

Abstract
The purpose of this study was to measure the impact of electronic signature on report turnaround time. The Radiology Information System (RIS) database was interrogated to obtain a file containing all examinations recorded within a one-month period. Two sectors were specifically studied: abdominal ultrasound and chest radiography. Each of these sectors had one reader per day. The periods studied were October 2001 (before implementation of electronic signature) and February 2002 (3 months after electronic signature implementation). For the abdominal ultrasound examinations, the median time from transcription to final signature decreased from 11 days to 3 days with the introduction of electronic signature (P < 0.001). For the chest radiographs, the median time from transcription to final signature decreased from 10 days to 5 days with the introduction of electronic signature (P < 0.001). Electronic signature significantly shortens the time interval between transcription and finalization of radiology reports.
Keywords: Electronic signature, diagnostic reporting, report turnaround
An important justification for the introduction of information technology in imaging departments is the expected impact on productivity. These technologies, by either eliminating or shortening steps in the traditional workflow, have been shown to increase productivity.1,2,3,4 The Radiology Information System (RIS) makes it possible to follow the status of individual examinations from the moment a study is requested until the moment a final report is available. This allows a time-line study of the workflow in a radiology department and also makes it possible to assess the impact of various modifications to the various processes.5 In our department, the electronic signature module was incorporated into the report management module of our RIS approximately 6 months after implementation of the RIS. This modification enabled us to study the impact of electronic signature on report turnaround time.
METHODS
The RIS records the time of each status change for each exam entry. The RIS database was interrogated to obtain a file containing all examinations recorded within a one-month period. For each exam entry the data file contained the date and time of each status change (i.e., requested, performed, dictated, transcribed, report confirmed). Two sectors were specifically studied: abdominal ultrasound and chest radiography. Each of these sectors had one reader per day, and a number of radiologists rotated through the sectors throughout the periods studied. The periods studied were October 2001 (before implementation of electronic signature) and February 2002 (3 months after electronic signature implementation). The time interval from transcription of a report to the signature of the report by the radiologist was computed for each examination, for the sectors mentioned and during the 2 months selected. For each month and for each sector the median time interval from transcription to final signature was computed. The results were compared using the Mann Whitney test.
To assess the radiologists’ reaction to the implementation of electronic signature a short survey was distributed. The following questions were asked: (1) Do you perform your own corrections on screen? (2) Do you consider electronic signature a positive addition? (3) Does electronic signature improve the radiologists’ workflow?
RESULT
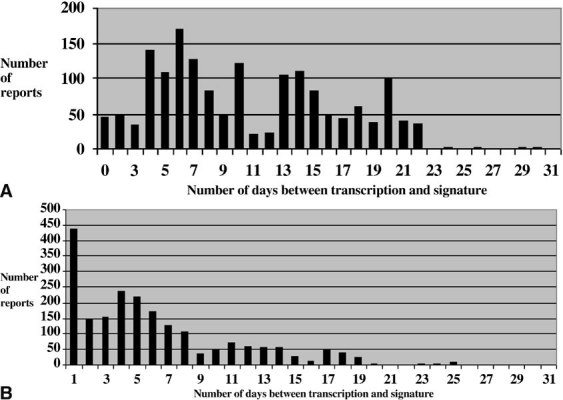
In the month of October 2001,466 abdominal ultrasound examinations and 1,651 chest radiographs were recorded in the RIS. In the month of February 2002, 402 abdominal ultrasound examinations and 2113 chest radiographs were recorded in the RIS. For the abdominal ultrasound examinations, the median time from transcription to final signature decreased from 11 days to 3 days with the introduction of electronic signature (P < 0.001). The proportion of finalized reports at 3 and 7 days after transcription increased from 8.8% and 26.6%, respectively, to 44.8% and 61.4% after the introduction of electronic signature. The histograms showing the number of reports as a function of the delay between transcription and finalization before (Fig 1a) and after (Fig 1b) implementation of electronic signature show a change in the distribution of the data. With electronic signature, most reports are signed in the first 2 days, with a sharp drop-off thereafter. For the chest radiographs, the median time from transcription to final signature decreased from 10 days to 5 days with the introduction of electronic signature (P < 0.001). The proportion of finalized reports at 3 and 7 days after transcription increased from 7.7%% and 40.8%%, respectively, to 34.9%% and 70.8%% after the introduction of electronic signature. The histograms showing data distribution before (Fig 2a) and after (Fig 2b) electronic signature show an effect similar to that seen for abdominal ultrasound examinations.
Figure 1.

A. Number of days between transcription and signature before implementation of electronic signature for abdominal ultrasound reports. B. Number of days between transcription and signature after implementation of electronic signature for abdominal ultrasound reports.
Figure 2.
A. Number of days between transcription and signature before implementation of electronic signature for chest radiograph reports. B. Number of days between transcription and signature after implementation of electronic signature for chest radiograph reports.
All 42 radiologists surveyed answered the questions. All radiologists claimed to perform their own corrections on screen. When asked if they believed that electronic signature was a positive addition, 100% answered yes, and 80% believed that it improved the radiologists’ workflow.
DISCUSSION
The introduction of information technology is seen as an opportunity to improve efficiency and quality in all facets of operation in a radiology department. In this context, the RIS can be used as a management tool, not only to obtain an ongoing assessment of the many processes occurring in a clinical imaging department, but also to identify problems and assess the impact of various interventions designed to modify the workflow or re-engineer the operations of the department. Our study exemplifies the use of the RIS for this purpose; more specifically, it permitted us to study the effect of electronic signature on the timeliness of delivery of radiology reports.
The timely delivery of radiology reports is an important objective in any department. Many steps are involved, from the moment an imaging study is requested to the moment a final report is produced and available, either on paper or on a computer network. The introduction of electronic signature can accelerate this process by shortening the time between transcription and signature. In a paper-based system, the transcribed report may travel several times between the radiologist and the secretary before it is finalized. This loop can effectively be eliminated by replacing the paper-based system and allowing the radiologist to view, correct or modify, and sign reports electronically. At the moment the reports are signed, they immediately become available on the hospital information network and are identified as final. The reports are also available after transcription, but they are labeled preliminary until signed. Our study shows that the median time from transcription to final report status significantly decreased after the introduction of electronic signature. This finding is in agreement with studies published earlier.6,7 Also, a larger proportion of the reports are signed earlier, as demonstrated by the distribution of reports as a function of delay between transcription and signature. Although this seems obvious, there was hesitation and skepticism on the part of many radiologists who were not convinced they would have the time or patience to read and correct reports on a computer. Some radiologists perceived this as a shift of secretarial duties to them. This is reflected in the opinion of 20% of radiologists who felt that their workflow was not improved. Taking into consideration the smaller number of working days in the month of February, the results do not show a decrease in productivity, as determined by the overall number of studies completed before and after the introduction of electronic signature. Abdominal ultrasound and chest radiographs were chosen because of the high volume of cases and a standardized mode of functioning in each sector. Whether or not the actual workload of the radiologists is increased by the introduction of electronic signature was not assessed by our study. The workload includes the time planning, performing, and interpreting imaging studies, as well as the time reading, correcting, and signing the reports.
Voice recognition systems can accelerate the production of radiology reports to an even greater extent. Studies have shown an important decrease in the time needed to make a final report available when such a system is used.3 If a voice recognition system is not available, however, electronic signature can be an effective means of improving efficiency compared to a paper-based system. Aside from the economic factors involved in implementing a voice recognition system, delays in the introduction of such systems can arise because they have not attained the same level of sophistication in all languages. Some studies have shown that voice recognition can actually diminish the radiologist’s productivity.8 So although, ultimately, voice recognition systems will become the norm, at present electronic signature is an interesting alternative offering significant advantages. Also, electronic signature can represent an intermediate step before the introduction of voice recognition, allowing familiarization with on-screen editing for those radiologists still working in a paper-based system.
CONCLUSION
Electronic signature significantly shortens the time between transcription and finalization of radiology reports. The RIS allows assessment of workflow by recording the timeline of status changes of imaging studies and can be used to evaluate the impact of interventions on the processes in a radiology department.
References
- 1.Reiner BI, Siegel EL, Hooper FJ, et al. Effect of film-based versus filmless operation on the productivity of CT technologists. Radiology. 1998;207:481–485. doi: 10.1148/radiology.207.2.9577498. [DOI] [PubMed] [Google Scholar]
- 2.Mehta A, Dreyer K, Boland G, et al. Do picture archiving and communication systems improve report turnaround times? J Digit Imaging. 2000;13(Suppl 1):105–107. doi: 10.1007/BF03167637. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Langer SG. Impact of speech recognition on radiologist productivity. J Digit Imaging. 2002;15:203–209. doi: 10.1007/s10278-002-0014-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Mattern CW, King Jr BF, Hangiandreou NJ, et al. Electronic imaging impact on image and report turnaround times. J Digit Imaging. 1999;12(Suppl 1):155–159. doi: 10.1007/BF03168787. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Crabbe JP, Frank CL, Nye WW. Improving report turnaround time: an integrated method using data from a radiology information system. AJR Am J Roentgenol. 1994;163(6):1503–1507. doi: 10.2214/ajr.163.6.7992756. [DOI] [PubMed] [Google Scholar]
- 6.Frank MS, Rowberg AH. Authentication and management of radiologic reports: value of a computer workstation integrated with a radiology information system. AJR Am J Roentgenol. 1993;161:1309–1311. doi: 10.2214/ajr.161.6.8249749. [DOI] [PubMed] [Google Scholar]
- 7.Seltzer E, Kelly P, Adams DF, et al. Expediting the turnaround of radiology reports in a teaching hospital setting. AJR Am J Roentgenol. 1997;168:889–893. doi: 10.2214/ajr.168.4.9124134. [DOI] [PubMed] [Google Scholar]
- 8.Gale B, Safriel Y, Lukban A, et al. Radiology report production times: voice recognition vs. transcription. Radiol Manage. 2001;23:18–22. [PubMed] [Google Scholar]