

Abstract
The objective of this study was to determine the differential cost between film-based radiology and a hospital-wide picture archiving and communication system (PACS) implemented all at once. The cash flow and running costs of PACS and film-based operation were measured over an 8-year time horizon. When the hospital-wide PACS was implemented over a short period, there was instant conversion into digital film and archives. The net present value (NPV) for PACS operation is US $1,598,698, whereas the NPV for film-based operation is US $2,083,856, indicating a net saving of US $485,157. The payback period is 4 years. The costs of computed radiography and image plates account for 40% of the initial capital expenditure in PACS implementation, followed by computer hardware (30%) and software (9%) costs. Our experience shows that implementation of hospital-wide PACS all at once can produce cost savings. For hospitals intending to go filmless, this study offers a model for financial evaluation of PACS to help in decision making.
Key Words: Medical economics, picture archiving and communicating system (PACS), cost analysis, computer-assisted radiography, radiology and radiologists
Background
Picture archiving and communication systems (PACS) reduce the number of unread, retaken, and lost films. PACS can improve performance through changes in work flow. Productivity of technologists is also increased in computed tomography (CT) and plain-film studies after PACS implementation.1–7 Many hospitals implement the system gradually, starting with a mini-PACS in the radiology department. However, because of the complexity of patient care, films are still produced for viewing outside the department. Building a partial PACS in a hospital involves accessory costs. In many studies, the costs of PACS exceed the savings.8–10 In today's health care environment, reducing health care expenditures is a major object for hospital management. Whether implementation of PACS can create net savings through reduction of film-related expenses remains to be proven. Pratt et al10 performed an incremental cost analysis and found that when film-based operation was gradually replaced by PACS over an 8-year time horizon, the department incurred additional net costs with PACS. At Hammersmith Hospital in the United Kingdom, where a PACS was constructed from 1991 to 1996, computed radiography (CR) was used within the department but laser-printed images were provided to outside users until the whole hospital switched to digital imaging.11 PACS was associated with significantly increased costs. Our review of the PACS literature revealed no comprehensive cost analyses of implementation of a hospital-wide PACS all at once. We tried to build a model for financial assessment of hospital-wide, full-scale PACS to help in the formulation of strategies for PACS implementation.
Methods
The study hospital is a government-owned hospital. It has 482 beds and 100 physicians. The radiology department performed 150,000 studies in 2002. Between 1997 and 2002, there was a 10% annual increase in utilization of the radiology department.
By 2004, some imaging modalities had already been installed, including four conventional x-ray machines, one DICOM (digital imaging and communications in medicine)-compatible ultrasound, one CT unit, and one magnetic resonance unit. An older CT unit was already transforming images into DICOM format by gateway. A hospital-wide PACS was proposed in mid 2003 and implemented from January to March 2004. As part of PACS, additional imaging modalities were also purchased, including three high-capacity CR processors and one autochest CR.
The PACS was fully integrated with a hospital information system (HIS) via a radiology information system (RIS). The requested information generated by HIS was transformed into a modality work list for the DICOM-compatible machine as image tags. The modality performed procedure step allows study completion information to feed back to HIS.
The reason we chose to move from film-based operation to filmless all at once was to avoid running costs of dual systems and to reduce the cost of laser films, which are more expensive than conventional films. After installation of and education about PACS, the hospital reached the goal of a 100% reduction in film within 2 weeks, except in the mammography and remote fluoroscopic units. Because films in outpatient clinics are the least frequently viewed, we began the transition to filmless operation at outpatient clinics, followed by the emergency room and wards. After PACS was fully implemented, two of the five full-time employees in the film library were dismissed, and the remaining three switched to doing registration and scheduling. Besides the supporting staff from the vendor, half of the employees in the information technology (IT) department share the management of PACS. The net present value (NPV) of the differential cost between film-based operation and PACS was calculated.
Assumptions
All assumptions used in this research were based on the experience of five heads of radiology departments, two professors expert in administration of health care organizations, and one professor of computer science. The assumptions were as follows:
An 8-year time horizon is used.
A discount rate of 3% is assumed.
The number of examined images increases by 5% per year, with 2002 as the reference year.
If PACS were not installed, the hospital would have to purchase three film processors at years 0, 4, and 8.
The PACS short-term storage holds 1 year of recent images, and the long-term images are stored in redundant array of independent disks (RAID) arrays, purchased annually according to the amount of image files.
Backup tapes for disaster recovery are purchased constantly every year during the estimation period.
The annual maintenance cost of PACS is estimated at 5% of the initial purchase cost.
The hardware of PACS work stations used by clinicians and radiologists can last for 4 years and will be replaced in the fifth year.
The upgrade costs of software PACS are included in the maintenance cost.
Both CR and conventional film cassettes are replaced at a similar rate and similar prices; it is assumed that there is no significant price difference between them.
The concurrent web viewing for multiusers can cover the increasing demand for viewing images.
The price of computer-related hardware remains the same during the estimation period.
Differential Cost Analysis
PACS Cost Model
Time zero is the time when the hospital became 100% filmless. Maintenance for the first 2 years was included in the initial purchasing contract.
The CR cassettes bought at time zero were guaranteed for 2 years. No additional CR cassettes were needed in the first 2 years. We estimated that from the third year, 10 cassettes would be replaced annually.
Two database servers perform in a high-availability backup pattern. The archive server is composed of two database servers under the database management system of ORACLE 9i with the function of real application cluster (RAC) and Dataguard to reach the availability of 99.999%. When there is a network failure, a plan of manually connecting machinery directly to a laser printer for temporary film output is used. Storage is categorized as short-term storage, long-term storage, and backup tape systems. The short-term storage consists of a 2 terabyte (TB) hard disk; after partition, there are 1.4 TB available, including 1 TB for image storage. There are two forms of images, with different compression rates for client-server image viewing and web-based image viewing. The short-term storage can keep at least 6 months of studies. RAID arrays are used for long-term storage and are purchased annually. With the 5% yearly increase in examined images, the annual long-term storage needed is adjusted by 1-TB steps according to the amount of image data to be generated.
Two of the five full-time employees in the film library were dismissed. Besides supporting staff from the vendor, half of the personnel of the IT department share the management of PACS.
Film-Based Cost Model
Operation costs of a film-based system include the cost of purchasing and maintaining film processors; the cost of films, chemicals, film jackets, conventional film cassettes, and film disposal; and the wages of film library clerks. Previous records of film-related costs were used to calculate costs of film-based operation. Ten cassettes are replaced annually. Space in the film library is kept for archiving old studies.
Net Present Value
When the financial impact of a project is assessed, after identification of all annual cash flows, the timing of the cash flows determines their relative values from today's perspective. A dollar is worth more today than it will be 1 year from now.10,12,13 NPV is estimated according to the following formula:
 |
where Ct is cash flow at time t, r is the discount rate, and N is the lifetime of the project. The capital expenditure for PACS is a negative value. The cost savings of film-based operation are a positive value. NPVs were calculated according to the discount rate of 3%. The payback period is the time when PACS produces cost savings compared with film-based operation.
For the sensitivity analysis, NPVs were recalculated for discount rates of 0%, 3%, and 5%13; initial capital expenditure; annual increase in examined images; CR-related costs; computer-related hardware costs; and maintenance costs, to compare with the NPV for base-case assumption.
Results
Costs of PACS Operation
Table 1 presents a summary of costs for PACS operation. The initial capital expenditure for PACS implementation at time zero was US $699,497. There is a surge in costs in year 5 because of work station-related hardware replacement. The NPV is US $1,598,698. CR processors and CR cassettes account for most of the cost (40.0%), followed by work station-related hardware (29.8%), work station software (8.9%), storage (8.3%), servers (7.8%), web access (4.3%), and network (0.9%).
Table 1.
Costs of PACS Operation, 2004–2012 (US $)
| NPV | Year 0 | Year 1 | Year 2 | Year 3 | Year 4 | Year 5 | Year 6 | Year 7 | Year 8 | |
|---|---|---|---|---|---|---|---|---|---|---|
| CR readers | 203,030 | |||||||||
| CR cassettes | 76,618 | 15,152 | 15,152 | 15,152 | 15,152 | 15,152 | 15,152 | |||
| Image and database server | 54,603 | |||||||||
| Work station-related hardware | 208,736 | 208,736 | ||||||||
| Client-server work station software | 62,424 | |||||||||
| Web server and licenses | 30,303 | |||||||||
| Storage | 57,895 | 6,061 | 6,061 | 6,061 | 6,061 | 9,091 | 6,061 | 9,091 | 6,061 | |
| Network | 5,886 | |||||||||
| Maintenance | 34,975 | 34,975 | 34,975 | 34,975 | 34,975 | 34,975 | ||||
| IT staff | 7,273 | 7,273 | 7,273 | 7,273 | 7,273 | 7,273 | 7,273 | 7,273 | ||
| Mammography film and chemical and film magazine | 9,382 | 9,382 | 9,382 | 9,382 | 9,382 | 9,382 | 9,382 | 9,382 | ||
| Full-time employee for administration | 36,000 | 36,000 | 36,000 | 36,000 | 36,000 | 36,000 | 36,000 | 36,000 | ||
| Film processor maintenance | 6,545 | 6,545 | 6,545 | 6,545 | 6,545 | 6,545 | 6,545 | 6,545 | ||
| Annual cost | 699,497 | 65,261 | 65,261 | 115,387 | 115,387 | 327,154 | 115,387 | 118,417 | 115,387 | |
| PV | 699,497 | 63,360 | 61,515 | 105,595 | 102,520 | 282,206 | 96,634 | 96,284 | 91,088 | |
| NPV | 1,598,698 |
CR: computed radiography; IT: information technology; NPV: net present value; PACS: picture archiving and communication system; PV: present value.
Costs of Film-Based Operation
Table 2 shows the costs of film-based operation. The NPV is US $2,083,856. The film-related costs such as films, film processing chemicals, and film jackets and stickers increased as the number of examined images increased annually. The costs of films, chemicals, and film jackets make up 58% of the total costs, followed by film processor costs and related costs (22%), and wages for film library clerks (20%).
Table 2.
Costs of Film-Based Operation, 2004–2012 (US $)
| NPV | Year 0 | Year 1 | Year 2 | Year 3 | Year 4 | Year 5 | Year 6 | Year 7 | Year 8 | |
|---|---|---|---|---|---|---|---|---|---|---|
| Film processors | 60,606 | 60,606 | 60,606 | |||||||
| Film cassettes | 15,152 | 15,152 | 15,152 | 15,152 | 15,152 | 15,152 | 15,152 | 15,152 | ||
| Films, chemicals, film jackets | 145,533 | 152,810 | 160,450 | 168,473 | 176,896 | 185,741 | 195,028 | 204,780 | ||
| Film processor maintenance | 26,182 | 26,182 | 26,182 | 26,182 | 26,182 | 26,182 | 26,182 | 26,182 | ||
| Film-related employee | 60,000 | 60,000 | 60,000 | 60,000 | 60,000 | 60,000 | 60,000 | 60,000 | ||
| Annual cost | 60,606 | 246,866 | ,254,143 | 261,783 | 330,412 | 278,230 | 287,074 | 296,362 | 366,719 | |
| PV | 60,606 | 239,675 | 239,555 | 239,569 | 293,568 | 240,004 | 240,419 | 240,969 | 289,492 | |
| NPV | 2,083,856 |
NPV: net present value; PV: present value.
Differential Cost Analysis
The NPV for the differential cost between PACS and film-based operation for the time horizon of the project is equal to the NPV for film-based operation minus the NPV for PACS operation. The NPV for the differential cost is US $485,157, indicating a net saving for PACS operation (Table 3).
Table 3.
Incremental Cost Summary, 2004–2012 (US $)
| NPV | Year 0 | Year 1 | Year 2 | Year 3 | Year 4 | Year 5 | Year 6 | Year 7 | Year 8 | |
|---|---|---|---|---|---|---|---|---|---|---|
| Costs related to PACS implementation | ||||||||||
| CR processors | −203,030 | |||||||||
| CR image plates | −76,618 | −15,152 | −15,152 | −15,152 | −15,152 | −15,152 | −15,152 | |||
| Image and database server | −54,603 | |||||||||
| Work station-related hardware | −208,736 | −208,736 | ||||||||
| Work station-related software | −62,424 | |||||||||
| Web server and licenses | −30,303 | |||||||||
| Storage | −57,895 | −6,061 | −6,061 | −6,061 | −6,061 | −9,091 | −6,061 | −9,091 | −6,061 | |
| Network | −5,886 | |||||||||
| Maintenance | −34,975 | −34,975 | −34,975 | −34,975 | −34,975 | −34,975 | ||||
| IT staff | −7,273 | −7,273 | −7,273 | −7,273 | −7,273 | −7,273 | −7,273 | −7,273 | ||
| Mammography film, chemical and film magazine | −9,382 | −9,382 | −9,382 | −9,382 | −9,382 | −9,382 | −9,382 | −9,382 | ||
| Film processor maintenance | −6,545 | −6,545 | −6,545 | −6,545 | −6,545 | −6,545 | −6,545 | −6,545 | ||
| Savings from film-based operation for 8 years | ||||||||||
| Dismissal of full-time employee | 24,000 | 24,000 | 24,000 | 24,000 | 24,000 | 24,000 | 24,000 | 24,000 | ||
| Film processors | 60,606 | 60,606 | 60,606 | |||||||
| Film cassettes | 15,152 | 15,152 | 15,152 | 15,152 | 15,152 | 15,152 | 15,152 | 15,152 | ||
| Films, chemicals, film jackets | 145,533 | 152,810 | 160,450 | 168,473 | 176,896 | 185,741 | 195,028 | 204,780 | ||
| Film processor maintenance | 26,182 | 26,182 | 26,182 | 26,182 | 26,182 | 26,182 | 26,182 | 26,182 | ||
| Incremental cost per annum | −638,891 | 181,606 | 188,882 | 146,397 | 215,025 | −48,924 | 171,687 | 177,944 | 251,332 | |
| Incremental PV per annum | −638,891 | 176,316 | 178,041 | 133,973 | 191,048 | −42,202 | 143,785 | 144,685 | 198,404 | |
| Incremental NPV | 485,157 | |||||||||
CR: computed radiography; IT: information technology; NPV: net present value; PACS: picture archiving and communication system; PV: present value.
Sensitivity Analysis
Table 4 shows the sensitivity analysis for each parameter. The NPV of US $485,157 by our assumptions was the base case.
Table 4.
Sensitivity Analysis
| Low Sensitivity | Base Case | High Sensitivity | Comments/Reference | |
|---|---|---|---|---|
| Discount rate | 0% | 3% | 5% | 13 |
| NPV ($) | 645,058 | 485,157 | 399,658 | |
| % of base NPV | 133% | 100% | 82% | |
| Annual increase in examined images | 0% | 5% | 10% | At Baltimore Veteran Affairs Medical Center, utilization of radiology services increased 48% in 3 years [13]. There was a 10% annual increase in examined images at our hospital from 1998 to 2003 |
| NPV ($) | 252,954 | 485,157 | 767,250 | |
| % of base NPV | 52% | 100% | 158% | |
| Initial cash flow | 70% | 100% | 130% | When a large number of equipment purchases are to be made, vendor-estimated discounts of 15–50% are assumed for many purchases3 |
| NPV ($) | 695,006 | 485,157 | 275,308 | |
| % of base NPV | 143% | 100% | 40% | |
| CR-related costs | 70% | 100% | 130% | Same as above |
| NPV ($) | 590,471 | 485,157 | 201,471 | |
| % of base NPV | 121% | 100% | 66% | |
| Computer-related hardware costs | 70% | 100% | 130% | Same as above |
| NPV ($) | 586,021 | 485,157 | 384,294 | |
| % of base NPV | 21% | 100% | 79% | |
| Maintenance costs | 3% | 5% | 10% | Annual maintenance cost at Hammersmith Hospital is approximately 6%. Usual cost of computer-related maintenance (without hardware replacement) is set at 5%; with hardware replacement, cost sometimes ranges up to 10% |
| NPV ($) | 556,593 | 485,157 | 306,568 | |
| % of base NPV | 115% | 100% | 63% |
CR: computed radiography; NPV: net present value.
Figure 1 shows the accumulated present value for every year of the project. The accumulated NPV becomes positive at the beginning of the fourth year. In the fifth year, with the accessory costs generated from replacement of work station-related hardware including diagnostic and physician usage, the PACS operation shows fewer net costs than film-based operation. Therefore, the payback period is roughly 4 years.
Fig 1.
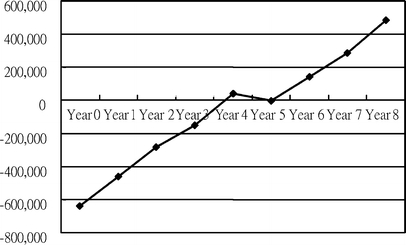
Accumulated present value. Adjusted payback period is 4 years.
After the implementation of PACS, clinicians are pleased with the new benefits such as saved time on film archiving, telephone consultation on images by concomitant image sharing, and a decreased number of lost films. The emergency room and ICU can accelerate patient treatment by omitting the time used for film transportation. The outpatient clinics also benefit by the reduction of patient waiting time for instant imaging reading. Since the set-up of the filmless environment and this article was written (an 8-month period), there has been no server failure except for a 5-h downtime at night for the entire hospital IP address change. No exact film output was made.
Discussion
Our study shows that implementation of PACS all at once can produce net savings. With low initial capital outflow and a sufficient number of examinations, a hospital-wide PACS with carefully controlled expenditures brings the advantage of computer technology and has a favorable economic impact.
The keys to success in implementing PACS all at once include full support of the chief executive officer, support of clinical physicians, cost savings, and process simplification. Cost savings are the main issue in adoption of PACS. The main savings of PACS are attributable to the tremendous reduction in film-related variable costs, followed by savings in film processors and wages of film library clerks. When a PACS is set up, the rapid transformation to a filmless environment is a key factor in reducing costs. A hospital-wide, whole-scale PACS set up all at once can produce the best chance to filmless operation.
However, there are some risk factors associated with implementation of PACS all at once. Acceptance by clinical physicians; a user-friendly interface for registration employees, technicians, radiologists, and physicians; and integration of HIS-RIS and PACS are the most difficult components. The IT and radiology departments should work together for request for proposal. For the system to be fully accepted by the physicians, we had a previous version of mini-PACS for the limited DICOM-compatible US and CT modalities implemented in year 2000. Physicians were already aware of the advantages of PACS and had the basic idea of image viewing. They viewed images from mini-PACS while the original films were being used by other physicians or radiologists. In planning for a hospital-wide PACS, clinical physicians had input about the sites of image work stations, the functions of image viewers, the length of time for image pop-up, the hot keys of HIS that bring out images, etc. Before the transition to working without hard-copy films, the advanced concept of PACS was introduced to each hospital department via a scheduled program, and several hospital-wide briefings of the system were conducted. During the 2-week transformation, the system was gradually incorporated into outpatient clinics, then the emergency room and wards. The members of the vendor and radiology departments offered on-site consultation to assist others to retrieve images without hard-copy film.
To establish a PACS, we faced the issues of multimodality and multivendor scenarios, including vendors of system integrators, image viewing software, x-ray machinery, CR readers, networking, personal computers, high-resolution monitors for medical purposes, etc. However, our institution purchased PACS all in one project to simplify the administrative procedure. A vendor with a well-established reputation and experience is required. The multimodality vendors, integrated together for competition purposes, and a program manager led the process of implementation.
Those image files from previous mini-PACS were migrated into the new system. The film library is still opened for the retrieval of old films. The film library is still opened for the retrieval of old films. However, the usage of the service reduced rapidly from 20 film jackets per day to 5 per day in 2 months. This number further decreased to 10 films per month in 6 months because the new images were digitized as opposed to being made into hard-copy films. As a result of the reduction in workload, two out of five film library clerks were reassigned to other departments. We did not plan for space recovery because additional manpower and space would be needed to move these old films. Thus, the cost for space of film library as a sunk cost in both operations was not included in the differential cost analysis. The PACS servers consist of two racks and are stored in the computer room of the IT department that has been set up for all mainframe servers. However, after 8 years, the films can be disposed of (thereby freeing up some space).
The average life of x-ray machines is estimated to be 8 years. However, computers are usually less durable than x-ray machines. This means that in the fifth year of the project, work station hardware will need to be replaced. Although most companies replace computers every 3 years, some replace computers after a longer period for cost saving. According to the Internal Revenue Service (IRS), “The entire acquisition cost of a computer purchased for business use can be...depreciated over a 5-year recovery period.” We counted on using this hardware for PACS for 4 years and then purchasing new materials in the fifth year. This factor was not considered in most of the existing articles on financial evaluation of PACS,8–10 or the costs were probably included in maintenance costs.
For comparison between PACS and film-based operation, the differential cost should include costs of film processors and costs of maintenance required for both types of operation. The costs of film processors will have a positive impact, in terms of NPV, on implementation of PACS, as in our case.
In recent years, interest rates have lowered to historic levels. We used 3% as the discount rate on the basis of average bank interest rates. As the NPV is positive, increasing the discount rate would decrease the NPV by a certain amount, but it does not make it negative.
Annual incremental increases in the expected number of images examined have a great influence on NPV. At the Baltimore Veterans Affairs Medical Center,15 use of radiology services increased, in 3 years, by 82% among inpatients and 38% among outpatients after PACS implementation. Our hospital had a 10% annual rate of increase from 1998 to 2002. Although we expect (after PACS implementation) a higher annual increase in number of examinations, insurance reimbursement factors have a tremendous impact on the behavior of physicians. We adopted a modest rate of 5% as the base case. If there is no increase in number of examinations, the NPV is still positive, which is about 24% of the base case. When the volume of examinations increases more than we assumed it would, the variable costs of PACS operation will be the costs of storage of image files—costs far lower than the variable costs of film-based operation—and thus there will be a great cost advantage.
The initial capital expenditure is determined by the PACS design. Minimizing purchase price without hampering daily medical service is the key to cost savings. In our design, there is no expensive form of long-term storage. RAID arrays are purchased annually according to the expected volume of image files, and tapes are used for disaster recovery. These approaches cut the purchase price to a large degree. CR processors and cassettes account for 40% of the initial cost. Therefore, the need for CR processors should be carefully evaluated.
Expense of work station-related hardware makes up 30% of cost for PACS. We have an equal number of diagnostic work stations and radiologists. For clinician work stations, imaging graphic ports and high-resolution monitors were added on to existing computers if possible. Web design with a certain number of concurrent users offers the unlimited image viewing capability for new work station demand and uses already existing computers, without added hardware costs.
Mammography was not digitized in our design, because the high costs of direct radiography mammography machines and accessory diagnostic work stations with 5 K-resolution monitors offset any savings achieved through filmless operation. For mammography to be digitized, the number of examinations should be high enough to achieve economies of scale. If a mammography screening center has a high study volume, a separate NPV evaluation could be performed to help in decision making. In our hospital, the cost of film-based operation for mammography is less than US $15,152 per year, which does not justify digitization.
Maintenance fee is a highly fluctuating variable that might include service on software and/or hardware. The maintenance cost is set at 5% of the initial purchasing price in the base case analysis, and after plugging in a range of scenarios from 3% to 10% maintenance fee, the NPV of the project remains beneficial with the worst scenario being 63% savings.
There are a lot of difficult tasks in PACS implementation. Being a large investment, PACS requires the support of the CEO. Due to the high price, cost savings should be expected from the installation of PACS. If this was not the case, the investment would impede the financial structure of the hospital. For hospitals planning on adopting PACS, all of the departments in which medical imaging is generated should plan early and gradually replaced equipment with standardized DICOM-compatible plug-in-and-play function. Otherwise, by upgrading the equipment or inserting gateways (which cannot offer full imaging adjustment), the costs of PACS will increase.
Cooperation between the IT and radiology departments and general agreement in the entire workplace are easier to achieve for small- to medium-sized hospitals. Larger medical institutions may face more difficulties from resolute physicians who wish to adhere to traditional film reading. If the equipment in the hospital is mostly non-DICOM-compatible, the costs of installing PACS will be higher, and its benefits will be limited. Also, the computer apparatus may not be as durable and replacements may be needed earlier than scheduled, which will increase the cost.
Conclusion
PACS can reduce patients' waiting time, prompt the management of critical patients, reduce unavailability of images, increase productivity of devices and technicians, enable on-line phone consultation, save time for physicians and radiologists, and reduce staffing needs.14,16 Our study shows that a properly designed PACS can produce cost savings compared with film-based operation. For hospitals intending to go filmless soon, this study offers evidence, obtained through differential cost analysis, in support of PACS implementation.
Acknowledgment
I thank Professor Hsin-Ginn Hwang for his encouragement and advice regarding the content of this paper. I am grateful to Dr. Ta-Yi Huang and Mr. Tsair-Jin Perng for help in PACS design and process reorganization. Thanks also to Dr. Ran-Chou Chen and Dr. Adeline Woan-Chwen Jaw for suggestions about assumptions.
References
- 1.Reiner BI, Siegel EL, Hooper FJ, Glasser D. Effect of film-based versus filmless operation on the productivity of CT technologists. Radiology. 1998;207:481–485. doi: 10.1148/radiology.207.2.9577498. [DOI] [PubMed] [Google Scholar]
- 2.Reiner BI, Siegel EL, Carrino JA, Goldburgh MM. SCAR Radiologic Technologist Survey: Analysis of the impact of digital technologies on productivity. J Digit Imaging. 2002;15:132–140. doi: 10.1007/s10278-002-0021-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Chan L, Trambert M, Kywi A, Hartzman PACS in private practice—effect on profits and productivity. J Digit Imaging. 2002;15(suppl 1):131–136. doi: 10.1007/s10278-002-5019-8. [DOI] [PubMed] [Google Scholar]
- 4.Andriole KP. Productivity and cost assessment of computed radiography, digital radiography, and screen-film for outpatient chest examinations. J Digit Imaging. 2002;15:161–169. doi: 10.1007/s10278-002-0026-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Reiner BI, Siegel EL. Technologists’ productivity when using PACS: comparison of film-based versus filmless radiography. AJR Am J Roentgenol. 2002;179:33–37. doi: 10.2214/ajr.179.1.1790033. [DOI] [PubMed] [Google Scholar]
- 6.Tamm EP, Raval B, West OC, Dinwiddie S, Holmes R. Evaluating the impact of workstation usage on radiology report times in the initial 6 months following installation. J Digit Imaging. 1999;12(suppl 1):152–154. doi: 10.1007/BF03168786. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Bryan S, Weatherburn GC, Watkins JR, Buxton MJ. The benefits of hospital-wide picture archiving and communication systems: a survey of clinical users of radiology services. Br J Radiol. 1999;72:469–478. doi: 10.1259/bjr.72.857.10505012. [DOI] [PubMed] [Google Scholar]
- 8.Siegel EL, Reiner BI. Filmless radiology at the Baltimore VA Medical Center: a 9 year retrospective. Comput Med Imaging Graph. 2003;27:101–109. doi: 10.1016/S0895-6111(02)00083-6. [DOI] [PubMed] [Google Scholar]
- 9.Charvet-Protat S, Thoral F. Economic and organizational evaluation of an imaging network (PACS) (in French) J Radiol. 1998;79:1453–1459. [PubMed] [Google Scholar]
- 10.Pratt HM, Langlotz CP, Feingold ER, Schwartz JS, Kundel HL. Incremental cost of department-wide implementation of a picture archiving and communication system and computed radiography. Radiology. 1998;206:245–252. doi: 10.1148/radiology.206.1.9423679. [DOI] [PubMed] [Google Scholar]
- 11.Bryan S, Weatherburn G, Buxton M, Watkins J, Keen J, Muris N. Evaluation of a hospital picture archiving and communication system. J Health Serv Res Policy. 1999;4:204–209. doi: 10.1177/135581969900400405. [DOI] [PubMed] [Google Scholar]
- 12.Arenson RL. PACS: current status and cost-effectiveness. Eur Radiol. 2000;10:S354–S356. doi: 10.1007/PL00014092. [DOI] [PubMed] [Google Scholar]
- 13.Drummond MR, O’Brien BJ, Stoddart GL, Torrance GW. Methods for the Economic Evaluation of Health Care Programmes. 3rd ed. Oxford: Oxford University Press; 2005. pp. 55–101. [Google Scholar]
- 14.Avrin DE, Arenson RL. Avoiding unread images with PACS. Acad Radiol. 2002;9:1331–1332. doi: 10.1016/S1076-6332(03)80567-6. [DOI] [PubMed] [Google Scholar]
- 15.Reiner BI, Siegel EL, Flagle C, Hooper FJ, Cox RE, Scanlon M. Effect of filmless imaging on the utilization of radiologic services. Radiology. 2000;215:163–167. doi: 10.1148/radiology.215.1.r00ap41163. [DOI] [PubMed] [Google Scholar]
- 16.Gennip V, Enning J, Fischer F, Glaser KJ, Kilbinger M. Guidelines for cost-effective implementation of picture archiving and communication systems: an approach building on practical experiences in three European hospitals. Int J Biomed Comput. 1996;43:161–178. doi: 10.1016/S0020-7101(96)01201-9. [DOI] [PubMed] [Google Scholar]