred anywhere (and everywhere) on the Internet within a reasonable amount of time. These technical advancements envision a future of diagnostic imaging services that overcome geographical constraints and enable a real teleradiology. These changes will accelerate development of more specialized, more distinctive services in diagnostic imaging, and therefore competitive IT infrastructure that supports easy and efficient collaboration through networks will be increasingly required.
In this article, we have examined and analyzed the business processes of imaging centers that are currently providing imaging services. From our examination, we were able to identify several important requirements for providing successful imaging services through the Internet. To successfully meet those requirements, we have considered a more efficient method to manage and share diagnostic information in a collaborative manner. As a result, we have proposed a PACS/RIS system equipped with an efficient report management module based on the XForms standard.
The proposed system provides a convenient and efficient environment for publishing, editing, and sharing diagnostic reports of patients through web interfaces. In particular, our report structure, which separately manages contents and their styles, provides the many benefits of managing large volumes of reports in more competitive ways. Such benefits include efficient storage management, fast and easy searching, and protected variation of data for easy customization of report styles.
References
- 1.Wong STC, Tajndra D, Wang H, Shen W. Workflow-enabled distributed component-based information architecture for digital medical imaging enterprises. IEEE Trans Inf Technol Biomed. 2003;7(3):171–182. doi: 10.1109/TITB.2003.813790. [DOI] [PubMed] [Google Scholar]
- 2.Cao X, Huang HK. Current status and future advances of digital radiology and PACS. IEEE Eng Med Biol. 2000;19(5):80–88. doi: 10.1109/51.870234. [DOI] [PubMed] [Google Scholar]
- 3.IHE Technical Framework, Integration Profiles, Revision 5.5. Radiological, Society of North America, Apr. 2003. [Online]. Available at: http://www.ihe.net/Technical Framework/index.cfm
- 4.Grimes SL. The challenge of integrating the healthcare enterprise. IEEE Eng Med Biol. 2005;24(2):122–124. doi: 10.1109/MEMB.2005.1411360. [DOI] [PubMed] [Google Scholar]
- 5.National Electrical Manufacturers Association, Digital Imaging and Communications in Medicine (DICOM) PS-3, NEMA standard, Oct. 2004; dicom.nema.org
- 6.Grimson J, Stephens G, Jung B, Grimson W, Berry D, Pardon S. Sharing health-care records over the internet. IEEE Internet Comput. 2001;5(3):49–58. doi: 10.1109/4236.935177. [DOI] [Google Scholar]
- 7.Jepsen T: IT in healthcare: Progress report. IEEE IT Prof pp. 8–14, Jan./Feb. 2003
- 8.Bedel V. PACS strategy for imaging centers. Radiol Manage. 2004;26(5):24–29. [PubMed] [Google Scholar]
- 9.Boyer J: XForms, ver. 1.1, W3C recommendation, Mar, 2006; http://www.w3.org/TR/2006/REC-xforms-20060314/
- 10.Hur W, et al. Customizable workflow monitoring. Concurr Eng Res Appl. 2004;11(4):313–325. doi: 10.1177/1063293X03039903. [DOI] [Google Scholar]
- 11.Clark J: XPath, ver. 1.0, W3C recommendation, Nov. 1999; http://www.w3.org/TR/xpath
- 12.Boag S, et al. XQuery, ver 1.0, W3C recommendation, Nov. 2005; http://www.w3.org/TR/xquery
- 13.Microsoft Co. Ltd: Native XML Web Services Overview. http://msdn2.microsoft.com/en-us/library/ms188266.aspx
- 14.Kay M: XSL Transformation(XSLT), ver 2.0, W3C recommendation, Nov. 1999; http://www.w3.org/TR/xslt20